行政院國家科學委員會補助專題研究計畫 ■ 成 果 報 告
□期中進度報告
Treating Postpartum Depressive Disorder –
A Prospective Study of Patients’ Choices of Antidepressants, Their Side-effects and Treatment Responses
產後憂鬱症之治療--病患對於抗鬱劑副作用之選擇、耐受及療效探討
計畫類別:■個別型計畫 □ 整合型計畫 計畫編號:NSC 92-2314-B-038-053-
執行期間:2003.08.01 至 2005.07.30
計畫主持人:沈武典 共同主持人:鄧惠文 計畫參與人員:
成果報告類型(依經費核定清單規定繳交):■精簡報告 □完整報告 本成果報告包括以下應繳交之附件:無
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:臺北醫學大學精神科
中 華 民 國 94 年 10 月 30 日
I
中文摘要:
背景:台灣婦女產後憂鬱症盛行率約為12%,但其中僅少數病患願意接受醫療。由於產後
憂鬱症常併有焦慮症狀,選用可同時增加中樞神經之血清胺素(5-HT)及去甲基腎上腺素 (NE)之抗鬱劑(venlafaxine [Efexor], moclobemide [Aurorix] 或 mirtazapine [Remeron])應 能獲致療效,但此三種藥物各具某些副作用。產後婦女處於特殊之身體及心理狀態,對於 抗鬱藥物之副作用可能有特殊顧慮及耐受性問題,影響治療意願及治療效果。現有之抗鬱 劑副作用知識並非針對產後憂鬱族群研究所得,台灣婦女的心理或體質特性也未被探討。
目的:本計畫為一前瞻性研究。目的為(一)探討產後憂鬱症之臨床表現 (二)提供病 患主動選擇抗鬱劑種類的治療模式,藉以瞭解產後憂鬱症婦女對抗鬱劑副作用之顧慮與選 擇 (三)評估三種抗鬱劑用於治療產後憂鬱症時之副作用及療效。
研究設計與方法:以台灣版愛丁堡產後憂鬱量表(the Taiwanese Version of the Edinburgh Postnatal Depression Scale)篩檢產後憂鬱症個案,經精神科專科醫師確認診斷後收案。
個案接受對於三種抗鬱劑(venlafaxine [Efexor], moclobemide [Aurorix] 及 mirtazapine [Remeron])副作用之說明後,依其意願選擇一種起始藥物。後續四個月中安排六次追蹤評 估,內容包括憂鬱、焦慮症狀,副作用及療效,使用貝氏憂鬱/焦慮量表、漢米爾頓憂鬱/
焦慮量表及研究團隊所設計之藥物副作用評估問卷。
結果:產後憂鬱症婦女在開始治療之前,對於三種抗鬱藥物的選擇機會平均。開始治療後,
三種藥物都能顯著減少憂鬱症狀,但本研究中,僅使用Aurorix 及 Efexor XR 的兩組達到
完全緩解。Aurorix 的主要副作用為增加睡眠時間。Efexor XR 為口乾、噁心及便秘。
Remeron 的副作用為體重增加、暈眩感、作夢增加。
II
Abstract
Background: Postpartum depression (PPD) affects about 12% of childbearing women but is
seriously under-recognized and under-treated. Three antidepressants (venlafaxine [Efexor], moclobemide [Aurorix] and mirtazapine [Remeron]) which can improve both serotonin and norepinephrine transmission in the central nervous system, are effective in treating depressive disorders with anxiety symptoms although each of them has some distinct side effects.Therefore, it is thought that these antidepressants can benefit PPD patients. However, they are physically and psychologically distinct from non-puerperal patients. Pharmacological
knowledge specifically concerning the use of antidepressants in PPD patients is still lacking.
