Title: Subdural hematoma in patients with end-stage renal disease receiving hemodialysis
Short title: SDH and hemodialysis
I-Kuan Wang, MD a,b,c; Cheng-Li Lin, MSd,e; Yi-Ying Wu, PhDf, Huey-Liang Kuo, MDc, Shih-Yi Lin, MDc; Chiz-Tzung Chang, PhDc; Tzung-Hai Yen, PhDg,h; Feng- Rong Chuang, MDi; Yu-Kai Cheng, MDj; Chiu-Ching Huang, MDc,*; Fung-Chang
Sung, PhD, MPHa,d,e,*
aGraduate Institute of Clinical Medical Science, China Medical University College of
Medicine, Taichung, Taiwan.
bDepartment of Internal Medicine, China Medical University College of Medicine,
Taichung, Taiwan.
cDivision of Nephrology, China Medical University Hospital, Taichung, Taiwan
dManagement Office for Health Data, China Medical University Hospital, Taichung,
Taiwan.
eDepartment of Public Health, China Medical University, Taichung, Taiwan
fDepartment of Medical Laboratory Science and Biotechnology, China Medical
university, Taichng, Taiwan.
gDivision of Nephrology, Chang Gung Memorial Hospital, Taipei, Taiwan.
hChang Gung University College of Medicine, Taoyuan, Taiwan.
iDivision of Nephrology, Kaohsiung Chang Gung Memorial Hospital Medical Center,
Chang Gung University College of Medicine, Kaohsiung, Taiwan.
jDivision of neurosurgery, China Medical University Hospital, Taichung, Taiwan.
Correspondence:
Fung-Chang Sung, PhD, MPH Professor
China Medical University College of Public Health 91 Hsueh Shih Road
Taichung 404, Taiwan Tel: 886-4-2206-2295 Fax: 886-4-2201-9901
E-mail: [email protected]
*Contributed equally
Conducting the statistical analysis: Cheng-Li Lin, MS
Words count: 72 characters in title, 196 words in the Abstract, 3808 words in the Text, 4 tables, 1 figures, 1 supplement figure and 28 references
Funding: National Sciences Council, Executive Yuan, Taiwan (Grant Numbers NSC 100-2621-M-039-001), China Medical University Hospital (Grant Number 1MS1), and Taiwan Department of Health Clinical Trial and Research Center for Excellence (Grant Numbers DOH102-TD-B-111-004 and DOH102-TD-C111-005).
Abstract
Background: Hemodialysis (HD) may increase the risk of acute subdural hematoma (SDH) with high fatality, but the extent of this disease in non-Western populations is unclear. We examined the incidence of and fatality from SDH in patients with end
stage renal disease (ESRD) on HD for an Asian population.
Methods: From a universal insurance claims database of Taiwan, we identified a cohort of 4709 incident ESRD patients on HD from 1998 to 2010, and a control cohort of 18663 subjects without any kidney disease. Incidence and hazard of SDH for the two cohorts and 30-day mortality from SDH were measured by the end of
2010.
Results: The incidence of SDH was 4.47-fold higher in the HD cohort than in the control cohort (56.3 vs. 12.6 per 10,000 person-years) with an adjusted hazard ratio (HR) of 3.81 (95% CIs = 2.77-5.25). HD patients with SDH had a high odds of 30-
day mortality with an adjusted odds ratio of 6.34 (95% CI=2.37-16.9).
Conclusions: We demonstrated that ESRD patients with HD are at a high risk of subsequent SDH and have a high mortality risk from SDH. Proper care for HD patients is necessary to prevent the devastating disorder.
Keywords: Cohort study; end-stage renal disease; hemodialysis; subdural hematoma.
