Brief communication
Quality of life of lung cancer patients: Validation of the Taiwan Chinese
version of the EORTC QLQ-C30 and QLQ-LC13
Wei-Chu Chie1, Chih-Hsin Yang2, Chiun Hsu2& Pan-Chyr Yang3
1
School of Public Health and Graduate Institute of Preventive Medicine, College of Public Health, National Taiwan University (E-mail: [email protected]);2Department of Oncology;3Internal Medicine, National Taiwan University Hospital, Taiwan
Accepted in revised form 24 December 2002
Abstract
The purpose of this study was to test the validity and reliability of the Taiwan Chinese translation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 (EORTC QLQ-C30, version 3) and Quality of Life Questionnaire Lung Cancer-13 (QLQ-LC13) ques-tionnaires. Consecutively 51 patients with lung cancer undergoing active chemotherapy and 48 such pa-tients undergoing regular follow-up completed the questionnaires. The intraclass correlation between test and retest ranged from 0.46 to 0.85 for the QLQ-C30 and was 0.76 for dyspnea for the QLQ-LC13. The j coefficients between test and retest ranged from 0.51 to 0.73 for single items of the QLQ-C30 and 0.49–0.68 for five of the nine items in the QLQ-LC13. The Cronbach’s a coefficients were P0.70 for all scales of the two questionnaires apart from that of cognitive functioning. The correlation coefficients between indices measuring similar dimensions of the EORTC QLQ-C30 and the SF-36 questionnaires ranged from 0.43 to 0.73, and that between the dyspnea scales of the two EORTC questionnaires was 0.70. Patients in the follow-up group revealed higher scores of global status/quality of life, and lower scores of nausea/vomiting, as also physical functioning. The questionnaires could also detect expected adverse effects of radiotherapy, cisplatin, and paclitaxel.
Key words: EORTC QLQ-C30, EORTC QLQ-LC13, Lung cancer, Quality of life
Introduction
Lung cancer is a disease that is rapidly increasing in Taiwan [1]. The high case-fatality rate (95.7%) [1] spurred oncologists to develop new therapeutic measures to prolong lung cancer patients’ life [2].
More than 50 instruments measuring quality of life (QOL) for patients suffering from lung cancer emerged from 1970 to 1995 [3]. The Lung Cancer Symptom Scale (LCSS), Functional Assessment of Cancer Therapy-Lung (FACT-L) and the Euro-pean Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 (EORTC QLQ-C30) with Quality of Life Ques-tionnaire Lung Cancer-13 (QLQ-LC13) have good
reliability and validity [3]. The EORTC QLQ-C30 includes 30 questions that measure five function scales, three symptom scales, five single symptom items and financial difficulty. All scales/items are transformed to scores ranging between 0 and 100. For all functioning scales that measure function a higher score represents better QOL; and for all symptom scales/items a lower score means better QOL. Previous studies using this instrument re-vealed high internal consistency in most scales except for cognitive functioning, good inter-scale correlation, good discriminant validity [4], test– retest reliability [5], patient–observer agreement [6] and cross-cultural validity except a low discrimi-nant validity of role functioning scale in Japan [7].
The QLQ-LC13 is a supplementary module to the QLQ-C30 for patients with lung cancer and con-tains 13 questions to measure one symptom scale (dyspnea) and nine single symptom items. A pre-vious study demonstrated good internal consis-tency for the dyspnea scale and good clinical validity for most scores [8].
The only available Chinese translation prior to this study, the Cantonese version of the EORTC QLQ-C30 [9] included vocabulary that differed from the Mandarin typically used in Taiwan. The Standard Chinese version of the QLQ-C30 (ver-sion 2) was available in 1997 and the results of validation were published in 2000 [10]. As a result of the geographical, political and cultural separa-tion of China and Taiwan for over 50 years, each country’s corresponding languages and alphabeti-cal characters have evolved and become somewhat different. Here we present the result of translation and cross-validation of the EORTC QLQ-C30 version 3 and QLQ-LC13 questionnaires for lung cancer patients in Taiwan.
