A Clinical Notes Implementing System Based on Services-Oriented Architecture
Chia-Hsien Wen
a*, Szu-Yen Wang
a, Kuan-Ching Li
ba
Department of Computer Science and Information Management, Providence University, Taiwan
b
Department of Computer Science and Information Engineering, Providence University, Taiwan * Correspondence: Chia-Hsien Wen, chwen@pu.edu.tw
摘要 本篇論文旨在開發一套「標準化臨床紀錄網基製 作平台」。此系統建構在服務導向架構(SOA)之上, 提供三大功能:臨床紀錄樣式編輯器、臨床紀錄內容 編輯器與臨床紀錄產生器,各臨床單位藉由臨床紀錄 樣式編輯器設計臨床紀錄樣式;臨床醫師透過臨床紀 錄內容編輯器輸入病歷資料;臨床紀錄產生器提供閱 覽或列印臨床病歷紀錄。本平台以服務導向架構概念 建置臨床紀錄製作平台資訊系統,讓系統的「功能」 提升為「服務」,不僅縮短開發時間,還能快速適應 作業流程及環境變化節省醫院的成本。所建置的臨床 資料元件庫符合 HL7 CDA R2 及 TMT 3.0 等標準的要 求,臨床單位可根據其需求,自行客製化具有結構化 資料內容的病歷紀錄樣式,有效縮短臨床紀錄系統建 置及修改所需的軟體發展人力和時間。臨床醫師輸入 的資料自動儲存於臨床病歷紀錄資料庫中,可提供日 後進行醫學研究分析,提高醫學研究的品質及效率。 關鍵字:SOA、HL7、CDA、TMT、臨床紀錄 Abstract
Conventional clinical notes are written in narrative and are hardly to be analyzed for medical researches. In this paper, a web-based clinical notes implementing system based on Service-Oriented Architecture is presented. The system provides three major functions, namely template designer, content editor, and notes generator. Using the template designer, user may setup the template of a clinical note simply by choosing the needed system services, which are equivalent to data modules of the clinical note, and required attributes of each service which are stemmed from HL7 CDA R2 and TMT standards. Invoking the content editor, a physician may enter structured contents of a clinical note after selecting the appropriate template. The entered structured contents will be stored in a clinical database for subsequent analysis. The notes generator is used to generate and review a formal clinical note after its contents are completely entered. The SOA-based clinical note system will greatly reduces the manpower of developing and maintaining systems of miscellaneous individually implemented clinical notes. Meanwhile, the released clinical notes, which are conformed to HL7 CDA standard, are most suitable for exchanging.
Keywords: SOA, HL7, CDA, TMT, Clinical note. 1. Introduction
In recent years, the Electronic Medical Record (EMR) has been researched and developed. Although EMR has relieved some shortcoming of paper-based
medical record, computer-based medical record systems are still improvable [1]. Their functions did not achieve to support doctor's clinical diagnosis work completely. Existing EMRs are generally developed by and used in each hospital. It is difficult to exchange the EMR among hospitals, even though there are health care information exchange standards, such HL7 (Health Level 7) [2]. HL7 has too many exceptional conditions, lack of definition, complicated coding rule, and does not have the standard glossary. To solve the problem of HL7 v2, HL7 CDA R2, which is an object-oriented approach, is researched and widely used nowadays [3].
Clinical notes, such as admission note, discharge note, progressive note, etc., are important medical records. Each of them records a patient’s health status, received examinations and treatments while he/she is hospitalized. Their contents will be analyzed for subsequent health care planning and clinical research. Transcribing clinical notes is clinician’s daily routine work. A successful EMR must satisfy with their demands to be in accordance with clinical operations.
Although some current clinical notes have been computerized, some difficulties still exist: (1) Clinical notes without conforming to standards jeopardize their exchange among hospitals, (2) Most of their contents are narrative and are hardly to be analyzed subsequently; (3) It needs a lot of manpower to develop and maintain miscellaneous individually implemented clinical notes each with versatile contents.
