Significant Association of Cyclooxygenase 2 Genotypes with Upper Tract Urothelial
Cancer
Wen-Shin Chang1,2*, Cheng-Hsi Liao1,3*, Chin-Mu Hsu2*, Chung-Yu Huang4, Chia-Wen Tsai2, Hsi-Chin Wu5, Pei-Shin Hu6, Tzu-Chia Wang2, Yun-Ru Syu2, Hao-Ai Shui4 and Da- Tian Bau1,2
1 Graduate Institute of Clinical Medical Science, China Medical University, Taichung, Taiwan, R.O.C.;
2 Terry Fox Cancer Research Laboratory and 5 Department of Urology, China Medical University Hospital, Taichung, Taiwan, R.O.C.;
3 Department of Urology, Taichung Armed Forces General Hospital, Taichung, Taiwan, R.O.C.;
4 Graduate Institute of Medical Sciences, National Defense Medical Center, Taipei, Taiwan, R.O.C.;
6 Department of Ophthalmology, Changhua Christian hospital, Changhua, Taiwan, R.O.C.
* These Authors contribute equally to this work
Correspondence to: Da-Tian Bau, Terry Fox Cancer Research Laboratory, Department of
Medical Research, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan, R.O.C. Tel: +886 422052121 Ext. 7534, Fax: +886 422053366, e-mail:
[email protected]; [email protected]
Running title: Huang et al: COX-2 in Upper Tract Urothelial Cancer
Abstract. Aim: Reliable biomarkers are in urgent need for diagnosis, outcome
prediction or treatment effect monitoring for upper tract urothelial carcinomas (UTUC). Although up-regulation of cyclooxygenase 2 (COX-2) are found in stroma and tumor cells in more than half of the UTUC patients investigated, the genomic contribution of COX-2 to UTUC is never studied. The study was to evaluate the association of six polymorphic genotypes of COX-2 with UTUC within a Taiwanese population. Materials and Methods: A total of 218 UTUC patients and 580 healthy
controls were genotyped for six COX-2 polymorphisms, A-1195G, G-765C, T+8473C, intron 1, intron 5, and intron 6, of their association with UTUC risk.
Results: The distribution of genotypes of COX-2 G-765C and intron 5 were significantly different between UTUC patient and control groups (p=0.0001 and 0.0016, respectively), while others were not (p>0.05). The haplotype analysis showed that compared with GG/TT haplotype of COX-2 G-765C/intron 5, people carrying GG/AT variants have a significant increased risk of UTUC (odds ratio, OR=4.83, 95% confidence interval, 95%CI=1.79-13.06) while people carrying CG/TT variants have a decreased risk (OR=0.26, 95%CI=0.14-0.49). Conclusion: Our results suggested that individual and combined COX-2 G-765C/intron 5 genotypes play a role in controlling the COX-2 expression and UTUC development.
Key Words: COX-2, genotype, polymorphism, Taiwan, upper tract urothelial cancer.
Upper tract urothelial cancer (UTUC) is universal problem, however, the incidence of urothelial cancer of the renal pelvis, ureter and bladder for Western countries and Taiwan were 3:1:51 and 1:2.08:6.72, respectively (1). The higher incidence makes it valuable to start the genomic and proteomic studies for UTUC from Taiwan and then compare the counterpart findings in Western populations. Epidemiologically speaking, mounting evidence showed that the elevated incidence of UTUC may be associated with arsenic exposure, smoking habit, analgesics abuse, occupational carcinogen exposure, hypertension, long standing urinary obstruction, infection and Balkan nephropathy (2-6). Recently, mounting evidence has suggested that genetic
polymorphic variations may also predispose to the development of UTUC (7, 8).
