A ZigBee-based Wireless Monitoring and
Automatic Information Pushing and Caution
System for Pressure Ulcer Prevention
Tsui-Ying Wang
*,***, Shang-Liang Chen
**, We-Li Wang
*and
Ho-Chuan Huang
****Keywords : alarm system, position diagnosis,
pressure ulcer, ZigBee.
ABSTRACT
Pressure ulcer (PU) was caused by tissue necrosis due to long term pressure. We developed a ZigBee-based wireless monitoring and alarm system for pressure ulcer prevention. It uses pressure sensors in a ZigBee network to monitor pressured positions for patients. The system monitors the position in real time; makes position diagnosis; identifies a position at risk; and actively sends alarm messages to staff designated for PU management. The success rate of data collection was above 90% and the position diagnosis is 100% consistent with statistical clustering results and videotaping records. The alarm message was also successfully delivered to client devices. The pressure ulcer prevention system is therefore feasible for clinical use to assure the prevention of pressure ulcer and increase the quality of healthcare.
INTRODUCTION
A pressure ulcer (PU) is caused by unrelieved interface pressure that disrupts blood supply and leads to ulceration or tissue necrosis (Bluestein and Javaheri, 2008) The annual cost of PU care has been estimated at $11 billion in the US (Gordon, et al.,
2004; Kuhn and Coulter, 1992), and £1.4 - £2.1 billion in the UK (McInnes, et al., 2008), and the relevant expenditure was ranked the third, after those for cancer and cardiovascular disease, in the Netherlands (Netherlands THHCot, 1999). Moreover, if a patient develops PU in the hospital, it may have legal consequences (Reddy, et al., 2006). PU not only decreases the quality of life at the individual level, but also imposes a public burden for the healthcare system (Bluestein and Javaheri, 2008; Gorexki, et al., 2009; Russo, et al., 2008).
The risk factors of PUs include pressure, shearing forces, friction, and moisture (Bluestein and Javaheri, 2008). Pressure applied on the skin that is higher than arteriolar pressure (32 mmHg) causes an insufficiency of oxygen and nutrients in tissue, which results in tissue damage (Kosiak, 1959). An animal model study suggested that pressure exceeded of 70 mmHg for two hours would lead to irreversible tissue damage (Kosiak, 1961). The most common sites for PUs are over bony prominences, such as the sacrum, heels, ischial tuberosities, greater trochanters, and lateral malleoli, which are the weight-bearing points for different positions (Bluestein and Javaheri, 2008). The pressure applied on the skin is more significant than other factors in the management of ulcer preventions (Stekelenburg, et al., 2008). The effectiveness of pressure reduction devices, such as static mats and dynamic beds, is either not supported by research evidence or too expensive to clinical use, and patients may still develop PUs if left unattended for an extended period of time (Horn, et al., 2004; Reddy, et al., 2006). Currently, there is no effective strategy that works well for controlling PUs.
Intermittently relieving skin pressure prevents tissue damage and deterioration. Clinical guidelines recommend a two-hour schedule for repositioning (Bluestein and Javaheri, 2008; Reddy, et al., 2006). However, there is usually a gap between the best practice guideline and actual practice because of heavy loads of patient care, duty-shift patterns, and unawareness of the ulcer risk (Horn, et al., 2004; Park, et al., 2010). Because healthcare staffs are usually
Paper Received January, 2011. Revised April, 2011. Accepted May, 2011, Author for Correspondence: Shang-Liang Chen.
*
Graduate Student, Institute of Manufacturing Information and Systems, National Cheng Kung University, Tainan 701, Taiwan, ROC.
**
Professor, Institute of Manufacturing Information and Systems, National Cheng Kung University, Tainan 701, Taiwan, ROC.
***Assistant Professor, Department of Occupational Therapy,
National Cheng Kung University, Tainan 701, Taiwan, ROC.
****
Associate Professor, Department of Information Management, National Kaohsiung University of Applied Sciences, Kaohsiung 807, Taiwan, ROC.
J. CSME Vol.32, No.3 (2011)
immersed in busy and often trivial duties, an electronic reminder would be a good solution to increase their awareness of PUs without increasing their memory load.
