國立台灣大學公共衛生學院流行病學與預防醫學研究 所博士論文
Graduate Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University Doctoral Dissertation
泌尿系統微創治療的實證醫療:全人口回溯性世代研究 與網絡統合分析
Evidence-Based Approach in Minimally Invasive Urologic Therapy: Population-Based Retrospective Cohort Study
and Network Meta-Analysis
流行病學與預防醫學研究所 黃士維 Shi-wei Huang 指導教授:簡國龍教授 杜裕康教授
Advisor: Kuo-Liong Chien, M.D; Ph.D.
Yu-Kang Tu, D.D.S; Ph.D.
中華民國 108 年 7 月
July 2019
誌謝
能夠完成博士論文,首先要感謝的是指導教授簡國龍教授和杜裕康教授。這幾年 學業生涯,引導我對流行病學研究的深入了解,使我在這幾年獲益斐淺。在震波 碎石和高血壓的研究中,簡老師追求研究的真善美,懷大志而拘小節,讓我對於 研究及做學問的態度更加嚴謹,也讓論文能夠刊登在好的期刊。杜老師則帶領我 進入網路統合分析領域。老師對學生研究鉅細靡遺的指導,循循善誘的鼓勵,循 序漸進的幫助才能讓我複雜的網路統合分析研究能夠順利的完成。
接著我要感謝博士論文的口試委員,您們給我的建議讓我受益良多,也讓我的博 士論文能夠更完整而嚴謹。還有研究所同學和學長姊,銘杰,怡君,王睿在統計 分析研究上給我的協助。
這段期間時常奔波在醫院及大學兩地,也要感謝台大泌尿部和雲林分院泌尿部的 同仁,他們能夠適時替我分擔繁重及忙碌的臨床工作。感謝蒲永孝教授在論文研 究中給予相當多專業上的建議。
最後謝謝,我最親愛的家人,從小到大都很疼愛我的父母,我最摯愛的妻子-素榕 與兩位寶貝女兒-嘉嘉、甄甄。因為有你們的一路相伴與鼓勵,讓我在家庭生活上 無後顧之憂,得以專心處理學業上的瓶頸。
黃士維 July 2019
摘要
背景與目標
泌尿系統微創治療(minimally-invasive urologic therapy, MIUT)相較於傳統的 開腹手術有較低的手術併發症,且手術後復原也相對快速,在某些疾病的治療如 泌尿道結石、攝護腺肥大等已取代多數的傳統開刀手術,成為病人與醫師的治療 首選。然而 MIUT 在某些層面仍有待解決之問題,因此創新或改良的微創治療手 段仍持續進展。待解問題如:泌尿道結石的病患已知有較高的高血壓、糖尿病風 險,而體外震波碎石是否會增加病患在此兩病症的風險?眾多新的良性攝護腺乏 大手術治療如雷射和雙極電刀已在本世紀初問世,而相對於”黃金治療術式”的經尿 道單極電刀攝護腺括除手術,這些新穎手術是否有超前的療效及安全性?此論文 的主題為使用最實際與合適的流行病學方法,探究這些 MIUT 待解的問題。
方法
高血壓、糖尿病與震波碎石治療已被報導有非常長期的關聯性、又存在著來 自於病患本身預患因子的干擾,因此我們採用台灣全民健保資料庫之世代追蹤研 究資料(nationwide retrospective cohort data),並選取接受過體外震波碎石與輸尿管 鏡碎石術的兩組病人,利用 Cox 比例風險模式及時間相依共變數分析方法比較兩 組病人的長期罹患高血壓和糖尿病風險。另一方面,由於已問世的新型良性攝護 肥大 MIUT 多樣,我們依術式原理與組織清除機制選取了九種攝護腺手術方法,
運用系統性文獻回顧(meta-analysis)篩選針對這九種手術比較的文章、以 Cochrane risk of bias table 來評量文獻品質及 metafunnel 探尋發表誤差;之後採用網路統合 分析、隨機效應泛線性混合模型(random effect generalized linear mixed model)探 討這九種手術的功效和副作用.
結果
在中位期追蹤 74.9 和 82.6 個月後,震波碎石組和輸尿管鏡碎石組分別有 2028 位及 688 位病患得到高血壓。接受體外震波碎石病患比起接受輸尿管鏡碎石手術
的病患,有較高風險得到高血壓(風險比值:1.20, 95%信賴區間 1.10-1.31)。而且
這個風險隨著體外震波碎石的次數增加而增加;接受一次,兩次,三次,四次及 大於五次後的風險比值分別是 1.10 (95% 信賴區間 1.00-1.20), 1.30 (95% 信賴區 間 1.15-1.48), 1.55 (95% 信賴區間 1.31-1.85), 1.70 (95% 信賴區間 1.32-2.19,), 及 2.00 (95% 信賴區間 1.63-2.45)。相對的,糖尿病的風險和震波碎石則沒有相關。
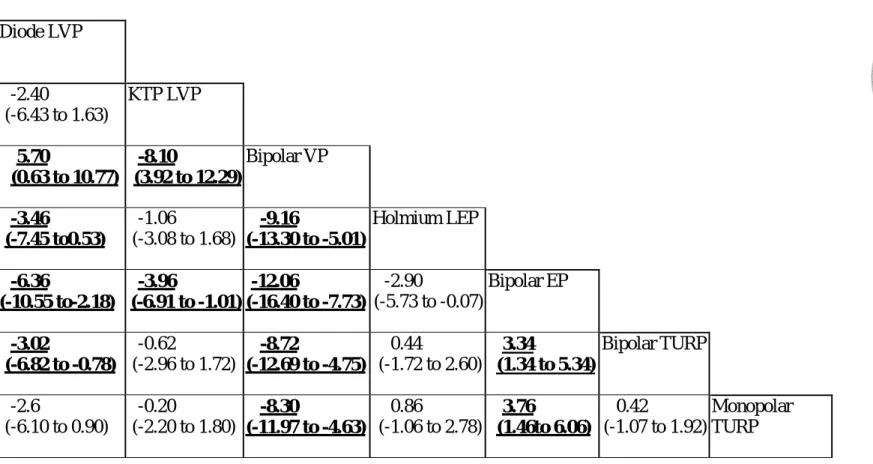
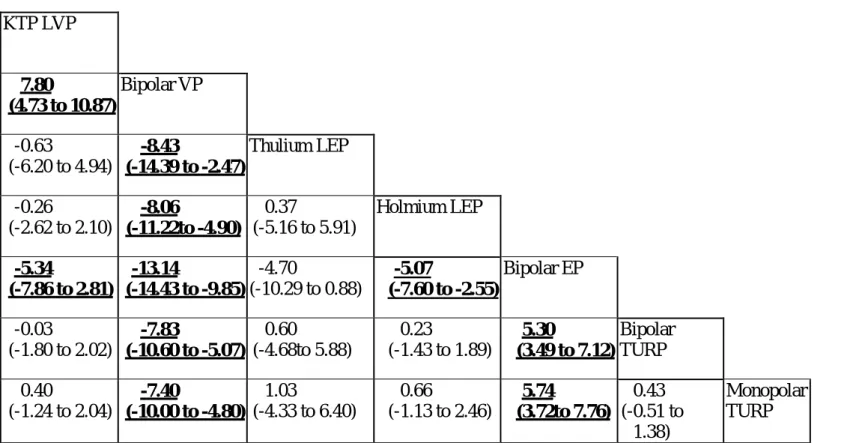
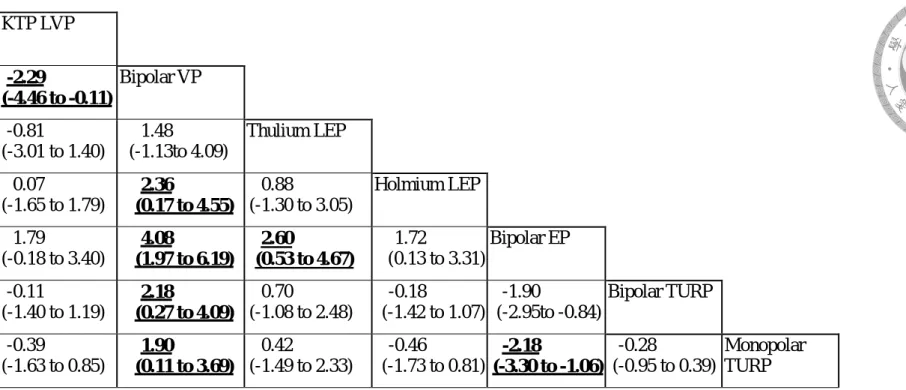
在網路統合分析法研究中,我們分析了 105 個試驗,一共有 13176 位病患。我們 發現剜除手術,在術後 6 個月及 12 個月的最大尿流速和國際攝護腺症狀分數都比 括除和汽化手術好。而且這個差異持續到手術後 24 和 36 個月。在術後 12 個月最 大尿流速中,前 3 名分別為極光雷射攝護腺剜除手術,雙極電刀攝護腺剜除手術 和鈥雷射攝護腺剜除手術,最差的是極光雷射攝護腺汽化術;和單極電刀攝護腺 刮除手術的平均差異分別是 3.15 ml/sec (95%信賴區間 0.63 to 5.67),2.80 ml/sec (95%信賴區間 1.43 to 4.16),1.13 ml/sec (95%信賴區間 0.13 to 2.13)和 -1.90 ml/sec (95%信賴區間 -5.04 to 1.24)。八種新的治療方式都比傳統單極電刀攝護腺括除手 術有較少的出血問題,因此縮短了導尿管放置時間,減少術後血紅素下降,膀胱 血塊塞住事件和輸血比例。但短期尿失禁仍然是剜除手術關切的問題。
結論
研究結果顯示:震波碎石會增加長期高血壓的發險,但是不會增加糖尿病風險;
剜除手術在功效方面表現最好,新手術方式都比傳統單極電刀刮除術安全。
關鍵詞:體外震波碎石,高血壓,攝護腺肥大,雷射,經尿道前列腺括除術,回 溯性世代研究,網路統合分析
Abstract
Background and Objectives
Minimally invasive urologic therapy (MIUT) has reduced surgery-associated complications and facilitates faster recovery compared to conventional open surgeries.