Aim: This study is aimed (1) to investigate the symptom profile of postpartum depression
prospectively ; (2) to treat postpartum depression with patients’ active participation in choosing their own antidepressants in order to explore patients’ concerns about medications’ side effects ; and (3) to evaluate the side effect profile, tolerability and effectiveness of antidepressants in the treatment of PPDDesign and Methods: PPD subjects are to be recruited with the screening of the Taiwanese
version of the Edinburgh Postnatal Depressive Scale first and then to be confirmed by psychiatric specialists. Each subject will receive a standardized version of explaining the possible side effects of 3 antidepressants (venlafaxine, moclobemide and mirtazapine) and choose one of them as her starting medication. The subjects are to be evaluated for 6 times in the following 4 months. The evaluation instruments include BDI, BAI, semi-structured questionnaire about side-effects, HAM-D and HARS.Results:
Their choices were almost equally distributed to the three antidepressants: 30 (32.6%) for moclobemide (Aurorix); 30 (32.6%) for venlafaxine (Efexor XR); 28 (30.4%) for mirtazapine (Remeron).
During the 4 months of treatment, all the four antidepressants revealed effectiveness in reducing depressive symptoms. However, only subjects treated with Efexor XR and Aurorix had full remission of depression (HAM-D score<7) at the end of follow-up.
The most common side effects of Aurorix are increased duration of sleep. Efexor XR causes prominent gastro-intestine problems, such as nausea/vomiting and constipation. Reduced salivation is another common side effect of Efexor. Patients reported a wide range of side effects with Remeron. The major complaints are weight gain, sleepiness, dizziness and increased dream activities.
II
A. Specific aims:
1. To investigate the symptom profile of postpartum depression (PPD) prospectively ; 2. To treat postpartum depression with patients’ active participation in choosing
antidepressants in order to explore patients’ concerns about side effects of antidepressants; and
3. To evaluate the side effect profile, tolerability and effectiveness of antidepressants in the treatment of PPD
4. To compare PPD patients with the non-puerperal counterparts and to highlight their special needs in the treatment of depression.
B. Background:
The problem of under-treatment of postpartum depressive disorder :
Postpartum depression (PPD) affects 10% to 22% of childbearing women all over the world (Abou-Saleh et al, 1997; Alexis et al, 1997; Lee et al, 1998). In our previous study (NSC-90-2314-B-038-020), the prevalence of postpartum depressive disorders among Taiwanese women is about 12% (Teng et al, 2005)Untreated maternal depression has negative impacts on mother’s health and infant’s development (Breznitz and Friemanl, 1988). Unfortunately, only a small portion of
depressed mothers receive psychiatric treatment. Some of them are not aware that they are suffering from a treatable disease. Even being aware of that, most women are still reluctant of taking antidepressants. Most participants in our previous study are afraid of unexpected side effects of antidepressants as the first reason of refusing to take any medication.
Specific concerns in treating PPD with antidepressants :
Until recently, the treatment of PPD has not been a research topic because most clinicians considered that PPD the same as non-puerperal depression. Pharmacological knowledge specifically concerning the use of antidepressants in PPD patients is still lacking. Therefore, the clinicians do not address and manage the specific characters and needs of women with PPD.
Women with PPD are physically and psychologically distinct from non-puerperal patients.
For examples, many postpartum women are eager to lose weight and restore their ideal body shape. They have to wake up at night to feed or check the baby. They may still suffer from postpartum sequelae such as sleep disturbances, fatigue or problems in engaging sexual activity, and what not. These factors may influence their preference, response and
1
tolerability of antidepressant treatment.
Furthermore, women with PPD frequently have severe anxiety symptoms (Epperson, 1999). In our previous study (NSC-90-2314-B-038-020), 67% of the PPD patients also met the DSM-IV criteria of anxiety disorders (American Psychiatric Association 1994).
Pharmacological background of antidepressants : 1. The action of mechanism of an antidepressant
The oversimplified version of action of mechanism in having depressive/anxiety symptoms is due to the decreased level of the brain-derived neurotrophic factor (BDNF).
The surrounding neurons become aptosis and death if the BDNF level in the neucleus is not adequate.
The body of a person under acute or chronic stress has increases cortisone, which
destroys BDNF directly in the central nervous system causing depressive/anxiety symptoms among those genetically vulnerable people. Those who have poor or barely enough BDNF production would become symptomatic if under cortisone influence in the CNS (Young 2001). The logical approach is to use an inhibitor to reduce the release of
corticotropin-releasing factor (CRF). But the use of a CRF inhibitor is to be realized in the future because it is still under pre-clinical or early phase of clinical investigation.