Because e-healthcare products are becoming more popular, researchers have integrated different functional sensors, wireless tags, and digital cameras for home automation, body area networks, and telemedicine services (Chan, et al., 2008). However, very few studies have proposed a solution for PU prevention (Yip, et al., 2009). Some commercial products have been developed, such as human & animal pressure mapping systems (Tekscan, South Boston, MA) and pressure imaging (XSENSOR, Alberta, Canada). They use body pressure mapping method to analyze the pressure distribution. Although these systems provide both data storage and reliable data in real time, they may still have some disadvantages, such as cost, durability, and maintenance difficulties, that limit the applicability for clinical settings. Moreover, some systems contain many sensors that need calibration for different positions and different patients every time. These systems do not provide any position information or feedback mechanism for critical states of patients, because their major purpose is to detect the pressure magnitude distribution of postures and movement in order to develop pressure deduction devices (Verbunt and Bartneck, 2010; Yip, et al., 2009). The pressure mapping method may provide high resolution of pressure distribution, but there are no criteria of the pressure threshold for a position alarm. To detect the interface pressure state of a specific position, one needs to perform data reduction by abstracting the information from sections of sensor array (Verbunt and Bartneck, 2010). Other studies or products use sensor embedded pressure beds with or pressure sensor pads to monitor the bed movement of the elderly. The pressure pad (or bed) with or without an alarm system is majorly used for fall detection or exit alarm, in order to reduce restraint use and increase patient safety (Kwok, et al.,2006). Therefore, they do not provide any position monitoring or recording function that can be applied to PU monitoring. Their expenses and designed functions limit the affordability and applicability, and therefore not suitable in meeting the needs of PU monitoring and alarm. Some researchers tried to develop a flexible, low-cost pressure monitoring system, which provides visual display of pressure magnitude with good resolutions, to solve the limitation of the above system (Yip, et al., 2009). However, this system has not been designed and applied to detect the pressured positions. In summary, all the systems mentioned above display only pressure information on a screen for observers, but provide no position status, no explanations or interpretations of any data patterns, nor do they permit remote retrieval of patient information.
Remote monitoring has been developed to enhance the quality of care and is imperative for clinicians or caregivers to gather patient's information. Remote monitoring systems with various sensing technologies for personal health have been extensively studied (Chan, et al., 2008). Integrated wireless sensor networks (WSNs), which have embedded microcontrollers, integrated physical sensors, and radio interfaces integrated on a single chip, are now being more frequently used for healthcare monitoring (Al Ameen, et al., 2010; Bonato, 2005; Milenkovic, et al., 2006; Jovanov, et al., 2000). WSNs have the advantages of unattended operation and high mobility, which make them suitable for remotely monitoring patients. There are reports, for example, on integrating motion sensors and a personal server for computer-assisted rehabilitation applications to monitor patients’ health states and movements in a system using the ZigBee protocol (Jovanov, et al., 2005; Milenkovic, et al., 2006). Several remote monitoring systems as such have been studied or developed for physiological information, but system for in-bed position or movement monitoring has been rarely addressed in this areas.
To prevent PUs, however, a pressure monitoring system is not enough. A caution system capable of identifying the repositioning needs and sending an alarm in a simple, efficient, and wireless network-based way would be more practical. In the present study, we developed a pressure ulcer caution system (PUCS), based on a ZigBee sensor network (ZSN), to monitor, record, and send wirelessly information about the patient's states to a caregiver. The main purpose of the PUCS is to establish a preventive mechanism that allows real-time monitoring of the patient's position and sending short messages (SMS) to the caregiver or nursing staff for further management. In addition, the PUCS is designed to be simple, low-cost, non-intrusive, and integrative for sensor data, position detection, and pressure alarm, in order to meet clinical needs.
