R E S E A R C H A R T I C L E
Open Access
The mediating effect of dietary patterns on
the association between mother
’s
education level and the physical aggression
of five-year-old children: a
population-based cohort study
Wen-Chi Wu
1, Ching-I Lin
2*, Yi-Fan Li
3, Ling-Yin Chang
4and Tung-liang Chiang
5Abstract
Background: Relatively few studies have investigated the effects of diet on behavior problems among
preschoolers, particularly, physical aggression. In addition, children raised by poorly educated mothers usually have a higher probability of developing negative outcomes. Additionally, highly educated mothers have a higher probability of providing more healthy foods for their children. Thus, mothers providing healthy foods might mitigate children’s behavior problems. The study aims to examine whether preschoolers’ dietary pattern, as a manipulable factor, mediates the association between maternal education level and physical aggression. Methods: Data came from the Taiwan Birth Cohort Study (TBCS), a nationally representative population-based cohort study, which included 18,513 five-year-old Taiwanese children. Mothers and primary caregivers reported the
information on preschoolers’ physical aggression and food consumption at age 5 and maternal education level at
age 6 months. Two dietary patterns, namely a healthy diet and a high-fat-sugar-salt (HFSS) diet, were retrieved by exploratory factor analysis. Mediation hypotheses were tested by a series of multiple regression models conducted using the PROCESS macro of SAS 9.4. All models were adjusted for children’s sex, parental marital status, household income, mental distress at age 5 and children’s physical aggression at age 3.
Results: Maternal education positively linked to healthy dietary patterns (B = 0.014,p = 0.002) which was negatively associated with preschoolers’ physical aggression (B = -0.096, p = 0.013), and it is negatively related to the HFSS dietary pattern (B = -0.042,p = 0.002) which was directly positively associated with preschoolers’ physical aggression (B = 0.123,p = 0.008). The association between maternal education and preschoolers’ physical aggression was partially mediated by preschoolers’ healthy (B = -0.001, p < .001) and HFSS (B = -0.005, p = <.001) dietary patterns, respectively. The R-square of the mediation model is 0.178.
(Continued on next page)
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence:cilin@mail.knu.edu.tw
2Department of Nutrition and Health Sciences, Kainan University, No. 1,
Kainan Road, Luzhu District, Taoyuan City 338, Taiwan
(Continued from previous page)
Conclusions: Preschoolers’ dietary patterns directly associate with their physical aggression. In addition, mothers with poor education may provide less healthy foods and more unhealthy foods to their children, which may increase the level of physical aggression. The results imply partial mediating effects of dietary patterns between maternal education and physical aggression. It is suggested that a parent-based nutritional education program focusing on healthy meal preparation for poor educated mothers might be beneficial for preschoolers’ healthy development.
Keywords: Dietary pattern, Physical aggression, Maternal education, Preschoolers
Background
Physical aggression in early childhood is a common havioral problem recognized by parents and teachers be-cause it is easily observed as overt acts. The behavior not only affects the children’s performance but also their interactions with siblings or peers [1,2]. Moreover, chil-dren with a higher level of physical aggression were more likely to develop adolescent physical aggression as well as anti-social and health risk behaviors [3,4]. Thus, understanding the related factors of young children’s ag-gression is essential for physical agag-gression prevention and child health promotion.
Many factors impact physical aggression in early child-hood [5]. One of the proximal factors raising consider-able concern is diet [6,7]. Diet has been associated with many conditions such as hyperactivity, attention defi-ciency, poor impulse control, conduct disorder, and ag-gressive behaviors [8–10]. Studies have found that some components of food may trigger behavioral problems, such as processed sugar, saturated fat, allergenic ele-ments, and chemical pigments [7,10]. However, the cav-eat of these studies is that they focused on the association of a single nutrient with behavior, while few studies have investigated the dietary patterns in relation to aggression, especially among preschoolers.
Instead of examining the single and relatively small ef-fect of a nutrient on behavior, understanding the cumu-lative effects of multiple nutrients contained in a dietary pattern may be more effective for risk prevention and health promotion [11]. Forming a proper dietary pattern is vitally important for young children because they are in the developmental stages of life. Although relatively few studies have empirically examined the effect of dietary pattern on physical aggression in early childhood [9], diet-ary pattern has been associated with depression [12], aut-ism [13], and attention deficit hyperactivity disorder [14]. Thus, to prevent and reduce preschoolers’ physical aggres-sion, more evidence is necessary to understand the influ-ences of different dietary patterns on physical aggression.
One important contextual factor of physical aggression in childhood is maternal education, that is, the highest level of schooling attended by mothers [15]. The theory of family functioning proposes that poorly educated
mothers, who may usually possess less knowledge and fewer resources to raise children adequately, are less likely to supervise and discipline their children, which increases the likelihood that a child will develop aggression-related behaviors [15]. Maternal education may have a larger effect than paternal education due to mothers commonly being the primary caregivers for pre-schoolers, especially in disadvantaged families [16, 17]. Maternal education was found to be an influential factor in preschoolers’ physical aggression [18]. Furthermore, it is also a crucial predictor of high-level physical aggres-sion from early childhood to adolescence [19].
Similarly, maternal education links to children’s diet-ary patterns because mothers are usually the primdiet-ary food providers for the majority of children [20]. Re-search has indicated that children with a poorly edu-cated mother had a higher score on the unhealthy dietary pattern [21]. Moreover, a highly educated mother may promote her children’s healthy diet through her own eating behavior [22].
