R E S E A R C H A R T I C L E
Open Access
Acceptance of disability and its predictors among
stroke patients in Taiwan
Shan-Yun Chiu
1†, Hanoch Livneh
2†, Long-Lung Tsao
3and Tzung-Yi Tsai
4,5,6*Abstract
Background: Modern medicine has increased the survival rate for stroke patients; however, the patient’s
psychosocial adaptation after stroke onset may be related to the clinical outcomes. This study aimed to investigate patients’ acceptance of disability (AOD) and its predictors in stroke patients.
Methods: This cross-sectional study used a purposive sampling method to recruit 175 stroke patients from a hospital in southern Taiwan. A structured questionnaire gathered data on respondent demographics and disease characteristics, and included the Chinese version of the AOD Scale-Revised. Factors associated with AOD were examined by a multiple linear regression analysis.
Results: The mean AOD score was 71.72, which indicated a lower level of disease acceptance (range, 32-128). Our findings showed that patients who reported no religious beliefs, shorter disease duration, recurrent stroke episodes, and poorer physical functioning also reported lower levels of disability acceptance. These factors accounted for 38.2% of the variance in AOD among participants.
Conclusions: The findings are beneficial to healthcare providers by identifying those stroke patients with predisposition of having lower disability acceptance, which could then facilitate the provision of appropriate rehabilitation interventions within six months after the diagnosis of stroke to support their adaptation process. Keywords: Acceptance of disability, Stroke, Taiwan
Background
The World Health Organization (WHO) predicted that by 2020, stroke will be second only to ischemic heart disease as the leading cause of disability worldwide [1]. Given the complex symptoms and long duration of rehabilitation, the economic burden regarding stroke cannot be ignored. In the United States, more than 795,000 patients experi-ence a new or recurrent stroke each year, accounting for direct and indirect healthcare costs totaling $21.8 billion and $65.5 billion, respectively [2]. Furthermore, the esti-mated medical expenses for one stroke patient per admis-sion total approximately $20,000, which is three times the cost of care for a non-stroke patient [2].
Stroke does not only cause an enormous economic bur-den, but also triggers subsequent disability. For example, the risk of dementia for stroke patients is more than two-fold higher than for those without the disease [3]. A study by Koton et al. reported a 31.1% mortality rate for first-time stroke patients over a 3-year follow-up period [4]. The irreversible nature and unsatisfactory prognostic out-come associated with strokes often result in the develop-ment of psychiatric disorders, especially depression, in stroke patients. A previous study reported that the preva-lence of depression after a stroke ranged from 13% to 72%, with a pooled estimate of 30% [5]. It should be noted that the diagnosis of depression, or of other mental disor-ders, in a stroke patient is associated with a 13% higher risk of mortality compared to a non-stroke patient, which emphasizes the urgent importance of mental health care for stroke patients [6].
An important intervention during rehabilitation focuses on helping patients with chronic disease accept their dis-abilities, learn how to cope and live with them, and adapt * Correspondence:[email protected]
†Equal contributors
4Department of Medical Research, Dalin Tzuchi Hospital, The Buddhist Tzuchi
Medical Foundation, No. 2, Minsheng Rd., Dalin Township, Chiayi 62247, Taiwan
5
Department of Nursing, Tzu Chi College of Technology, No. 880, Chien-Kuo Rd. Sec. 2, Hualien 97005, Taiwan
Full list of author information is available at the end of the article
© 2013 Chiu et al.; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
to the ensued physical and psychosocial sequelae [7]. Some researchers have suggested that one key factor that could account for such variation in psychosocial adjust-ment is acceptance of disability (AOD) [8,9]. In order to specifically measure the AOD, Linkowski developed a scale with 50 items that was based on the concepts con-cerning acceptance of loss proposed by Wright. According to Wright’s theory, AOD is associated with viewing one’s disability as a non-devaluating part of life through per-sonal coping efforts and the realization that one can suc-cessfully overcome many of the imposed restrictions and limitations [10]. Recently, some studies involving patients with chronic diseases, such as those involving ostomy, spinal cord injury, insulin-dependent diabetes mellitus, and Ehlers-Danlos syndrome, have shown that higher levels of acceptance are associated with increased health-promoting behaviors, which could lower the risk of recur-rence and medical complications [9,11,12]. Therefore, periodic screening of AOD for stroke patients should be integrated into routine care practice.