The SOA-based clinical notes implementing system proposed in this paper provides following advantages. The contents of implemented clinical notes conform to HL7 CDA R2 and TMT standards which allow hospitals to easily exchange these notes and contribute to improving compatibility and interoperability among a variety of medical applications and systems. Using this system, a clinical department may easily design the style sheets of all needed clinical notes. To record a patient’s clinical note, a clinician simply chooses the appropriate style sheet and enter/edit each field under system regulations. Storing the enter contents into a clinical database for each clinical note, this system extend the possibility of data usage, primarily used for patient care, also for health care planning and, for clinical research. Based on SOA, the System has properties, such as simpler software design and implementation, software reusability, and adaptability to changing business requirements [4].
2. Related work
Department of Health in Taiwan has delegate TAMI (Taiwan Association for Medical Informatics) to develop TMT basic format for electronic medical records [5][6]. Yuan established a system for transforming physical checkup data which conform to the TMT standard [7]. It helps health care professionals in making diagnoses without redundant examinations.
Raghupathi et al identified a prototype based on SOA model for the EHR in a health clinical setting [8]. The paradigm shift towards an SOA will act as the fundamental basis for developing next generation health care systems. Canforap et al asserted that each function of the legacy system should be treated as an independent black-box service to which other systems may access [9]. Wright et al implemented the SANDS (Service-oriented Architecture for NHIN (National Health Information Network) Decision Support) that allows disparate clinical information systems and clinical decision support systems to be seamlessly integrated over a network according to a set of interfaces and protocols [10].
Chen developed a web-based platform for implementing clinical notes [11]. The platform provides three functions: designing template of a clinical note, according to the template to enter contents, and save the content into a XML-based database. This web-based platform did not consider exchanging medical information under standards. Also it cannot regulate attributes of the template whether for clinical research or not.
Shih constructs a clinical information system based on SOA [12]. This system treats an OPD note into four dimensions, SOAP (Subjective, Objective, Assessment, Plan). Each of them is implemented as a service. The system also did not consider to exchange information under healthcare standards.
3. Methods
In this paper, we develop a web-based system for implementing clinical notes based on Service-Oriented Architecture. Figure 1 shows the general data of a GI admission note. It shows a GI admission note is composed of modules, such as general data, chief complaint, present illness, …, among others. A module consists of some data components, such as marital status, race, …, etc. A data component consists of some data attributes, such as single, married, …, etc. Based on SOA, the system treats each module as a service. Mapping the module to that of HL7 CDA R2 and TMT standards, we may obtain conformed data components and their data attributes.
Following steps shows how data components and their attributes are collected:
1. Refine HL7 CDA R2 message model. A CDA message is composed of header and body. The header contains the acts of the health event (ex. the provider who participated in the care, the document creator and authenticator), the organization, and the record target (ex. patient). The body contains “structure” section, for example, medical history, chief compliant, allergy history etc.
2. Refine TMT V3.0 templates. TMT currently
provides 12 clinical notes, such as discharge summary, progress note, medical encounter, face sheet, prescription, admission note, among others. This paper refines the data attribute of discharge summary and admission note. Those data components and attribute are fitted with the requirements of GI department of Taichung Veterans General Hospital.
3. Consider special issues of departmental requirements. The GI department had some special requirements for its admission note and discharge summary, such as some data items undefined in HL7, CDA and TMT.
4. Confirm data components and attributes by way of expert meeting.
Table 1 shows the data components of the admission note of GI department.
Figure 1 The general data part of the style sheet in a GI admission note
Table 1 Data components of the admission note of Gastroenterological department
Header
Service Data component and data attribute Information of
document
id, code, title, effective time, confidentiality code, language code, version number,…etc
Author id, address, name, birthday, telephone, organization,…etc
Patient id, address, marital, name, birthday, race, telephone,…etc Body Chief Compliant chief compliant Admission Diagnosis
illness name, start time, end time, level, description, plan to do,…etc Past Illness illness name, start time, end time,
level, description,…etc
Allergies food(name, time), drug(name, time), environment(name, time)
Psychosocial History
habit (cigarette smoking, alcohol consumption), sexual history(gender, frequency), travel history(date, region),…etc
Medications kind, drug name, amount, reason,…etc
Inoculation kind, drug name, amount, reason, age,…etc
Others, total 17 services
…
The 7-layer conceptual architecture of the implemented system is shown in Figure 2. Underlying Kernel layer provides the operating system. System Tool layer provides some libraries when web service was invoked. Department layer lists all departments in the system installed hospital. Template layer provides all kinds of clinical note. Service layer provides functions (services) in each note. Operation layer provides methods (operations) in each service. Messages layer is data attribute library. It provides data attributes in each template.