From the results of the above studies, maternal educa-tion and diet are directly associated with physical
aggres-sion. In addition, maternal education can affect
children’s problem behavior either independently or through diet. It is speculated that dietary pattern may be a potential mediator between maternal education and physical aggression. However, no study has investigated the dietary pattern as a pathway from maternal educa-tion to physical aggression. Due to the alterability of dietary patterns, it may be a feasible target for a behavior intervention strategy.
The present study aims to examine whether dietary patterns mediate the relationship between maternal edu-cation and physical aggression.
Methods
Participants
The study data came from the Taiwan Birth Cohort Study (TBCS), the first longitudinal study which follows up a nationally representative sample of children born in 2005 [23, 24]. The project team used birth certificate data from 2005 as a sampling frame, and conducted two-stage stratified random sampling methods for
selecting participants. First, using the urbanization level and birth rates of 369 residential areas, we selected 89 areas by systematic random sampling methods. Second, there were 24,200 participants selected from the areas using the probability proportional to size method. The average sampling rate was 11.7%. TBCS aimed to docu-ment Taiwanese children’s health and developdocu-mental trajectories in order to investigate the influence of social environment on children’s health, and to examine how early events influence adult health by using the life course approach. Mothers or primary caregivers pro-vided their information by face-to-face interviews when the subjects were 6 months, 8 months, 3 years and 5.5 years of age with response rates of 87.8, 94.9, 93.7, and 92.8%, respectively. The reasons for attrition included being too busy, low willingness to participate, moving house, etc.
The interviewers received a“letter to the participants” from the Director-General, Health Promotion Adminis-tration, Ministry of Health and Welfare, Taiwan. The letter elaborated on the purposes, sampling methods, confidential process and contact information of the ad-ministrator. Then, the participants obtained a letter of consent from the interviewers in person. After the inter-viewee fully understood their rights and obligations and signed the consent form, the interviewer started the interview.
This study included 19,721 subjects whose parents and primary caregivers completed the interview survey at 5.5 years old. We used their information which was mea-sured at 6 months, 3 years old, and 5.5 years old. After excluding the participants with missing values, there were 18,513 participants (52.49% boys) analyzed in this study (retention rate = 93.9%). There were no differences between the analytic sample (n = 18,513) and the original sample (n = 19,721) in terms of sex, maternal education level, food consumption, mental distress, and physical aggression. However, those who remained in the analytic sample were significantly more likely to have parents who were married (90.67% vs. 87.63%) or parents with a higher education level (mean = 3.91 vs. 3.87; both P < 0·05).
Instrument development
The TBCS instrument was developed according to the following process. First, the first version of the questions for measuring each concept, such as physical aggression, dietary pattern and mental distress, etc., was developed based on previous literature. Second, the first-version questionnaire was reviewed by experts to ensure its face validity and was revised according to the reviewers’ com-ments. Third, the revised-version questionnaire was used for the pilot study (n = 1620) for pre-testing all the ques-tions, and the participants’ comments and feedback were
further collected to revise the questionnaire into its final version. In addition, some concepts, such as aggression and mental distress, were excerpted for a small group two-week test-retest reliability construction (n = 18).
Measurements
Maternal education level
Maternal education was measured based on the partici-pants’ report of the highest level of education attained by the mother when the child was 6 months old, ranging from uneducated (coded as 0) to graduate school or above (coded as 17). One score unit represents 1 year of education the mother completed. For example, score 11 means the mother completed the second year of high school education but did not graduate from high school, and score 12 means the mother graduated from high school.
Food groups for dietary patterns
Children’s diet was measured by the reports of primary caregivers when their child was 5 years old. The respon-dents were asked “How many times does your child eat the following foods a week?” The options included never (score = 0), less than once per week (score = 1), once or twice per week (score = 2), three to five times per week (score = 3), and almost every day or every day (score = 4). The 11 food groups were presented: meats, seafood (such as fish and shrimp), beans/bean products, eggs, grains/starchy roots, vegetables, fruits, dairy products, burger/pizza/fried chicken, candy/cookies/cakes, and beverages/Coca-Cola/Soft drinks. The first eight food groups were developed based on the Daily Dietary Guidelines provided by Taiwan’s Ministry of Health and Welfare [25], and the other three groups were chosen because they are common foods that are high in fat, sugar or salt [26, 27]. These groups of foods were used for the Exploratory Factor Analysis (EFA) to extract diet-ary patterns based on the variable-centered approach.
Physical aggression
The measurement of physical aggression for five-year-old children was developed with reference to the scale developed by Tremblay et al. [1] and Cote et al. [19]. The respondents were asked,“Did your child exhibit any of these behaviors in the last month?” when their chil-dren were 5 years old. Three items were used to measure physical aggression, including beating others, fighting with others, and biting or kicking others. Scores on this 3-item scale ranged from 1 (never) to 5 (always). The level of physical aggression was measured by averaging the responses, with higher scores indicating a higher level of physical aggression (Cronbach’s α = 0.77). The correlation coefficient of two-week test-retest reliability is 0.82.