Within the Chinese culture, a stigma has been at-tached to the diagnosis of psychiatric disorders [13], so most of the literatures about stroke patients focused on survival rates [14], disease prevalence [15], or length of hospital stay [16]. Presently, no substantial discussions of AOD in stroke cases have been reported in the litera-ture. Therefore, the aims of this study were to examine AOD and its related factors among patients with stroke in Taiwan, with the hope that these findings could be used as a reference for instituting appropriate psycho-physical interventions for Chinese stroke patients.
Methods
Study design and samples
This study applied a cross-sectional, correlational design with purposive sampling to recruit stroke patients from a hospital in Taiwan between June 2011 and July 2012. The inclusion criteria were as follows: (i) age≥20 years old; (ii) absence of cognitive impairments and ability to express opinions in either Mandarin or Taiwanese; (iii) experi-enced a hemorrhagic or ischemic stroke >3 months before the study; and (iv) no family history of psychiatric disor-ders. Additionally, the sample size needed for this study
was determined by the Cohen method [17], whereα was
set to 0.05, power to 0.8, and an effect size to 0.15, result-ing in the need for a sample of at least 139 patients.
Instruments
The Chinese Version of the Acceptance of Disability Scale-Revised (AODS-R) and an additional questionnaire that contained information on demographic and disease characteristics were used for data collection.
AODS-R was developed by Groomes & Linkowski in 2007 [10], and focused on the “enlargement of scope of
values,” “subordination of physique,” “containment of dis-ability effect,” and “transformation from comparative values to asset values”, all of which reflect Wright’s suc-cessful coping with disability paradigm. This revised scale consists of 32 items, which address individual attitude using a 4-point Likert scale ranging from 1 (strongly dis-agree) to 4 (strongly dis-agree). Of the 32 items, 10 reflect positive values (#3, 6, 12, 16, 18, 21, 25, 28, 29, and 32), and the remaining 22 items reflect negative items. The full-scale range is from 32 to 128, with higher scores indi-cating a higher level of disease or disability acceptance. In terms of psychometric characteristics of this revised scale, a principal component analysis extracted four factors cor-responding to the initial version. 42% of the total variance was explained, which indicates that the construct validity of the revised scale was acceptable. AODS-R scale has demonstrated good internal consistency among different groups of people with disabilities (Cronbach’s α between 0.91 and 0.93) [10,12].
The AODS-R has been translated into Chinese by Chiang et al. [8] in order to evaluate disease acceptance among Taiwanese chronic disease patients; these au-thors also examined the validity of the Chinese version by correlating it with the Taiwanese Depression Ques-tionnaire (TDQ) [18] and reported a significant correl-ation coefficient of -0.45 (P < 0.01). As for internal consistency estimates of the Chinese version of the AODS-R, the findings of the corrected item-total score correlation were positive and statistically significant (P < 0.05), ranging from 0.28 to 0.55. Cronbach’s α derived from the present data yielded a coefficient of 0.94.
The second part of the questionnaire contained infor-mation on demographic and disease characteristics and was developed from previous literature and clinical ex-periences. The demographic data collected included gender, age, marital status, education, monthly income, living status, religion, and certain lifestyle factors, such as smoking, exercise, and sleep. Those who answered “currently” or “yes/past” to smoking were classified as
smokers. Those who exercised ≥3 days per week were
classified as regular exercisers. With respect to sleep, those patients who have awakened >2 times per week were classified as having a sleeping disturbance. The disease characteristics included the presence of chronic disease (ie, diabetes mellitus, hypertension, heart dis-ease, or cancer), the number of strokes (first/recurrent), the type of stroke (hemorrhagic or ischemic), the dur-ation of the stroke (in months), the body side of lesion, and activities of daily living (ADL); for the latter vari-able, it was determined using Barthel index. Scores on Barthel index ranged from 0 to 100 with higher scores indicating better functioning. All disease characteristics were obtained from the patients’ medical records.
