Adverse Outcomes after Major Surgery in Patients with Pressure Ulcer: A
Nationwide Population-Based Retrospective Cohort Study
Chia-Lun Chou1,2, Woan-Ruoh Lee1,2,3, Chun-Chieh Yeh43,54, Chun-Chuan Shih65, Ta-Liang Chen72,86,97†, Chien-Chang Liao2,6,7,8.9,10*†
1 Department of Dermatology, School of Medicine, College of Medicine, Taipei
Medical University, Taipei, TaiwanDepartment of Dermatology, Shuan Ho Hospital, Taipei Medical University, Taipei, Taiwan
2 Department of Dermatology, Shuang Ho Hospital, Taipei Medical University, New
Taipei City, Taiwan
3 Graduate Institute of Medical Sciences, Taipei Medical University, Taipei,
TaiwanSchool of Medicine, Taipei Medical University, Taipei, Taiwan
43 Department of Surgery, China Medical University Hospital, Taichung, Taiwan
54 Department of Surgery, University of Illinois, Chicago, USA
65 School of Chinese Medicine for Post-Baccalaureate, I-Shou University, Kaohsiung, Taiwan
76 Department of Anesthesiology, Taipei Medical University Hospital, Taipei, Taiwan
87 Health Policy Research Center, Taipei Medical University Hospital
1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Medical University, Taipei, Taiwan
108 School of Chinese Medicine, China Medical University, Taichung, Taiwan †These authors contributed equally to this work.
*Corresponding author Chien-Chang Liao, PhD, MPH Assistant Professor
Department of Anesthesiology Taipei Medical University Hospital 252 Wuxing Street
Taipei 11031 Taiwan
E-mail: [email protected]; [email protected] Abstract: 227 words; Text: 2539 words; Tables: 4; References: 40
Keywords: pressure ulcer, surgery, postoperative complications, mortality
List of abbreviations: CI, confidence interval; ICD-9-CM, International
Classification of Diseases, 9th Revision, Clinical Modification; ICU, intensive care unit; RR, relative risk.
Source of funding: This study was supported in part by a grant from the National
Science Council, Taiwan (NSC102-2314-B-038-021-MY3).
Competing Interests: The authors have declared that no competing interests exist. 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39
Category: Original article
Running head: Pressure ulcer and surgical outcomes
Contributors: All authors contributed substantially toward the design of the study,
the analysis and interpretation of the data, and drafting the manuscript. All authors approved the final version. Prof. Chen is the guarantor and has full access of the data. 40
41 42 43 44
Abstract
Background: Postoperative adverse outcomes in patients with pressure ulcer are not
completely understood. This study evaluated the association between preoperative pressure ulcer and adverse events after major surgeries.
Methods: Using reimbursement claims from Taiwan’s National Health Insurance
Research Database, we conducted a nationwide retrospective cohort study of 17391 patients with preoperative pressure ulcer receiving major surgery in 2008-2010. With propensity score matching procedure, 17391 surgical patients without pressure ulcer were selected for comparison. Eight major surgical postoperative complications and 30-day postoperative mortality were evaluated among patients with pressure ulcer of varying severity.
Results: Patients with preoperative pressure ulcer had significantly higher risk than
control for postoperative adverse outcomes, including septicemia, pneumonia, stroke, urinary tract infection, and acute renal failure. Surgical patients with pressure ulcer had approximately 1.83-fold risk (95% confidence interval 1.54-2.18) of 30-day postoperative mortality compared with control group. The most significant postoperative mortality was found in those with serious pressure ulcer, such as 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61
pressure ulcer with local infection, cellulitis, wound or treatment by change dressing, hospitalized care, debridement or antibiotics. Prolonged hospital or intensive care unit stay and increased medical expenditures were also associated with preoperative pressure ulcer.
Conclusion: This nationwide propensity score-matched retrospective cohort study
showed increased postoperative complications and mortality in patients with preoperative pressure ulcer. Our findings suggest the urgency of preventing and managing preoperative pressure ulcer by a multidisciplinary medical team for this specific population. 62 63 64 65 66 67 68 69 70
Introduction
Pressure ulcer remains a significant problem commonly found in disabled patients who need long-term care. It was estimated by researchers in 2003 and 2013 that between 1.3 and 3 million adults had pressure ulcer in the United States [1,2]. Hospital stays increased nearly 80% between 1993 and 2006 among patients with pressure ulcers, resulting in a remarkable increase in the annual financial burden of the disease [2,3].
Limited mobility due to spinal cord injury, cerebrovascular accident or hip fracture was an important contributing factor in pressure ulcer [4,5]. Diabetes, congestive heart failure, renal dysfunction, chronic obstructive pulmonary disease, progressive neurologic disorder, malnutrition and aging skin were also considered as medical comorbidities associated with pressure ulcer [4,5]. The influences of extrinsic
pressure, friction, shear stress and excessive moisture contribute to tissue hypoxia and poor wound healing followed by tissue necrosis [5]. Pressure ulcers may lead to patient distress, poor quality of life and recurrent severe infection; these often increase hospital stay length [3,6], mortality rates [7], and need for long-term health care [3]. Appropriate clinical intervention is recommended for patients receiving surgery with 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87
high risk of developing pressure ulcer [8-12]. However, whether preoperative pressure ulcer is associated with postoperative adverse outcomes was still unclear.