SYSTEM DESIGN
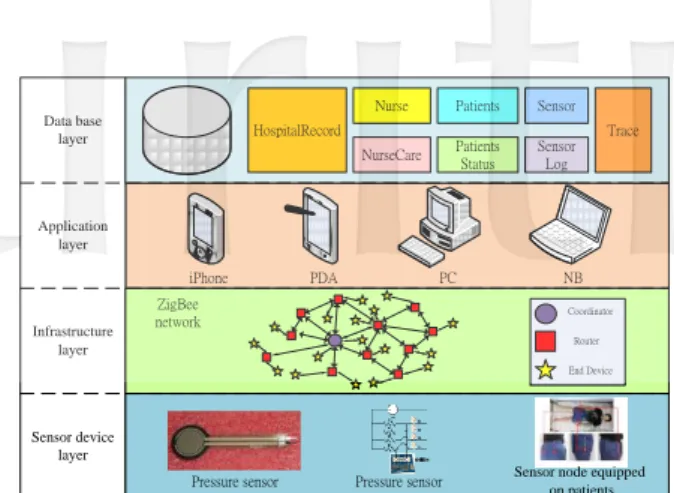
A four-layer architecture has been designed for the PUCS (see Fig. 1). They are infrastructure layer, application layer, database layer and sensor device layer. At the infrastructure layer, the pressure sensor node worn by the patient will collect pressure data from patient. The collected data will be transmitted wirelessly to PUCS through the ZigBee sensor network. At the application layer, the collected pressure data, including local pressure data and temporal data, will be converted into the appropriate format to analyze a patient's sustained positions in the PUCS server side. The end users of PUCS could be nurses, non-nurse caregivers, or other relevant staff. At the database layer, the PUCS
Data base layer Application layer HospitalRecord NurseCare Nurse Patients Patients Status Sensor Sensor Log Trace ZigBee network Infrastructure layer Sensor device layer
Pressure sensor Pressure sensor Sensor node equipped on patients
End Device Coordinator Router
iPhone PDA PC NB
Fig. 1. Four layers system architecture of the developed PUCS
application may access the stored data which is related to the patient medical information.
The names of the database table included in this PUCS are briefly explained as follows: (1) HospitalRecord table: This table stores the recorded data about the patient’s treatment in this hospital. The stored data include serial number, division, and treatment method, etc. (2) Nurse table: This table stores the personnel data of nurses in the hospital. The stored data include nurse’s ID number, name, mail address, phone number, and password, etc. Sensor table: This table stores the sensor’s setting parameters which is set for the patient. The stored data include sensor’s address, pressure data sensed, triggering frequency, first and second alarm time period, and counting time, etc. (3) Patients table: This table stores the personal data of patients. The stored data include patient’s ID number, name, mail address, phone number, blood type, telephone number, sensor matching, etc. (4) NurseCare table: This table stores the connection data between the nurse and the patient. The stored data include serial number, nurse ID, patient ID, and nurse’s sign in/out data, etc. (5) SensorLog table: This table stores the sensed data from the sensors worn by the patient. The stored data include serial number, chart number, date and time, data received from pressure sensor node, and status of threshold checking for received pressure data, etc. (6) Trace table: This table stores the data about the patient’s treatments for tracing purpose. The stored data include serial number between nurse and patient, nurse ID, chart number, medication, intake and discharge of medical treatment, etc. (7) PatientsStatus table: This table stores the status data of patient. The stored data include serial number, nurse ID, chart number, Date, doctor's prescriptions and notes, patient consciousness, ability of dressing, hygiene, eating, toileting, mobility, wheelchair bound or bedridden, etc.
At the sensor device layer, a pressure sensor is combined with a ZigBee sensor to form a ZigBee sensor node. Here, the ZigBee sensor node can be worn by the patient as the size of the sensor is small.
Of course, the type of sensors used may be varied depending on different applications.
Planning of ZigBee sensor network
In this developed PUCS, an end device node is consisted of one type A ZigBee sensor and four pressure sensors. There are two types of sensor nodes included in this ZigBee network. For type A sensor node (see Fig. 2a), the main functions included are RF unit, and CC2431 MCU (Micro Controller Unit). Size of the type A sensor node is very small and is suitable for the applications with subject in moving status. For the type B sensor node (Fig. 2b), a UART-to-USB IC is added into type A sensor node. Therefore, it is suitable to be applied as the sink sensor node, and links to PC for sending commands and receiving packets. Both the type A and type B sensor nodes can be used as coordinator sensor node depending on which program is installed. The specifications of the ZigBee sensor (type A and B) used in this research are as follows: (1) Size : 28 mm
28 mm. (2) Control unit: Chipcon CC2430/31, Texas Instruments, with one directional antenna. (3) One transceiver with IEEE 802.15.4 protocol. (4) RF range up to 100 meters. (5) 30-pin expansion connector. The 30-pin expansion connector can connect to four pressure sensors and be equipped with two AA batteries for longer life. (6) Two hardware asynchronous receiver/transmitter (UART) channels that support wireless data communication.