Cyclooxygenase-2 (COX-2) is an inducible enzyme for the conversion of arachidonic acid to prostanoid, prostaglandin and throboxane (9). Typically, COX-2 is often undetectable in normal tissues. In 2012, it was found that cyclooxygenase-2 (COX-2) was up-regulated in the stroma and tumor sites from UTUC, which could serve as a prognostic marker for poor clinical outcome of UTUC (10). The samples contained 128 paired tumor and stroma specimens, and the up-regulation of COX-2 was strongly associated with higher cancer-specific death and cancer recurrence rates (10). However, it is inconvenient to collect tissue from lots of normal people for prediction and the immunochemistry assay for protein expression is not as quick,
convenient, and repeatable as DNA sequencing assays. From the DNA level, the contribution of COX-2 genotype to UTUC has never been studied. The
overexpression of COX-2 may contribute to carcinogenesis via increasing cell proliferation, suppressing apoptosis, enhancing invasiveness, and inducing chronic activation of immune responses and angiogenesis (11-13). Based on the evidence collected from animal and clinical models, COX-2 specific inhibitors have both preventive and therapeutic effects as anticancer drugs for breast, bladder, lung and
pancreas cancers (14-18).
Following the rule of central dogma, subtle genetic variants on COX-2 gene may affect the quantity of COX-2 protein through altered self-regulated transcriptional activity or alternative splices resulting from polymorphic variations at promoter region or introns, respectively (19, 20). To clarify the hypothesis that the polymorphic variants at promoter or intron regions of COX-2 may be associated with the risk of UTUC, The aims of the current study were to determine the genotypic frequency of six polymorphisms of the COX-2 at A-1195G (rs689466), G-765C (rs20417), T+8473C (rs5275), intron 1 (rs2745557), intron 5 (rs16825748), intron 6 (rs2066826), and their contribution to UTUC susceptibility in Taiwan.
Materials and Methods
Sample collection. A total of 218 patients with UTUC were recruited at China
Medical University and Kaohsiung Medical University medical centers, all of whom were diagnosed by pathologic examination of specimens obtained by biopsy or surgical resection. The clinical and histopathologic information were collected from patient charts and pathologic reports. The information was reviewed, and the data were entered into the database. The tumor stage was assigned according to the TNM staging system (21), and the pathologic grade was determined according to the World Health Organization criteria (22). Five hundreds and eighty healthy individuals, who had been matched with the patients with age, admitted to the same hospital for health checkup and who had no previous diagnosis of urologic neoplastic disease or other malignancy were enrolled as controls. All the subjects enrolled were provided an informed consent and Human Research Committees have approved this study.
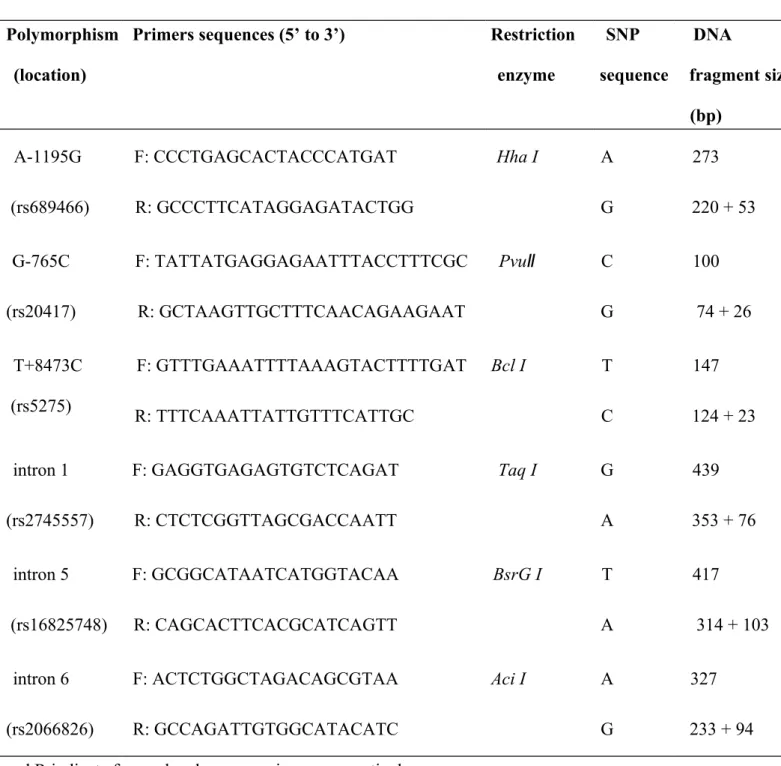
Genotyping conditions. The total genomic DNA of each subject was
extracted from the leucocytes of peripheral blood and stored as previously published (23-25). The polymerase chain reaction (PCR) cycling conditions were: one cycle at 94°C for 5 min; 35 cycles of 94°C for 30 sec, 55°C for 30 sec, and 72°C for 30 sec, and a final extension at 72°C for 10 min. Pairs of PCR primer sequences and restriction enzyme for each DNA product of COX-2 genotyping work are all listed in Table I. The PCR products were cut by proper restriction enzymes and
the reaction was incubated for 2 h at 37°C. Then, 10 l of each PCR product was loaded into a 3% agarose gel for electrophoresis.