In this nationwide population-based cohort study, we used Taiwan’s National Health Insurance Research Database to validate postoperative complications and mortality in patients with preoperative pressure ulcers undergoing major surgeries. The impact of various severities of pressure ulcers on surgical adverse events was also analyzed. 88 89 90 91 92 93
Methods
Source of data
Research data were obtained from reimbursement claims of the Taiwan National Health Insurance Program, which was implemented in March 1995 and covers more than 99% of the 22.6 million Taiwan residents. The National Health Research Institutes established the
National Health Insurance Research Database that records all beneficiaries’ medical services, including inpatient and outpatient demographics, primary and secondary diagnoses,
procedures, prescriptions and medical expenditures for public research interest. The validity of this database has been favorably evaluated, and research articles based on it have been accepted in prominent scientific journals worldwide [13-16].
Ethical approval
Insurance reimbursement claims used in this study were from Taiwan’s National Health Insurance Research Database, which is available for public access. This study was conducted in accordance with the Helsinki Declaration. To protect personal privacy, the electronic database was decoded with patient identifications scrambled for further public access for research. According to National Health Research Institutes regulations, informed consent is not required because of the use of decoded and scrambled patient identifications. However, this study was evaluated and approved by Taiwan’s National Health Research Institutes (NHIRD-103-121). The data are owned by the National Health Insurance Research Database 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112
Committee [13-16] and the contact information is available as email: [email protected].
Study Design
We examined medical claims and identified 17391 patients aged ≥20 years with
preoperative pressure ulcer from 1,499,745 patients who underwent major inpatient surgeries between 2008 and 2010 in Taiwan. These surgeries required general, epidural or spinal anesthesia and hospitalization for more than one day. To identify patients with pressure ulcer, the present study required at least one visit for outpatient or inpatient medical services for a diagnosis of pressure ulcer within the 24-month preoperative period. We matched each surgical patient with pressure ulcer with a randomly selected surgical patient without pressure ulcer by sex, age, type of surgery, type of anesthesia, coexisting medical conditions, operation in teaching hospital or not, and low income or not, and conducted the analysis with a
propensity score-matched pair procedure.
Measures and definition
We identified income status by defining low-income patients as those qualifying for waived medical copayment, because this status is verified by the Bureau of National Health
Insurance. Whether the surgery was performed in a teaching hospital and the types of surgery and anesthesia were also recorded. We used the International Classification of Diseases,
Ninth Revision, Clinical Modification (ICD-9-CM) to define preoperative medical diseases
and postoperative complications. Preoperative pressure ulcer (ICD-9-CM 707.0) was defined 113 114 115 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131
as the major exposure. Pre-existing medical conditions that were determined from medical claims for the 24-month preoperative period included hypertension (ICD-9-CM 401-405), mental disorders (ICD-9-CM 290-319), diabetes (ICD-9-CM 250), chronic obstructive
pulmonary disease (ICD-9-CM 490-496), stroke (ICD-9-CM 430-438), ischemic heart disease (ICD-9-CM 410-414), congestive heart failure (ICD-9-CM 428), liver cirrhosis (ICD-9-CM 571), hyperlipidemia (ICD-9-CM 272.0, 272.1, and 272.2), spinal cord injury (ICD-9-CM 806), hip fracture (ICD-9-CM 820), and peripheral vascular disease (ICD-9-CM 443). Renal dialysis was defined by administration code (D8, D9). In-hospital 30-day mortality after the index surgery was considered the study’s primary outcome. Eight major surgical
postoperative complications were noted, including septicemia (ICD-9-CM 038, 998.5), pneumonia 9-CM 480-486), stroke 9-CM 430-438), urinary tract infection (ICD-9-CM 599.0), acute renal failure (ICD-(ICD-9-CM 584), deep wound infection (ICD-(ICD-9-CM 958.3), pulmonary embolism (ICD-9-CM 415), postoperative bleeding (ICD-9-CM 998.0, 998.1 and 998.2) and acute myocardial infarction (ICD-9-CM 410) after the index surgery [15,16]. Admission to intensive care unit, prolonged length of stay, and increased medical expenditure after index surgery were analyzed as secondary outcomes. To investigate the severity of pressure ulcer on 30-day postoperative mortality, we identified some characteristics in
patients with pressure ulcer: debridement (administration code F48001C, F48002C, F48003C, F48004C, F48006C, F48006C), local infection (ICD-9-CM 686) and cellulitis (ICD-9-CM 132 133 134 135 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150
681, 682). The use of first-line (amoxicillin, ampicillin, amoxicillin/clavulanic acid, baktar, cefazolin, gentamicin, oxacillin, unasyn) or second-line (clindamycin, linezolid, meropenem, teicoplanin, tigecycline, vancomycin) antibiotics for treating pressure ulcer and related illness within 24 months preoperatively were considered in this study. The cumulative use (i.e. the total quantity) of such antibiotics was categorized into quartiles. The cumulative medical expenditure on antibiotics was also categorized as low (lowest quartile), moderate (second quartile), and high (third quartile and highest quartile).
Statistical analysis
To reduce confounding errors [16], this study used a propensity score-matched pair
procedure to balance the covariates between surgical patients with and without pressure ulcer. We developed a nonparsimonious multivariable logistic regression model to estimate a propensity score for preoperative renal dialysis. Clinical significance guided the initial choice of covariates in this model: sex, age, types of surgery, types of anesthesia, operation in a teaching hospital or not, low-income status, hypertension, mental disorders, diabetes, chronic obstructive pulmonary disease, stroke, ischemic heart disease, congestive heart failure, liver cirrhosis, hyperlipidemia, renal dialysis, and peripheral vascular disease. A structured iterative approach was used to refine this model, with the goal of achieving covariate balance within the matched pairs. We used chi-square tests to measure covariate balance, and p < 0.05 was suggested to represent meaningful covariate imbalance. We matched patients with pressure 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 169
ulcer to non-pressure ulcer patients using a greedy-matching algorithm with a caliper width of 0.2 SD of the log odds of the estimated propensity score. This method could remove 98% of the bias from measured covariates [16].