Methods
We followed the EORTC guidelines for the translation procedure and pilot testing of the questionnaire [11]. The Taiwan Standard version (version 1.0) of the SF-36 questionnaire, a generic instrument measuring eight separate dimensions of QOL [12, 13] was used as a comparison instru-ment. The Taiwan Standard version (version 1.0) of the SF-36 questionnaire has demonstrated good reliability and validity in Taiwan [14–17].
We consecutively contacted lung cancer patients undergoing active chemotherapy and undergoing post-therapy follow-up at the out patient clinic of the Department of Oncology of the National Taiwan University Hospital from November 2000 to December 2001 inclusively. Chemotherapy and the concurrent medical treatment data were also collected on patients undergoing active treatment. Written consent was obtained from all study par-ticipants. Patients who declined to participate, or who had participated in other studies or who had elected to amend their treatment plans were ex-cluded. Assuming that the standard deviation of the questionnaire-derived QOL score is 20, the sample size required for each group is 50 subjects
in order to achieve 80% power for detecting a difference of 10 points between two groups at the 5% significant level for a one-sided Z-test. The final participant distribution was 51 for the active treatment group and 48 for the follow-up group after correcting for misclassified patients and the excluding non-eligible patients. The selection of the two known groups was based upon the hy-potheses that patients undergoing chemotherapy typically revealed poorer QOL.
Patients were instructed to complete the ques-tionnaires themselves. However, four patients in the active treatment group and seven patients in the follow-up group who were illiterate were as-sisted by two interviewers fluent in both Mandarin and Taiwanese. The illiterate subjects were kept in the study to maintain the representativeness of the sample. Patients in the follow-up group were re-tested with the same questionnaires 1–2 weeks af-ter the first test, conducted by telephone inaf-terview or by mailing the questionnaires. Test/retest reli-ability of the translated questionnaire was carried out on the follow-up group since their medical condition was expected to be more stable than that of patients in active treatment.
Answers to the three questionnaires were scored according to the instructions and computer pro-grams provided [12, 13, 18]. The test/retest reli-ability was evaluated by intraclass correlation coefficients (ICCs) for each questionnaire-deter-mined dimension, and j value of two repeated tests for single items. Cronbach’s a coefficient was used in order to evaluate the internal consistency of each dimension. The validity of the two ques-tionnaires was examined by Pearson’s correlation coefficients between similar dimensions for the EORTC and the SF-36 questionnaires. The Wil-coxon’s rank sum test was used to examine the difference in scores for each dimension, and the Cochran Mantel–Haenszel test was used to ex-amine differences in single items between the two groups of patients. A p-value of <0.05 was con-sidered as statistically significant.
Results
Patients in the active chemotherapy group (n¼ 51) averaged 54.3 years of age (SD¼ 12.1 years), in-cluded more men (32) than women, had about the
same number with less than a high school educa-tion (22) as with a high school educaeduca-tion or better (29), spoke mostly Mandarin (39) or Taiwanese (39) and had adenocarcinoma or squamous cell cancer. Patients in the follow-up group averaged 55.0 years of age (SD¼ 12.4 years), included al-most equal numbers of men and women, had the same number with less than or at least a high school education (24), spoke mostly Taiwanese (38) and had mostly adenocarcinoma (32).
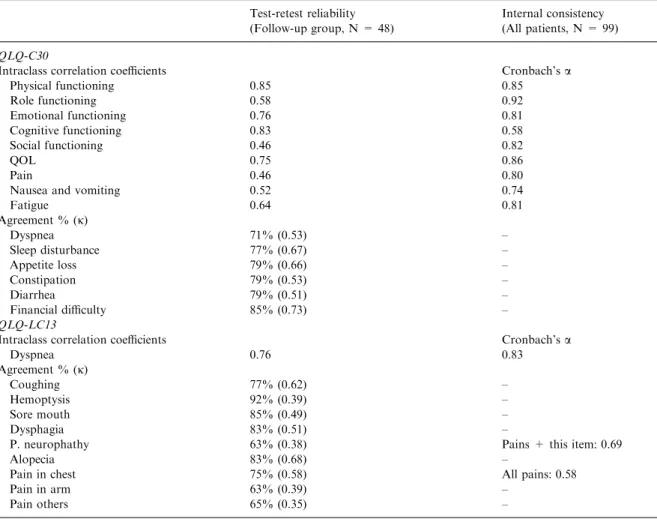
The ICCs were moderate to high in most scales (r¼ 0.46–0.85 for the QLQ-C30 and 0.76 for dyspnea of the QLQ-LC13). The j coefficients for and single items were moderate for the QLQ-C30 (j¼ 0.51–0.73) and also for five items in the QLQ-LC13 (j¼ 0.49–0.68), but low for the remaining four items of the QLQ-LC13 (hemoptysis, peri-pheral neuropathy, pain in arm and pain in other
part, j¼ 0.35–0.39). All Cronbach’s a coefficients for scales of the QLQ-C30 and the dyspnea scale of the QLQ-LC13 were satisfactory (P0.70) apart from that coefficient for cognitive functioning (a¼ 0.58). The Cronbach’s a coefficient of pain-related questions was only 0.58, while that for peripheral neuropathy plus pain questions was 0.69 (Table 1).