In medical conditions such as urolithiasis and benign prostate hyperplasia (BPH), MIUT has gained preference over conventional treatments. Nevertheless, MIUTs are continuously modified and refined for improvement, and new approaches are being introduced for better surgical outcomes. Although extracorporeal shockwave lithotripsy (SWL) is a favored treatment for urolithiasis, much debate has surrounded its association with long-term risk of hypertension and diabetes. On the other hand, despite monopolar transurethral resection of prostate (TURP) being the gold standard surgical treatment for BPH since the 1970’s, numerous methods including the use of different lasers and bipolar probes have been developed and made available since the start of the century. In the current thesis, we adopted the most appropriate and practical approaches of evidence-based medicine (EBM) to: 1) Study whether SWL will increase the subsequent risk of hypertension and diabetes later in life; and 2) Compare the efficacy and complications of new surgical methods with monopolar TURP.
Methods
To evaluate the reported long-term risk of new-onset hypertension and diabetes, associated with SWL in patients with urolithiasis, we sought to adopt the Taiwanese National Health Insurance Research Database, and a retrospective data collection of
cohorts who either received SWL or ureteroscopic lithotripsy (URSL). A Cox proportional model and Time-varying Cox models were applied to evaluate the association between SWL and the incidence of hypertension or diabetes. Meanwhile, a meta-analysis of publications reporting on any of the nine BPH MIUTs, selected based on the instrumental and resection method, was performed. The Cochrane risk of bias table was applied to appraise the quality of studies, metafunnel to identify publication bias, followed by random effects generalized linear mixed model to compare the efficacy and safety of these different surgical methods for BPH.
Results
After a median follow-up of 74.9 and 82.6 months, 2,028 and 688 patients developed hypertension in the SWL and URSL groups, respectively. Patients who underwent SWL had a higher probability of developing hypertension than patients who underwent URSL, with a hazard ratio (HR) of 1.20 (95% confidence interval 1.10-1.31) after adjusting for covariates. The risk increased as the number of SWL sessions increased, with a HR of 1.10 (95% CI 1.00-1.20, p=0.05), 1.30 (95% CI 1.15-1.48, p<0.001), 1.55 (95% CI 1.31-1.85, p<0.001), 1.70 (95% CI 1.32-2.19, p<0.001), and 2.00 (95% CI 1.63-2.45, p<0.001) in one, two, three, four and more than five SWL sessions, respectively. However, the risk of diabetes was similar between the two cohorts. In network meta-analysis, we identified 105 trials that enrolled a total of 13,176 participants. Nine surgical treatments were evaluated. Enucleation achieved better maximal flow rate (Qmax) and International Prostate Symptom Score (IPSS) than resection and vaporization, at 6 and 12 months after surgery, and the difference was
maintained postoperative up to 24 and 36 months. For 12-month Qmax, the 3 best methods, compared to monopolar TURP, were diode laser enucleation [mean difference (95% Confidence Interval)]: [3.15 (0.63 to 5.67) mL/s], bipolar enucleation [2.80 (1.43 to 4.16) mL/s], and holmium laser enucleation [1.13 (0.13 to 2.13) mL/s]. The worst was diode laser vaporization [-1.90 (-5.04 to 1.24) mL/s]. The eight new methods were all superior in controlling bleeding than monopolar TURP, resulting in shorter catheterization duration, reduced postoperative hemoglobin level declination, fewer blood clot tamponade events, and lower blood transfusion rate. However, short-term transient urinary incontinence was still a concern for enucleation methods. No inconsistency between direct and indirect evidence was detected in either primary or secondary outcomes.
Conclusion
The current thesis found that: SWL increased the long-term risk of new-onset hypertension but not diabetes; new surgical methods for BPH were superior in safety as compared to monopolar TURP: and enucleation methods were the best in primary efficacy. Our thesis demonstrated two best epidemiologic designs to answer contentious issues.
Keywords: shock wave lithotripsy, hypertension, benign prostatic hyperplasia, laser, transurethral resection of prostate, retrospective cohort study, network meta-analysis
Table of contents
誌謝 ... III 摘要 ... IV
背景與目標 ... IV 方法 ... IV 結果 ... V 結論 ... V Abstract ... VI
Background and Objectives ... VI Methods ... VI Results ... VII Conclusion ... VIII
1 Introduction ... 1
1.1Minimally-Invasive Treatments for Urinary Tract Diseases ... 1
1.1.1Extracorporeal Shock Wave Lithotripsy ... 3
1.1.1.1The First-Line Treatment for Urolithiasis with Known Side Effects ... 3
1.1.1.2Hypertension and Diabetes as Long-Term Adverse Effects: Published Evidence ... 5
1.1.2 Minimally Invasive Treatments for Benign Prostate Hyperplasia ... 7
1.1.2.1 Past and Present ... 7
1.1.2.2 Efficacy and Safety of BPH Treatments... 10
1.2 Evidence-Based Medicine ... 12
1.2.1 Nation-wide Retrospective Cohort Studies: Suitable for Studying Long-Term Side Effects Associated with SWL... 13