Now treating depressive /anxiety symptoms is still targeting on improving
neurotransmission of monoamines (i.e., serotonin [5-hydroxytryptaphan and/or 5-HT] and norepinephrine [NE]) within the CNS synaptic gaps. After the postsynaptic 5-HT and/or NE receptors are coupled with the monoamine transmitters, a series of intracellular molecular reactions takes place in G-proteins, the second messengers, the third messengers, etc. Then, cAMP-regulatory element binding (CREB) inside the nucleus is increased, and further in turns stimulates the production of BDNF that can vitalize the cells and prevent their apoptosis (Young 2001).
The monoamine hypothesis of depressive/anxiety symptoms is thought that dysregulation or inadequacy of the CNS monoamines (5-HT or NE) leads to these disorders (Schildkraut 1965). Treatment with an antidepressant can improve the synaptic monoamine
neurotransmission, resulting in increasing BDNF production in the nucleus.
2. The classification systems of antidepressants
Table 1 is a list of antidepressants which are classified into three categories according to their psychopharmacologic action.
As shown in Table 1, medications in Category I, “reuptake inhibitors,” do not increase the total CNS levels of 5-HT and NE, but increase the concentration only in the synaptic gaps and increase their bioviability of their transmission by having more time to stimulate 2
the postsynaptic receptors. Medications in Category II, “oxidase inhibitors,” prevent the destruction (through deamination) of monoamine oxidase inside the presypnatic neuron, resulting in increasing the total CNS concentration of 5-HT and NE and further in improving monoamine neurotransmission. Medications in Category III, “receptor modulators” not only increase the monoamine transmission, but also block specific postsynaptic receptor resulting in modifying the side effect profile of the medications.
Table 1 Pharmacological Classification of Antidepressants
I. M onoamine reuptake inhibitors:
1. Serotonin and norepinephrine reuptake inhibitors a. Tricyclic antidepressants (e.g., imipramine, doxepin) b. Tetracyclic antidepressants (e.g., maprotiline) c. Bicyclic antidepressants (e.g. venlafaxine)
2. Selective serotonin reuptake inhibitors (SSRI, e.g., fluoxetine)
3. Norepineprine and dopamine reuptake inhibitors (NaDRI, e.g. bupropion)
II. M onoamine oxidase inhibitors (MAOI) 1. Traditional MAOIs (e.g. phenelzine)
2. Reversible inhibitor of monoamine inhibitor A (RIMA, e.g. moclobemide)
III. M onoamine receptor modulators
1. Serotonin receptor modulator (e.g. trazodone、nefazodone)
2. Norepinephrine and specific serotonin antidepressant (e.g. mirtazapine)
Abbreviated from Shen WW. Clinical Psychopharmacology for the 21st Century (in Madarine). Taipei: Hochi Publishing Co., 2002
Figure 1 is the clinical classification of antidepressants based on which monoamine (5-HT or NE) can be transmitted. Figure 1 lists only those antidepressants available in Taiwan can be easily prescribed up to an adequate therapeutic dose.
¶
B u p rop ion
5 -H T N E
*A ls o im p ro v es in D A tra nsm issio n
†H ig h d os e im p ro v es N E tra nsm issio n
¶Its m eta b o lite a lso im p ro v es D A tra nsm issio n
V en lafa x in e M oclo b em id e M irtazap in e Flu o xetin e
*S ertralin e
†
P aroxetin e Flu v ox am in e C italop ram
5 -H T + N E
Figure 1. Clinical Classification of Antidepressants (Reprinted from Shen. WW. Clinical Psychopharmacology for the 21st Century-Revised [in Madarine].Taipei: Hochi Publishing Co., in press)
3
3. The relationship of 5-HT/NE and antidepressant/anxiety disorders
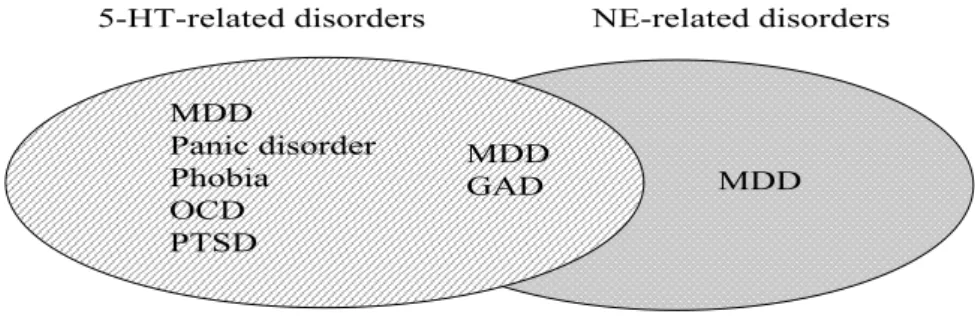
Figure 2 lists the relationship of 5-HT/NE and depressive/anxiety disorders. An
antidepressant can treat all subtypes DSM-IV anxiety disorders except generalized anxiety disorder (GAD), which needs the increase in both 5-HT and NE neurotransmission. As shown in Figure 2, the pathophysiology of major depressive disorder is caused by the dysregulation or deficiency of either 5-HT or NE or both.