Data collection
This study was approved by the Institutional Review Board of Dalin Tzu Chi Hosiptal (B10001011). To ensure pa-tients’ rights, the researchers explained the purpose of the study and procedures to the patients. Informed consent was obtained after the patient understood and agreed to participate in the study. During completion of the ques-tionnaires, the researchers were available to answer any questions. For illiterate patients, the researchers read the questionnaires and recorded their answers. To ensure pa-tients’ anonymity, the questionnaires were returned with-out any identifying information on them. Patients were also assured of complete confidentiality of all obtained data and were given the option to withdraw from the study at any time without any penalty.
Data analysis
Data were analyzed using SPSS, version 17.0 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive and inferential statistical analyses were conducted in accordance with the study aims and the nature of the variables. Descriptive analyses, including means and standard deviations (SD), were used to describe the distributions of the demographic data and disease characteristics. Intergroup difference of AOD level was tested using independent t-test for categor-ical variables and Pearson correlation for continuous vari-ables, as appropriate. Variables that correlated significantly with the criterion measure (AOD level) were entered into multiple linear regression analysis to determine the signifi-cant predictors of disability acceptance.
To control for possible multicollinearity effects among AOD predictive variables, collinearity analyses, including tolerance value, variance inflation factor, and condition index, were performed before conducting the multivariate analysis. Also, the assumptions of normality, linearity, and homoscedasticity were tested. p-value was set at 0.05 for all statistical analyses.
Results
Demographic data and disease characteristics
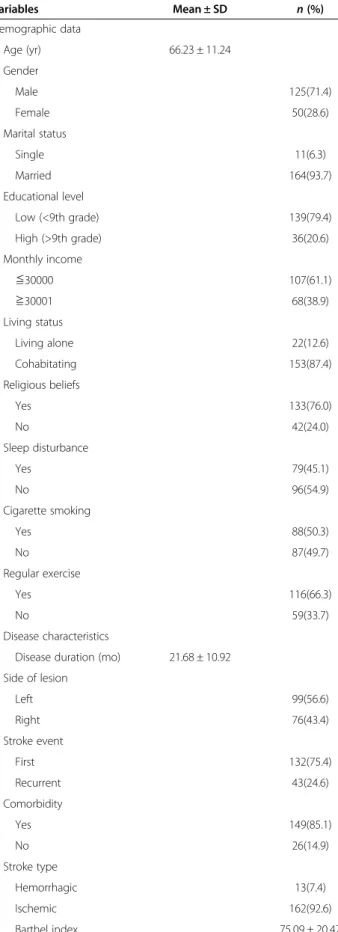
A total of 175 stroke patients with a mean age of 66.23 years (SD = 11.24) were recruited during the period of data collection. The majority were males (71.4%), mar-ried (93.7%), had a low educational level (below 9thgrade) (79.4%), and cohabitating (87.4%). The majority of patients
had a monthly income of New Taiwan Dollar (NTD)≤
30,000 (61.1%) and reported having religious beliefs (76.0%). Slightly less than a half reported sleep distur-bances (45.1%), and approximately half were smokers (50.3%). Two-thirds of the patients engaged in regular ex-ercise (66.3%). With regard to disease characteristics, the mean duration of stroke was 21.68 months (SD = 10.92), and the mean Barthel Index score was 75.09 (SD = 20.47). Most patients presented with an ischemic stroke (92.6%),
a left side lesion (56.6%), a first stroke event (75.4%), and experienced other comorbidities (85.1%) (Table 1).
AOD scores
The mean score of AOD level was 71.72, with a SD of
11.27. Of the four AODS-R subscales, “enlargement of
scope of values” had the highest standardized score (77.64), and “subordination of physique” had the lowest standardized score (43.95) (Table 2).