Covariates
Five covariates were included to account for the poten-tial confounding in the association between parental education level, food consumption, and physical aggres-sion. Children’s sex was coded as 1 = boy and 0 = girl. Paren-tal mariParen-tal status at age 5 was coded as 1 = married and 0 = not married. Children’s physical aggression at the age of 3 was measured with the same three items which were used to measure physical aggression at age 5 (Cronbach’s α = 0.77). The responses of the three items were averaged to indicate the level of children’s physical aggression at the age of 3. Children’s mental distress scale was developed with reference to internalizing items of the Behavioral Assessment Scale for Children [28] and the Brief Problem Monitor-Parent Form [29]. To save space in the questionnaire, three questions, namely“Your child looks sad or depressed for no special rea-son,” “Your child feels fearful or anxious because of small matters” and “Your child worries about things not being well-done,” were selected and revised by some experts spe-cializing in child psychology, and the questions were rated on a 5-point scale (ranging from 1 to 5) at age 5 (Cronbach’s α = 0.61). The correlation coefficient of two-week test-retest reliability is 0.76. The mental distress level was constructed by averaging the responses to the three items, with higher scores indicating a higher level of mental distress. Household income was measured when the child was 6 months old by the respondents’ reports of the total family income in the last year, ranging from less than 100,000 NTD (coded as 1) to more than 3,000,000 NTD (coded as 8; 30 NTD≒ 1 USD).
Analytical strategy
Dietary patterns were extracted by EFA. Descriptive sta-tistics, including sample size, percentages, means, and
standard deviations, were used to describe the
characteristics of the study sample. Correlation analysis was conducted to determine the associations among ma-ternal education, children’s dietary patterns, and chil-dren’s physical aggression, as well as covariates.
In order to examine whether children’s dietary pat-terns mediate the association between maternal educa-tion and preschoolers’ physical aggression, we conducted a parallel multiple mediator model proposed by Hayes [30]. A series of multiple regression models were used to examine the association between maternal education and preschoolers’ dietary patterns (Fig. 1, path a1 and
a2), between preschoolers’ dietary patterns and their
physical aggression (path b1and b2), and between
mater-nal education and preschoolers’ physical aggression (path c, total effect) after adjusting for covariates. The direct effect of maternal education on preschoolers’ physical aggression (path c’) after adjusting for pre-schoolers’ dietary patterns and covariates was also com-puted. The mediation effects, i.e., the product of the coefficients of paths aiand bi were determined by using
a bootstrapping method with 10,000 resamples. The 95% bias-corrected bootstrap confidence interval (CI) was used to judge the significance of the mediation effect by not containing zero. All of the above analyses were con-ducted with the PROCESS macro version 2.2 of SAS 9.4. All models were adjusted for children’s sex, parental marital status, household income, mental distress at age 5 and children’s physical aggression at age 3.
Results
Dietary patterns
Exploratory Factor Analysis (EFA) using the original five-ordinal level of food groups with oblique rotation (Promax) was conducted to generate the latent structure
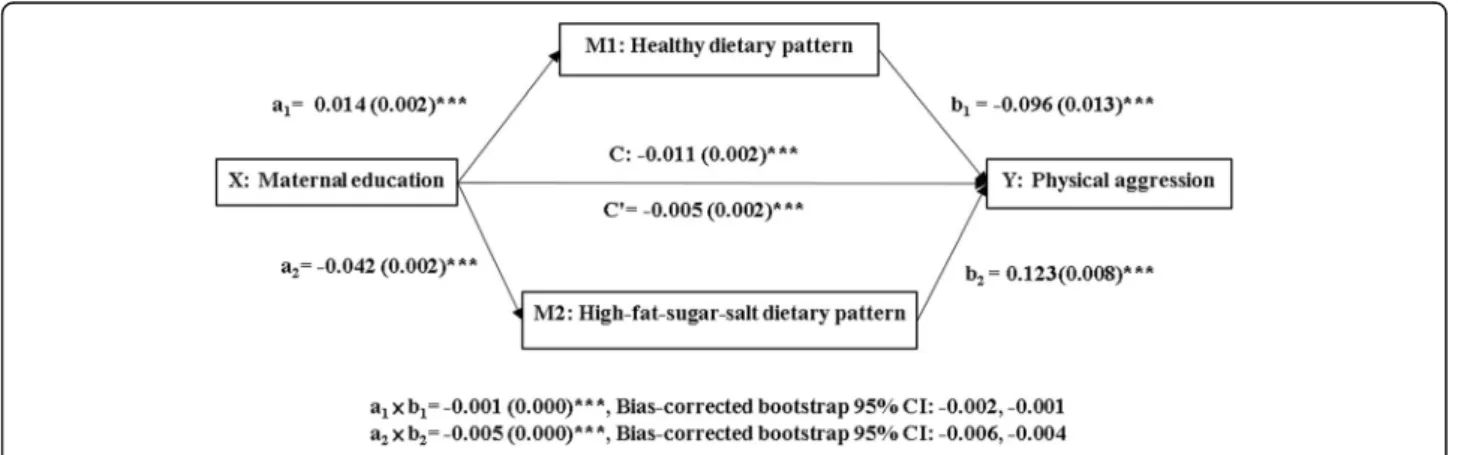
Fig. 1 A mediation model of association between maternal education and children’s physical aggression through dietary patterns. a1and a2= effects of maternal education on a healthy dietary pattern and a high-sugar-fat-salt dietary pattern. b1and b2= effects of healthy and high-sugar-fat-salt dietary patterns on physical aggression. C = total effects of maternal education on physical aggression. C′ = direct effect of maternal education on physical aggression after adjustment for dietary patterns and covariates. ai× bi= mediation effects of dietary patterns on the relationship between maternal education and physical aggression. The parameter estimates were presented as B(SE). X: independent variable. Mi: mediators. ***:p < .001. CI: confidence interval
of dietary patterns [31, 32]. The maximum likelihood method was used during iteration to estimate commu-nalities. Diagonals on the correlation matrix are squared multiple correlations (SMC) [33]. The Kaiser–Meyer–
Olkin value was 0.68. All analyses were conducted in the Statistical Analysis System software package version 9.4 (SAS Institute, Cary, NC, USA). Two factors were retained based on the retaining factors that accounted for greater than 75% of the common variance and had an eigenvalue greater than one. Eigenvalues of the weighted reduced correlation matrix are 1.82 and 1.23. The pro-portion of variance explained by each factor is 60 and 40%. Cumulative variance for the two factors is 100%. The factor loadings of each factor are shown in Table1.