Introduction
Subdural hematoma (SDH) is the most common traumatic brain injury with high mortality rate . The disease forms between the dura and the arachnoid membranes usually because of tearing in bridging veins that cross the subdural space to drain into the dural sinuses . Arterial rupture can also lead to SDH and the origin as a whole comprises 20 to 30% of SDH . SDH may increase the intracranial pressure, which can compress and damage brain tissue. The clinical manifestations of the disease are protean, and diagnosis requires a high index of suspicion . Clinical presentations of SDH are classified into acute, subacute, and chronic. Acute SDH usually develops over 24 to 48 hours, while subacute SDH usually develops over 3 to 14 days, and chronic SDH develops over more than 14 days . Acute SDH often occur with major trauma, most commonly resulting from motor vehicle collisions in young adults and falls in the elderly . Chronic SDH is most seen in the elderly and may be preceded by a trivial injury or fall . There is no identifiable trauma history in 30 to 50% patients with chronic SDH . The mortality rate in acute SDH is 50 to 60% for patients requiring surgery and 57 to 68% for patients presenting with coma . Patients with chronic SDH have much better prognosis if properly managed. The overall in-hospital mortality rate was 15.6% in a large-scale study of 715 patients .
The risk factors for SDH include advancing age, fall, head injury, use of
anticoagulants or antiplatelet drugs, bleeding diatheses, alcohol use, epilepsy, low intracranial pressure, and hemodialysis . Studies on the risk of SDH in dialysis patients have been few . An earlier Japanese study reported that acute SDH accounted for 8.6% of sudden deaths in hemodialysis (HD) patients . Sood et al. found in the US long-term HD dialysis patients are at 10-fold higher risk, comparing with general population . The present study evaluated the incidence in patients with incident end- stage renal disease (ESRD) on HD, and in comparisons of subjects without any kidney disease, using population-based universal insurance claims database. The risk of 30-day mortality from SDH was estimated as well. In addition, we also analyzed the age-standardized incidence rate of SDH in prevalent ESRD patients receiving HD from 1998 to 2010.
Methods
Data Sources
The Taiwanese government implemented the National Health Insurance (NHI) program in March 1995, which has provided the universal health insurance coverage to 99% of the entire population (23.74 million) in Taiwan since 1999. We obtained a subset of Taiwan’s National Health Insurance Research Database (NHIRD)
containing data on reimbursement claims from 1996 to 2010 for 1,000,000 randomly selected insured people representative of whole population. For confidentiality, the data set was provided to researchers with all insured identification numbers
scrambled. We used the scrambled numbers to link files, including the registry of beneficiaries, inpatient orders, ambulatory cares, and registry of catastrophic illness.
Diagnoses were coded with the International Codes of Disease 9th Edition Clinical Modification (ICD-9-CM). This study complied with the guidelines of the Declaration of Helsinki and was approved by the Ethics Review Board at China Medical
University (CMU-REC-101-012).
Study subjects
We identified patients with newly diagnosed ESRD (ICD-9 code 585) from the registry of catastrophic illness and by special treatment codes for HD (58027C, 58029C, and 58001C) as the HD cohort. The index date was the date a patient registered for ESRD care. Patients with a history of subdural hemorrhage diagnosed before index date (n = 45) and kidney transplantation (n = 151), and younger than 20 years of age (n = 27) were excluded. The remaining 4709 HD patients were included in this study as the HD cohort. For comparison, we randomly selected 4-fold persons from insured population without any kidney disease (ICD-9 code 403, 404, and 580-
589) as the control cohort, frequency matched by age (every 1 year), sex and index year. The comparison cohort included 18663 subjects.
Outcome measure
Each study subject was followed to evaluate the occurrence of SDH including non- traumatic SDH (ICD-9 code 432.1) and traumatic SDH (ICD-9-CM codes 852.2- 852.3) until December 31, 2010 or censored because of loss to follow-up, death, or withdrawal from the insurance program. Incidence of SDH was estimated by sex, age and comorbidity.