The physical functioning, emotional functioning and pain scales of the QLQ-C30 were highly cor-related (r P 0:70) with scales measuring the same domains in the SF-36. The dyspnea scale of the QLQ-LC13 was highly correlated (r¼ 0.70) with the single item of dyspnea (short of breath) of the QLQ-C30. Correlation coefficients between the remaining pairs of scales were moderate (r¼ 0.43– 0.63). The follow-up group demonstrated a higher score for the QOL scale, a lower score for the
Table 1. Reliability of the EORTC QLQ-C30 and the EORTC QLQ-LC13
Test-retest reliability Internal consistency (Follow-up group, N = 48) (All patients, N = 99) QLQ-C30
Intraclass correlation coefficients Cronbach’s a
Physical functioning 0.85 0.85 Role functioning 0.58 0.92 Emotional functioning 0.76 0.81 Cognitive functioning 0.83 0.58 Social functioning 0.46 0.82 QOL 0.75 0.86 Pain 0.46 0.80
Nausea and vomiting 0.52 0.74
Fatigue 0.64 0.81 Agreement % (j) Dyspnea 71% (0.53) – Sleep disturbance 77% (0.67) – Appetite loss 79% (0.66) – Constipation 79% (0.53) – Diarrhea 79% (0.51) – Financial difficulty 85% (0.73) – QLQ-LC13
Intraclass correlation coefficients Cronbach’s a
Dyspnea 0.76 0.83 Agreement % (j) Coughing 77% (0.62) – Hemoptysis 92% (0.39) – Sore mouth 85% (0.49) – Dysphagia 83% (0.51) –
P. neurophathy 63% (0.38) Pains + this item: 0.69
Alopecia 83% (0.68) –
Pain in chest 75% (0.58) All pains: 0.58
Pain in arm 63% (0.39) –
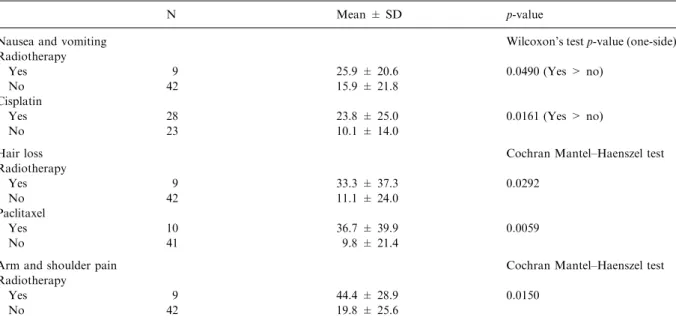
nausea/vomiting scale, and a lower score for physical functioning scale than the active chemo-therapy group. Scores of the two groups did not appear to differ for any other dimensions (Table 2) or single items (not shown in the table). Compared wit patients who did not have the following treatments, patients who underwent radiotherapy and who received cisplatin experienced more nausea and vomiting, patients who received ra-diotherapy experienced more hair loss and arm/ shoulder pain, and patients who received paclitaxel revealed greater level of hair loss (Table 3).