Statistical analyses. Two hundreds and eighteen cases and five hundreds and eighty
controls were analyzed in the presented Tables. To ensure that the controls used were representative of the general population and to exclude the possibility of genotyping error, the deviation of the genotype frequencies of COX-2 single nucleotide polymorphism in the controls from those expected under the Hardy-Weinberg equilibrium was assessed using the goodness-of-fit test. Pearson’s chi-square test or Fisher’s exact test (when the expected number in any cell was less than five) was used to compare the distribution of the COX-2 genotypes between cases and controls.
Cancer risk associated with the genotypes was estimated as odds ratio (ORs) and 95%
confidence intervals (CIs) using unconditional logistic regression. All statistical tests were performed using SPSS for Windows (version 14.0; SPSS Inc., Chicago, IL, USA) on two-sided probabilities. The correlation between categorical variables was calculated for statistical significance using Pearson’s chi-square test and the threshold for significance was p<0.05.
Results
The frequency distributions of clinical characteristics for the subjects (218 UTUC
patients and 580 healthy controls) are shown in Table II. Epidemiologically, there was no difference in the frequency distribution between the gender (p=0.4256) or age (p=0.8518) since the population was well matched (Table II). From the clinical and pathological viewpoints, tumors distributed in renal pelvic, ureter and multiple sites were 38.5%, 34.9% and 26.6%, respectively. Among the patients, 60.6% were high
grade, and 77.1% were of stages lower than pT3 (Table II).
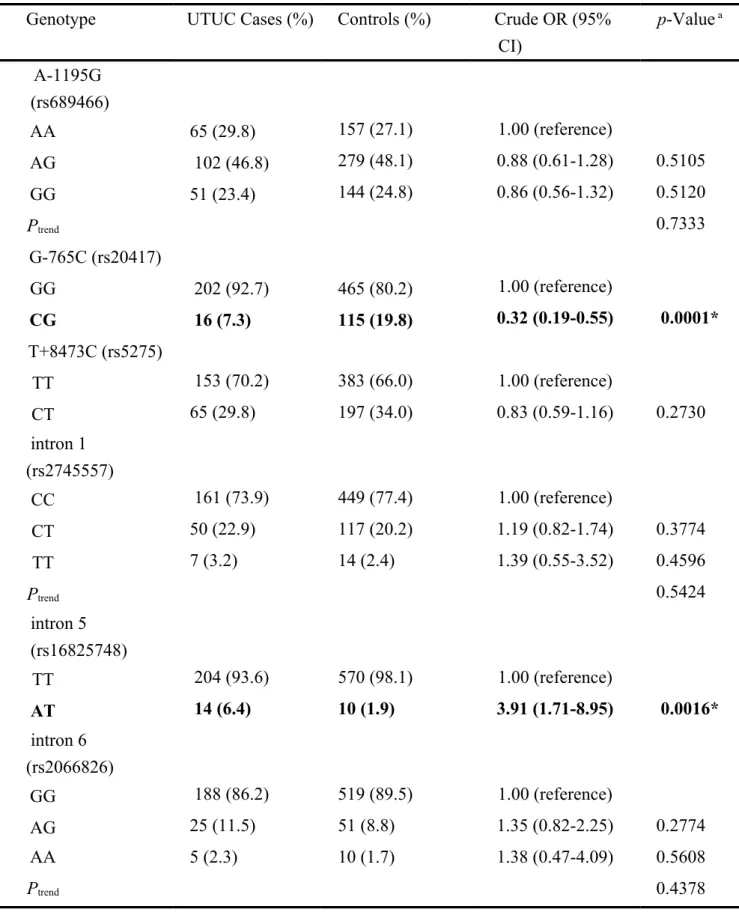
The frequencies of the genotypes for COX-2 A-1195G, G-765C, T+8473C, intron 1, intron 5, and intron 6 among the UTUC patients and healthy controls are summarized and analyzed in Table III. Among the six polymorphic genotypes investigated, two of them, G-765C (OR=0.32, 95%CI=0.19-0.55, p=0.0001) and intron 5 (OR=3.91, 95%CI=1.71-8.95, p=0.0016), were found to be differentially distributed between UTUC case and control groups (Table III). First, the frequencies of GG and CG genotypes of COX-2 G-765C were 92.7 and 7.3% among UTUC cases, and 80.2 and 19.8% among healthy controls, respectively. Second, the frequencies of TT and AT genotypes of COX-2 intron 5 were 93.6 and 6.4% among UTUC cases, and 98.1 and 1.9% among healthy controls, respectively (Table III). As for other polymorphic sites of COX-2, there was no difference in the distribution of genotypes among UTUC cases and controls (Table III).