The first factor was labeled as a healthy dietary pat-tern, which included the aforementioned first eight kinds of high-protein-and-high-fiber foods, and the score of this factor was constructed by averaging the frequencies of these eight food groups. The second factor was named as a high-fat-salt-sugar (HFSS) dietary pattern, which included the last three kinds of common un-healthy food groups which are high in fat, sugar, or salt [34]. Also, this factor score was constructed by averaging the frequencies of these three food groups (Table1).
Descriptive analysis
Table 2 shows the characteristics of the study sample. The children’s mothers had a mean educational level of 12.93 years (standard deviation (SD) = 2.62), and a mean household income of 3.91 units (SD = 1.29) which was
about 600,000 to 1,000,000 NTD (1 USD ≒ 30 NTD)
per year. The average score of healthy dietary pattern was 3.35 (SD = 0.4) indicating that the sample children consumed healthy foods about three to five times a
week, while the average score of HFSS dietary pattern was 1.93 (SD = 0.65) showing that they consumed un-healthy foods about once or twice a week. The average level of children’s physical aggression at age 5 was 1.68 (SD = 0.74) suggesting a low level, while the level of ag-gression was a little higher at age 3 (mean = 2.04, SD = 0.87). The mean score of the children’s mental distress was 1.54 (SD = 0.61), indicating a low level of mental dis-tress at age 5.
Table3presents the bivariate correlations among con-tinuous study variables. Maternal education is positively associated with children’s healthy dietary pattern, house-hold income, and mental distress, and negatively associ-ated with an HFSS dietary pattern, and physical aggression at ages 5 and 3. At the same time, the healthy dietary pattern was negatively associated with physical aggression at ages 5 and 3, and mental distress, and posi-tively associated with household income. Also, the HFSS dietary pattern was positively associated with physical aggression at ages 5 and 3, was not associated with men-tal distress, and was negatively associated with house-hold income. Physical aggression at ages 5 and 3 are highly positively correlated with each other, have a weak positive association with mental distress, and are nega-tively associated with household income.
Mediation analysis
Figure1and Table4demonstrate the relative total effect of maternal education on children’s physical aggression, considering dietary patterns and covariates. Children with mothers having a higher level of education showed less physical aggression (path C: B = -0.011, p = < .001). The mediation effects of children’s healthy dietary pat-tern and HFSS dietary patpat-tern on the associations
Table 1 Exploratory factor analysis of dietary patterns
Food groups n % Factor loadings
Factor 1: Healthy dietary pattern Factor 2: High-fat-sugar-salt dietary pattern Healthy food groups (never or < 1 time/week)
Fish, Shrimp, Seafood 1218 6.58 0.543 0.130
Meat 553 2.99 0.509 0.136 Fruits 323 1.74 0.453 −0.153 Bean 1542 8.33 0.440 −0.083 Vegetables 246 1.33 0.425 −0.187 Egg 541 2.92 0.421 0.078 Dairy products 1027 5.55 0.197 0.053
Grains and Roots 39 0.21 0.176 −0.037
HFSS food groups (almost every day or every day)
Beverages/ Coke / Soda 1479 7.99 −0.047 0.592
Hamburger/ Pizza/ Fried Chicken 90 0.49 0.036 0.484
Sweets/ Cookies/ Cakes 5024 27.14 0.023 0.436
between maternal education and children’s physical ag-gression are also shown. Results indicate that maternal education was positively associated with children’s healthy dietary pattern (path a1: B = 0.014, p = 0.002)
which was negatively associated with their physical ag-gression (path b1: B =− 0.096, p = 0.013). The indirect
ef-fect of maternal education on children’s physical aggression through the healthy dietary pattern was established (a1 b1=− 0.001, p < .001, Bias-corrected
bootstrap 95% CI: − 0.002, − 0.001). On the other hand, maternal education was negatively associated with chil-dren’s HFSS dietary pattern (path a2: B = -0.042, p =
0.002), which was positively associated with children’s physical aggression (path b2: B = 0.123, p = 0.008). The
indirect effect of maternal education on children’s phys-ical aggression through the HFSS dietary pattern was also confirmed (a2 b2=− 0.005, p = < .001,
Bias-corrected bootstrap 95% CI: − 0.006, − 0.004). Dietary patterns acted as partial mediators since they accounted
for some, but not all, of the relationship between mater-nal education and children’s physical aggression. The direct effect of maternal education on children’s physical aggression was suppressed but still moderately signifi-cant (path c’: B = − 0.005, p = 0.036). Approximately 18% of the variance for preschoolers’ physical aggression can be explained by the mediation model (R-square = 0.178). Discussion
Our findings show significant associations between diet-ary patterns and physical aggression among pre-schoolers, and maternal education level is an antecedent of dietary patterns and physical aggression. These results indicate that high maternal education level increases the score of a healthy dietary pattern and decreases the score of an HFSS dietary pattern, which in turn de-creases the level of preschoolers’ physical aggression. Dietary patterns may play an important role as media-tors, and can be manipulated to intervene in the
Table 2 Descriptive statistics of study variables (complete data,n = 18,513)
Mean SD Minimum Maximum
Maternal education (6 months) 12.93 2.62 0.00 17.00
Healthy dietary pattern (5 years old) 3.35 0.40 0.50 4.00
High-fat-sugar-salt dietary pattern (5 years old) 1.93 0.65 0.00 4.00
Physical aggression (5 years old) 1.68 0.74 1.00 5.00