MDD
GAD MDD
5-HT-related disorders NE-related disorders
Adapted and expanded from: Healy D, et al. J Psychopharmacol 1997; 11 (Suppl): S25-S31
MDD
Panic disorder Phobia
OCD PTSD
Figure 2 Dysregulation of Neurotransmitters Involved in Depressive/Anxiety Disorders. (Adapted and expanded from: Healy D, et al. J Psychopharmacol 1997; 11 (Suppl): S25-S31)
By this classification, the patients with panic disorder, phobia, obsessive-compulsive disorder, posttraumatic stress disorder can be treated with an SSRI (i.e., fluoxetine,
paroxetine, sertraline, fluvoxamine or citalopram) as well as those listed under in the middle related to both 5HT + NE (i.e. venlafaxine, moclobemide or mirtazapine) as shown in Figure 1. But patients with GAD and with some subtype of major depressive disorder need an antidepressant with the potential of increasing 5-HT and NE instead of increasing only 5-HT.
As shown in Figure 1 and Figure 2, SSRIs can improve only 5-HT transmission, whereas as venlafaxine (Efexor, Thase 1998), moclobemide (Aurorix, Shen 2002) and mirtazapine (Remeron, Holm and Markham, 1999).can improve both 5-HT and NE CNS
neurotransmissions. Referring from the literature (Thase 1998), we hypothesize those three antidepressants (but not any SSRIs) are thought to be more appropriate and/or effective for patients with PPD and PPD with anxiety symptoms.
As shown in Figure 2, three antidepressants (venlafaxine, moclobemide and mirtazapine) can be used clinically to treat all kind of depressive/anxiety disorders except a certain subtype of patients with major depressive disorder. In this case, there is no need to consider the use on any SSRIs as the first choice in clinical decision.
4
4. The side effects of antidepressants
Tricyclic antidepressants (TCAs) have anticholinergic side effects (memory disturbance, learning disturbances, dryness of the mouth, urination incontinence, blurred vision, cardiac conduction disturbances with the potential of fetal death if overdosed, etc.),
antihistaminergic side effects (sedation, drowsiness, weight gain, etc.) and alpha1
antiadrenergic side effects (postural hypotension, delayed ejaculation, dizziness, sedation, etc).
Now TCAs are obsolete due to the advent of newer antidepressants as listed in Figure 1.
Except bupropion, all antidepressants have the serotonergic side effects which consist of (Clayton and Shen, 1998). :
(1) GI side effects (nausea, upset stomach, appetite disturbances, diarrhea, constipation, etc.)
(2) CNS side effects (agitation, nervousness, tremors, sleep disturbances, vivid dreams, etc)
(3) Sexual side effect (decreased libido, erectile disturbance, difficulty in lubrication, delayed orgasm, etc) (This topic is currently under a separates [NSC
91-2314-B-038-018] by Shen WW, Pan JJ, Chiu FY.)