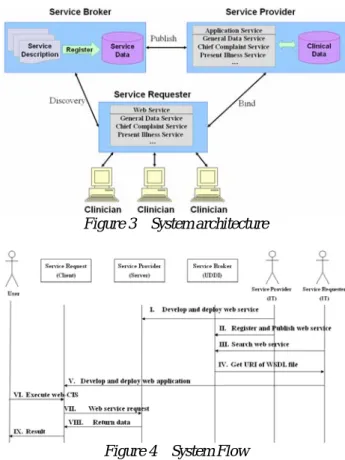
Figure 2 The 7-Layer Conceptual Architecture The system architecture is shown in Figure 3. Conforming to SOA, the system consists of three parts, i.e. Service Provider, Service Request, and Service Broker. Service Provider supplies miscellaneous web services, each serves as a module of the clinical notes. These web services have to be registered to Services Broker with WSDL file. Service Broker is responsible for cataloging services and archiving information of services. Service Requester is used to search the service information on Service Broker with service category or service name. A clinician may connect his/her client to Service Requester to receive services.
Figure 4 shows the system flow which involves several actors, including User, Service Requester, Service Provider, Service Broker, and IT staff. The system flow is described as following steps.
I. IT staff (Service Provider) develop and deploy web service to application sever (Microsoft Windows Sever 2003 and Oracle 9i).
II. IT staff (Service Provider) register its service to Service Broker with necessary information.
III. Others IT staff (Service Requester) search for web service at Service Broker.
IV. Service Broker return URI of WSDL file.
V. IT staff (Service Requester) download the WSDL file. The IT staff develop and deploy web application that according the information in WSDL file to web server (Microsoft Windows Sever 2003) VI. The user, which means clinician, executes browser
to start web-CIS and web service.
VII. Web server invokes service to retrieve the request data.
VIII. Sever application return a detailed dataset which the web sever request in XML format by SOAP message.
IX. At last, clinician saves the patient record into clinical database.
Figure 3 System architecture
Figure 4 System Flow
4. System Implementation
The system is implemented using Microsoft Visual Studio .net 2008 as the development tool. Designed templates and entered data are stored in Oracle 9i database. We built private UDDI in Microsoft Server 2003 and Microsoft SQL Server 2005.
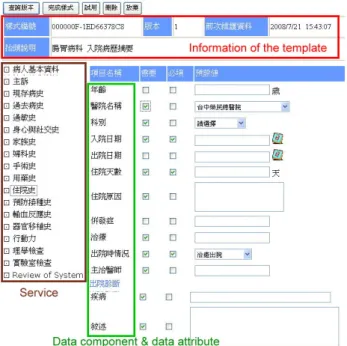
The system provides three major functions, named Clinical Note Template Designer, Clinical Note Content Editor, and Clinical Note Generator. Template Designer is used to set up the style sheet of a clinical note. While using this function, the system will list different services and data attributes depend on user’s department. Figure 5 shows a snapshot of clinical note template designer. The upper side of the screen shows some information about this template, such as template id, version, the time of last modify, and name. The lower-left side lists all kinds of services that provide by Service Provider, such as chief compliant, medical history, and family history etc. The lower-right side displays data attributes of selected service. A designer may tick the needed attributes, and then check each of them as required and has default value or not. As soon as the template is completely designed, an according database is created for succeeding content entering.
Figure 6 Editing a patient record
5. Conclusion
The system has several significant advantages over other kind of clinical information system architectures. Some salient ones list as follows.
ㅡ Easy to create and maintain the clinical notes: The template of miscellaneous clinical notes are created and maintained by clinical departments. In this way, a lot of system implementation time waiting for the information professionals will be reduced.