Physical aggression (3 years old) 2.04 0.87 1.00 5.00
Mental distress (5 years old) 1.54 0.61 1.00 5.00
Household income (6 months) 3.91 1.29 1.00 8.00
n %
Boys 9718 52.49
Preschoolers living with married parents 16,785 90.67
Missing numbers: 6 of marital status, 595 of maternal education, 186 of income, 1 of healthy dietary pattern, 2 of high-fat-sugar-salt dietary pattern, 535 of aggression at 3 years old, 4 of mental distress, 4 of aggression at 5 years old
Table 3 Bivariate correlations among maternal education, dietary patterns, physical aggression and related factors (n = 18,513)
Maternal education Healthy dietary pattern High-fat-sugar-salt dietary pattern Physical aggression Physical aggression Mental distress Maternal education (6 months) (Range: 0–
17)
1.000 Healthy dietary pattern (5 years old) (Range: 0–4)
0.170 *** 1.000 High-fat-sugar-salt dietary pattern (5 years
old) (Range: 0–4)
− 0.216*** −0.007 1.000
Physical aggression (5 years old) (Range: 1–
5) − 0.103*** − 0.090***
0.170*** 1.000
Physical aggression (3 years old) (Range: 1– 5)
−0.126*** −0.078*** 0.149*** 0.381 *** 1.000
Mental distress (5 years old) (Range: 1–5) 0.036*** −0.029*** 0.003 0.104 *** 0.042 *** 1.000
Household income (6 months) (Range: 1–8) 0.527*** 0.194*** −0.164*** − 0.098 *** − 0.105 *** 0.002
association between maternal education and physical ag-gression. The direct association between diet and aggres-sion implies that encouraging preschoolers to have a healthy dietary pattern and avoid an unhealthy dietary pattern can protect them from physical aggression development.
We found a partial mediation effect of dietary pattern between maternal education and physical aggression among preschoolers, which reveals that dietary patterns partially intervene in the relationship between them. To the best of our knowledge, this is the first study that identifies a pathway showing that maternal education af-fects preschoolers’ dietary patterns, which in turn influ-ences their physical aggression. It should be noted that a previous study discovered that low zinc levels and low maternal education were associated with externalizing behaviors, respectively; however, the study did not con-sider the mediation effect of diet [35]. Our study sug-gests that greater attention to the education of parents
about a healthy dietary pattern is probably a practical way for physical aggression prevention in the preschool period.
Based on our EFA result, two dietary patterns were ex-tracted which are similar to the results of Ambrosini et al.’s study which retrieved two dietary patterns, the healthy and the Western pattern, among Australian adolescents [32]. The food groups used for EFA were selected by the research team following the instrument development process and can represent common foods rather than all kinds of foods among preschoolers. A healthy dietary pattern signifies a bal-anced diet which includes foods from the six essential food groups. A healthy diet has profound influences for young children in the preschool period because healthy eating be-haviors not only affect their health status but also affect their development of externalizing problem behaviors [35, 36]. The sufficient nutrients provided by these food groups, such as minerals and vitamins, have a positive influence on chil-dren’s moods [10,37].
Table 4 Results for the mediation analysis (n = 18,513)
M1: Healthy dietary pattern M2: High-fat-sugar-salt dietary pattern Y: Physical aggression
Direct effects Coeff. SE P Coeff. SE P Coeff. SE P
Constant 3.076 0.026 <.001 2.413 0.032 <.001 1.022 0.054 <.001
X: Maternal education (6 months) a1 0.014 0.002 <.001 a2 −0.042 0.002 <.001 c’ − 0.005 0.002 0.036
M1: Healthy dietary pattern (5 years old) b1 −0.096 0.013 <.001
M2: High-fat-sugar-salt dietary pattern (5 years old) b2 0.123 0.008 <.001
Cov 1: Child sex (ref: girl) (6 months) 0.008 0.006 0.157 0.008 0.009 0.405 0.120 0.010 <.001
Cov 2: Married parents (ref: not-married) (6 months) −0.002 0.010 0.839 −0.013 0.016 0.437 0.057 0.017 0.001
Cov 3: Physical aggression (3 years old) −0.024 0.003 <.001 0.090 0.005 <.001 0.291 0.006 <.001
Cov 4: Mental distress (5 years old) −0.020 0.005 <.001 0.004 0.008 0.574 0.109 0.008 <.001
Cov 5: Household income (6 months) 0.044 0.003 <.001 −0.032 0.004 <.001 −0.017 0.005 <.001
R2= 0.048 R2= 0.065 R2= 0.178 F(6, 18,506) = 154.34, p < .001 F(6, 18,506) = 213.21, p < .001 F(8, 18,504) =500.64, p < .001 Effect Bootstrap SE Bootstrap 95% CI Total effect of X on Y c −0.011 0.002 −0.016 −0.007 Direct effect of X on Y c’ −0.005 0.002 −0.009 0.000
Indirect effect of X on Y Effect Bootstrap
SE
Bootstrap 95% CI
M1: Healthy dietary pattern (5 years old) a1× b1 −0.001 0.000 −0.002 −0.001
M2: High-fat-sugar-salt dietary pattern (5 years old) a2× b2 −0.005 0.000 −0.006 −0.004
a1and a2= effects of maternal education on healthy dietary pattern and high-sugar-fat-salt dietary pattern b1and b2= effects of healthy and high-sugar-fat-salt dietary patterns on physical aggression
C = total effects of maternal education on physical aggression
C′ = direct effect of maternal education on physical aggression after adjustment for dietary patterns and covariates ai× bi= mediation effects of dietary patterns on the relationship between maternal education and physical aggression CI confidence interval
X independent variable Mi mediators Cov covariates
We found that high intakes of HFSS foods are posi-tively associated with physical aggression. This result is consistent with other studies which emphasized problem behaviors, such as attention deficit hyperactivity dis-order, depressive symptoms, and autism [13, 14, 34, 38,