Fig. 2a. Type A sensor node
Fig. 2b. Type B sensor node with USB port The transmission distance in the wireless transmission depends on RF power, transmission sensitivity, and the transmission frequency. The data of these three specifications can be applied into wireless free space propagation model for obtaining the ideal transmission distance. The transmission specifications of ZigBee sensor node used in this
J. CSME Vol.32, No.3 (2011)
research are summarized as follows: (1) Power Transmitter, Pt: 1mW. (2) Power receiver, Pr: -85dB. (3) Transmission frequency, f: 2.4GHz.
The transmission distance in a free space environment can be calculated using the propagation path loss model (Rappaport, 1996). The equation is given in the following:
Pr(dB) = Pt + Gr + Gt - L (1) Pr (dB) is the link budget in decibels. Pt (dB) is the transmitted power in decibels referred to milliwatts (mW) or watts. Gt (dB) is the transmitter-antenna gain in decibels. Gr (dB) is the receiver-antenna gain in decibels. L (dB) is the receiver sensitivity.
Here, the power transmitter is Pt = 1mW. The power transmitter in decibels can be calculated using the decibel’s definition:
Pt (dB) =10 log (Pt mW) = 10 log(1 mW) Then,
Pt (dB) = 0 (dB)
There are no transmitter-antenna and receiver-antenna used in this Zigbee sensor node. Therefore, Gt = 0 dB and Gr = 0 dB. Replace the obtained data of Pt, Pr, Gt, Gr into Eq. 1, we have
-85dB = 0 + 0 + 0 –L
Therefore, receiver sensitivity is: L = 85dB
Receiver sensitivity is defined as the minimum L signal that the system can detect with an acceptable LF (signal-to-noise ratio). With the free space propagation model applied, the receiver sensitivity can be defined as:
LF (dB) = 32.4 + 20 logR + 20logf (MHz) (2) In the above equation, R is transmission distance (m) and f is transmission frequency (MHz). Replace the obtained data into Eq. 2, we have
85dB = 32.4 + 20 logR + 20 log2400 Then, R can be calculated,
R = 102.63 x 1000/2400 = 177 (m)
From the above calculation, the free space transmission distance of ZigBee sensor node used in this research is 177 m. Many instruments and equipment in the hospital may affect the transmission distance. Therefore, a radius of 20 meters is planned in this research for placing a ZigBee router in a hospital.
Selection of piezo-resistive sensor
Three types of pressure sensor are widely used in the industry. There are capacitive pressure sensor, piezo-electric pressure sensor and piezo-resistive pressure sensor. A thin film piezo-resistive pressure sensor was selected and applied into the tests in this research. The pressure sensor is packed, using a polymer material, to form a thin film appearance, and it was thin (0.03-0.1 mm) and highly durable against environmental interference. The characteristic of thin film is important for this research (see Fig. 3), as it will not cause any uncomfortable feeling for the patient.
Fig. 3. A thin-film piezo-resistive pressure sensor The piezo-resistive pressure sensor was inserted into the clothes of the patients. It will generate a voltage variation signal when the physical pressure on the patient skin is varied. Four resistors are designed and connected with four piezo-resistive sensors separately for enhancing the sensing sensitivity. Fig. 4 shows the circuit design diagram of the piezo-resistive sensor. The voltage values of P1 (Lh1)、P2 (Lh2)、P3 (Rh1)、P4 (Rh2) can be obtained by using a simple voltage divider rule. The physical meaning of (Lh1), (Lh2), (Rh1), and (Rh2) is shown in Fig. 6. The collected pressure data will be transferred back (in wireless) to nurse station by using the developed ADC software which is installed in the memory of end device. The voltage divider rule is a simple method of determining the output voltage across one of two impedances connected in series way. From Fig. 4, the voltage divider rule is:
Pi : Ri = VP : VR (3) VP + VR = V (4) VP is Pi’s partial pressure, and VR is Ri’s partial pressure. Eq. 4 is replaced into Eq. 3, VP can be obtained as:
PUCS monitoring is technically feasible for actual patients. It requires no complicated calibration procedure, because the sensors are easily attached to a patient’s clothes. The body weight and figure did not affect the sensor sensitivity to an interface pressure between body and the bed. The time-series sensor data was transmitted at a success rate of 91.4%. Unsuccessful data transmissions did not affect the position diagnosis or alarm trigger for a setup time threshold.