Exposure Variables
We identified baseline comorbidities and medications of patients, including coronary
artery disease (CAD, ICD-9- code 410 to 413, 414.01 to 414.05, 414.8, and 414.9), congestive heart failure (CHF, ICD-9- code 428, 398.91, 402.x1), stroke (ICD-9- code 430–438), hyperlipidemia (ICD-9- code 272), atrial fibrillation (ICD-9- code 427.31), hypertension (ICD-9- code 401 to 405), diabetes (ICD-9- code 250), dementia (ICD- 9- code 290.0 to 290.4, 294.1 and 331.0), atrial fibrillation (ICD-9-code 427.31) and usage of warfarin, clopidogrel and aspirin.
Statistical Analysis
Annual age-standardized incidence rate of SDH for the prevalent HD patients was calculated from 1998 to 2010 based on the HD population in 1998. We compared the distributions of age, sex, comorbidities and medications between HD and control cohorts, which were examined using Chi-square test and t-test. The incidence density rates were estimated by these variables, and the HD cohort to the control cohort incidence rate ratios (IRRs) were estimated by Poisson regression for the
corresponding variables. Cox proportional hazards regression analysis was used to assess the hazard ratios (HRs) and 95% confidence intervals (CIs) of developing SDH in the HD cohort, compared to the control cohort. The multivariate Cox model
controlling for demographic factors and comorbidities was used for adjustment. A further analysis assessed whether the risk of SDH varied by traumatic status and the follow-up period. We compared the incidence between traumatic SDH and non- traumatic SDH within 1 year and longer than 1 year. Moreover, logistic regression analysis was used to measure the odds ratio (OR) of the 30-day mortality from SDH
in HD patients, compared with the control cohort.
The cumulative incidence curves of SDH in the HD cohort and the control cohort were assessed using the Kaplan-Meier method and the difference was assessed with a log-rank test. All statistical analyses were performed using the SAS statistical package (version 9.2 for Windows; SAS Institute, Inc., Cary, NC, USA) and the Kaplan-Meier
survival curve was plotted using R software (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was regarded as P< 0.05.
Results
The annual age-standardized incidence rate of SDH for the prevalent HD patients increased from 3.38 per 1000 patient-years in 1998 to 5.25 per 1000 patient-years in 2010, with a peak of 6.85 per 1000 patient-years in 2004, although the increase was not significant (P for trend = 0.299) (Figure S1 online only). Table 1 shows
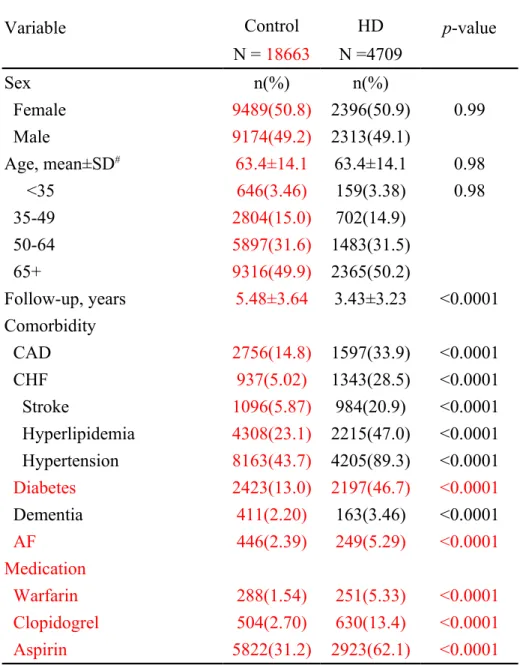
distributions of demographic characteristics were similar in both HD and control cohorts. The mean duration of follow-up was shorter in the HD cohort than in the control cohort (3.43 vs. 5.48 years, p <0.0001), while HD patients were more
prevalent with CAD, CHF, stroke, hyperlipidemia, hypertension, diabetes, dementia, AF, and warfarin, clopidogrel and aspirin (all p <0.0001).