39]. In addition, a previous study which investigated the one-by-one associations between various junk foods and violent behaviors also found a positive association be-tween daily consumption of salty snacks and children’s physical fighting [34]. Intriguingly, compared to healthy foods, our result indicates that HFSS foods affect pre-schooler’s physical aggression to a greater extent. The mechanism between unhealthy dietary pattern and phys-ical aggression might be the imbalanced intake of nutri-ents because a diet consisting of HFSS foods usually contains insufficient nutrients related to syntheses of neurotransmitters which may affect children’s mood [10]. On the other hand, the HFSS foods, usually highly processed, might contain high levels of trans fatty acids which might lead to a higher possibility of manifesting physical aggression [40].
The quality of preschoolers’ diet can be affected by family environment, which is usually constructed by mothers [17]. In this study, we found that maternal edu-cation directly links to preschoolers’ dietary patterns. The results echoed previous literature that a higher level of maternal education increases children’s healthy eating behavior [17,20,22]. Recent empirical evidence shows that mothers with a higher level of education had a higher prob-ability of providing high-nutrient foods (e.g., cereals, dairy products, fruits, and vegetables) for their preschoolers instead of low-nutrient foods (e.g., sweetened beverages, fast foods, salty snacks, and sweets) [21,36,41]. Well-educated mothers will provide a better home food environment in many ways, including increasing the healthy food availability at home and setting food consumption roles, and this will increase children’s healthy eating behavior [20].
Indeed, maternal education level is not only related to their children’s eating behaviors but is also associated with their physical aggression [16, 42]. Mothers with a higher education level affect preschoolers’ physical ag-gression via using contemporary knowledge about par-enting to educate and discipline their children, and this will subsequently prevent and protect them from devel-oping problem behaviors [42]. For mothers with low levels of education, special attention should be paid, and the provision of some services, such as non-mother childcare services, is suggested for reducing exposure to risks in the family environment [42].
Strengths and limitations
The main strength of this study is the large national rep-resentative sample, which can reflect the phenomena of Taiwanese preschoolers. Due to the sampling strategy
used in this study, the results can be generalized to the population of preschoolers in Taiwan. The other strength is the long-term follow-up design that more clearly indicates the temporal sequence between mater-nal education and behavioral outcomes. Although this study controlled for baseline aggression and other re-lated factors including household income, parental mari-tal status, and preschoolers’ menmari-tal health to reduce the effect of possible confounding factors, there are still some other confounders that were not considered, for example, knowledge of healthy eating and parenting skills. In addition, because the dietary patterns and phys-ical aggression were measured in the same year, the re-sults cannot rule out the possibility that maternal education impacts on dietary patterns via physical ag-gression among preschoolers. Besides, the sample size for the two-week test-retest reliability for the measure-ment of aggression and measure-mental distress is relatively small, although the coefficients of the reliabilities are quite acceptable (both > 0.7). Furthermore, since 97% of children went to daycare in the day time, the informa-tion about their problem behaviors and food consump-tion while in daycare might be unknown to their mothers. Last, the study cannot exclude the possibilities that the reporters might have underreported the fre-quencies of preschoolers’ physical aggression and un-healthy dietary behaviors. Despite these limitations, this study reveals the mediating roles of preschoolers’ dietary patterns between maternal education and physical ag-gression, and sheds light on the importance of nutri-tional education for mothers with preschoolers.
Conclusions
Our findings support the proposition that dietary pat-terns as manipulable factors can mediate the association between maternal education and preschoolers’ physical aggression; however, only slightly partial mediation ef-fects were found. The pathway through a healthy dietary pattern may result in lowering the level of physical ag-gression, while the pathway through an HFSS dietary pattern may increase the level of physical aggression. Thus, it is suggested that nutritional education for poorly-educated mothers might be an effective interven-tion strategy for decreasing or preventing their
pre-schooler’s physical aggression. However, future
interventional studies may be needed to examine the protective effect of a healthy balanced diet on physical aggression, especially among preschoolers raised by poorly-educated mothers.
Abbreviations
HFSS:High-fat-sugar-salt; TBCS: Taiwan Birth Cohort Study; EFA: Exploratory Factor Analysis; SMC: Squared multiple correlations; CI: Confidence interval; SD: Standard deviation
Acknowledgements
The author gratefully acknowledges the time and continuing support of the participating families.
Authors’ contributions
W-C.W. and T-L.C. designed the studies; W-C.W. analyzed and interpreted the data as well as drafted and edited the manuscript; W-C.W. and C-I.L. revised the manuscript; Y-F.L., L-Y.C. and T-L.C. made substantial contributions to the conceptualization; T-L.C. received research grants. All authors have read and approved the manuscript.