In the next step, we have performed the allelic frequency analysis, and the
frequencies of the alleles for COX-2 A-1195G, G-765C, T+8473C, intron 1, intron 5, and intron 6 among the UTUC cases and healthy controls are summarized in Table IV. Consistent to the findings of Table III, G-765C and intron 5 of COX-2 were found to be associated with UTUC risk in Table IV. In detail, higher frequencies of G allele in G-765C and A allele in intron 5 in the UTUC case group than the control group, associating to higher risk of UTUC (Table IV; p=0.0001 and 0.0017, respectively).
Regarding to the other four COX-2 polymorphic sites, no distribution of their allelic frequencies was found to be significantly different between the control and UTUC
case groups (Table IV).
Considering the possible interactions between the two determinant COX-2 genotypes for UTUC susceptibility, the haplotypic distributions of COX-2 G-765C and intron 5 were further analyzed (Table V). We have set the most abundant genotypes for both G-765C and intron 5 genotypes as wild-type for haplotypic combination. Under this criteria, the “GG” genotype for COX-2 G-765C and “TT” for COX-2 intron 5 were selected, resulting in setting GG/TT combinative genotype in G-
765C/intron 5 as the reference haplotype. Compared with the reference haplotype of COX-2 G-765C/intron 5, the GG/AT group has a significant higher risk of UTUC (OR=4.83, 95%CI=1.79-13.06, p=0.0014) while CG/TT has a lower risk (OR=0.26, 95%CI=0.14-0.49, p=0.0001) (Table V). After adjusting for age and gender, the
significances became more obvious for the GG/AT and CG/TT groups with their individual ORs altered to 4.86 and 0.32, remained statistically significant (Table V).
The combination of CG/AT did not confer significantly altered cancer risk compared to the wild-type haplotype before or after adjusting for age and gender (Table V).
Discussion
Urothelial carcinoma is the second most common cancer which usually arises from the urothelium with transitional cell differentiation, including that of the renal pelvis, ureter and bladder. In literature, there were at least 600 papers investigating the contribution of individual genomic variations to bladder cancer (26-30), while few to UTUC (7, 31, 32). Following the rule of molecular central dogma, the single nucleotide variations on COX-2 among people may determine their differential expression of COX-2 and personal susceptibility to cancers. The supporting data comes from that COX-2 is often undetectable in normal tissues, whereas overexpression of COX-2 has been observed in neoplastic cells of canine (33) and human RCC (34-36). In our previous report, COX-2 was found to be up-regulated in both stromal and tumor cells of more than half of the UTUC patients and the positive expression of COX-2 in stromal cells may be a biomarker for UTUC-specific death and recurrence (10). However, the contribution of COX-2 genotypes to UTUC has
never been studied. In this study, the genotypes of COX-2 of 218 UTUC patients together with 580 controls (Table III) were examined. Statistically, the distributions of COX-2 genotypes for G-765C and intron 5 were differentially distributed among the
UTUC and healthy control groups (Table III). In addition, the allelic frequencies of the two polymorphisms were also differentially distributed between the two groups (Table IV). The results showed that the G allele of G-765C and A allele of intron 5 were associated with higher risk for UTUC and the haplotype analysis suggested that individuals with GG/AT and CG/TT haplotypes at G-765C/intron 5 were at altered risk of UTUC before and after adjusting of gender and age (Table V). UTUC is not a common cancer in Taiwan and the world, which may be one of the limitation for genomic study of UTUC. Compared with previous finding, we have enlarged the sample size from 56 cases and 436 controls in 2011 (37) to 218 cases and 580 controls (Table II). The strengthened sample size and the same trend of significant genotype distribution after age and gender adjustments highlighted the value, accuracy and
reliability of the overall findings (Table V).