For the simplicity, Table 2 classifies the side effects of three 5-HT/NE antidepressants (venlafaxine, moclobemide, and mirtazapine) into four categories with different severity:
Table 2 The Side Effects of Three 5-HT/NE Antidepressants
A ntidepressant Side effects W eight Sexual N ausea gain Insomnia Sedation dysfunction
V enlafaxine + + – + – + +
M oclobemide + + + + – + + M irtazapine – + + – + + –
C. Research design and methods:
1. Subjects:
Recruitment of patients with PPD
The subjects will be recruited from the Outpatient Clinics of obstetrics/gynecology, pediatrics and psychiatry in Taipei Medical University-Wan Fang Hospital. The research
5
assistants make first contact with the postpartum women and introduce this study. After obtaining the informed consent, the Taiwanese version of the Edinburgh Postnatal Depression Scale (T-EPDS) which was developed in our previous study will be applied.
The subjects who scored above 12 points on T-EPDS will be invited to visit psychiatric Outpatient Clinics and receive antidepressant treatment after the confirmation by a psychiatric specialist. The expected number of cases is 100.
2. Initial assessment:
The subjects will be assessed with the following instruments:
(1) Questionnaires about their basic socio-demographic, obstetric and physical conditions
(2) the 21-item Beck Depression Inventory (BDI) ( Beck et al, 1961) (3) the Beck Anxiety Inventory (BAI) ( Beck et al, 1988a)
(4) the Hamilton Rating Scale for Depression (HAM-D) (Hamilton, 1960) and the Hamilton Anxiety Rating Scale (HARS) (Hamilton, 1959), by trained psychiatric professions
3. Patient’s choice of antidepressant:
Before prescribing medication, the subjects are oriented with the common side effects of three antidepressants--venlafaxine (Efexor), moclobemide (Aurorix) and mirtazapine (Remeron). They are allowed to choose one of the three antidepressants as the “starting”
medication. Then the clinician gives prescription according to the subject’s choice of antidepressants, with standard dose schedule.
To unify the explanations made by different staffs and for different subjects, the contents of explanations are stipulated to follow an education pamphlet developed in advance.
4. Data collection schedules and follow-ups:
During the course of treatment, the subjects will be asked to return to the OPD every two weeks for twice, and then once per month for three times. On each visit, the subject is assessed with:
(1) BDI and BAI
(2) Semi-structured questionnaires about side-effects (3) HAM-D and HARS by trained professions
The decisions of how to adjust medication will be left to the clinicians who are in charge of these subjects. The reasons of changing or discontinuation of antidepressants will be assessed and recorded with details.
D. Data Analysis:
We have access to statistical computer soft wares SPSS at our institution (Taipei Medical University). The data of medication side effects, rating scores, etc. are to be presented with regular descriptive statistics.
6
The categorical variables (such as the presence or absence of a side effect) of the data will be analyzed with chi-square, whereas the continuous variables (the scores from rating scales) will be compared with t-test. The differences are considered to be significant, p is greater than 0.05.
E. Result
1. The PPD women’s choices for antidepressants based on the discrimination of their side effects
During the period of research, 92 women with postpartum depressive disorder were enrolled in this study. They completed the initial evaluation and chose their antidepressants after they received orientations about the possible side effects of each antidepressant.
Their choices were almost equally distributed to the three antidepressants: 30 (32.6%) for moclobemide (Aurorix); 30 (32.6%) for venlafaxine (Efexor XR); 28 (30.4%) for
mirtazapine (Remeron). 4 of them wouldn’t accept any of the three antidepressants, for them fluoxetine was prescribed.