Discussion
The test/retest reliabilities of the questionnaires for the follow-up group in this study were lower than was the case for the 1995 study of Hjermstad et al. [5] but consistent with our previous study on pa-tients with nasopharyngeal carcinoma [19]. Our test/retest interval was within the range suggested by Streiner and Norman [20]. It is possible that a patient’s condition may have changed within the range even for members in the follow-up group. The results for internal consistency in this study
Table 3. Differences in nausea/vomiting scores of patients with and without certain treatments (only significant results were included)
N Mean ± SD p-value
Nausea and vomiting Wilcoxon’s test p-value (one-side)
Radiotherapy
Yes 9 25.9 ± 20.6 0.0490 (Yes > no)
No 42 15.9 ± 21.8
Cisplatin
Yes 28 23.8 ± 25.0 0.0161 (Yes > no)
No 23 10.1 ± 14.0
Hair loss Cochran Mantel–Haenszel test
Radiotherapy Yes 9 33.3 ± 37.3 0.0292 No 42 11.1 ± 24.0 Paclitaxel Yes 10 36.7 ± 39.9 0.0059 No 41 9.8 ± 21.4
Arm and shoulder pain Cochran Mantel–Haenszel test
Radiotherapy
Yes 9 44.4 ± 28.9 0.0150
No 42 19.8 ± 25.6
Table 2. Comparison of QOL scores of each scale in the EORTC QLQ-C30 and QLQ-LC13 among two groups of patients Active chemotherapy N = 51 Mean ± SD Follow-up N = 48 Mean ± SD Wilcoxon’s test p-value (one-side) Physical functioning 79.9 ± 18.3 72.2 ± 22.1 0.0262* (T > F) Role functioning 71.6 ± 25.9 74.7 ± 31.5 NS Emotional functioning 75.8 ± 16.1 75.0 ± 21.0 NS Cognitive functioning 80.4 ± 18.8 78.8 ± 22.0 NS Social functioning 69.3 ± 28.4 76.7 ± 21.4 NS QOL 56.5 ± 19.6 63.2 ± 20.8 0.0449* (F > T) Fatigue 39.2 ± 21.6 34.3 ± 19.7 NS
Nausea and vomiting 17.6 ± 21.7 5.6 ± 11.1 0.0004 (T > F)
Pain 24.8 ± 24.8 19.4 ± 18.3 NS
Dyspnea 20.3 ± 18.3 24.1 ± 21.8 NS
were consistent with the findings of previous studies [4, 7, 8, 10]. We changed the translation peripheral neuropathy (tingling) from ‘pain as having been stung’ to ‘like having been stung with needles’ because of the unexpectedly high Cron-bach’s a coefficient of tingling and pain questions. The moderate to high correlation of similar di-mensions between the QLQ-C30 and the SF-36 and the high correlation between dyspnea scales of the two EORTC questionnaires imply that both EORTC questionnaires exhibited good validity. The scores for the active chemotherapy group of this study were similar to or better than for those of patients during treatment in previous studies [4, 8, 10]. The scores for the follow-up group of this study were similar to the reference values of local or locoregional non-small cell lung cancer pro-vided by the EORTC [21], but better than that of previous studies [4, 7]. The significantly higher scores in the QOL and lower score in the nausea/ vomiting scale of the follow-up group corre-sponded with the finding of Bergmen et al. [8]. The corresponding symptoms of cisplatin (nausea/ vomiting), paclitaxel (hair loss), and radiotherapy (shoulder/arm pain) were consistent with previous knowledge of the adverse effects. The pronounced hair loss experienced by patients undergoing ra-diotherapy was, however, difficult to explain and warrants further investigation.
Acknowledgments
This study was supported by a two-year research grant provided by the National Science Council, Taiwan, no. NSC89-2314-B002-469 and no. NSC89-2320-B-002-096. The authors of this study are grateful to Ms Karen West for her professional help in translation review, Drs Pei-Ching Oon and Fong Liew, Mr Wei-Hua Tan and Mr Jui-Ming Shih for translation, Professor Jen-pei Liu for statistical consultation, as well as Dr Chia-Chi Lin, Ms Chia-Chun Lai, and Mr Ming-Jer Chang for assistance with data collection.
References
1. Department of Health, the Executive Yuan, Cancer Reg-istry Annual Report, Republic of China, 1998. Web-site of Department of Health: www.doh.gov.tw, 2002.