Correlations among demographic data, disease characteristics, and AOD scores
Table 3 shows the correlation between potential predictors and AODS-R. The results demonstrated that religious be-liefs and sleep disturbance were related to the level of AOD (t = 2.55,p = 0.01; t = 2.89, p = 0.004, respectively). In terms of disease characteristics, all measured disease char-acteristics correlated with AOD score, with the exception of lesion side of body. For example, patients with first-ever stroke (t = 2.74;p = 0.007), no other chronic diseases (t = 2.87;p = 0.005), or higher daily activity levels (r = 0.49; p < 0.001) had higher AODS-R scores than those without these condition. On the other hand, disease duration cor-related positively with AODS-R scores, indicating that higher AODS-R scores are related to longer disease dur-ation (r = 0.2;p = 0.008).
Our study indicated a positive relationship between the duration of stroke and the AOD level, implying that those with longer time since stroke episode reported more positive disability acceptance. In the further ana-lysis, we assessed the variation level of AOD within four different time periods (≤6 months, 7-12 months,
13-24 months, ≥25 months) and observed that the mean
AODS-R score was the lowest in patients with disease
duration≤ 6 months. Mean AOD scores for the four
time frames were 61.55 (SD = 9.17), 68.64 (SD = 15.70), 71.04 (SD = 12.79) and 74.19 (SD = 10.18), respectively (test for trend,p < 0.05) (Figure 1).
Related factors affecting AOD
Multiple linear regression analysis was applied to examine which variables contributed to acceptance among stroke patients. Table 4 reveals that four predictor variables, in-cluding the presence of religious beliefs, disease duration, stroke event, and Barthel index scores, accounted for 38.2% of the variance in AODS-R scores. In other words, stroke patients with longer disease duration, religious be-liefs, first-ever stroke and engaging in more daily activities reported higher levels of disability acceptance.
Discussion
In this study of patients who experienced stroke, we found a raw mean AOD score of 71.72, and a standardized score of 56.03. Compared with AOD scores of patients with
other chronic diseases assessed with the same tool (stan-dardized score 62-87) [11,12,19,20], stroke patients had re-markably lower AOD scores. These lower scores likely reflect the overall disease burden, associated with chronic physical, cognitive and emotional impairments and the en-countered economic and environmental barriers. For ex-ample, one study showed that the average hospital cost for a stroke patient is almost $20,000 dollars, which is nearly three times the cost for a non-stroke patient [21]; further-more, disability-adjusted life-years (DALY) lost from strokes has become the fourth highest among all diseases worldwide [1]. Stroke unquestionably has an enormous impact on the patient, the family, and society at large, which may reduce AOD level to some extent.
Table 2 further demonstrated that lower AOD scores are primarily reflections of the“subordination of physique” and “containment of disability effects” domains, implying that the motor impairment may play a predominate role affect-ing AOD level among stroke patients. Recently, modified constraint-induced movement therapy (CIMT) was proven to be the most promising intervention to strengthen the mobility and fluency of movement in the affected limbs [22]. A randomized clinical trial conducted by Wolf and colleagues evaluated the effect of CIMT for 6 hours per day for two weeks on stroke patients, and reported that the CIMT participants had greater improvements than the those in the control group in the time of Wolf Motor Func-tion Test (WMFT) and Motor Activity Log (MAL), by 34% and 43%, respectively [23]. Therefore, CIMT may be inte-grated into discharge planning in order to facilitate inter-ventions, which will increase the self-care ability of stroke patients [24].