Adjusted rate ratios (RRs) with 95% confidence intervals (CIs) for 30-day postoperative complications and mortality between patients with and without pressure ulcer were analyzed with multivariate Poisson regression models by controlling for sex, age, low-income status, operation in a teaching hospital or not, coexisting medical conditions, and types of surgery and anesthesia. We also performed stratification analysis in age, sex and coexisting medical conditions for the association between preoperative pressure ulcer and postoperative
mortality. The multivariate Poisson regression analyses were applied to investigate 30-day postoperative mortality associated with severity of pressure ulcer after controlling for sex, age, low-income status, operation in a teaching hospital or not, preoperative coexisting medical conditions, and types of surgery and anesthesia. SAS version 9.1 (SAS Institute Inc., Cary, NC, USA) statistical software was used for data analyses; two-sided p < 0.05 indicated significant differences. 170 171 172 173 174 175 176 177 178 179 180 181 182 183 184
Results
Table 1 shows demographic characteristics of patients with and without preoperative pressure ulcer who underwent major surgeries. After propensity score matching, there were no significant differences in perioperative characteristics between surgical patients with and without pressure ulcer, including sex, age, types of surgery and anesthesia, operation in a teaching hospital or not, low-income status, hypertension, mental disorders, diabetes, chronic obstructive pulmonary disease, stroke, ischemic heart disease, congestive heart failure, liver cirrhosis, hyperlipidemia, renal dialysis and peripheral vascular disease.
Compared with patients without pressure ulcer (Table 2), patients with pressure ulcer showed higher risks of postoperative complications, including pneumonia (RR 2.94, 95% CI 2.76-3.13), septicemia (RR 2.85, 95% CI 2.68-3.04), stroke (RR 2.02, 95% CI 1.88-2.17), urinary tract infection (RR 2.05, 95% CI 1.90-2.20), acute renal failure (RR 2.17, 95% CI 1.91-2.47), acute myocardial infarction (RR 1.45, 95% CI 1.12-1.87), and overall
complications (RR 2.13, 95% CI 2.06-2.21). Preoperative pressure ulcer was associated with a significant increase in 30-day postoperative mortality (RR 1.83, 95% CI 1.54-2.18).
Admission to ICU, prolonged length of hospital stay, and increased medical expenditures were all significantly associated with preoperative pressure ulcer, with respective RRs of 1.64 (95% CI 1.57-1.70), 2.73 (95% CI 2.58-2.88), and 2.03 (95% CI 1.94-2.14). 185 186 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201 202
pressure ulcer and postoperative mortality was more significant in women (RR 1.87, 95% CI 1.43-2.46) than in men (RR 1.81, 95% CI 1.44-2.26). Surgical patients aged 70-79 years with pressure ulcer had the highest postoperative mortality of all age groups (RR 2.32, 95% CI 1.68-3.20).
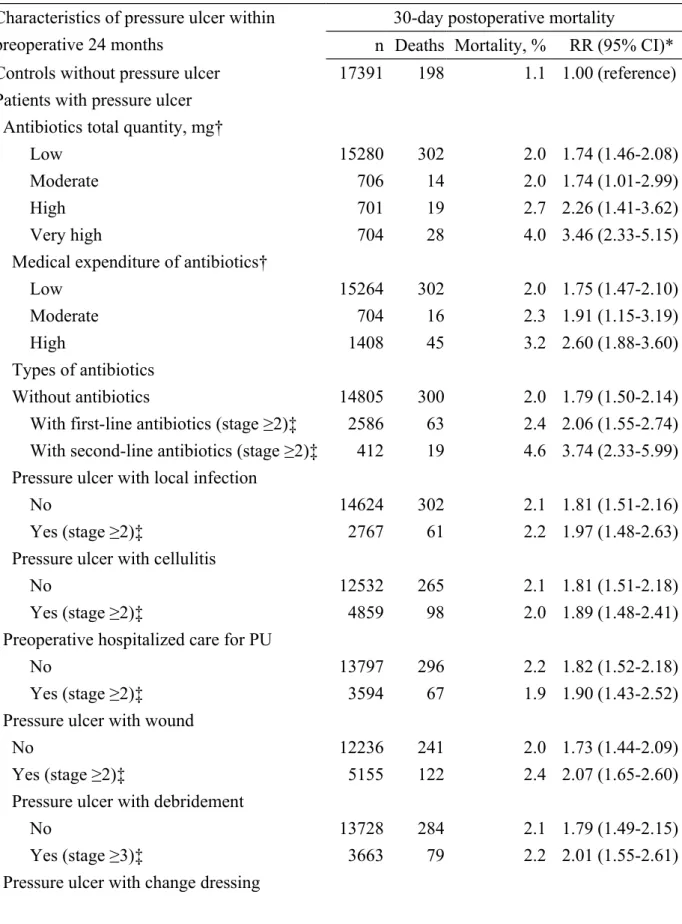
Compared with surgical patients without pressure ulcer (Table 4), patients with pressure ulcer were more likely to have significantly higher postoperative mortality with debridement (RR 2.01, 95% CI 1.55-2.61), cellulitis (RR 1.89, 95% CI 1.48-2.41), wound (RR 2.07, 95% CI 1.65-2.60), and treatment by change dressing (RR 1.90, 95% CI 1.59-2.28), hospitalized care (RR 1.90, 95% CI 1.43-2.52), and antibiotics (with first-line antibiotics, RR 2.06, 95% CI 1.55-2.74; with second-line antibiotics, RR 3.74, 95% CI 2.33-5.99). The significant 30-day postoperative mortality compared with surgical patients without pressure ulcer was found in patients who had pressure ulcer with high total quantity of antibiotics (RR 3.46, 95% CI 2.33-5.15) and high medical expenditure on antibiotics (RR 2.60, 95% CI 1.88-3.60). Preoperative moderate-to-severe pressure ulcer was also associated with increased 30-day mortality after surgery (RR 1.92, 95% CI 1.61-2.29).