The incidence rate of SDH was 4.47-fold higher in the HD cohort than in the control cohort comparisons (56.3 vs. 12.6 per 10,000 person-years) with an adjusted HR of 3.81 (95% CI = 2.77-5.25) (Table 2). Males had greater incidence rates of SDH than females in both the HD cohort (69.4 vs. 45.0 per 10,000 person-years
respectively) and the control cohort (15.9 vs. 9.61 per 10,000 person years). The SDH incidence increased with age in both cohorts, with the HD cohort to control cohort IRR the highest for 50-64 years old subjects. Subjects with any comorbidity had
increased incidence of SDH compared with those without the comorbidity. The Kaplan-Meier analysis displayed that the cumulative incidence of SDH was 5.02%
greater in the HD cohort than in the control cohort (log-rank test: p<0.0001) (Figure
1).
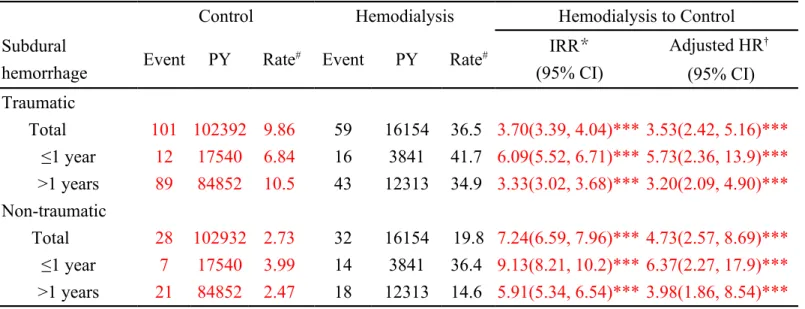
Table 3 shows the incidence rate and adjusted HR of traumatic SDH and non-
traumatic SDH measured during follow-up. The traumatic SDH incidence was higher than the non-traumatic SDH incidence in both cohorts. However, the adjusted HR of the HD cohort compared to the control cohort was greater for non-traumatic SDH than that for traumatic SDH (4.73 vs. 3.53). Higher SDH hazard appeared in the first year of follow-up for both traumatic SDH (adjusted HR = 5.73, 95% CI = 2.36–13.9)
and non-traumatic SDH (adjusted HR = 6.37, 95% CI = 2.27-17.9) for the HD cohort.
HD patients with SDH was associated with a significant higher 30-day mortality risk than controls with SDH (adjusted OR = 6.34, 95% CI = 2.37-16.9) (Table 4).
Compared with the control cohort, the OR of 30-day mortality was greater for HD patients with non-traumatic SDH than those with traumatic SDH (adjusted OR = 19.4 vs. 4.36).
Discussion
Our study demonstrated that incident ESRD patients undergoing HD had an adjusted HR of 3.67 for SDH and an adjusted HR of 6.54 for SDH-associated mortality,
compared to the control cohort. The traumatic SDH incidence was higher than non- traumatic; but the HD cohort had a higher relative HR of non-traumatic SDH than traumatic SDH compared to the control cohort, indicating the relative impact of HD
was stronger than that of trauma. Although the events were infrequent (91 vs. 129 cases or 56.3 vs. 12.6 per 10,000 person-years in the HD cohort vs. in the control cohort, respectively), the mortality rates were high. In addition, subjects with chronic kidney disease not yet on dialysis had a slightly higher hazard of SDH compared with those without chronic kidney disease [adjusted HR=1.21(95% CI, 1.06-1.37)] (data not shown). The SDH risk associated with chronic kidney disease on yet on dialysis
was lower than that associated with ESRD on HD.
Several factors may explain the increased risk of SDH in association with HD.
Platelet dysfunction contributes to bleeding diathesis in ESRD patients. Dysfunction of glycoprotein IIb/IIIa may contribute to reduced platelet aggregation and impaired platelet adhesion . The bleeding tendency is exacerbated by the use of systemic anticoagulation, such as heparin during HD and coumadin for patients with atrial fibrillation or vascular access patency, and increased INR variability in HD patients . Antiplatelet drugs for high prevalence of cardiovascular disease in ESRD patients may further result in bleeding tendency . In addition, brain atrophy is common in ESRD patients . The increased length of bridging veins makes these patients
vulnerable to SDH. Arachnoid cysts in 8.1% patients with adult polycystic kidney disease also contribute to the risk of SDH in these patients . The other possible mechanisms for non-traumatic SDH include changes in intracranial pressure during
hemodialysis.