Funding
Taiwan Birth Cohort Study was supported financially and administratively by the Health Promotion Administration, Ministry of Health and Welfare (BHPPHRC-92-4, DOH93-HP-1702, DOH94-HP-1802, DOH95-HP-1802, DOH96-HP-1702, DOH101-HP-1703, and DOH102-HP-1701). The funding source had no role in this study design, statistical analyses, data interpretation, or deci-sion to submit.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Institutional Review Board of Health Promotion Administration, Ministry of Health and Welfare (No. 0990800242). Written informed consent was obtained from all subjects/patients. Consent for publication
Not applicable. Competing interests
The authors declare that they have no competing conflicts of interest. Author details
1Department of Health Promotion and Health Education, National Taiwan
Normal University, 17 Xuzhou Road, Taipei 100, Taiwan.2Department of Nutrition and Health Sciences, Kainan University, No. 1, Kainan Road, Luzhu District, Taoyuan City 338, Taiwan.3Division of Clinical Chinese Medicine, National Research Institute of Chinese Medicine, Ministry of Health and Welfare, 11221 Room, No. 155-1, Section 2, Linong St, Beitou District, Taipei City 112, Taiwan.4Institute of Health Behaviors and Community Sciences,
School of Public Health, National Taiwan University, 17 Xuzhou Road, Taipei 100, Taiwan.5Institute of Health Policy and Management, School of Public
Health, National Taiwan University, 17 Xuzhou Road, Taipei 100, Taiwan. Received: 30 January 2020 Accepted: 5 May 2020
References
1. Tremblay RE, Nagin DS, Séguin JR, Zoccolillo M, Zelazo PD, Boivin M, Pérusse D, Japel C. Physical aggression during early childhood: trajectories and predictors. Pediatrics. 2004;114:e43–50.
2. Tremblay RE, Côté SM, Salla J, Michel G: The Development of Aggression from Early Childhood to Adulthood. In: The Wiley Handbook of Violence and Aggression. edn. Edited by Sturmey P. New Jersey: Wiley; 2017:1–12. 3. Brame B, Nagin DS, Tremblay RE. Developmental trajectories of physical
aggression from school entry to late adolescence. J Child Psychol Psychiat. 2018;42:503–12.
4. Campbell SB, Spieker S, Burchinal M, Poe MD. Trajectories of aggression from toddlerhood to age 9 predict academic and social functioning through age 12. J Child Psychol Psychiatry. 2006;47:791–800.
5. Liu J. Concept analysis: aggression. Issues in Mental Health Nursing. 2004; 25(7):693–714.
6. Fishbein D, Pease SE. Diet, nutrition, and aggression. J Offender Rehabil. 1994;21(3–4):117–44.
7. Mysterud I, Poleszynski DV. Expanding evolutionary psychology: toward a better understanding of violence and aggression. Soc Sci Inform. 2003;42(1):5–50.
8. Sinn N. Nutritional and dietary influences on attention deficit hyperactivity disorder. Nutr Rev. 2008;66(10):558–68.
9. Stevenson J. Dietary influences on cognitive development and behaviour in children. Proc Nutr Soc. 2006;65(04):361–5.
10. Wallner B. Influence of nutrition on aggression. CAB Reviews: Perspectives in Agriculture, Veterinary Science, Nutrition and Natural Resources. 2009;4(075): 1–10.
11. Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002;13(1):3–9.
12. Oddy WH, Allen KL, Trapp GSA, Ambrosini GL, Black LJ, Huang RC, Rzehak P, Runions KC, Pan F, Beilin LJ, et al. Dietary patterns, body mass index and inflammation: pathways to depression and mental health problems in adolescents. Brain Behav Immun. 2018;69:428–39.
13. Siddiqi S, Urooj A, D'Souza MJ. Dietary patterns and anthropometric measures of Indian children with autism Spectrum disorder. J Autism Dev Disord. 2019;49(4):1586–98.
14. Abbasi K, Beigrezai S, Ghiasvand R, Pourmasoumi M, Mahaki B. Dietary patterns and attention deficit hyperactivity disorder among Iranian children: a case-control study. J Am Coll Nutr. 2019;38(1):76–83.
15. Dekovic M, Janssens JMAM, Van NMC. Family predictors of antisocial behavior in adolescence. Fam Proc. 2003;42:223–35.
16. Harding JF. Increases in maternal education and low-income children's cognitive and behavioral outcomes. Dev Psychol. 2015;51(5):583–99. 17. Jackson M, Kiernan K, McLanahan S. Maternal education, changing family
circumstances, and Children's skill development in the United States and UK. Ann Am Acad Pol Soc Sci. 2017;674(1):59–84.
18. Nagin DS, Tremblay RE. Parental and early childhood predictors of persistent physical aggression in boys from kindergarten to high school. Arch Gen Psychiatry. 2001;58:389–94.
19. Cote SM, Vaillancourt T, LeBlanc JC, Nagin DS, Tremblay RE. The development of physical aggression from toddlerhood to pre-adolescence: a nation wide longitudinal study of Canadian children. J Abnorm Child Psychol. 2006;34(1):71–85.
20. van Ansem WJC, Schrijvers CTM, Rodenburg G, van de Mheen D. Maternal educational level and children’s healthy eating behaviour: role of the home food environment (cross-sectional results from the INPACT study). Int J Behavioral Nutri Physical. 2014;11(113):1–12.