204 205 206 207 208 209 210 211 212 213 214 215 216 217 218
Discussion
This nationwide population-based, propensity score-matched cohort study showed that patients with preoperative pressure ulcer had increased risk of postoperative 30-day in-hospital mortality and complications such as septicemia, pneumonia, stroke, urinary tract infection and acute renal failure. Patients with pressure ulcer receiving debridement, or having local infection, cellulitis or treatment with antibiotics had significantly higher 30-day
postoperative mortality. Postoperative admission to intensive care unit, prolonged length of hospital stay and increased medical expenditures were also associated with preoperative pressure ulcer. To our knowledge, this investigation is the first study investigating adverse events after surgery in patients with preoperative pressure ulcer.
Although the association between preoperative pressure ulcer and postoperative adverse outcomes was still unclear, previous studies had identified factors associated with
postoperative pressure ulcer such as old age, types of surgeries and coexisting medical
conditions [17,18]. These factors were also associated with major adverse events after surgery [14-16,19-25]. To reduce the confounding errors, we adjusted these covariates using
propensity score-matched procedure and then controlled these factors in the multivariate Poisson regression models. In the present study, preoperative pressure ulcer was associated with postoperative mortality in both sexes and all age groups, confirming the association 219 220 221 222 223 224 225 226 227 228 229 230 231 232 233 234 235 236
The National Pressure Ulcer Advisory Panel had proposed a classification system to grade pressure ulcer from stage I to stage IV according to the integrity of epidermis and the involved depth of wound [26]. As skin defects provide entrances for bacteria to colonize, invade and infect the underlying tissues, local or systemic infection is the most prevalent complication of pressure ulcers presenting open wounds (stage II-IV), and debridement is indicated for such infected necrotic tissues [27]. As a result, coexisting local infection of skin implied more advanced pressure ulcer, as did performance of debridement, abscess and cellulitis, particularly in those using second-line antibiotics and with higher total quantities of antibiotics and higher expenditures on antibiotics. Our study found that such advanced
pressure ulcers were associated with significantly higher postoperative mortality.
Some possible explanations may clarify the association between preoperative pressure ulcer and postoperative adverse outcomes. First, the major predisposing factor of pressure ulcer is immobilization, which may result from stroke, spinal cord injury, progressive neurologic disorders or hip fracture. Immobilization also impairs the ability to clear bronchial secretions, and can eventually result in atelectasis and hypostatic pneumonia [28]. Second, pressure ulcer is one of causes several complications, including localized abscess, cellulitis, bacteremia, sepsis, osteomyelitis, fistula and carcinoma [27]. Among these complications, infection resulting from polymicrobial organism is the most prevalent; such infection can be life-threatening when complicated by bacteremia, sepsis, endocarditis and meningitis [27,29-31]. 238 239 240 241 242 243 244 245 246 247 248 249 250 251 252 253 254 255 256
Infected pressure ulcers have been independently associated with bloodstream infection as well as with higher 30-day mortality in hospitalized patients [32]. Third, chronic pressure ulcer features persistent chronic inflammation with leukocyte infiltration and release of proinflammatory cytokines [33,34]. Repetitive pressure and relief also lead to cutaneous ischemia-reperfusion injury, causing infiltration of inflammatory cells, deleterious cellular reactions and tissue damage by reactive free oxygen radicals [35]. Extensive evidence shows that chronic inflammation and infection outside the brain are associated with an increased risk of ischemic stroke via endothelial cell dysfunction, impaired fibrinolysis and activation of platelet aggregability altered by immune-mediated inflammatory cells and cytokines [36-39]. These biochemical cascades in pressure ulcer lead to repetitive chronic inflammation,
endothelial cell dysfunction and microvasculature system thrombosis that may contribute to stroke and ischemic renal injury. Finally, presence of pressure ulcers may indicate inadequate services, poor nutrition or insufficient family support for the patients; these factors might indirectly contribute to poor surgical outcomes and higher mortality. Regarding nutritional deficiency in particular, fewer scavengers to remove free oxygen radicals may result in reactive vasoconstriction and increased cell damage.