ㅡ Independent service: The system is designed based on SOA. Software reusability are improved through enhancing reuse the existing IT resources. ㅡ EMR quality improvement: After the integrated
medical record is created, it can increase the completeness, consistency, reusability of EMR, use in the teaching and the researching, improve quality of the decision support, and reduce the cost of the medical treatment.
ㅡ EMR sharing: Hospitals may share the electronic clinical notes which conform to the standard of the HL7 and TMT. It can greatly reduce the waste resources of redundant examinations.
Figure 5 A snapshot of designing hospitalize history module
Invoking the content editor, a clinician may enter and edit contents of a clinical note after choosing the appropriate template. Figure 6 is the snapshot of clinical note content editor. The content editor provides some convenient tools that make a clinician enter clinical data easily. For example, the system shows calendar when date-type data is entering. Another example is that the system may provide an auto complete when a string type attribute is entering. The entered contents of each service will be saved into the corresponding database automatically.
Acknowledgment
This research is sponsored in part by National Science Council (NSC), Taiwan, under grants NSC95-2221-E-126-006-MY3, NSC96-2221-E-126-004 -MY3 and NSC95-2218-E-007-025. Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the NSC.
References
[1] R. Haux, "Health information systems-past, present, future," International Journal of Medical Informatics, pp.268-281, 2006
According to the designed template and entered contents, the note generator will generate a formal clinical note in narrative for review and printing. A user who would like to view a clinical note have to enter a searching keyword, such as patient’s name, patient’s ID, or physician’s name and chooses a record. The generator will check a version number of the clinical note to decide whether a data attribute has to be shown. The service named “Review of System” has a lot of data components, such as general condition, skin, head etc. General condition has many data attributes, such as fever, chills, night fever, malaise etc. The note generator will list data attributes in order depends on that data attribute has been ticked or not.
[2] N. Wirsz, “Overview of IT-Standards in Healthcare,” Electromedica, vol 68, no.1, pp. 21-24, 2000
[3] HL7 Version Standard, http://www.hl7.org/v3ballot/html/welcome/environ
ment/index.htm
[4] P.M. Nadkarni and R.A. Miller, "Service-oriented Architecture in Medical Software: Promises and Perils," Journal of the American Medical Informatics Association, Volume 14, pp.244-246, Number 2 Mar / Apr 2007
[5] Taiwan Electronic Medical Record Template, http://emr.doh.gov.tw/
[6] W.S. Jian, C.Y. Hsu, T.H. Hao, H.C. Wen, M.H. Hsu, Y.L. Lee, Y.C. Li, and P. Chang, ”Building a portable data and information interoperability infrastructure—framework for a standard Taiwan Electronic Medical Record Template", Computer Methods and Programs in Biomedicine Volume 88, Issue 2, pp. 102-111, November 2007
[7] R.W. Yuan, The Establishment and Application Study of TMT-Based Standardized Health Examination Data, Tzu Chi University, Institute of Medical Information, Master Thesis, Hualien Taiwan R.O.C., July 2006
[8] W. Raghupathi and S. Kesh, ”Interoperable Electronic Health Records Design:Towards a Service-Oriented Architecture,” e-Service Journal ,Volume 5, pp. 39-57, Number 3 Summer 2007
[9] G. Canfora, A.R. Fasolino, and G. Frattolillo, P. Tramontana, “A wrapping approach for migrating legacy system interactive functionalities to Service Oriented Architectures,” The Journal of Systems and Software, pp.463–480, 2008
[10] A. Wright and D.F. Sittig, “SANDS: A service-oriented architecture for clinical decision support in a National Health Information Network,” Journal of Biomedical Informatics, 2008
[11] K. Z. Chen, C.H. Wen, D.C. Ye, and C.W. Chen, ”A Web-based Platform for Implementing Clinical Notes,” International Medical Informatics Symposium in Taiwan 2007, pp.17-21, October 2004
[12] C.Y. Shih, Study of Using Service-Oriented Architecture to Construct Clinical Information System-An Example on Ophthalmology, National Yang Ming University, Institute of Health Informatics and Decision Making, Master Thesis, Taipei Taiwan R.O.C., July 2006