This is the first UTUC genomic study showing COX-2 G-765C and intron 5 genotypes were associated with UTUC risk. The G allele of Cox-2 G-765C and A allele of COX-2 intron 5 were genomic risk factors and may serve as early screening and prediction biomarkers for UTUC in Taiwan and all over the world.
Acknowledgements
We thank all the colleagues in both China Medical University and Kaohsiung Medical University medical centers (Dr. Ke, Lin and Wu) for their contribution in sample collection. We also appreciate the technical assistance from our teammates Liang-Yi Lin, Yi-Kai Huang, and Ding-Hao Sun. This study was supported by research grants from Terry Fox Cancer Research Foundation, and in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103- TDU-B-212-113002).
References:
1 Carroll P. Urothelial carcinoma:cancers of bladder, ureter and renal pelvis. In:
Tanagho EA, McAninch JW, editors. General Urology. Philadelphia: Prentice-
Hall Int; 1995. pp. 353-71.
2 Mellemgaard A, Carstensen B, Norgaard N, Knudsen JB and Olsen JH:
Trends in the incidence of cancer of the kidney, pelvis, ureter and bladder in
Denmark 1943-88. Scand J Urol Nephrol 27: 327-332, 1993.
3 McLaughlin JK, Silverman DT, Hsing AW, Ross RK, Schoenberg JB, Yu MC, Stemhagen A, Lynch CF, Blot WJ and Fraumeni JF, Jr.: Cigarette smoking and cancers of the renal pelvis and ureter. Cancer Res 52: 254-257,
1992.
4 Chen CJ, Hsueh YM, Lai MS, Shyu MP, Chen SY, Wu MM, Kuo TL and Tai TY: Increased prevalence of hypertension and long-term arsenic exposure.
Hypertension 25: 53-60, 1995.
5 Linet MS, Chow WH, McLaughlin JK, Wacholder S, Yu MC, Schoenberg JB, Lynch C and Fraumeni JF, Jr.: Analgesics and cancers of the renal pelvis and
ureter. Int J Cancer 62: 15-18, 1995.
6 Liaw KL, Linet MS, McLaughlin JK, Yu MC, Schoenberg JB, Lynch CF, Niwa S and Fraumeni JF, Jr.: Possible relation between hypertension and cancers of the renal pelvis and ureter. Int J Cancer 70: 265-268, 1997.
7 Lin HH, Ke HL, Hsiao KH, Tsai CW, Wu WJ, Bau DT and Chang LL:
CCND1 1722 polymorphism and potential relevance to upper tract urothelial
cancer. Anticancer Res 31: 1043-1047, 2011.
8 Chang WS, Lin SS, Li FJ, Tsai CW, Li LY, Lien CS, Liao WL, Wu HC, Tsai CH, Shih TC and Bau DT: Significant association of caveolin-1 (CAV1) genotypes with upper urothelial tract cancer. Anticancer Res 33: 4907-4912,
2013.
9 DeWitt DL: Prostaglandin endoperoxide synthase: regulation of enzyme
expression. Biochim Biophys Acta 1083: 121-134, 1991.
10 Ke HL, Tu HP, Lin HH, Chai CY, Chang LL, Li WM, Li CC, Lee YC, Yeh HC, Wu WJ and Bau DT: Cyclooxygenase-2 (COX-2) up-regulation is a prognostic marker for poor clinical outcome of upper tract urothelial cancer.
Anticancer Res 32: 4111-4116, 2012.
11 O'Byrne KJ and Dalgleish AG: Chronic immune activation and inflammation
as the cause of malignancy. Br J Cancer 85: 473-483, 2001.
12 Kanaoka S, Takai T and Yoshida K: Cyclooxygenase-2 and tumor biology.
Adv Clin Chem 43: 59-78, 2007.