Prevention of pressure ulcer is always an important issue for hospitalized patients requiring coordination among multidisciplinary medical teams. We suggest that assessment of risk of developing pressure ulcer and grading of existing pressure ulcer are essential for surgical 257 258 259 260 261 262 263 264 265 266 267 268 269 270 271 272 273 274 275
patients. Patients with serious or infected pressure ulcer must receive adequate wound dressing, debridement of necrotic tissues and early empiric antimicrobial therapy
preoperatively to reduce potential postoperative mortality. Pressure ulcer patients receiving surgery require appropriate monitoring and adequate control of coexisting medical conditions such as cardiovascular disease, diabetes mellitus and neurogenic degenerative disease. Due to the documented correlation between nutritional status and pressure ulcer [40], adequate protein, vitamins and mineral supplements should be provided for patients with pressure ulcer.
There are some limitations in this study. First of all, detailed information on patient sociodemographics, lifestyle, nutritional status, biomedical measurements, and the clinical stage and causes of pressure ulcer was not available from the National Health Insurance Research Database. However, we added some information regarding the possible stage of pressure in the tables according to previous investigations [41-45]. Second, because this study lacks detailed grading of preoperative pressure ulcer [26], we could not investigate the impact of severity of pressure ulcer on postoperative mortality. In addition, as our study used ICD-9-CM codes to define coexisting medical conditions and postoperative complications,
miscoding due to human error could not be avoided; however, the accuracy of the National Health Insurance Research Database has been accepted in numerous scientific publications [13-16,24]. Finally, possibly inadequate adjustment of confounding factors in use of 276 277 278 279 280 281 282 283 284 285 286 287 288 289 290 291 292 293 294
propensity score-matched pair technique might cause neglected bias in the study. Although we controlled for several confounders, residual confounding is always possible.
This nationwide, propensity score-matched, retrospective cohort study is the first report investigating increased adverse events after surgery in patients with preoperative pressure ulcer. We suggest that preoperative pressure ulcers may be a marker for more severely morbid patients who tolerate surgery more poorly.
Acknowledgments
This study is based in part on data obtained from the National Health Insurance Research Database provided by the Bureau of National Health Insurance of the Taiwan Department of Health and managed by the National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, the Taiwan Department of Health, or the National Health Research Institutes. 295 296 297 298 299 300 301 302 303 304 305 306
References
1. Chou R, Dana T, Bougatsos C, Blazina I, Starmer AJ, Reitel K, et al. (2013) Pressure ulcer risk assessment and prevention: a systematic comparative effectiveness review. Ann Intern Med 159: 28-38.
2. Lyder CH (2003) Pressure ulcer prevention and management. JAMA 289: 223-226. 3. Brem H, Maggi J, Nierman D, Rolnitzky L, Bell D, Rennert R, et al. (2010) High cost of
stage IV pressure ulcers. Am J Surg 200: 473-477.
4. Smith ME, Totten A, Hickam DH, Fu R, Wasson N, Rahman B, et al. (2013) Pressure ulcer treatment strategies: a systematic comparative effectiveness review. Ann Intern Med 159: 39-50.
5. Garcia AD, Thomas DR (2006) Assessment and management of chronic pressure ulcers in the elderly. Med Clin North Am 90: 925-944.
6. Graves N, Birrell F, Whitby M (2005) Effect of pressure ulcers on length of hospital stay. Infect Control Hosp Epidemiol 26: 293-297.
7. Thomas DR, Goode PS, Tarquine PH, Allman RM (1996) Hospital-acquired pressure ulcers and risk of death. J Am Geriatr Soc 44: 1435-1440.
8. Tschannen D, Bates O, Talsma A, Guo Y (2012) Patient-specific and surgical characteristics in the development of pressure ulcers. Am J Crit Care 21: 116-125.
9. Lindgren M, Unosson M, Krantz AM, Ek AC (2005) Pressure ulcer risk factors in patients 307 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325
undergoing surgery. J Adv Nurs 50: 605-612.
10. Hoshowsky VM, Schramm CA (1994) Intraoperative pressure sore prevention: an analysis of bedding materials. Res Nurs Health 17: 333-339.
11. Feuchtinger J, Halfens RJ, Dassen T (2005) Pressure ulcer risk factors in cardiac surgery: a review of the research literature. Heart Lung 34: 375-385.
12. Schoonhoven L, Defloor T, Grypdonck MH (2002) Incidence of pressure ulcers due to surgery. J Clin Nurs 11: 479-487.
13. Liao CC, Chiu WT, Yeh CC, Chang HC, Chen TL (2012) Risk and outcomes for traumatic brain injury in patients with mental disorders. J Neurol Neurosurg Psychiatry 83: 1186-1192.
14. Lin CS, Lin SY, Chang CC, Wang HH, Liao CC, Chen TLet al. (2013) Postoperative adverse outcomes after non-hepatic surgery in patients with liver cirrhosis. Br J Surg 100: 1784-1790.
15. Liao CC, Shen WW, Chang CC, Chang H, Chen TL (2013) Surgical adverse outcomes in patients with schizophrenia: a population-based study. Ann Surg 257: 433-438.
16. Yeh CC, Liao CC, Chang YC, Jeng LB, Yang HR, Shih CC, et al. (2013) Adverse outcomes after noncardiac surgery in patients with diabetes: a nationwide population-based retrospective cohort study. Diabetes Care 36: 3216-3221.
17. Frankel H, Sperry J, Kaplan L (2007) Risk factors for pressure ulcer development in a best practice surgical intensive care unit. Am Surg 73: 1215-1217.
326 327 328 329 330 331 332 333 334 335 336 337 338 339 340 341 342 343 344 345
18. Lardenoye JW, Thiéfaine JA, Breslau PJ (2009) Assessment of incidence, cause and consequences of pressure ulcers to evaluate quality of provided care. Dermatol Surg 35: 1797-1803.