1.2.2 .. Network Meta-analysis and Systematic Reviews: Fit for Comparing Multiple BPH MIUTs... 15
2 Purpose ... 17
3 Methods and Materials ... 18
3.1 Assessing the Risk of New-Onset Hypertension and Diabetes after Shock Wave Lithotripsy - a Population-Based Retrospective Cohort Study ... 18
3.1.1 Data sources ... 18
3.1.2 Study design and study participants ... 18
3.1.3 Statistical analysis... 19
3.2 Comparative Efficacy and Safety of Surgical Treatments for Benign Prostate Hyperplasia - an Application of Network Meta-Analysis... 23
3.2.1 Data sources and searches ... 23
3.2.2 Study selection ... 24
3.2.3 Data Extraction and quality assessment ... 24
3.2.4 Data synthesis and analysis ... 26
4 Results ... 30
4.1 Assessing the Risk of New-Onset Hypertension and Diabetes after Shock Wave Lithotripsy - a Population-Based Retrospective Cohort Study ... 30
4.1.1 Baseline Characteristics ... 30
4.1.2 New-Onset Hypertension ... 31
4.1.3 New-Onset Diabetes ... 32
4.1.4 Sensitivity Analysis ... 33
4.2 Comparative Efficacy and Safety of Surgical Treatments for Benign Prostate Hyperplasia: an Application of Network Meta-Analysis... 35
4.2.1 Demographics ... 35
4.2.2 Functional outcomes ... 36
4.2.3 Peri-operative parameter... 37
4.2.4 Complications ... 38
4.2.5 Sensitivity analysis and inconsistency ... 39
5 Discussion ... 41
5.1 Assessing the Risk of New-Onset Hypertension and Diabetes after Shock Wave Lithotripsy - a Population-Based Retrospective Cohort Study ... 41
5.1.1 Main findings... 41
5.1.2 Results in relation to other studies and reviews ... 41
5.1.3 Clinical imlications ... 44
5.1.4 Strengths and limitations ... 45
5.2 Comparative Efficacy and Safety of Surgical Treatments for Benign Prostate Hyperplasia - an Application of Network Meta-Analysis... 47
5.2.1 Main findings... 47
5.2.2 Results in relation to other studies and reviews ... 47
5.2.3 Clinical implications ... 50
5.2.4 Strengths and limitations ... 52
6 Conclusions ... 54
6.1 Assessing the Risk of New-Onset Hypertension and Diabetes after Shock Wave Lithotripsy - a Population-Based Retrospective Cohort Study ... 54
6.2 Comparative Efficacy and Safety of Surgical Treatments for Benign prostatic hyperplasia - an Application of Network Meta-Analysis... 54
6.3 Future research for SWL with urolithiasis ... 54
6.4 Future research for BPH surgery ... 55
References... 56
List of Tables
Table 1: Studies regarding new onset HTN or diabetes in shock wave lithotripsy
patients ... 73
Table 2: Description of two projects ... 75
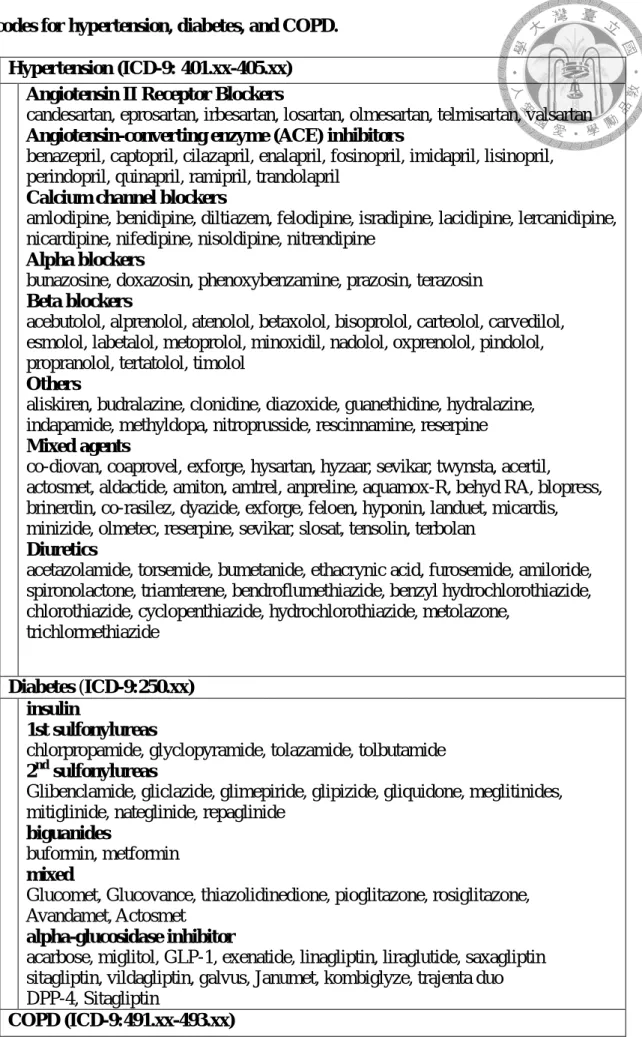
Table 3: Medication and International Classification of Diseases, Ninth Revision codes for hypertension, diabetes, and COPD. ... 76
Table 4: Nomenclature of nine methods for BPH surgery ... 78
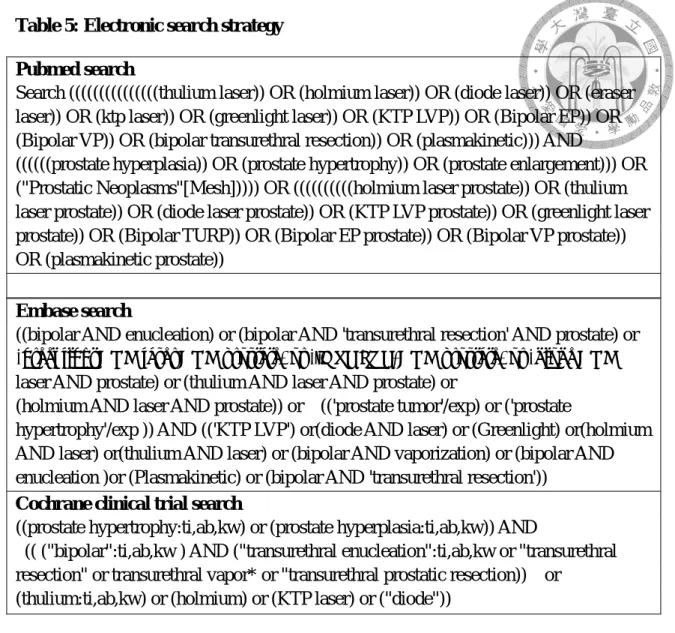
Table 5: Electronic search strategy ... 79
Table 6: Baseline patient characteristics ... 80
Table 7: Incidence of new-onset hypertension and diabetes ... 82
Table 8: Risk of new-onset hypertension/diabetes ... 83
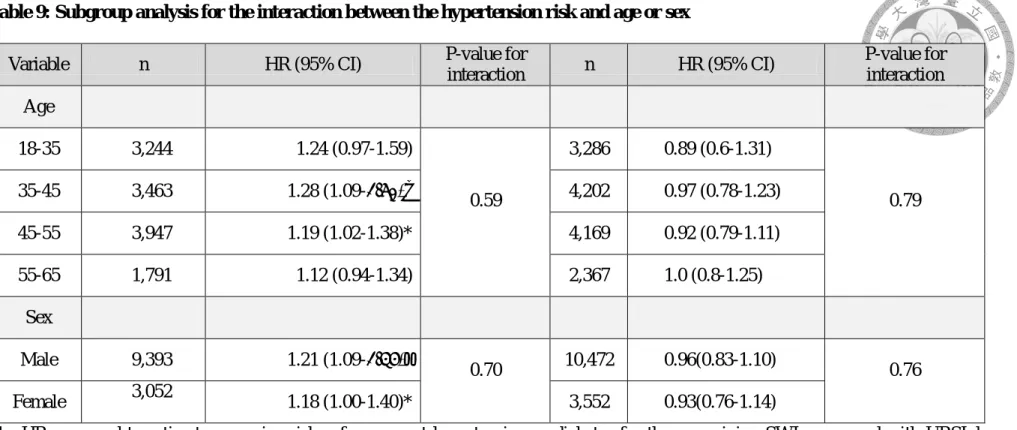
Table 9: Subgroup analysis for the interaction between the hypertension risk and age or sex ... 84
Table 10: Risk of new-onset hypertension and diabetes in the large stone and SWL groups ... 85
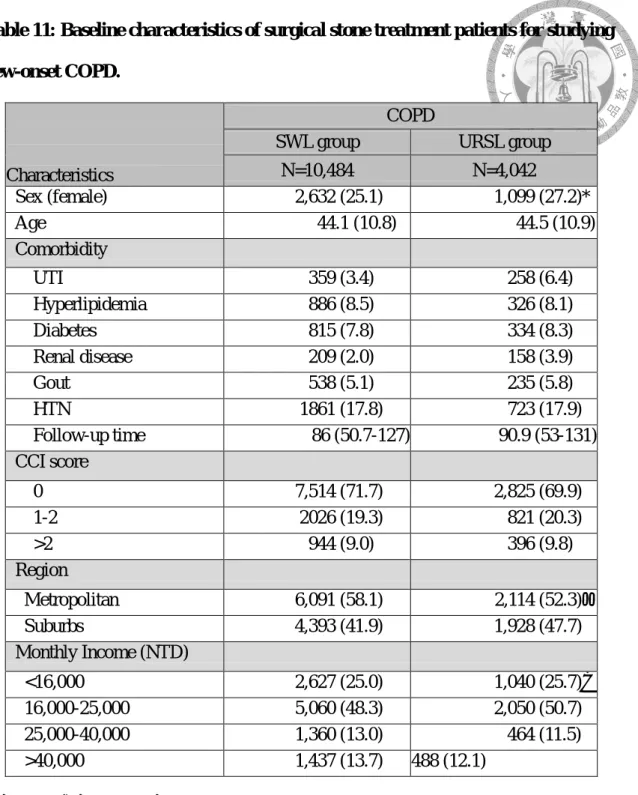
Table 11: Baseline characteristics of surgical stone treatment patients for studying new-onset COPD. ... 86
Table 12: The risk of new-onset COPD for SWL and URSL treatment. ... 87
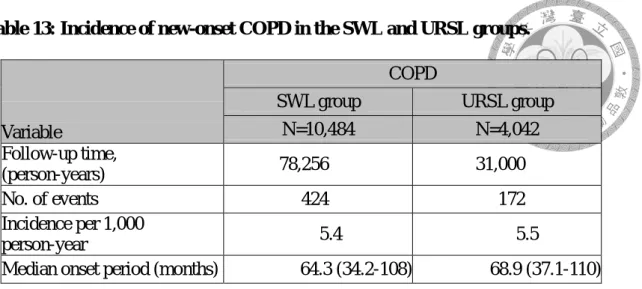
Table 13: Incidence of new-onset COPD in the SWL and URSL groups. ... 88
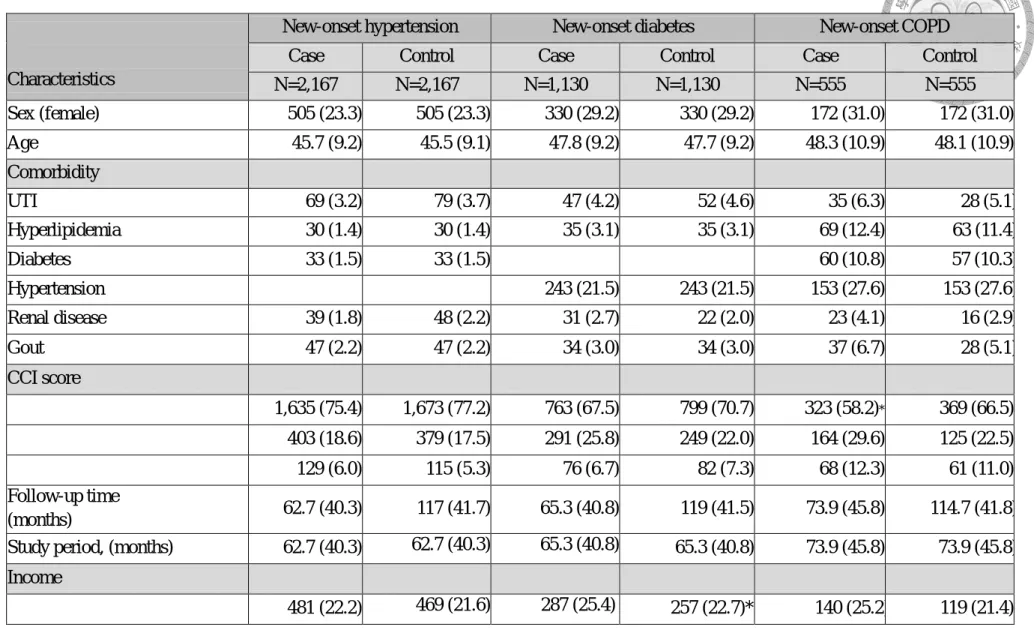
Table 14: Baseline characteristics among all cases and their matched controls in new-onset hypertension, diabetes, and COPD ... 89
Table 15: SWL sessions among all cases (new-onset hypertension, diabetes, and COPD) and their matched controls. ... 91
Table 16: Studied outcome ... 92
Table 17: Description of included studies ... 93
Table 18: Studied outcome of included studies ... 101
Table 19: Results of network meta-analysis ... 106
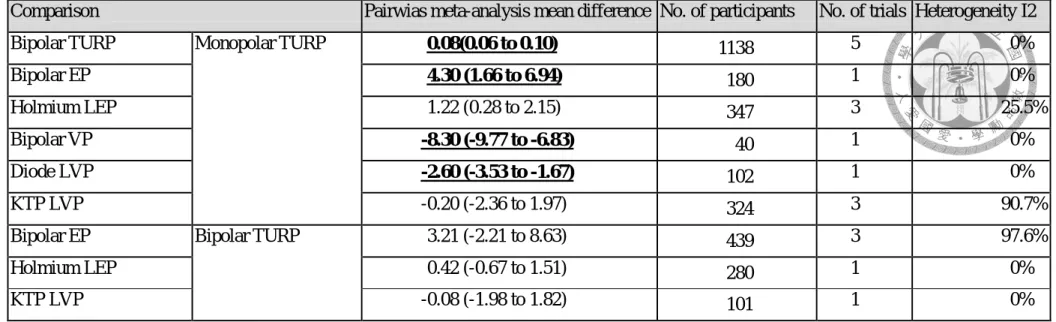
Table 20: Results of meta-analysis of direct comparison ... 117
Table 21: Sensitivity analysis ... 135
Table 22: Assessment of inconsistency ... 137
List of Figures
Figure 1: Minimally invasive urologic therapy development ... 139
Figure 2: Conceptual diagram involving for evaluation of minimally invasive urologic therapy (MIUT) ... 140
Figure 3: Flow diagram of patients... 141
Figure 4: Cumulative risk probability for new-onset hypertension and diabetes in the SWL and URSL groups ... 142
Figure 5: Flow diagram of patients who were used for the study of COPD ... 143
Figure 6: Cumulative risk probability for new-onset COPD in the SWL and URSL groups ... 144
Figure 7: PRISMA flowdiagram ... 145
Figure 8: Risk of bias assessment for the included trials ... 146
Figure 9: network treatment comparisons. ... 148
Figure 10: Network meta-analysis ... 150
Figure 11: Sensitivity analysis ... 152
Figure 12: Comparison-adjusted funnel plot for the network of primary outcome... 154
1 Introduction
1.1 Minimally-Invasive Treatments for Urinary Tract Diseases