Fall also has been related to an increased risk of traumatic SDH in HD patients.
Rossier et al. found that the incidence of fall in the elderly was four times higher in HD patients than in the general population . Advanced age, comorbidities, cognitive impairment, psychotropic drug use, blood pressure drug use, malnutrition, post- dialysis hypotension, renal bone diseases, and vitamin-D deficiency are factors have
been found to increase the vulnerability to fall for HD patients .
The present study demonstrated the incidence of traumatic SDH was 1.8-fold higher than that of non-traumatic SDH (36.5 vs. 19.8 patients per 10000 person-years).
Similar incidence of non-traumatic SDH has been found in HD patients in two studies: 19.1 per 10000 patient-years reported by a European single center study and 18.9 per 10000 patient-years measured from the US Renal Data System . The SDH incidence in the US increased from 1991 to 2002, while the European single center study showed a stable annual incidence in 2002-2009 . However, both studies did not adjust age for comparison. Our study showed that the age-standardized incidence rate of SDH increased in 2010 (5.25 per 1000 patient-years) compared to 1998 (3.38 per
1000 patients-years). Although coumadin was not used for vascular access patency in Taiwan, it is likely that the increased use of anticoagulants and antiplatelet agents for cardiovascular diseases might contribute to the increasing rate. The age-standardized incidence could have increased over time due to improvements in coding or diagnosis
rather than a true increase.
We found a higher risk of SDH within one year after the diagnosis of ESRD.
Previous research indicated that the survival rate of incident dialysis patients was lowest during the first year of dialysis . Patients with a shorter vintage of dialysis may have unstable physical conditions and therefore are more vulnerable to SDH. We took the HD cohort from the start of HD therapy rather than day 90 which most HD
registries report on. Therefore, the HD cohort was sicker and the rate of SDH could be inflated. The 30-day mortality of SDH in our study was 35.2% with an adjusted HR of
6.54 compared to the non-ESRD cohort. Similar to our findings, the mortality rate in
previous studies was about 40% .
This study has the advantages of using a large population-based sample size and a matched cohort study model in design. However, there are several limitations. First, information on lifestyle, smoking habit, body-mass index, Glasgow coma scale score, frailty, and laboratory measures on adequacy of dialysis are unavailable from the claims file. These variables could not be adjusted in the data analysis. Secondly,
because the neuroimaging findings are also not available from this database, we could not classify SDH and were unable to differentiate the prognostic outcomes between patients with acute SDH and those with chronic SDH. Thirdly, SDH and other comorbidities were identified using ICD-9-CM codes. We were unable to calculate the validity of diagnostic codes for SDH. However, the high validity of the diagnostic codes of the NHRI database has been reported . In addition, HD patients were visited by health care professionals frequently, the claims data is reliable. Furthermore, the cause of death cannot be obtained from the database. The mortality risk of HD
patients is expected to be higher than general population with a 3-month relative survival estimate of 95%. However, the odds ratio of 30-day mortality from SDH for HD patients in our study was extremely high. In addition, the incidence and risk of
SDH might be underestimated in ESRD patients due to the competing risk of death.
In conclusion, this study has demonstrated that HD patients are at an increased risk of SDH and the fatality is elevated further for patients who develop SDH. Because the consequence of SDH is devastating, appropriate preventive strategy of SDH is needed for the HD patients. Judicious use of anticoagulants and antiplatelet agents, adequate dialysis to improve platelet dysfunction, and intervention to prevent falls such as exercise or physical therapy, and vitamin D supplementations may have roles in preventing the occurrence of SDH .