19. Mashour GA, Shanks AM, Kheterpal S (2011) Perioperative stroke and associated mortality after noncardiac, nonneurologic surgery. Anesthesiology 114: 1289-1296. 20. Bower WF, Jin L, Underwood MJ, Lee JF, Lee KF, Lam YH, et al. (2010) Overt diabetes
mellitus adversely affects surgical outcomes of noncardiovascular patients. Surgery 147: 670-675.
21. Marchant MH Jr, Viens NA, Cook C, Vail TP, Bolognesi MP (2009) The impact of glycemic control and diabetes mellitus on perioperative outcomes after total joint arthroplasty. J Bone Joint Surg Am 91: 1621-1629.
22. Khuri SF, Henderson WG, DePalma RG, Mosca C, Healey NA, Kumbhani DJ, et al. (2005) Participants in the VA National Surgical Quality Improvement Program. Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann Surg 242: 326-341.
23. Sabaté S, Mases A, Guilera N, Canet J, Castillo J, Orrego C, et al. (2011) Incidence and predictors of major perioperative adverse cardiac and cerebrovascular events in non-cardiac surgery. Br J Anaesth 107: 879-890.
24. Liao CC, Lin CS, Shih CC, Yeh CC, Chang YC, Lee YW, et al. (2014) Increased risk of fracture and postfracture adverse events in patients with diabetes: two nationwide 346 347 348 349 350 351 352 353 354 355 356 357 358 359 360 361 362 363 364 365
population-based retrospective cohort studies. Diabetes Care 37: 2246-2252. 25. Daley J, Khuri SF, Henderson W, Hur K, Gibbs JO, Barbour G, et al. (1997) Risk
adjustment of the postoperative morbidity rate for the comparative assessment of the quality of surgical care: results of the National Veterans Affairs Surgical Risk Study. J Am Coll Surg 185: 328-340.
26. National Pressure Ulcer Advisory Panel (1989) Pressure ulcers prevalence, cost and risk assessment: consensus development conference statement. Decubitus 2: 24-28.
27. Kanj LF, Wilking SV, Phillips TJ (1998) Pressure ulcers. J Am Acad Dermatol 38: 517-536.
28. Teasell R, Dittmer DK (1993) Complications of immobilization and bed rest. Part 2: other complications. Can Fam Physician 39: 1440-1442.
29. Brooke OG, Ford PM, Mackintosh A (1970) Recurrent meningitis. Br Med J 4: 218-219. 30. Sugarman B, Brown D, Musher D (1982) Fever and infection in spinal cord injury
patients. JAMA 248: 66-70.
31. Bryan CS, Dew CE, Reynolds KL (1983) Bacteremia associated with decubitus ulcers. Arch Intern Med 143: 2093-2095.
32. Braga IA, Pirett CC, Ribas RM, Gontijo Filho PP, Diogo Filho Aet al. (2013) Bacterial colonization of pressure ulcers: assessment of risk for bloodstream infection and impact on patient outcomes. J Hosp Infect 83: 314-320.
33. Bronneberg D, Spiekstra SW, Cornelissen LH, Oomens CW, Gibbs S, Baaijens FP, et al. 366 367 368 369 370 371 372 373 374 375 376 377 378 379 380 381 382 383 384 385
(2007) Cytokine and chemokine release upon prolonged mechanical loading of the epidermis. Exp Dermatol 16: 567-573.
34. Tarnuzzer RW, Schultz GS (1996) Biochemical analysis of acute and chronic wound environments. Wound Repair Regen 4: 321-325.
35. Saito Y, Hasegawa M, Fujimoto M, Matsushita T, Horikawa M, Takenaka M, et al. (2008) The loss of MCP-1 attenuates cutaneous ischemia-reperfusion injury in a mouse model of pressure ulcer. J Invest Dermatol 128: 1838-1351.
36. Libby P (2002) Inflammation in atherosclerosis. Nature 420: 868-874.
37. Ross R (1999) Atherosclerosis: an inflammatory disease. N Engl J Med 340: 115-126. 38. Lindsberg PJ, Grau AJ (2003) Inflammation and infections as risk factors for ischemic
stroke. Stroke 34: 2518-2532.
39. Mattila KJ, Valtonen VV, Nieminen MS, Asikainen S (1998) Role of infection as a risk factor for atherosclerosis, myocardial infarction, and stroke. Clin Infect Dis 26: 719-734. 40. Hanan K, Scheele L (1991) Albumin vs. weight as a predictor of nutritional status and
pressure ulcer development. Ostomy Wound Manage 33: 22-27.
41. Health Quality Ontario (2009) Management of chronic pressure ulcers: an evidence-based analysis. Ont Health Technol Assess Ser 9:1-203.
42. Woolsey RM1, McGarry JD (1991) The cause, prevention, and treatment of pressure sores. Neurol Clin 9:797-808.
43. Bergstrom N, Horn SD, Smout RJ, Bender SA, Ferguson ML, Taler G, et al. (2005) The 386 387 388 389 390 391 392 393 394 395 396 397 398 399 400 401 402 403 404 405
National Pressure Ulcer Long-Term Care Study: outcomes of pressure ulcer treatments in long-term care. J Am Geriatr Soc 53:1721-1729.