13 Li W, Mao Z, Fan X, Cui L and Wang X: Cyclooxygenase 2 promoted the tumorigenecity of pancreatic cancer cells. Tumour Biol 35: 2271-2278, 2014.
14 Davies G, Salter J, Hills M, Martin LA, Sacks N and Dowsett M: Correlation
between cyclooxygenase-2 expression and angiogenesis in human breast
cancer. Clin Cancer Res 9: 2651-2656, 2003.
15 Levitt RJ and Pollak M: Insulin-like growth factor-I antagonizes the antiproliferative effects of cyclooxygenase-2 inhibitors on BxPC-3 pancreatic
cancer cells. Cancer Res 62: 7372-7376, 2002.
16 Mizutani Y, Kamoi K, Ukimura O, Kawauchi A and Miki T: Synergistic cytotoxicity and apoptosis of JTE-522, a selective cyclooxygenase-2 inhibitor,
and 5-fluorouracil against bladder cancer. J Urol 168: 2650-2654, 2002.
17 Sanchez-Alcazar JA, Bradbury DA, Pang L and Knox AJ: Cyclooxygenase (COX) inhibitors induce apoptosis in non-small cell lung cancer through
cyclooxygenase independent pathways. Lung Cancer 40: 33-44, 2003.
18 Wang YX, Gao JX, Wang XY, Zhang L and Liu CM: Antiproliferative effects of selective cyclooxygenase-2 inhibitor modulated by nimotuzumab in
estrogen-dependent breast cancer cells. Tumour Biol 33: 957-966, 2012.
19 Szczeklik W, Sanak M and Szczeklik A: Functional effects and gender association of COX-2 gene polymorphism G-765C in bronchial asthma. J
Allergy Clin Immunol 114: 248-253, 2004.
20 Sugie S, Tsukino H, Mukai S, Akioka T, Shibata N, Nagano M and Kamoto T:
Cyclooxygenase 2 genotypes influence prostate cancer susceptibility in Japanese Men. Tumour Biol 35: 2717-2721, 2014.
21 Greene FL, Page DL, Fleming ID, A.G. F, C.M. B, D.G. H and M. M (eds.)
AJCC Cancer Staging Manual, 6 edition. New York: Springer-Verlag, 2002.
22 Epstein JI, Amin MB, Reuter VR and Mostofi FK: The World Health Organization/International Society of Urological Pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder.
Bladder Consensus Conference Committee. Am J Surg Pathol 22: 1435-1448,
1998.
23 Tsai CW, Chang WS, Liu JC, Tsai MH, Lin CC and Bau DT: Contribution of DNA Double-strand Break Repair Gene XRCC3 Genotypes to Oral Cancer
Susceptibility in Taiwan. Anticancer Res 34: 2951-2956, 2014.
24 Chang WS, Tsai CW, Ji HX, Wu HC, Chang YT, Lien CS, Liao WL, Shen WC, Tsai CH and Bau DT: Associations of cyclooxygenase 2 polymorphic genotypes with bladder cancer risk in Taiwan. Anticancer Res 33: 5401-5405,
2013.
25 Tsai CW, Tsai MH, Shih LC, Chang WS, Lin CC and Bau DT: Association of interleukin-10 (IL10) promoter genotypes with nasopharyngeal carcinoma risk
in Taiwan. Anticancer Res 33: 3391-3396, 2013.
26 Primdahl H, Wikman FP, von der Maase H, Zhou XG, Wolf H and Orntoft TF: Allelic imbalances in human bladder cancer: genome-wide detection with
216-223, 2002.
27 Hoque MO, Lee CC, Cairns P, Schoenberg M and Sidransky D: Genome-wide genetic characterization of bladder cancer: a comparison of high-density single-nucleotide polymorphism arrays and PCR-based microsatellite analysis.
Cancer Res 63: 2216-2222, 2003.
28 Chang CH, Chang CL, Tsai CW, Wu HC, Chiu CF, Wang RF, Liu CS, Lin CC and Bau DT: Significant association of an XRCC4 single nucleotide polymorphism with bladder cancer susceptibility in Taiwan. Anticancer Res 29: 1777-1782, 2009.