Acknowledgments
The study was supported partly by the National Sciences Council, Executive Yuan, Taiwan (Grant Numbers NSC 100-2621-M-039-001), China Medical University Hospital (Grant Number 1MS1), and Taiwan Department of Health Clinical Trial and Research Center for Excellence (Grant Numbers DOH102-TD-B-111-004 and
DOH102-TD-C111-005).
Disclosure of conflict of interest
The authors declare no conflicts of interest.
References
1. Harvey LA, Close JC. Traumatic brain injury in older adults: characteristics,
causes and consequences. Injury. 2012 43: 1821-1826.
2. Maas AI, Steyerberg EW, Butcher I, et al. Prognostic value of computerized tomography scan characteristics in traumatic brain injury: results from the IMPACT
study. J Neurotrauma. 2007 24: 303-314.
3. Gottesman RF, Komotar R, Hillis AE. Neurologic aspects of traumatic brain
injury. Int Rev Psychiatry. 2003 15: 302-309.
4. Maxeiner H, Wolff M. Pure subdural hematomas: a postmortem analysis of their form and bleeding points. Neurosurgery. 2002 50: 503-508; discussion 508-509.
5. Brouns R, De Deyn PP. Neurological complications in renal failure: a review.
Clin Neurol Neurosurg. 2004 107: 1-16.
6. Nolan S. Traumatic brain injury: a review. Crit Care Nurs Q. 2005 28: 188-194.
7. Adhiyaman V, Asghar M, Ganeshram KN, Bhowmick BK. Chronic subdural
haematoma in the elderly. Postgrad Med J. 2002 78: 71-75.
8. Bullock MR, Chesnut R, Ghajar J, et al. Surgical management of acute subdural
hematomas. Neurosurgery. 2006 58: S16-24; discussion Si-iv.
9. Wilberger JE, Jr., Harris M, Diamond DL. Acute subdural hematoma: morbidity,
mortality, and operative timing. J Neurosurg. 1991 74: 212-218.
10. Rozzelle CJ, Wofford JL, Branch CL. Predictors of hospital mortality in older
patients with subdural hematoma. J Am Geriatr Soc. 1995 43: 240-244.
11. Leonard A, Shapiro FL. Subdural hematoma in regularly hemodialyzed patients.
Ann Intern Med. 1975 82: 650-658.
12. Power A, Hamady M, Singh S, Ashby D, Taube D, Duncan N. High but stable incidence of subdural haematoma in haemodialysis--a single-centre study. Nephrol Dial Transplant. 2010 25: 2272-2275.
13. Sood P, Sinson GP, Cohen EP. Subdural hematomas in chronic dialysis patients:
significant and increasing. Clin J Am Soc Nephrol. 2007 2: 956-959.
14. Takeda K, Harada A, Okuda S, et al. Sudden death in chronic dialysis patients.
Nephrol Dial Transplant. 1997 12: 952-955.
15. Gawaz MP, Dobos G, Spath M, Schollmeyer P, Gurland HJ, Mujais SK.
Impaired function of platelet membrane glycoprotein IIb-IIIa in end-stage renal
disease. J Am Soc Nephrol. 1994 5: 36-46.
16. Elliott MJ, Zimmerman D, Holden RM. Warfarin anticoagulation in
hemodialysis patients: a systematic review of bleeding rates. Am J Kidney Dis. 2007
50: 433-440.
17. Phelan PJ, O'Kelly P, Holian J, et al. Warfarin use in hemodialysis patients: what
is the risk? Clin Nephrol. 2011 75: 204-211.
18. Hiremath S, Holden RM, Fergusson D, Zimmerman DL. Antiplatelet
medications in hemodialysis patients: a systematic review of bleeding rates. Clin J Am Soc Nephrol. 2009 4: 1347-1355.
19. Savazzi GM, Cusmano F, Musini S. Cerebral imaging changes in patients with chronic renal failure treated conservatively or in hemodialysis. Nephron. 2001 89: 31-
36.