Minimally invasive urologic therapy (MIUT) is the treatment technique for people with disorders of the genitourinary system. Surgeons use small tools passed through tiny keyhole cuts on the skin (percutaneous) into the abdomen (laparoscopy), tools passed through the natural lumen assisted by micro-telescopic camera (endoscopy), or even extracorporeal energy (shock-wave) to treat patients. Compared to traditional urologic treatment options, MIUT has many advantages such as less post-treatment pain, short healing time, and less side effects; hence, patients can get back to normal daily activities more quickly. The improvement in technology in the last 30 years makes MIUT the mainstream treatment in most urologic diseases.1 (Figure 1)
To facilitate decision making in the use of MIUT, it is equally important to weigh between efficacy and side effects associated with the therapy. Hence the retrospective cohort studies and meta-analysis based on randomized controlled trials (RCT) are vital in identifying the most appropriate MIUT for the respective disease entities.
Among the MIUTs currently available in the clinic for benign urologic conditions in Taiwan, extracorporeal shock-wave lithotripsy (SWL) and endoscopically-assisted transurethral surgeries are two of the most commonly used procedures for treating urolithiasis and benign prostate hyperplasia (BPH), respectively.2 While urolithiasis and
BPH are frequently observed urologic conditions in the out-patient clinic as of today, the efficacy and safety of the current treatment options, remain to be the focus of the national health-care system and associated epidemiology research.
In this thesis, we will adopt two epidemiological research methods to tackle the long-term effects of SWL and the efficacy/safety of MIUT in BPH.
1.1.1 Extracorporeal Shock Wave Lithotripsy
SWL when first introduced in 1982, quickly revolutionized stone treatment in the urology field due to its minimally invasive nature. However, the long-term side effects such as incidence of hypertension and diabetes was still a contentious issue.
1.1.1.1 The First-Line Treatment for Urolithiasis with Known Side Effects
SWL, introduced to the clinical setting for stone management in 1982,3 became the first-line treatment for uncomplicated renal and proximal ureteral stones. Accompanied by endoscopic surgery, it was easier and more convenient for patients, and caused less morbidity than the open surgical approach. Along with SWL, endourologic techniques such as ureterorenoscopic lithotripsy (URSL) or percutaneous nephrolithotomy (PCNL) replaced open surgery. Although SWL was initially considered the treatment option for stones in almost all anatomical locations, it was soon discovered to be limited by high stone debris that could result in an ureteral obstruction.4 As a result, SWL was adopted to treat renal stones <1–2 cm, while PCNL with or without SWL was used to manage more complicated kidney stones. Ureteral stones on the other hand, were either treated by SWL or by URSL depending on the size and localization of the stone.
Although SWL is a minimally-invasive method available to remove stones, which are thereafter thought to pass harmlessly through the kidney, it is now well documented that renal injury as in a hemorrhagic lesion in the renal vasculature can occur as a side effect.1 4 The volume of the hemorrhagic lesion in the kidney, is dependent on the dose
of the shockwave; hence, the lesion size increases as the number of shocks increase.5 6 In 29% of the patients who have undergone SWL treatment, subcapsular hematoma was observed immediately as revealed by magnetic resonance imaging.7 Hematomas can persist for many months to years, and although it has been reported to mostly resolve within weeks without long-term adverse effects,8 catastrophic internal hemorrhage and irreversible acute kidney failure can potentially occur and has indeed been noted.9 10
Recently published studies suggest new-onset hypertension and development of diabetes as potential long-term side effects resulting from SWL treatment received almost a decade ago in some patient groups. Despite the patho-mechanism of SWL causing hypertension and diabetes, yet to be identified, the acute injury to the kidneys and pancreas, post SWL treatment as evidently shown by numerous research groups, may be a possible underlying reason. Paradoxically, urolithiasis is a common urological problem that has been shown to be associated with hypertension, diabetes, obesity, insulin resistance, and metabolic syndrome.11 12 In addition, patients with urolithiasis have a higher long-term risk of developing cardiovascular diseases and osteoporosis, than the general population.13 Preclinically, Handa et al. designed a juvenile pig model to demonstrate the effects of shock waves on the development of metabolic syndrome.14 An increased risk of early-onset hypertension was found, but there were no signs of worsening glucose tolerance after shock wave treatment, when compared to sham therapy. In the next section, we will review the published epidemiological findings regarding new-onset hypertension and diabetes, as long-term side effects of SWL.