29 Chang CH, Wang RF, Tsai RY, Wu HC, Wang CH, Tsai CW, Chang CL, Tsou YA, Liu CS and Bau DT: Significant association of XPD codon 312 single nucleotide polymorphism with bladder cancer susceptibility in Taiwan.
Anticancer Res 29: 3903-3907, 2009.
30 Selinski S, Lehmann ML, Blaszkewicz M, Ovsiannikov D, Moormann O, Guballa C, Kress A, Truss MC, Gerullis H, Otto T, Barski D, Niegisch G, Albers P, Frees S, Brenner W, Thuroff JW, Angeli-Greaves M, Seidel T, Roth G, Volkert F, Ebbinghaus R, Prager HM, Lukas C, Bolt HM, Falkenstein M, Zimmermann A, Klein T, Reckwitz T, Roemer HC, Hartel M, Weistenhofer W, Schops W, Rizvi SA, Aslam M, Banfi G, Romics I, Ickstadt K, Hengstler JG and Golka K: Urinary bladder cancer risk in relation to a single nucleotide
polymorphism (rs2854744) in the insulin-like growth factor-binding protein-3
(IGFBP3) gene. Arch Toxicol 86: 195-203, 2012.
31 Yates DR, Roupret M, Drouin SJ, Audouin M, Cancel-Tassin G, Comperat E, Bitker MO and Cussenot O: Genetic polymorphisms on 8q24.1 and 4p16.3 are not linked with urothelial carcinoma of the bladder in contrast to their association with aggressive upper urinary tract tumours. World J Urol 31: 53-
59, 2013.
32 Lin HH, Ke HL, Hsiao KH, Tsai CW, Wu WJ, Bau DT and Chang LL:
Potential role of CCND1 G870A genotype as a predictor for urothelial carcinoma susceptibility and muscle-invasiveness in Taiwan. Chin J Physiol 54: 196-202, 2011.
33 Khan KN, Stanfield KM, Trajkovic D and Knapp DW: Expression of cyclooxygenase-2 in canine renal cell carcinoma. Vet Pathol 38: 116-119,
2001.
34 Mungan MU, Gurel D, Canda AE, Tuna B, Yorukoglu K and Kirkali Z:
Expression of COX-2 in normal and pyelonephritic kidney, renal intraepithelial neoplasia, and renal cell carcinoma. Eur Urol 50: 92-97;
discussion 97, 2006.
35 Ristimaki A, Nieminen O, Saukkonen K, Hotakainen K, Nordling S and
carcinoma of the urinary bladder. Am J Pathol 158: 849-853, 2001.
36 Miyata Y, Koga S, Kanda S, Nishikido M, Hayashi T and Kanetake H:
Expression of cyclooxygenase-2 in renal cell carcinoma: correlation with tumor cell proliferation, apoptosis, angiogenesis, expression of matrix
metalloproteinase-2, and survival. Clin Cancer Res 9: 1741-1749, 2003.
37 Chang CH, Wu HC, Ke HL, Lin HH, Shen WC, Sun SS, Tsai CW, Tsai RY and Bau DT: The genetic role of cyclooxygenase 2 in ureter cancer in Taiwan.
Adaptive Medicine 3: 99-105, 2011.
Table I. Primer sequences and restriction fragment length polymorphism conditions for cyclooxygenase 2
(COX-2) genotyping analysis.
Polymorphism (location)
Primers sequences (5’ to 3’) Restriction enzyme
SNP sequence
DNA
fragment size (bp)
A-1195G (rs689466)
F: CCCTGAGCACTACCCATGAT R: GCCCTTCATAGGAGATACTGG
Hha I A
G
273 220 + 53 G-765C
(rs20417)
F: TATTATGAGGAGAATTTACCTTTCGC R: GCTAAGTTGCTTTCAACAGAAGAAT
PvuⅡ C
G
100 74 + 26 T+8473C
(rs5275)
F: GTTTGAAATTTTAAAGTACTTTTGAT R: TTTCAAATTATTGTTTCATTGC
Bcl I T
C
147 124 + 23 intron 1
(rs2745557)
F: GAGGTGAGAGTGTCTCAGAT R: CTCTCGGTTAGCGACCAATT
Taq I G
A
439 353 + 76
intron 5 (rs16825748)
F: GCGGCATAATCATGGTACAA R: CAGCACTTCACGCATCAGTT
BsrG I T
A
417 314 + 103 intron 6
(rs2066826)
F: ACTCTGGCTAGACAGCGTAA R: GCCAGATTGTGGCATACATC
Aci I A
G
327 233 + 94 F and R indicate forward and reverse primers, respectively.