One might question that the PUCS used only 4 pressure sensors to detect the pressure that maybe too simple or the precision is questionable. However, cross-validation of the sensor states and position diagnosis from PUCS, clustering technique, and the position sequence by video recording were 100% consistent, which confirmed that the theoretical values set for sensor on/off states, and the inference method were appropriate. Our design was to find certain anatomical locations of a position which bear pressure most frequently. We assumed these frequently pressed locations should be watchful and also sensitive to sensor measurement. Areas at risk of PU development provide good observing targets for sensor deployment. We chose four sites that near but avoid the bony sites, and the results showed that number and location of sensors were sufficient for the pressure detection purpose and able to collect data for lying position diagnosis of patient. The prone position was less in bedding patients and was not tested. The sitting position was not monitored in this study but PU is also a significant issue for wheelchair user for their lack of mobility and sensation awareness. PUCS paradigm used with this population will be studied in the future.
The on/off criteria were set as 1565 (32mmHg) which may be criticized as too subjective. The criterion was chosen because 32 mmHg has been mostly cited in PU literature as a reference pressure value for further risk of tissue damage. Since the critical pressure-time relationship has not been studied in human research, and recent guidelines and studies usually used 2 hours and 32mmHg for the maximum tolerance of a risk condition of PU (Bluestein and Javaheri, 2008; Verbunt and bartneck, 2010), we decided to use the same criteria but leave it adjustable if reserch evidence or clinical guidelines updated in the future.
The advantages of the PUCS design are its adaptability and scalability. The simple sensors used in the PUCS's end-devices are very thin and durable. The force-resistive sensors can, if necessary, be replaced with other types of pressure sensors or sensor sheets to give more precise measurements of pressure magnitude. The time threshold of the sustained position and pressure magnitude in the sensor setting can be easily adjusted based on individual patient risk levels or future guidelines updated by pressure-time relationship
studies. Finally, the functions of the PUCS can be expanded by adding additional sensors for other monitoring purposes, such as temperature, humidity, or motion.
CONCLUSIONS
A ZigBee-based wireless monitoring, automatic information pushing and caution system is developed, implemented, and tested for pressure ulcer prevention for immobile patients. The developed PUCS is a low-cost and high-efficiency monitoring system that provides remote monitoring and actively sends alarms to remind users to check for critical conditions that cause PUs. The lying position of patients can be continuously monitored, and time-series sensor data can be wirelessly transmitted, processed, and recorded in a database. Correctness of pressure sensing data transmission and position diagnosis was successfully validated. Future refinement of the PUCS to apply to real patients is warranted. The PUCS should improve the quality of healthcare because it should reduce the incidence of PUs in immobile patients with its preventive mechanism.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the support to part of this research by the National Science Council, Republic of China, under Grant Nos. NSC-99-2221-E-006-207-MY3 and NSC-99-2221-E- 006-176.
REFERENCES
Al Ameen M., Liu J., and Kwak K., "Security and Privacy Issues in Wireless Sensor Networks for Healthcare Applications," J Med Syst. Epub ahead of print, pp.1-9 (2010).
Bluestein D. and Javaheri A., "Pressure ulcers: prevention, evaluation, and management," Am Fam Physician. Vol. 78, No. 10, pp.1186-1194 (2008).
Bonato P., "Advances in wearable technology and applications in physical medicine and rehabilitation," J Neuroeng Rehabil Vol.2, No.1, pp.2-8 (2005).
Chan M., Estève D., Escriba C., and Campo E., "A review of smart homes--Present state and future challenges," Comput Methods Programs Biomed.Vol. 91, No. 1, pp.55-81 (2008).