21. Rashid V, Engberink MF, van Eijsden M, Nicolaou M, Dekker LH, Verhoeff AP, Weijs PJM. Ethnicity and socioeconomic status are related to dietary patterns at age 5 in the Amsterdam born children and their development (ABCD) cohort. BMC Public Health. 2018;18(1):115.
22. Lioret S, Cameron AJ, McNaughton SA, Crawford D, Spence AC, Hesketh K, Campbell KJ. Association between maternal education and diet of children at 9 months is partially explained by mothers' diet. Matern Child Nutr. 2015; 11(4):936–47.
23. Wu JC. Parental work characteristics and diet quality among pre-school children in dual-parent households: results from a population-based cohort in Taiwan. Public Health Nutr. 2018;21(6):1147–55.
24. Chen G, Chiang WL, Shu BC, Guo YL, Chiou ST, Chiang TL. Associations of caesarean delivery and the occurrence of neurodevelopmental disorders, asthma or obesity in childhood based on Taiwan birth cohort study. BMJ Open. 2017;7(9):e017086.
25. Daily Dietary Guidelines for Taiwanese [https://www.hpa.gov.tw/Pages/ EBook.aspx?nodeid=1208]. Accessed 1 Dec 2019.
26. CJ L, MS T, MD K, WT Y, WH P: Eating habits and patterns of four to twelve year-old children in Taiwan. In Reports of Nutrition and Health Survey in Taiwan (NAHSIT) 1993–1996. In: Reports of Nutrition and Health Survey in Taiwan (NAHSIT) 1993–1996. edn. Taipei: Department of Health, Executive Yuan; 1999: 115–130.
27. Lin W, Yang HC, Hang CM, Pan WH. Nutrition knowledge, attitude, and behavior of Taiwanese elementary school children. Asia Pac J Clin Nutr. 2007;16(Suppl 2):534–46.
28. Tan CS: Test Review: Reynolds, CR, & Kamphaus, RW (2004). Behavior assessment system for children . Circle Pines, MN: American Guidance Service. Assessment for Effective Intervention 2007, 32(2):121–124. 29. Piper BJ, Gray HM, Raber J, Birkett MA. Reliability and validity of brief
problem monitor, an abbreviated form of the child behavior checklist. Psychiatry Clin Neurosci. 2014;68(10):759–67.
30. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York London: The Guilford Press; 2013.
31. Ryman TK, Austin MA, Hopkins S, Philip J, O'Brien D, Thummel K, Boyer BB. Using exploratory factor analysis of food frequency questionnaires to identify dietary patterns among Yup’ik people. Public Health Nutr. 2014; 17(3):510–8.
32. Ambrosini GL, O'Sullivan TA, de Klerk NH, Mori TA, Beilin LJ, Oddy WH. Relative validity of adolescent dietary patterns: a comparison of a FFQ and 3 d food record. Br J Nutr. 2011;105(4):625–33.
33. Suhr D: Exploratory factor analysis with the world values survey. Proceedings of the SAS Global Forum 2012 Conferences 2012:22–25. 34. Zahedi H, Kelishadi R, Heshmat R, Motlagh ME, Ranjbar SH, Ardalan G, Payab
M, Chinian M, Asayesh H, Larijani B, et al. Association between junk food consumption and mental health in a national sample of Iranian children and adolescents: the CASPIAN-IV study. Nutrition. 2014;30(11):1391–7. 35. Cao S, Ma C, Hanlon A, Compher C, Zhao S, Liu J. Low blood zinc, Iron, and
other Sociodemographic factors associated with behavior problems in preschoolers. Nutrients. 2014;6:530–45.
36. Nasreddine L, Shatila H, Itani L, Hwalla N, Jomaa L, Naja F. A traditional dietary pattern is associated with lower odds of overweight and obesity among preschool children in Lebanon: a cross-sectional study. Eur J Nutr. 2019;58(1):91–102.
37. Zaalberg A, Nijman H, Bulten E, Stroosma L, van der Staak C. Effects of nutritional supplements on aggression, rule-breaking, and psychopathology among young adult prisoners. Aggress Behav. 2010;36(2):117–26. 38. Akbaraly TN, Brunner EJ, Ferrie JE, Marmot MG, Kivimaki M, Singh-Manoux A.
Dietary pattern and depressive symptoms in middle age. Br J Psychiatry. 2009;195(5):408–13.
39. Wu W-C, Luh D-L, Lin C-I, Chiang Y-C, Hung C-C, Wang S, Wu C-C, Hurng B-S, Chang Y-H, Yen L-L, et al. Reciprocal relationship between unhealthy eating behaviours and depressive symptoms from childhood to adolescence: 10-year follow-up of the child and adolescent behaviors in long-term evolution study. Public Health Nutr. 2016;19:1654–65. 40. Golomb BA, Evans MA, White HL, Dimsdale JE. Trans fat consumption and
aggression. PLoS One. 2012;7(3):e32175.
41. Rutayisire E, Wu X, Huang K, Tao S, Chen Y, Wang S, Tao F. Dietary patterns are not associated with overweight and obesity in a sample of 8900 Chinese preschool children from four cities. J Nutr Sci. 2018;7:e24. 42. Coˆte´ SM, Boivin M, Nagin DS, Japel C, Xu Q, Zoccolillo M, Junger M,
Tremblay RE: The role of maternal education and nonmaternal care services in the prevention of children’s physical aggression problems. Arch Gen Psychiatry 2007, 64(11):1305–1312.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.