2.The effectiveness of different antidepressants
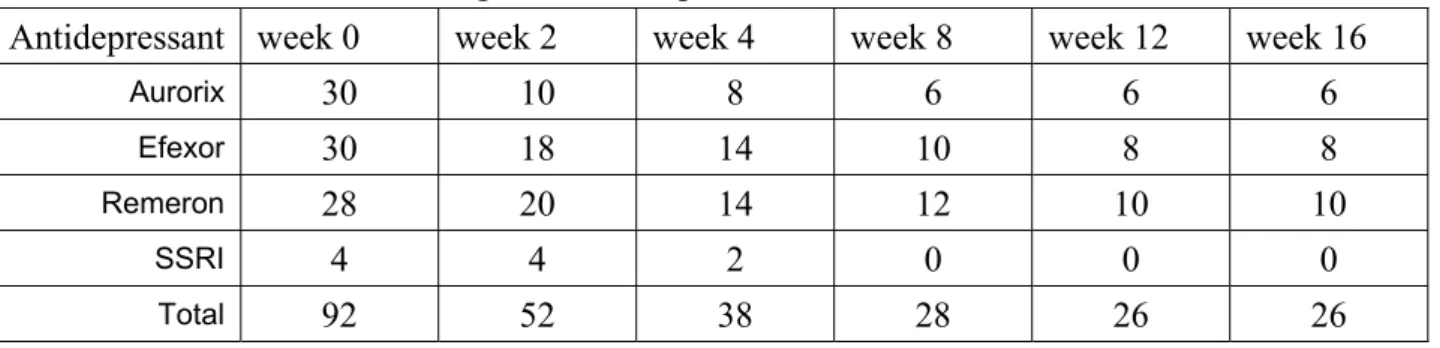
Table 3 shows the number of cases in each follow-up visit. The drop out rate is high for all the three kinds of antidepressant.
Table 3. Case numbers during the follow-up:
Antidepressant week 0 week 2 week 4 week 8 week 12 week 16
Aurorix
30 10 8 6 6 6Efexor
30 18 14 10 8 8Remeron
28 20 14 12 10 10SSRI
4 4 2 0 0 0Total
92 52 38 28 26 26
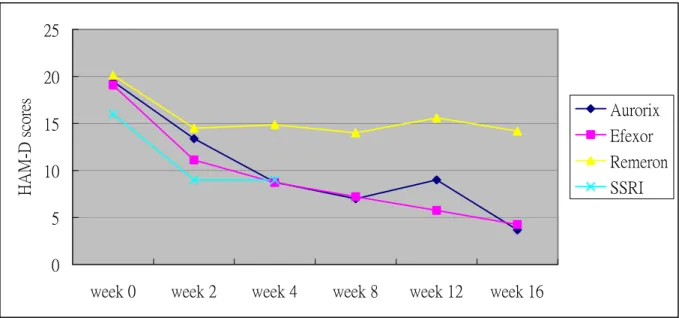
HAM-D scores and antidepressants
Fig. 3 shows the change of mean HAM-D scores of subjects using different antidepressants.
During the 4 months of treatment, all the four antidepressants revealed effectiveness in reducing depressive symptoms. However, only subjects treated with Efexor XR and Aurorix had full remission of depression (HAM-D score<7) at the end of follow-up.
7
0 5 10 15 20 25
week 0 week 2 week 4 week 8 week 12 week 16
H A M -D scores
Aurorix Efexor Remeron SSRI
Fig. 3. Mean HAM-D scores of subjects using different antidepressants.
HARS scores and antidepressant
Fig. 4 shows the change of mean HARS scores of subjects using different antidepressants.
0 5 10 15 20 25
week 0 week 2 week 4 week 8 week 12 week 16
HA RS sc or es Aurorix
Efexor Remeron SSRI
Fig. 4. Mean HARS scores of subjects using different antidepressants.
3.The side effects of dual-mechanism antidepressants
Fig 5~7 showed the side effects reported by PPD women using different antidepressants at the second visit. (Only symptoms coded >= 2 on UKU rating scale are counted as a
8
significant side effects).
Aurorix:
Discussion
The specific characters and needs of PPD women when they receive treatment
Fig.5
Efexor XR:
Side effects of Efexor XR
0 5 10 15 20 25
sleepiness increased duration of sleep
reduced duration of sleep
reduced salivation nausea/vomiting constipation
% 數列1
Fig.6
Remeron:
Side effects of Remeron
0 5 10 15 20 25 30 35
sl ee pi ne ss F ail in g me mo ry te ns io n in cr ea se d dur at io n of sl ee p re du ce d dur at io n of sl ee p in cr ea se d dr ea m ac ti vi ty em ot io na l in di ff er en ce re du ce d sa li va ti on co ns ti pa ti on or th os ta ti c di zz in es s sk in r as h pr ur it is we ig ht g ai n ps yc hi c de pe nd en ce
%
Fig.7
9
Side effects of Aurorix
0 10 20 30 40 50
Increased duration of
sleep
Akathisia parasthesis increased salivation
reduced salivation
constipation orthostatic dizziness
pruritis amenorrhea
%
The most common side effects of Aurorix are increased duration of sleep, some neurologic symptoms like akathisia and parasthesis. Compared to Aurorix, Efexor XR causes prominent gastro-intestine problems, such as nausea/vomiting and constipation. Reduced salivation is another common side effect of Efexor. Patients reported a wide range of side effects with Remeron. The major complaints are weight gain, sleepiness, dizziness and increased dream activities.