Gordon M.D., Gottschlich M.M., Helvig E.I., Marvin J.A., and Richard R.L., "Review of Evidenced-Based Practice for the Prevention of Pressure Sores in Burn Patients," J Burn Care Res. Vol. 25, No. 5, pp.388-410 (2004). Gorecki C., Brown J.M., Nelson E.A. et al., "Impact
T.Y. Wang et al.: A ZigBee-based Wireless Monitoring and Automatic Information.
patients: a systematic review," J Am Geriatr Soc. Vol. 57, No.7, pp.1175-1183 (2009). Horn S.D., Bender S.A., Ferguson M.L., et al., "The
National Pressure Ulcer Long-Term Care Study: Pressure Ulcer Development in Long-Term Care Residents," J Am Geriatr Soc. Vol. 52, No.3, pp.359-367 (2004). IAR. IAR Embedded Workbench for ARM. 2010;
http://www.iar.com/website1/1.0.1.0/68/1/. Accessed 19 December, (2010).
Jovanov E., Milenkovic A., Otto C., and de Groen P. A., "Wireless body area network of intelligent motion sensors for computer assisted physical rehabilitation," J Neuroeng Rehabil.Vol. 2, No.1, pp. 6-10 (2005).
Jovanov E., Price J., Raskovic D., Kavi K., Martin T., Adhami R., "Wireless personal area networks in telemedical environment," Paper presented at: Proceedings of IEEE EMBS International Conference on Information Technology Applications in Biomedicine (2000).
Kosiak M. Etiology and pathology of ischemic ulcers. Arch Phys Med Rehabil.;Vol. 40, No.2, pp.62-69 (1959).
Kosiak M., "Etiology of decubitus ulcers," Arch Phys Med Rehabil. Vol. 42, pp.9-29 (1961)
Kuhn B.A., "Coulter SJ. Balancing the pressure ulcer cost and quality equation," Nurs Econ.; Vol.10, No. 5, pp.353-359 (1992).
Kwok T., Mok F., Chien W.T., Tam E., "Does access to bed-chair pressure sensors reduce physical restraint use in the rehabilitative care setting?" J Clin Nurs.Vol. 15, No.5, pp.581-587 (2006). McInnes E., Cullum Nicky A., Bell-Syer Sally E.M.,
Dumville Jo C., and Jammali-Blasi A., "Support surfaces for pressure ulcer prevention," Cochrane Database Syst Rev. Vol. 4;http://www.mrw.interscience.wiley.com/coc hrane/clsysrev/articles/CD001735/frame.html. (2008).
Milenković A., Otto C., and Jovanov E., "Wireless sensor networks for personal health monitoring: Issues and an implementation. Computer Communications," Special issue: Wireless Sensor Networks: Performance, Reliability, Security, and Beyond.Vol. 29, pp.2521-2533 (2006).
Netherlands THHCot., "Health Council of the Netherlands: Pressure Ulcers," 1999; http://www.gezondheidsraad.nl/en/publication s/pressure-ulcers. Accessed July 29, (2010). Park H-A.E., Cho I., and Chung E., "Exploring Use
of a Clinical Data Repository Containing International Classification for Nursing Practice-Based Nursing Practice Data," Comput Inform Nurs. Epub ahead of print. (2010).
Rappaport, T. S., "Wireless Communications," New Jersey: Prentice Hall PTR. (1996).
Reddy M., Gill S.S., and Rochon P.A. "Preventing Pressure Ulcers: A Systematic Review," J Am Med Assoc. Vol. 296, No.8, pp.974-984 (2006).
Russo C.A., Steiner, C., and Spector, W., "Hospitalization related to pressure ulcers among adults 18 years and older," 2006. Statistical Brief #64. Healthcare Cost and Utilization Project (HCUP). December 2008; http://hcup-us.ahrq.gov/reports/statbriefs/sb64 .pdf. Accessed July 29, (2010).
Stekelenburg A., Gawlitta D., and Bader D.L., "Oomens CW. Deep Tissue Injury: How Deep is Our Understanding?" Arch Phys Med Rehabil. Vol. 89, No.7, pp.1410-1413(2008). Verbunt M., and Bartneck C., "Sensing senses:
Tactile feedback for the prevention of decubitus ulcers," Appl Psychophysiol Biofeedback.Vol. 35, pp.243-250 (2010). Yip M., He D.D., Winokur E., Balderrama A.G.,
Sheridan R., and Hongshen M., "A flexible pressure monitoring system for pressure ulcer prevention," Annual International Conference of the IEEE Engineering in Medicine and Biology Society pp.1212-1215 (2009).