2. Division of Cancer Research, National Health Research Institutes and Taiwan Cooperative Organization of Cancer. Consensus of Diagnosis and Treatment of Lung Cancer. Taipei: National Health Research Institutes, 1998. 3. Montazeri A, Gills CR, McEwen J. Quality of life in
pa-tients with lung cancer. Chest 1998; 113: 467–481. 4. Aaronson NK, Ahmedzai A, Berman B, et al. The
Euro-pean Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in interna-tional clinical trials in oncology. J Natl Cancer Inst 1993; 85: 365–376.
5. Hjerstad MJ, Fossa SD, Bjordal K, Kaasa S. Test/retest study of the European Organization for Research and Treatment of Cancer Core Quality-of-Life Questionnaire. J Clin Oncol 1995; 13: 1249–1254.
6. Groenvold M, Klee MC, Sprangers MAG, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life ques-tionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol 1997; 50: 441–450.
7. Kobayashi K, Takeda F, Teramukai S, et al. A cross-vali-dation of the European Organization for Research and Treatment of Cancer QLQ-C30 (EORTC QLQ-C30) for Japanese with lung cancer. Eur J Cancer 1998; 34: 810–815. 8. Bergman B, Aaronson NK, Ahmedzai S, et al. The EO-RTC QLQ-C13: A modular supplement to the EOEO-RTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. Eur J Cancer 1994; 30A: 635–642. 9. EORTC quality of Life Study Group. Questionnaire for the Department of Obstetric and gynecology, Hong Kong University (Chinese Translation of the EORTC QLQ-C30 version 2.0). Brussels: Quality of Life Unit, EORTC Data Center, 1997.
10. Zhao H, Kanada K. Translation and validation of the Standard Chinese version of the EORTC QLQ-C30. Qual Life Res 2000; 9: 139–137.
11. Cull A, Sprangers M, Bjordal K, et al. EORTC Quality of Life Study Group Translation Procedure. Brussels: EO-RTC Quality of Life Study Group, 1998.
12. New England Medical Center Hospital. IQOLA SF-36 Taiwan Standard Version 1.0. Boston: The Health Institute, New England Medical Center, 1996.
13. Ware JE, Kosinski M, Keller SD. SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Boston: The Health Institute, New England Medical Center, 1994. 14. Chie WC, Huang CS, Chen JH, Chang KJ. Measurement of the quality of life during different clinical phases of breast cancer. J Formos Med Assoc 1999; 98: 254–260. 15. Fuh JL, Wang SJ, Lu SR, Juang KD, Lee SJ. Psychometric
evaluation of a Chinese (Taiwanese) Version of the SF-36 Health Survey amongst middle-aged women from a rural community. Qual Life Res 2000; 9: 675–683.
16. Chiu HC, Chern JY, Shi HY, Chen SH, Chang JK. Physi-cal functioning and health-related quality of life: Before and after total hip replacement. Kaohsiung J Med Sci 2000; 16: 285–292.
17. Wang SJ, Fuh JL, Lu SR, Juang KD. Quality of life differs among headache diagnoses: Analysis of SF-36 survey in 901 headache patients. Pain 2001; 89: 285–292.
18. Fayers P, Aaronson N, Bjordal K, Curran D, Groenvold M. EORTC QLQ-C30 Scoring Manual. 2nd ed. Brussels: EORTC Quality of Life Study Group, 1999.
19. Chie WC, Hong RL, Lai CC, Ting LL, Hsu MM. Quality of life in patients of nasopharyngeal carcinoma: Validation of the Taiwan Chinese version of the EORTC QLQ-C30 and the EORTC QLQ-H&N35. Qual Life Res 2003; 12: 93–98. 20. Streiner DL, Norman GR. Reliability. In Streiner DL, Norman GR (eds). Health Measurement Scales. A Practical Guide to Their Development and Use. Oxford: Oxford Medical, 1994; 79–96.
21. Fayers P, Weeden S, Curran D. EORTC QLQ-C30 Re-ference Values. Brussels: EORTC Quality of Life Study Group, 1998.
Address for correspondence: Wei-Chu Chie, School of Public Health and Graduate Institute of Preventive Medicine, College of Public Health, National Taiwan University, Room 209, 19 Hsuchow Road, Taipei 10020, Taiwan
Phone: +886-2-23920460; Fax: +886-2-23920456 E-mail: [email protected]