20. Wijdicks EF, Torres VE, Schievink WI. Chronic subdural hematoma in
autosomal dominant polycystic kidney disease. Am J Kidney Dis. 2000 35: 40-43.
21. Rossier A, Pruijm M, Hannane D, Burnier M, Teta D. Incidence, complications and risk factors for severe falls in patients on maintenance haemodialysis. Nephrol Dial Transplant. 2012 27: 352-357.
22. Boudville N, Inderjeeth C, Elder GJ, Glendenning P. Association between 25-
hydroxyvitamin D, somatic muscle weakness and falls risk in end-stage renal failure.
Clin Endocrinol (Oxf). 2010 73: 299-304.
23. Desmet C, Beguin C, Swine C, Jadoul M. Falls in hemodialysis patients:
prospective study of incidence, risk factors, and complications. Am J Kidney Dis.
2005 45: 148-153.
24. Collins AJ, Foley RN, Herzog C, et al. Excerpts from the US Renal Data System
2009 Annual Data Report. Am J Kidney Dis. 2010 55: S1-420, A426-427.
25. Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan.
Pharmacoepidemiol Drug Saf. 2011 20: 236-242.
26. Lin CC, Lai MS, Syu CY, Chang SC, Tseng FY. Accuracy of diabetes diagnosis
in health insurance claims data in Taiwan. J Formos Med Assoc. 2005 104: 157-163.
27. Nordio M, Limido A, Maggiore U, Nichelatti M, Postorino M, Quintaliani G.
Survival in patients treated by long-term dialysis compared with the general
population. Am J Kidney Dis. 2012 59: 819-828.
28. Abdel-Rahman EM, Turgut F, Turkmen K, Balogun RA. Falls in elderly hemodialysis patients. QJM. 2011 104: 829-838.
Table 1. Demographic characteristics and comorbidities in the end- stage renal disease patients receiving hemodialysis and the comparison subjects of general population
Variable Control HD p-value
N = 18663 N =4709
Sex n(%) n(%)
Female 9489(50.8) 2396(50.9) 0.99
Male 9174(49.2) 2313(49.1)
Age, mean±SD# 63.4±14.1 63.4±14.1 0.98
<35 646(3.46) 159(3.38) 0.98
35-49 2804(15.0) 702(14.9)
50-64 5897(31.6) 1483(31.5)
65+ 9316(49.9) 2365(50.2)
Follow-up, years 5.48±3.64 3.43±3.23 <0.0001 Comorbidity
CAD 2756(14.8) 1597(33.9) <0.0001
CHF 937(5.02) 1343(28.5) <0.0001
Stroke 1096(5.87) 984(20.9) <0.0001
Hyperlipidemia 4308(23.1) 2215(47.0) <0.0001 Hypertension 8163(43.7) 4205(89.3) <0.0001 Diabetes 2423(13.0) 2197(46.7) <0.0001
Dementia 411(2.20) 163(3.46) <0.0001
AF 446(2.39) 249(5.29) <0.0001
Medication
Warfarin 288(1.54) 251(5.33) <0.0001
Clopidogrel 504(2.70) 630(13.4) <0.0001
Aspirin 5822(31.2) 2923(62.1) <0.0001
Chi-Square Test; #T-test
HD, hemodialysis; CAD, coronary artery disease;
CHF, congestive heart failure AF, atrial fibrillation
Table 2. Incidence rate and hazard of subdural hematoma in patients with end-stage renal disease receiving hemodialysis compared to those without any kidney disease
Hemodialysis to Control
Control Hemodialysis
Variables Event PY Rate# Event PY Rate# IRR* Adjusted HR†
(95% CI) (95% CI)
All 129 102392 12.6 91 16154 56.3 4.47(4.11, 4.86)*** 3.81(2.77, 5.25)***
Sex
Female 52 54099 9.61 39 8663 45.0 4.68(4.16, 5.28)*** 3.64(2.23, 5.94)***