1.1.1.2 Hypertension and Diabetes as Long-Term Adverse Effects: Published Evidence
Although SWL is easy to perform, it is a kind of renal trauma, and earlier studies argued that early-onset hypertension would develop after SWL treatment.15 16 In 2006, Krambeck et al. performed a retrospective, hospital-based study. They found that patients receiving SWL for renal and proximal ureteral stones, had an increased risk of developing hypertension and diabetes after 19 years, as compared to patients who received conservative treatment.17 Nevertheless, subsequent studies (hospital-based and database studies) showed conflicting results regarding the long-term side effects of SWL.18 19 We performed database search from Pubmed (1950 to March 2016) and Embase (1970 to March 2016), to find relevant studies regarding the association between SWL and hypertension or diabetes. After excluding duplicated articles, studies with no comparison group, irrelevant studies, or studies with less than one-year follow-up, 10 and 3 studies regarding SWL vs hypertension and SWL vs diabetes, respectively were included in our qualitative analysis. (Table2)
Before 2006, there were two hospital-based prospective cohort studies,19 20 and two RCT,21 22 studying the association between SWL and new-onset hypertension. These fours studies showed no increased risk of new-onset hypertension after SWL when compared to other modalities of treatment. However, these four studies had limited case numbers (100-200) with just one-session of SWL, and limited follow-up time (1-4 years).
After Krambeck et al first demonstrated the long-term risk of hypertension and diabetes after SWL, they performed a registry-based retrospective cohort study using a health claim database.23 They compared patients with urolithiasis, treated with or without SWL, and having a median follow-up of 103 months. No difference in the incidence of hypertension and diabetes between the two groups were found. In their cohort, only a small portion (8%) received SWL treatment, of which only 15% received two or more sessions; furthermore, other surgical treatments in the non-SWL group were not differentiated. With a low treatment rate and a small number of SWL cases, they could not estimate the relationship between SWL treatment sessions and new-onset hypertension. Moreover, since only a cohort from a single community was studied, it was difficult to generalize the results.
In contrast, a questionnaire-based retrospective cohort study that comprised of 1,758 patients with urolithiasis treated with SWL, and having a median follow-up of 6 years,24 showed an increase in the risk of new-onset hypertension compared to matched controls from the National Health and Nutritional Examination Survey database.
However, the response rate was only 30%, and the control group was the general population.
Denburg et al. conducted a retrospective cohort study to assess the risk of incident hypertension after exposure to SWL and URS.24 SWL in the kidney was associated with incident hypertension, while URS was not. When further stratifying SWL to the kidney
or ureter, only SWL to the kidney was related to incident hypertension.
Despite the conflicting results, the possibility of new-onset hypertension and diabetes as potential side effects of SWL ought to be a cause for concern, especially in some patient groups, and clearly deserves further investigation.
1.1.2 Minimally Invasive Treatments for Benign Prostate Hyperplasia
Regarding BPH, multiple minimally invasive new surgical methods, including different laser therapies and bipolar technologies are available since 2000. The decision of choosing a specific surgical method is still controversial for patients, health-care providers and the insurance company.
1.1.2.1 Past and Present
BPH is the main etiology of lower urinary tract symptoms (LUTS) in middle- and old-aged men25. It affects 30% of men in their fifties and up to 90% of those in their eighties. As the urinary symptoms become more severe, it affects the patient’s quality of life.26 LUTS is the most common urologic problem in urologic outpatient clinics.27 Although medication can improve symptoms for most BPH patients, some still need surgical intervention to resolve the complications of BPH, such as urine retention, bilateral hydronephrosis, bladder stone, recurrent urinary tract infection, hematuria, bladder diverticulum or severe complications (as in international prostate symptoms
score (IPSS) >20) that are refractory to medication.28
Monopolar transurethral resection of prostate (TURP) has been the gold standard surgical treatment for BPH since the 1970’s, because of substantial improvement in the functional outcome (symptoms score and maximal flow rate).29 Nevertheless, due to the invasiveness and side effects of monopolar TURP, the surgery is still risky for elderly patients or those with comorbidities.30 Hence, urologists have been continually searching for new approaches in minimally invasive surgeries, to decrease side effects while keeping up the same functional outcome as monopolar TURP. Therefore, the main stream minimally invasive treatment in the 1990’s was coagulation of the prostate which could cause sloughing of prostate tissue, and included procedures such as:
transurethral microwave thermotherapy (TUMT), transurethral ethanol ablation (TEP), transurethral needle ablation (TUNA), and laser coagulation.31-36 Despite the decreased side effects associated with these MIUTs, their functional outcomes were inferior to monopolar TURP.37 Therefore these earlier generation MIUT soon fell out of popularity.
After the 2000’s, new surgical methods for BPH including bipolar energy, holmium laser, KTP (potassium-titanyl-phosphate) laser, thulium laser, and diode laser burgeoned and infiltrated the urology practice.38-41 Bipolar systems use a specialized loop or electrode that incorporates both the active and return portions of the circuit on the same electrode. It can incise, resect, or vaporize prostate tissue by creating an ionized plasma corona using an axipolar electrode. Furthermore, these new methods all used normal saline instead of distilled water as irrigation fluid during operation, to avoid
transurethral resection (TUR) syndrome (hyponatremia).
In specifics, BPH treatments including the monopolar, bipolar and laser-assisted methods that are summarized later, can be further differentiated into those that resect, vaporize, or enucleate the prostate. The resection method involves resecting the prostate adenoma piece by piece, and washing out with an evacuator, vaporization involves vaporizing the prostate adenoma while enucleation involves peeling the adenoma from the capsule, and morcellating the adenoma with a morcellator.
Of the laser-assisted BPH MIUTs, the holmium laser acts as an enucleating probe by emitting a pulsatile wavelength at 2104 nm, which is mainly absorbed by water. The thulium laser, on the other hand, emits a continuous wavelength at 2013 nm and enucleates the prostate adenoma. Continuous energy emission has been suggested to create cleaner incisions with stronger hemostatic effects, thereby achieving enucleation.
The KTP laser vaporizes the prostate tissue with a 532-nm wavelength laser that is selectively absorbed by hemoglobin. The diode laser is a 980-nm laser that is simultaneously absorbed by water and hemoglobin, and can provide significant tissue vaporization or enucleation with good hemostasis.
With the numerous MIUT options currently available for treating BPH, clinicians are faced with the decision of which approach is the best for their patients. Without head-to-head comparisons in RCT trials, it remains an epidemiological question whether and how new treatments out-perform the more conventional one, i.e.
monopolar TURP. In the following section, we will introduce the major outcomes
considered important in decision making in BPH treatments, and briefly review published meta-analysis aimed to facilitate the decision making.
1.1.2.2 Efficacy and Safety of BPH Treatments
LUTS, often resulting from BPH, includes three storage symptoms (frequency, urgency, and nocturia) and four voiding symptoms (small caliber of stream, intermittency, residual urine sensation, and strain to urinate). We commonly use IPSS as a subjective symptom score, objective flowmetry and residual urine to evaluate the severity of BPH. The three storage and four voiding symptoms are included in IPSS, and each symptom is scored from 0-5, and the total scores 0-7, 8-18, and 19-35 are interpreted as mild, moderate and severe symptoms of BPH, respectively. Maximal flow rate less than 15 is viewed as a poor flow rate.42
As described earlier, monopolar TURP has been the gold standard surgical treatment for BPH because of improvement in the maximal flow rate (Qmax) and IPSS.29 Despite this, post-operative morbidities such as failure to void, urinary tract infection, bleeding requiring transfusions, and TUR syndrome can occur as early complications30. Late complications such metal stenosis, urethral stricture, bladder neck contracture, incontinence, BPH recurrence, retrograde ejaculation, and erectile dysfunction limited widespread use of the surgery.44
As such, the aim of developing new or advanced therapies for BPH was to achieve non-inferiority in the functional outcomes, while significantly reducing the
post-operative adverse events.
A comparison of the earlier generation MIUT was performed by Lourenco et al.37 The authors performed a systematic review and included 22 RCT with 2434 patients.
They compared the functional outcome and side effects of transurethral microwave therapy, transurethral ethanol injection, transurethral needle ablation, and laser coagulation, with monopolar TURP. They found lesser side effects including bleeding, TUR syndrome, blood transfusion, and loss of ejaculation, in the earlier generation MIUT, as compared to monopolar TURP. However, the functional outcome improvement as in symptoms score, maximal flow rate, urinary retention rate and reoperation rate, was inferior for MIUT than monopolar TURP.
Omer et al.43 performed a systematic review comparing bipolar TURP with monopolar TURP with 24 RCT. They found no difference in functional outcomes (IPSS and Qmax) between monopolar TURP and bipolar TURP. However, the side effects including TUR syndrome (RR=0.12, 95% CI: 0.05–0.31), blood clot retention (RR=0.48, 95% CI: 0.30–0.77), and blood transfusion (RR=0.53, 95% CI: 0.35–0.82) were less frequent in bipolar TURP than monopolar TURP. There is no difference in incontinence, stricture and urinary tract infection.
For approaches that enucleate hyperplastic prostate tissue, Yin et al. performed a systematic review comparing holmium laser enucleation of the prostate (HOLEP) with monopolar TURP, including 6 RCT involving 541 patients.44 They found that Qmax
was better in HOLEP than monopolar TURP, 12 months postoperative. Blood loss and blood transfusion rates were lesser in HOLEP than monopolar TURP. The hospital -stay and catheterization time were also shorter for the HOLEP group than monopolar TURP group .