44. Cushing CA, Phillips LG (2013) Evidence-based medicine: pressure sores. Plast Reconstr Surg 132:1720-1732.
45. Khor HM, Tan J, Saedon NI, Kamaruzzaman SB, Chin AV, Poi PJ, et al. (2014)
Determinants of mortality among older adults with pressure ulcers. Arch Gerontol Geriatr 59:536-541. 406 407 408 409 410 411 412
Table 1. Characteristics of surgical patients with or without pressure ulcer* Table 1. Characteristics of surgical patients with or without pressure ulcer*
No PU (N=17391) PU (N=17391) n (%) n (%) P Age, years 1.00 20-29 397 (2.3) 397 (2.3) 30-39 541 (3.1) 541 (3.1) 40-49 883 (5.1) 883 (5.1) 50-59 1515 (8.7) 1515 (8.7) 60-69 2454 (14.1) 2454 (14.1) 70-79 5845 (33.6) 5845 (33.6) 80-89 5041 (29.0) 5041 (29.0) ≥90 715 (4.1) 715 (4.1) Sex 1.00 Female 7987 (45.9) 7987 (45.9) Male 9404 (54.1) 9404 (54.1) Low income 1100 (6.3) 1100 (6.3) 1.00 Urbanization 1.00 Low 5369 (30.9) 5369 (30.9) Moderate 4312 (24.8) 4312 (24.8) High 4326 (24.9) 4326 (24.9) Very high 3384 (19.5) 3384 (19.5)
Operation in teaching hospital 15780 (90.7) 15780 (90.7) 1.00
Type of surgery 1.00 Skin 1854 (10.7) 1854 (10.7) Breast 49 (0.3) 49 (0.3) Musculoskeletal 7856 (45.2) 7856 (45.2) Respiratory 775 (4.5) 775 (4.5) Cardiovascular 927 (5.3) 927 (5.3) Digestive 2381 (13.7) 2381 (13.7)
Kidney, ureter, bladder 1278 (7.4) 1278 (7.4)
Delivery, CS, abortion 50 (0.3) 50 (0.3) Neurosurgery 1679 (9.7) 1679 (9.7) Eye 78 (0.5) 78 (0.5) Others 464 (2.7) 464 (2.7) Type of anesthesia 1.00 General 12085 (69.5) 12085 (69.5) 413
Epidural or spinal 5306 (30.5) 5306 (30.5) Coexisting medical conditions
Hypertension 5924 (34.1) 5924 (34.1) 1.00 Mental disorders 5119 (29.4) 5119 (29.4) 1.00 Diabetes 4990 (28.7) 4990 (28.7) 1.00 COPD 3660 (21.1) 3660 (21.1) 1.00 Stroke 2856 (16.4) 2856 (16.4) 1.00 Hip fracture 2104 (12.1) 2104 (12.1) 1.00
Ischemic heart disease 1929 (11.1) 1929 (11.1) 1.00
Congestive heart failure 658 (3.8) 658 (3.8) 1.00
Renal dialysis 526 (3.0) 526 (3.0) 1.00
Spinal cord injury 340 (2.0) 340 (2.0) 1.00
Hyperlipidemia 307 (1.8) 307 (1.8) 1.00
Liver cirrhosis 269 (1.6) 269 (1.6) 1.00
Peripheral vascular disease 123 (0.7) 123 (0.7) 1.00 CS, caesarian section; COPD, chronic obstructive pulmonary disease; PU, pressure ulcer.
*Surgical patients with and without decubitus ulcer were matched with propensity score by age, sex, low income, urbanization, operation in teaching hospital, type of surgery, type of anesthesia and coexisting medical conditions.
CS, caesarian section; COPD, chronic obstructive pulmonary disease; PU, pressure ulcer. *Surgical patients with and without decubitus ulcer were matched with propensity score by age, sex, low income, urbanization, operation in teaching hospital, type of surgery, type of anesthesia and coexisting medical conditions.
414 415 416 417
Table 2. Adverse events after surgeries in patients with preoperative pressure ulcer Table 2. Adverse events after surgeries in patients with preoperative pressure ulcer
No PU, % PU, % RR (95% CI)*
Postoperative complications
Pneumonia 7.4 21.8 2.94 (2.76-3.13)
Septicemia 7.4 21.1 2.85 (2.68-3.04)
Stroke 6.6 13.3 2.02 (1.88-2.17)
Urinary tract infection 6.3 12.9 2.05 (1.90-2.20)
Acute renal failure 2.0 4.3 2.17 (1.91-2.47)
Deep wound infection 0.9 1.1 1.21 (0.98-1.50)
Acute myocardial infarction 0.6 0.8 1.45 (1.12-1.87)
Postoperative bleeding 0.5 0.5 0.89 (0.67-1.20)
Pulmonary embolism 0.2 0.2 1.04 (0.61-1.78)
Any of the above 23.4 50.0 2.13 (2.06-2.21)
30-day in-hospital mortality 1.1 2.1 1.83 (1.54-2.18)
ICU stay 22.4 36.7 1.64 (1.57-1.70)
Prolonged length of hospital stay 10.3 28.1 2.73 (2.58-2.88) Increased medical expenditure 13.2 26.8 2.03 (1.94-2.14) CI, confidence interval; PU, pressure ulcer; ICU, intensive care unit; RR, rate ratio. *Adjusted for age, sex, low income, urbanization, operation in teaching hospital, types of anesthesia, types of surgery and coexisting diseases.
CI, confidence interval; PU, pressure ulcer; ICU, intensive care unit; RR, rate ratio. *Adjusted for age, sex, low income, urbanization, operation in teaching hospital, types of anesthesia, types of surgery and coexisting diseases.