Reference
Abou-Saleh, M T.(1997). Postpartum psychiatric illness in Arab culture. Arab Journal of
Psychiatry. Vol 8(1) May 1997
Alexis M, Llewellyn, Zachary N, Stoew, Charles B, Nemeroff CB (1997) Depression during pregnancy and puerperium. Journal of Clinical Psychiatry, 58: 26-32.
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders, The Fourth Edition (DSM-IV), Washington DC: American Psychiatric Association.
Breznitz Z, Friedman SL (1988) Toddlers’ concentration: does maternal depression make a difference? Journal of Child Psychology and Psychiatry, 29: 267-279
Clayton DO, Shen WW (1998). Psychotropic drug-induced sexual function disorders, diagnosis, incidence, and management. Drug Safety, 9: 299-312.
Cox J L, Holden JM, Sagovsky R. (1987) Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry 1987;150:782-786.
Epperson CN, (1999). Postpartum Major Depression: Detection and Treatment. American Family Medicine, Vol 59(8): 2247-2254
Holm KJ, Markham A (1999). Mirtazapine: a review of its use in major depression. Drugs, 57:
607-631.
Lee DTS, Yip ASK, Chiu HFK, Leung TYS, Chan KPM, Chau IOL, Leung HCM, Chung TKH.
(1998). Detecting postnatal depression in Chinese women validation of the Chinese version of the Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 172: 433-437.
Misri, Shaila; Kostaras, Xanthoula; Fox, Don; Kostaras, Demetra.(2000) The impact of partner support in the treatment of postpartum depression. Canadian Journal of Psychiatry, 45, 554-558.
O’Hara MW. (1991) Postpartum mental disorders. In: Droegemeuller W, Sciarra J. (eds).
Gynecology and Obstetrics. Philadelphia, Pa: Lippincott.
Schildkraut JJ (1965). The catecholamine hypothesis of affective disorders: a review of supporting evidence. American Journal of Psychiatry, 122: 509-522.
10
Shen. WW (2002) Clinical Psychopharmacology for the 21st Century-Revised, (in Madarine).Taipei: Hochi Publishing Co.
Shen. WW. (in press) Clinical Psychopharmacology for the 21st Century-Revised, in Madarine].Taipei: Hochi Publishing Co.
Small, Rhonda; Brown, Stephanie; Lumley, Judith; Astbury, Jill. (1994) Missing voices: What women say and do about depression after childbirth. Journal of Reproductive & Infant
Psychology. Vol 12(2), 89-103.
Teng HW, Hsu CS, Shih SM , Lu ML,Pan JJ, Shen WW. Screening postpartum depression with the Taiwanese version of the Edinburgh Postnatal Depression Scale. Comprhensive psychiatry.
2005; 46:261-265
Thase ME (1998). Effects of venlafaxine on blood pressure: a meta-anlysis of original data from 3744 depressed patients. Journal of Clinical Psychiatry, 59: 502-508.
Young LT (2001). Postreceptor pathways for signal transduction in depression and bipolar disorder. Journal of Psychiatry and Neuroscience, 26 (suppl): S17-S22.
11
![Figure 1. Clinical Classification of Antidepressants (Reprinted from Shen. WW. Clinical Psychopharmacology for the 21st Century-Revised [in Madarine].Taipei: Hochi Publishing Co., in press)](https://thumb-ap.123doks.com/thumbv2/9libinfo/7373880.92349/6.892.217.657.806.955/clinical-classification-antidepressants-reprinted-clinical-psychopharmacology-madarine-publishing.webp)