Regarding vaporization methods, a systematic review including six RCT with 1398 patients and five case-control studies, showed no difference in functional outcomes (symptoms scores and maximal flow rate) between photoselective vaporization (PVP) and monopolar TURP if the prostate size was less than 70 gm.45 However, PVP was inferior to monopolar TURP in primary efficacy if the prostate size was larger than 70 gm. Regarding side effects, PVP had lesser transfusion rates, capsular perforation, incidence of TUR syndrome, and blood clot retention events. The catheterization and hospitalization time were shorter for the PVP group than the monopolar TURP group.
The majority of the reviews or studies evaluating new BPH treatments, compared TURP, the gold standard surgery, with one MIUT alone, in context of efficacy and safety. In contrast, simultaneous comparison of several BPH MIUTs in the same study, should provide more direct answers regarding the superiority of treatments. This type of research is highly anticipated, but currently lacking.
1.2 Evidence-Based Medicine
Evidence-based medicine (EBM) is an approach in medical practice, intended to
optimize decision-making, by emphasizing the use of evidence from well-designed and well-conducted research. The level of evidence is classified by epidemiologic strength.46 RCT are considered to be the most reliable form of scientific evidence because they minimize bias, control confounding factors and show statistical reliability. However, RCT are costly, time consuming and have ethical limitations. Besides, RCT are usually designed to compare efficacy and short-term safety between different treatments. To evaluate the benefit and risk of MIUT, efficacy and side effects of the long term are equally important. Hence, a cohort study as well as meta-analysis of RCT are appropriate epidemiological tools for evaluating clinically available MIUTs in a real-world context. The conceptual flowchart for evaluation of long-term side effects and multiple treatment options in MIUT is schematically shown in Figure 2.
1.2.1 Nation-wide Retrospective Cohort Studies: Suitable for Studying Long-Term Side Effects Associated with SWL
Although RCT are in the higher level of evidence hierarchy, the follow-up periods for RCT are limited by the study design and sample size; sufficient statistical power is usually estimated based on efficacy endpoints. Hence, the long-term side effects or rare events, associated with a treatment can be missed or underestimated in RCT. In contrast, real-world cohort studies are usually better-suited for the purpose of identifying and determining long-term safety issues associated with treatments. Nonetheless, prospective cohort studies are open-ended, time consuming and costly; in comparison, retrospective cohort studies with secondary data almost always are benefited with larger
sample size, long-term follow-up and real-world scenario. Hence, retrospective cohort studies using the nationwide registry are rational and practical options to evaluate treatment-associated long-term and rare side effects, as well as small but definitive differences between treatment options.
Epidemiologically, not only is it difficult to demonstrate a long-term side effect that appears nearly a decade after exposure, but it is also equally challenging to show the risk of a disease as a treatment-associated side effect, in a patient group with known predisposed risk for the same disease in question. Since patients with urolithiasis have a higher prevalence of hypertension and diabetes than the general population, it is difficult to prove that the development of hypertension or diabetes after SWL is due to the treatment and not the stone itself.
A suitable comparison group with a large cohort and long-term follow-up is needed, to evaluate the outcomes of SWL in patients undergoing lithotripsy. Moreover, the high recurrence and re-treatment rates in patients undergoing lithotripsy should be considered.
Taiwan has a high prevalence and recurrence rate of urolithiasis.47 After the Taiwan National Health Insurance program was established in 1995,48 comprehensive medical and surgical stone treatments were reimbursed and recorded in all clinical settings. SWL and URSL are the first-line surgical treatments for urolithiasis, and approximately 100,000 and 30,000 procedures, respectively, are performed annually in Taiwan.49 PCNL and open stone surgeries are usually reserved for patients with a large stone burden or those who underwent a failed first-line surgical treatment. Hence, patients
treated with SWL and URSL share similar characteristics and are more suitable for comparison with each other.
1.2.2 Network Meta-analysis and Systematic Reviews: Fit for Comparing Multiple BPH MIUTs
Meta-analyses using data from RCT were viewed as level one evidence for evaluating the efficacy of different treatments. Using statistical analysis to merge data from RCT, meta-analysis can quantitatively summarize available scientific evidence and provide pooled estimates of relative risk. Hence, a meta-analysis is more effective in detecting small but significant clinical effects that may not have statistical significance in individual trials.50 Therefore, meta-analysis enables timely detection of benefits contributed by new treatments and helps improve health care.
However, conventional meta-analyses can only differentiate between two treatments. Given that there are always many different treatments for a single disease, head-to-head active comparisons are not always feasible or available. Research has been devoted to develop a model for solving this problem. Network meta-analysis is a meta-analytic method which integrates results of direct comparison within trials, and indirect comparison between trials, for simultaneous comparison of 3 or more treatments.51 Under the assumptions of homogeneity of each relative treatment effect, and the similarity of trial characteristics across the trials, network meta-analyses can facilitate multiple head-to head comparisons across a variety of treatments.52 53
For any given comparison, i.e., A vs B, direct evidence will be provided by trials that compare these two treatments directly, as in a standard comparison meta-analysis.
Indirect evidence for A vs B can be provided if studies that compare A to C, and B to C are assessed jointly. In the assumption of transitivity, it is assumed that the A vs C trial and the A vs B trial are similar with respect to the distribution of all possible effect modifiers. Hence, we will assume that the common treatment used to compare the different surgical treatments is similar, and the missing treatment in each trial is absent randomly. The network meta-analysis aims to combine the direct and indirect evidence into a single effect size.52 Hence, it becomes feasible to compare different treatments simultaneously.
Nowadays, there are eight new methods for treatment of BPH. The following questions remain: Which method is the best for primary efficacy with less complications?
Are enucleation methods really better than vaporization methods in primary efficacy?
Are new methods really safer than monopolar TURP with the same efficacy? We believe a network meta-analysis using RCT is the best EBM method to answer these questions.
2 Purpose
Urolithiasis and BPH are the two most common urologic diseases in urologic clinics and usually affect middle- to old-aged men.
SWL, upon its introduction in 1982, quickly revolutionized the stone treatment in clinical urology due to its minimally invasive nature. However, the long-term side effects such as incident hypertension and diabetes are still contentious. The aim of our first study is to perform a retrospective cohort study using secondary data to assess the long-term risk of new-onset hypertension and diabetes between SWL and URSL.
On the other hand, for BPH, there are multiple minimally invasive new surgical methods comprising of different laser therapies and bipolar technologies, that became clinically available after the year 2000. The decision of selecting the most appropriate surgical method is still controversial for patients, health-care providers and insurance companies. Our second study aims to use network meta-analysis to evaluate the efficacy and safety of different surgical treatments for BPH. The study logistics and description of the two topics are depicted schematically in Figure 2 and Table 2.
3 Methods and Materials
3.1 Assessing the Risk of New-Onset Hypertension and Diabetes after Shock Wave Lithotripsy - a Population-Based Retrospective Cohort Study
3.1.1 Data sources
The longitudinal health insurance database 2000 (LHID-2000), a data subset randomly sampled from the Taiwan National Health Research Insurance Database (NHIRD)between 1996 and 2013, was used for the analysis. The LHID-2000 contains 1,000,000 beneficiaries who are randomly selected from the approximately 23.75 million people who were recorded in the 2000 registry of NHIRD. There was no significant difference in the sex distribution compared to the population in the original NHIRD.54
3.1.2 Study design and study participants
The potential study subjects were patients who received SWL or URSL as the first stone surgical treatment. The first stone surgical treatment date was defined as the index date. We used a newuser design and recruited those with an index date between January 1, 1999 and December 31, 2011 to exclude prevalent cases (1996-1998 was the wash-out period), ensuring that every patient had at least two years of follow-up. We only included patients aged between 18 and 65 years because children are seldom treated with URSL and older people have more comorbidities and a greater risk of death.
We then compared SWL and URSL in terms of the risk of new-onset hypertension.
We excluded patients with a history of hypertension before surgical treatment, patients who were treated with both SWL and URSL to avoid contamination between groups, and those with less than 3 months of follow-up (including new-onset hypertension). We applied similar criteria to investigate diabetes.
Hypertension or history of diabetes was defined as at least two outpatient claims or one inpatient claim of hypertension/diabetes or prescription of hypertension/diabetes medication for hypertension/diabetes within one year before the index date, since we only wanted to recruit normotensive patients and those with normal glucose levels. The incidence of new-onset hypertension or diabetes was defined as a diagnosis of hypertension after the index date with administration of anti-hypertensive medication for more than 90 days or a diagnosis of diabetes with administration of anti-diabetic medication for more than 30 days in 1 year, respectively. Therefore, patients with borderline hypertension or high glucose were excluded. The anti-hypertensive and anti-diabetic medications in this study included angiotensin-converting enzyme inhibitors, calcium channel blockers, angiotensin II antagonists, α-blockers, ß-blockers, diuretics, insulin, sulfonylureas, meglitinides, biguanides, thiazolidinediones, α-glucosidase inhibitors, and D-phenylalanines (Table3).