Table II. Frequency distributions of clinical characteristics among upper tract urothelial cancer patients
and healthy controls.
Characteristics UTUC (n=218)
n (%)
Control (n=580)
n (%)
p-Value
Gender
Male 114 (52.3) 323 (55.7)
Female 104 (47.7) 257 (44.3) 0.4256
Mean age 65.4 ± 4.7 62.9 ± 3.9 0.8518
Location
Renal pelvic tumor 84 (38.5)
Ureter tumor 76 (34.9)
Multiple tumors 58 (26.6)
Grade
Low 86 (39.4)
High 132 (60.6)
Stage
I and II 168 (77.1)
III and IV 50 (22.9)
Table III. Distributions of COX-2 genotypic frequencies among the UTUC cases and controls.
Genotype UTUC Cases (%) Controls (%) Crude OR (95%
CI)
p-Value a
A-1195G (rs689466)
AA 65 (29.8) 157 (27.1) 1.00 (reference)
AG 102 (46.8) 279 (48.1) 0.88 (0.61-1.28) 0.5105
GG 51 (23.4) 144 (24.8) 0.86 (0.56-1.32) 0.5120
Ptrend 0.7333
G-765C (rs20417)
GG 202 (92.7) 465 (80.2) 1.00 (reference)
CG 16 (7.3) 115 (19.8) 0.32 (0.19-0.55) 0.0001*
T+8473C (rs5275)
TT 153 (70.2) 383 (66.0) 1.00 (reference)
CT 65 (29.8) 197 (34.0) 0.83 (0.59-1.16) 0.2730
intron 1 (rs2745557)
CC 161 (73.9) 449 (77.4) 1.00 (reference)
CT 50 (22.9) 117 (20.2) 1.19 (0.82-1.74) 0.3774
TT 7 (3.2) 14 (2.4) 1.39 (0.55-3.52) 0.4596
Ptrend 0.5424
intron 5 (rs16825748)
TT 204 (93.6) 570 (98.1) 1.00 (reference)
AT 14 (6.4) 10 (1.9) 3.91 (1.71-8.95) 0.0016*
intron 6 (rs2066826)
GG 188 (86.2) 519 (89.5) 1.00 (reference)
AG 25 (11.5) 51 (8.8) 1.35 (0.82-2.25) 0.2774
AA 5 (2.3) 10 (1.7) 1.38 (0.47-4.09) 0.5608
Ptrend 0.4378
a the significant p-value is bolded and marked with a star;
OR: odds ratio; CI: confidence interval
Table IV. Distributions of COX-2 allelic frequencies among the UTUC cases and controls.
Allele UTUC cases % Controls % Crude OR (95% CI) p-Value a
A-1195G (rs689466)
Allele A 232 53.2% 593 51.1% 1.00 (reference)
Allele G 204 46.8% 567 48.9% 0.92 (0.74-1.47) 0.4654
G-765C (rs20417)
Allele G 420 96.3% 1045 90.1% 1.00 (reference)
Allele C 16 3.7% 115 9.9% 0.35 (0.20-0.59)* 0.0001*
T+8473C (rs5275)
Allele T 371 85.1% 963 83.0% 1.00 (reference)
Allele C 65 14.9% 197 17.0% 0.86 (0.63-1.16) 0.3628
intron 1 (rs2745557)
Allele G 372 85.3% 1015 87.5% 1.00 (reference)
Allele A 64 14.7% 145 12.5% 1.20 (0.88-1.65) 0.2789
intron 5 (rs16825748)
Allele T 422 96.8% 1150 99.1% 1.00 (reference)
Allele A 14 3.2% 10 0.9% 3.81 (1.68-8.66)* 0.0017*
intron 6 (rs2066826)
Allele G 401 92.0% 1089 93.9% 1.00 (reference)
Allele A 35 8.0% 71 6.1% 1.34 (0.88-2.04) 0.1768
a the significant p-Value and odds ratio are bolded and marked with a star