418
419 420 421
Table 3. Stratification analysis by age, sex and coexisting medical conditions regarding
association between preoperative pressure ulcer and postoperative mortality
Table 3. Stratification analysis by age, sex and coexisting medical conditions
regarding association between preoperative pressure ulcer and postoperative mortality 30-day postoperative mortality n Deaths Mortality, % RR (95% CI)* Sex Female 15974 227 1.4 1.87 (1.43-2.46) Male 18808 334 1.8 1.81 (1.44-2.26) Age, years 20-59 6672 68 1.0 1.62 (0.99-2.63) 60-69 4908 56 1.1 2.29 (1.30-4.06) 70-79 11690 176 1.5 2.32 (1.68-3.20) ≥80 11512 261 2.3 1.56 (1.22-2.00)
CI, confidence interval; RR, rate ratio.
*The rate ratio of postoperative mortality associated with pressure with multivariate adjustment.
CI, confidence interval; RR, rate ratio.
*The rate ratio of postoperative mortality associated with pressure with multivariate adjustment. 422 423 424 425 426 427
Table 4. Risk of 30-day postoperative in-hospital mortality associated with preoperative
characteristics of pressure ulcer
Table 4. Risk of 30-day postoperative in-hospital mortality associated with preoperative
characteristics of pressure ulcer
Characteristics of pressure ulcer within preoperative 24 months
30-day postoperative mortality
n Deaths Mortality, % RR (95% CI)* Controls without pressure ulcer 17391 198 1.1 1.00 (reference) Patients with pressure ulcer
Antibiotics total quantity, mg†
Low 15280 302 2.0 1.74 (1.46-2.08)
Moderate 706 14 2.0 1.74 (1.01-2.99)
High 701 19 2.7 2.26 (1.41-3.62)
Very high 704 28 4.0 3.46 (2.33-5.15)
Medical expenditure of antibiotics†
Low 15264 302 2.0 1.75 (1.47-2.10)
Moderate 704 16 2.3 1.91 (1.15-3.19)
High 1408 45 3.2 2.60 (1.88-3.60)
Types of antibiotics
Without antibiotics 14805 300 2.0 1.79 (1.50-2.14)
With first-line antibiotics (stage ≥2)‡ 2586 63 2.4 2.06 (1.55-2.74) With second-line antibiotics (stage ≥2)‡ 412 19 4.6 3.74 (2.33-5.99) Pressure ulcer with local infection
No 14624 302 2.1 1.81 (1.51-2.16)
Yes (stage ≥2)‡ 2767 61 2.2 1.97 (1.48-2.63)
Pressure ulcer with cellulitis
No 12532 265 2.1 1.81 (1.51-2.18)
Yes (stage ≥2)‡ 4859 98 2.0 1.89 (1.48-2.41)
Preoperative hospitalized care for PU
No 13797 296 2.2 1.82 (1.52-2.18)
Yes (stage ≥2)‡ 3594 67 1.9 1.90 (1.43-2.52)
Pressure ulcer with wound
No 12236 241 2.0 1.73 (1.44-2.09)
Yes (stage ≥2)‡ 5155 122 2.4 2.07 (1.65-2.60)
Pressure ulcer with debridement
No 13728 284 2.1 1.79 (1.49-2.15)
Yes (stage ≥3)‡ 3663 79 2.2 2.01 (1.55-2.61)
Pressure ulcer with change dressing 428
No 4794 82 1.7 1.63 (1.26-2.12)
Yes (stage ≥2)‡ 12597 281 2.2 1.90 (1.59-2.28)
Moderate-to-severe pressure ulcer§
No (stage=1)‡ 2852 42 1.5 1.37 (0.98-1.91)
Yes (stage ≥2)‡ 14539 321 2.2 1.92 (1.61-2.29)
CI, confidence interval; PU, pressure ulcer; RR, rate ratio.
*Adjusted for age, sex, low income, urbanization, coexisting medical conditions, operation in teaching hospital, types of anesthesia and types of surgery.
†Antibiotics total quantity was categorized into low (non-antibiotics users and lowest quartile), moderate (second quartile), high (third quartile), and very high (highest quartile). Medical expenditure of antibiotics was categorized into low (non-antibiotics users and lowest quartile), moderate (second quartile), and high (third quartile and highest quartile)
‡Based on the criteria of The National Pressure Ulcer Advisory Panel, the stage of pressure ulcer was categorised by clinical physicians in Taiwan and previous investigations.
§Patients with pressure have at least one of characteristics, such as debridement, local infection, cellulitis, wound, change dressing, use of antibiotics, and hospitalized care. CI, confidence interval; PU, pressure ulcer; RR, rate ratio.
*Adjusted for age, sex, low income, urbanization, coexisting medical conditions, operation in teaching hospital, types of anesthesia and types of surgery.
†Antibiotics total quantity was categorized into low (non-antibiotics users and lowest quartile), moderate (second quartile), high (third quartile), and very high (highest quartile). Medical expenditure of antibiotics was categorized into low (non-antibiotics users and lowest quartile), moderate (second quartile), and high (third quartile and highest quartile)
‡Based on the criteria of The National Pressure Ulcer Advisory Panel, the stage of pressure ulcer was categorised by clinical physicians in Taiwan and previous investigations.
§Patients with pressure have at least one of characteristics, such as debridement, local infection, cellulitis, wound, change dressing, use of antibiotics, and hospitalized care. 430 431 432 433 434 435 436 437 438 439 440