3.1.3 Statistical analysis
The demographic and clinical characteristics of patients were described using mean ±
standard deviation. Student’s t-test or analysis of variance was used for continuous variables, and chi-square tests were used for categorical variables. The associations between different surgical treatments and hypertension/diabetes were analyzed using Kaplan–Meier survival curves and log-rank tests. Multivariable Cox proportional-hazards models were further conducted to estimate adjusted associations.
The proportional hazards assumption was evaluated by plotting the Kaplan-Meier survival curves for the investigated covariates against follow-up time. Study entry was defined as the index date. In the models estimating the hazard ratio (HR) of hypertension and diabetes, observations were censored on December 31, 2013, the date patients developed hypertension/diabetes, received PCNL or open stone surgery, or loss of follow-up, whichever occurred first. The characteristics that were adjusted in the multivariable Cox proportional hazards models included sex, age, hyperlipidemia, gout, chronic kidney disease, index year, D’Hoore’s Charlson comorbidity index (CCI) score, monthly income, region, and diabetes or hypertension. We further used a time-varying Cox model to estimate the association between the number of SWL treatment sessions and new-onset hypertension or diabetes. The number of SWL sessions was used as a time-varying variable in the study group. The variables were enumerated as 1, 2, 3, 4, and ≧5 after the first, second, third, fourth, and fifth SWL sessions, respectively. Since multiple treatment sessions may have been due to either residual or recurrent stones, a longer interval to the second event implied a recurrent stone. We stratified patients with a second event into three groups according to the time to the second event to determine the hypertension risk in these subgroups. We further performed a subgroup analysis investigating the possible interaction between the hypertension or diabetes risk and sex
or age.
Sensitivity analysis
Comparing the SWL and large stone groups
Because stone severity, which may be associated with hypertension and diabetes, was not recorded in the NHIRD, we selected patients for a large stone group (those receiving PCNL or open surgery) and compared the risk of new-onset hypertension and diabetes between the SWL and large stone groups. We divided the large stone group into two subgroups: patients receiving PCNL or open stone surgery without SWL and patients receiving PCNL or open stone surgery with SWL. In model 1, we compared the risk of new-onset hypertension or diabetes between the patients undergoing SWL and patients undergoing PCNL or stone surgery without SWL by means of a Cox proportional model. In model 2, we used a time-varying Cox model to estimate the association between the number of SWL treatment sessions and new-onset hypertension or diabetes. In model 3, we assessed the effect of SWL in the large stone group by comparing patients receiving PCNL or open stone surgery with SWL to patients receiving PCNL or open stone surgery without SWL.
Negative control
We also chose chronic obstructive pulmonary disease (COPD) as a negative outcome, because there is no evidence that COPD is associated with stone disease or
SWL. The associations between different surgical treatments and COPD were analyzed using Kaplan–Meier survival curves and log-rank tests. Multivariable Cox proportional-hazards models were conducted to estimate adjusted associations. We further used a time-varying Cox model to estimate the association between the number of SWL treatment sessions and new-onset hypertension or diabetes. The definition and characteristics that were adjusted were similar to the model for evaluating new-onset diabetes.
Nested Case-Control Study Approach
In this time-varying, nested case-control model, we compared shock wave lithotripsy (SWL) treatment and ureterorenoscopic lithotripsy (URSL) with the risk of new-onset hypertension, diabetes, and chronic obstructive pulmonary disease (COPD).
An incidence density sampling approach was applied to match new-onset hypertension (diabetes and COPD) cases with controls (1:1) based on age, sex, diabetes, hypertension, hyperlipidemia, gout, and index date within 60 days. After matching, we assigned the length of the follow-up period (the interval from the index date to the event date) in each case to his/her matched control to ensure the same length of study periods between the cases and controls. The Mantel-Hansel test and Wilcoxon sign rank test were applied to compare the differences in treatment sessions between cases and matched controls.
Analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA). A two-sided p-value <0.05 was considered statistically significant. This
study was approved by the Institutional Review Board of the National Taiwan University Hospital. The need for informed consent was waived because of the anonymous nature of the data.
3.2 Comparative Efficacy and Safety of Surgical Treatments for Benign Prostate Hyperplasia - an Application of Network Meta-Analysis
Nowadays, there are eight new methods including bipolar resection, bipolar vaporization, holmium laser enucleation, thulium laser enucleation, PVP, diode laser vaporization and diode laser enucleation most commonly used. (Table 4)
This network meta-analysis would be conducted to determine which new surgical method could achieve the best functional outcomes with fewer complications, using data from randomized controlled trials.
3.2.1 Data sources and searches
We conducted online English literature searches of Pubmed (1996-March 2018), Embase (1980-March 2018), and Cochrane clinical trial registers, not restricted to publication year or language. We also manually searched the reference lists of the identified publications to identify additional potentially eligible studies. The search terms included prostate hyperplasia / prostate hypertrophy / prostate tumor, and bipolar (TURP, enucleation, vaporization) diode laser, thulium laser, KTP laser, greenlight laser,
and holmium laser. The detailed study searching strategies are provided in Table 5.
3.2.2 Study selection
Inclusion and exclusion criteria were defined prior to the literature search. Studies were chosen if they met the following criteria:
Randomized, parallel-group design clinical trials comparing monopolar transurethral resection of the prostate (TURP), bipolar TURP, Bipolar EP (including vapo-enucleation), Holmium LEP, Thulium LEP (including vapo-enucleation), Diode LEP (including vapo-enucleation), Bipolar VP (including vaporization with apical resection), KTP LVP, and Diode LVP for BPH surgeries.
Patients with maximal flow rates <15 mL/s and IPSS >8
Exclusion criteria: neurogenic bladder, previous urethral, prostate, and bladder surgeries, suspected prostate cancer
3.2.3 Data Extraction and quality assessment
The following information will be extracted and entered independently into the study databases by two investigators.
Study characteristics: Authors, journal and year of publication, country, intervention method, number of patients, age, prostate-specific antigen (PSA), International Prostate Symptoms Score (IPSS), quality of life QOL, post void residual urine (PVR), maximal flow rate (Qmax), prostate volume.
Peri-operative parameters: Hb-decline, operation time, blood loss, duration of catherization, length of hospital stay.
Functional outcomes: IPSS, Qmax, PVR, health-related QOL (HRQOL), postoperative PVR at 6, 12, 24, and 36 months.
Complication:
Early complications: TUR syndrome, blood transfusion, re-catheterization, blood clot tamponade, urinary tract infection.
Late complications: meatal stenosis, urethral stricture, bladder neck contracture, incontinence, BPH recurrence (recurrence requiring surgical intervention or repeat apical resection), retrograde ejaculation, erectile dysfunction.
Studies reported in non-English and non-Chinese language journals will be electronically translated before assessment. Where more than one publication of a study exists, reports will be grouped together. We will plan to contact the author(s) for missing data. In some instances, if standard deviation (SD) data are missing, we would calculate SD mathematically or measure it from figure. If the author only offers medians, we would use the median as a mean and the interquartile range (IQR)3-IQR1/1.35 as the standard deviation.55
We plan to use the Cochrane Collaboration’s risk of bias tool to appraise the quality of the articles. The following domains will be assessed in all included studies:
random sequence generation, allocation concealment, blinding of participants, blinding of outcome assessment (according to functional outcome), incomplete outcome data
(only appraised for >3 months’ follow-up article), selective reporting (according to the complications reported56.
Two reviewers (H-SW, T-CS) will independently appraise the articles and come to an agreement on the final decisions. A third reviewer (TCY), who would act as an arbiter will be consulted for any unresolved discrepancies.
The primary outcome will be the functional outcome, and the secondary outcome will be the perioperative parameters and complications.
We will estimate the relative ranking of the competing interventions according to the following outcomes:
Functional outcomes: Qmax and IPSS, at 6, 12, 24, and 36 postoperative months.
Perioperative parameters: catheterization duration, Hb-decline.
Complications: blood clot tamponade (bladder tamponade secondary to blood clot) blood transfusion, urinary tract infection, re-catheterization, urethral stricture, retrograde ejaculation, incontinence, BPH recurrence.
3.2.4 Data synthesis and analysis
All data from each eligible study will be extracted and entered into a standardized spreadsheet software program (Microsoft access 2013, Microsoft Corp, Redmond, WA, USA).
Methods for direct treatment comparisons
The weighted mean differences and risk ratio reductions will be reported for continuous and binary variables, respectively. Heterogeneity will be assessed by a visual inspection of the forest plots, and subsequently test using I2 statistical method. We will choose a random effects model if I2 >50%, otherwise the fixed effect model will be used.
A traditional pair-wise meta-analysis will be performed using Stata software (StataCorp.2011, Stata Statistical Software: Release 14, College Station, TX56
Methods for direct and indirect comparisons
We will fit a network meta-analysis model separately for each outcome, combining direct evidence for each comparison with indirect evidence for all pair-wise comparisons simultaneously.57
Assessment of statistical inconsistency
We will perform local approaches and global approaches for evaluating inconsistency.58 59 To evaluate local inconsistencies, we will use the Loop inconsistency method. This method evaluates the consistency assumption in each closed triangular or quadratic loop separately as the difference between the direct and indirect estimate for a specific comparison in the loop and also to test for global loop inconsistencies in the entire network. To evaluate for global inconsistencies in the entire network, we will use the design-by-treatment interaction model. This method accounts for different sources of inconsistency that can occur when studies with different designs give different results
or disagreements between direct and indirect evidence. Using this approach, we will infer the presence of inconsistency from any sources in the entire network based on a chi-square test.