Male 77 48293 15.9 52 7492 69.4 4.35(3.87, 4.90)*** 3.99(2.61, 6.12)***
Age, years
<50 7 23405 2.99 11 4796 22.9 7.67(6.27, 9.38)*** 3.66(0.99, 13.5) 50-64 20 34588 5.78 38 5757 66.0 11.4(9.81, 13.3)*** 8.36(4.14, 16.9)***
65+ 102 44399 23.0 42 5601 75.0 3.26(2.88, 3.70)*** 2.55(1.69, 3.86)***
Rate#, incidence rate, per 10,000 person-years; IRR*, incidence rate ratio; Adjusted HR†: multivariable analysis including age, sex, and co-morbidities of coronary artery disease, congestive heart failure, stroke, hyperlipidemia, hypertension, diabetes, dementia, atrial fibrillation and medications; *p<0.05, **p<0.01, ***p<0.001
Table 3. The risk of subdural hematoma stratified by traumatic status and follow-up years in patients with end-stage renal disease receiving hemodialysis
Control Hemodialysis Hemodialysis to Control
Subdural
hemorrhage Event PY Rate# Event PY Rate# IRR*
(95% CI)
Adjusted HR† (95% CI) Traumatic
Total 101 102392 9.86 59 16154 36.5 3.70(3.39, 4.04)*** 3.53(2.42, 5.16)***
≤1 year 12 17540 6.84 16 3841 41.7 6.09(5.52, 6.71)*** 5.73(2.36, 13.9)***
>1 years 89 84852 10.5 43 12313 34.9 3.33(3.02, 3.68)*** 3.20(2.09, 4.90)***
Non-traumatic
Total 28 102932 2.73 32 16154 19.8 7.24(6.59, 7.96)*** 4.73(2.57, 8.69)***
≤1 year 7 17540 3.99 14 3841 36.4 9.13(8.21, 10.2)*** 6.37(2.27, 17.9)***
>1 years 21 84852 2.47 18 12313 14.6 5.91(5.34, 6.54)*** 3.98(1.86, 8.54)***
Rate#, incidence rate, per 10,000 person-years; IRR*, incidence rate ratio; Adjusted HR†: multivariable analysis including age, sex, and co-morbidities of coronary artery disease, congestive heart failure, stroke, hyperlipidemia, hypertension, diabetes, dementia, atrial fibrillation and medications; *p<0.05, **p<0.01, ***p<0.001 ICD-9-CM codes: Traumatic 852.2, 852.3; Non-traumatic 432.1
Table 4. Odds ratio of 30-day mortality of subdural hematoma for the hemodialysis cohort compared to the control cohort
Control Hemodialysis Hemodialysis to Control
n/N(%) n/N(%) Crude OR(95% CI) AdjustedORs†(95% CI)
All 11/129(8.5) 32/91(35.2) 5.82(2.74, 12.4)*** 6.34(2.37, 16.9)***
≤1 year 3/19(15.8) 11/30(36.7) 3.09(0.73, 13.0) 3.07(0.47, 20.1)
>1 years 8/110(7.27) 21/61(34.4) 6.69(2.74, 16.3)*** 9.49(2.81, 32.0)***
Traumatic 9/101(8.91) 17/59(28.8) 4.14(1.71, 10.0)*** 4.36(1.36, 14.1)***
Non-traumatic 2/28(7.14) 15/32(46.9) 11.5(2.32, 56.6)*** 19.4(2.47, 151.7)***
Adjusted ORs†: adjusted for age, sex, and co-morbidities of coronary artery disease, congestive heart failure, stroke, hyperlipidemia, hypertension, diabetes, dementia, atrial fibrillation and medications; *p<0.05, **p<0.01, ***p<0.001
Legends
Figure 1. The cumulative incidence of subdural hemorrhage in incident end-stage renal disease patients receiving hemodialysis (dashed line) and subjects without any kidney disease (solid line).
Figure S1. Annual age-standardized incidence rate of subdural hemorrhage in prevalent end-stage renal disease patients receiving hemodialysis from 1998 to 2010.