We also estimate the probability of each treatment being at each possible rank for each intervention and each outcome. We will obtain a treatment hierarchy using the surface under the cumulative ranking curve (SUCRA) and mean ranks methods.
For continuous variables such as functional outcomes and peri-operative parameters, we will conduct a trial-based meta-analysis using STATA (StataCorp.2011, Stata Statistical Software: Release 14, College Station, TX, USA) using the ‘mvmeta’
command and self-programmed STATA routines.60
For dichotomous variables such as complications, the rare events will be noted. We will perform an arm-based meta-analysis using SAS software without 0-cell correction, version 9.4 (SAS Institute, Cary, NC, USA) using GLIMMIX with Laplace integration methods. Statistical significance will be defined as p<0.05 via a two-tailed test.
Sensitivity analysis Potential effect modifier
Prostate size might affect the outcome of different surgical treatments. Therefore, large prostates might be better treated using enucleation methods and less effectively managed using vaporization methods. We will conduct a meta-regression according to
the mean prostate volume provided in each trial. We will use the weighted average preoperative prostate volume reported by the authors in each trial. If prostate volume information is not present, but the resected prostate volume data is reported, we will estimate the preoperative prostate volume as the resected volume/0.5 if the resected volume is <50 and, resected volume/0.8 if the volume is >50.
Since incontinence is always a concern for enucleation methods. We further performed an analysis comparing enucleation methods and resection methods in short-term transient incontinence (incontinence<1 month and used the earliest reported incontinence events if multiple time points) and permanent incontinence (incontinence more than 6 or 12 months). In enucleation methods, we excluded vapo-enucleation study since vapo-enucleation methods are aimed to reduce incontinence events by preserving apex region of prostate.
Post-hoc analysis
During the study, we found that the TURP group in the Bachman et al. trial included both monopolar and bipolar energy methods. The participants were not randomly allocated to monopolar or bipolar treatment groups, and the authors did not reply to our requests for further information. Therefore, we did not include data from this trial in the main analysis. We will perform further analyses by assuming that the TURP group comprises monopolar or bipolar methods to see if the results and ranking changed after adding this trial.
4 Results
4.1 Assessing the Risk of New-Onset Hypertension and Diabetes after Shock Wave Lithotripsy - a Population-Based Retrospective Cohort Study
In the LHID-2000, we found 20,219 patients aged between 18 and 65 years who first received a surgical treatment of SWL or URSL between 1999 and 2011. We further excluded 3,897, 3,598, and 279 patients because of a history of hypertension before treatment, received SWL and URSL, or follow-up less than 3 months, respectively.
There were 9,025 and 3,420 patients remaining in the SWL and URSL groups, respectively, and these patients formed our study cohort to assess the risk of new-onset hypertension. Applying similar criteria, we included 347 patients in the large stone group for the sensitivity analysis (Figure 3A). Regarding the risk of diabetes, 10,145, 3,879, and 472 patients were included in the SWL, URSL, and large stone groups, respectively (Figure 3B).
4.1.1 Baseline Characteristics
Table 6 illustrates the demographic data of patients in the SWL, URSL, and large stone groups. Regarding the cohort for studying new-onset hypertension, the SWL and URSL groups were similar in terms of mean age (42.6 vs. 42.9 years, p=0.18), prevalence of hyperlipidemia (4.9% vs. 4.4%, p=0.34), diabetes (4.8% vs. 4.6, p=0.73), CCI score (p=0.32), and gout (3.9% vs. 4.2%, p=0.43). However, women (25.9% vs.
24.0%, p=0.04) and patients with a history of urinary tract infection (5.6% vs. 3.3%,
p<0.01) or renal disease (2.7% vs. 1.5%, p<0.001) were more common in the URSL group than in the SWL group. SWL was more commonly used for people with a higher income (p<0.01) and those who lived in metropolitan areas (58.6% vs. 51.4%, p<0.001) than in those with a lower income or those who lived in rural regions. However, the baseline characteristics in the large stone group differed from those of the SWL and URSL groups. The patients in the large stone group were older and predominantly women compared to those in the SWL and URSL groups. The prevalence of urinary tract infection, diabetes, chronic kidney disease was also higher in the large stone group than in the SWL and URSL groups. The demographic data for studying new-onset diabetes were similar to those of the cohort that was used for studying new-onset hypertension (Table 6).
4.1.2 New-Onset Hypertension
After a median follow-up of 74.9 and 82.6 months, 2,028 and 688 patients developed hypertension in the SWL and URSL groups, with an incidence rate of 33.5 and 28.3 per 1,000 person-years, respectively. The number need to harm (NNH) is 215.
The median onset period was 55.2 and 57.2 months in the SWL and URSL groups, respectively (Table 7). The cumulative risk probability of new-onset hypertension was higher in the SWL group than in the URSL group (log-rank test, p<0.001, Figure 4A).
After adjusting for age, sex, diabetes, gout, hyperlipidemia, renal disease, calendar year, CCI score, region, and monthly income, we found that the SWL group had a higher probability of new-onset hypertension than the URSL group, with an HR of 1.20
(95% CI, 1.10-1.31). Among 9,025 patients, 1,612, 649, 279, and 420 received two, three, four, and five or more SWL sessions, respectively. After adjusting for covariates, we discovered that the risk of new-onset hypertension increased as the number of SWL sessions increased, with an HR of 1.10 (95% CI, 1.00-1.20), 1.30 (95% CI, 1.15-1.48), 1.55 (95% CI, 1.31-1.85), 1.70 (95% CI, 1.32-2.19), and 2.00 (95% CI, 1.63-2.45) in one, two, three, four, and five or more SWL sessions, respectively (Table 8). Regarding the time to the second event, we found that the risk of new-onset hypertension was 1.38 (95% CI, 1.21-1.58), 1.64 (95% CI, 1.40-1.93), and 1.43 (95% CI, 1.21-1.69) for the<3 months, 3-24 months, and >24 months’ groups, respectively. In subgroup analysis, the risk of new-onset hypertension was not different for age (p for interaction=0.59) or sex (p for interaction=0.70) (Table 9).
4.1.3 New-Onset Diabetes
Regarding new-onset diabetes, after a median follow-up of 82.7 and 88 months, 1,021 and 420 patients in the SWL and URSL groups, respectively, developed diabetes, with an incidence of 13.9 and 14.5 per 1,000 person-years. The median onset period was 57.6 and 62.4 months in the SWL and URSL groups, respectively (Table 7). The SWL group had a similar probability of new-onset diabetes to that of the URSL group (Figure 4B, log-rank test p=0.48).
After adjusting for age, sex, hypertension, gout, hyperlipidemia, renal disease, CCI score, calendar year, monthly income, and region, we found that the risk of new-onset diabetes was also similar in the SWL and URSL groups (HR: 0.95, 95% CI, 0.85-1.06).
Among the 10,145 SWL patients, 1841, 755, 342, and 520 received two, three, four, and five or more SWL sessions, respectively. The risk of new-onset diabetes did not increase significantly as the number of SWL sessions increased, with an HR of 0.91 (95% CI, 0.80-1.03), 1.00 (95% CI, 0.84-1.19), 1.01 (95% CI, 0.79-1.30), 1.11 (95% CI, 0.79-1.57), and 1.17 (95% CI, 0.88-1.55) in one, two, three, four, and five or more SWL sessions, respectively (Table 8). In subgroup analysis, the risk of new-onset diabetes was not different in different age (p for interaction=0.79) or sex (p for interaction=0.76) (Table 9).
4.1.4 Sensitivity Analysis
Table 10 depicts the risk of new-onset hypertension for different numbers of SWL sessions compared with the risk in the large stone group and that of the large stone group treated with or without SWL. Among 347 patients in the large stone group who were used for studying new-onset hypertension, 216 also received SWL and 131 were treated with open surgery or PCNL alone. The risk of new-onset hypertension was similar in patients who underwent SWL and patients with large stones who were treated without SWL (model 1, HR: 1.18 95% CI, 0.83-1.68, p=0.35). Among 9,025 patients, 1,612, 649, 279, and 420 received two, three, four, and five or more sessions of SWL treatment, respectively. After adjusting for covariates, we discovered that the risk of new-onset hypertension increased as the number of SWL treatment session increased, with an HR of 1.07 (95% CI, 0.75-1.53, p=0.69), 1.28 (95% CI, 0.89-1.84, p=0.18), 1.53 (95% CI, 1.05-2.25, p=0.028), 1.68 (95% CI, 1.10-2.57, p=0.017), and 1.98 (95%
CI, 1.33-2.94, p<0.001) in patients who received one, two, three, four, and five or more