We found that patients who reported having religious be-liefs had higher AOD scores than those who did not turn to religion. An earlier study had shown that religious beliefs was related to improved mental health [25]. People with ligious beliefs may have more intangible psychological re-sources and support through spiritual guidance along with a reduction in psychological stress. This, in turn, can en-hance the immune system and reduce symptoms associated
Table 1 Demographic and disease characteristics (N = 175)
Variables Mean ± SD n (%) Demographic data Age (yr) 66.23 ± 11.24 Gender Male 125(71.4) Female 50(28.6) Marital status Single 11(6.3) Married 164(93.7) Educational level Low (<9th grade) 139(79.4) High (>9th grade) 36(20.6) Monthly income ≦30000 107(61.1) ≧30001 68(38.9) Living status Living alone 22(12.6) Cohabitating 153(87.4) Religious beliefs Yes 133(76.0) No 42(24.0) Sleep disturbance Yes 79(45.1) No 96(54.9) Cigarette smoking Yes 88(50.3) No 87(49.7) Regular exercise Yes 116(66.3) No 59(33.7) Disease characteristics
Disease duration (mo) 21.68 ± 10.92 Side of lesion Left 99(56.6) Right 76(43.4) Stroke event First 132(75.4) Recurrent 43(24.6) Comorbidity Yes 149(85.1) No 26(14.9) Stroke type Hemorrhagic 13(7.4) Ischemic 162(92.6) Barthel index 75.09 ± 20.47
Table 2 Means and SD of the four AODS-R subscales (N = 175)
Dimension Mean SD Standardized
score(1)
Rank Transformation from comparative
values to asset values (9-36)
18.86 3.91 52.38 2 Enlargement of scope of values (9-36) 27.95 4.13 77.64 1 Containment of disability effect (9-36) 16.12 4.94 44.78 3 Subordination of physique (5-20) 8.79 1.96 43.95 4 Total scores (32-128) 71.72 11.27 56.03 (1)
with disease [26]. But our result is inconsistent with the findings of Chao et al. [19], who reported the null associ-ation between AOD level and religious beliefs among colo-rectal cancer patients. For most people, the diagnosis of cancer is psychologically associated with incurable illness or death, and often results in a significant psychological im-pact on people of Asian descent [27]. Therefore, the influ-ence of psychological and spiritual support from religion may not be so apparent for cancer patients.
The duration of disease was positively correlated with AOD, which is consistent with a previous argument that AOD research is more meaningful when conducted in the context of patients with chronic diseases [9,19]. We specu-late that stroke patients with a longer duration of disease have gradually learned to accept the consequences and fu-ture implications of their disability and thus have higher AOD scores. It is notable that patients whose duration of
disease was≤ 6 months had the lowest AOD scores. We
recommend that healthcare providers should pay greater attention to newly-diagnosed stroke patients by establish-ing a set of rehabilitation care process for evaluatestablish-ing their signs of psycho-physical status to facilitate early referral for further therapeutic interventions [28].
The findings of this study also indicate that AOD scores of recurrent stroke patients were lower than those of first-time stroke patients. This finding is consistent with a previ-ous argument that secondary stroke patients tend to become more distressed and therefore experience more negative emotions, such as anxiety, posttraumatic stress and depression [29,30]. Recurrent strokes often result in ag-gravated cerebral leukoaraiosis, and thus worsen limb dys-function and intellectual impairment [31,32]. Furthermore, recurrent stroke patients were found to have higher monthly medical expenditures than those with newly-diagnosed stroke by 375 US dollars [33], which may result in lower levels of AOD because of heavier economic bur-dens and concerns about their future.
Findings from our study also suggest that there was a significant positive correlation between mobility and AOD scores in stroke patients, echoing previous research find-ings about physical mobility and emotional distress [11,34]. Patients with greater mobility are more likely to be successfully integrated into social support networks, maintain good interpersonal relationships, require less help from others in daily activities, and thus have higher
Table 3 Relationships between demographic data, disease characteristics, and acceptance of disability (N = 175)
Variables AOD score
Mean SD t/r p Demographic data Age (yr) r = -0.03 0.73 Gender Male 71.73 11.59 t = -0.02 0.99 Female 71.70 12.14 Marital status Single 71.70 11.78 t = 0.11 0.91 Married 72.09 11.34 Educational level
Low (below 9th grade) 71.53 11.99 t = -0.44 0.66 High (above 9th grade) 72.50 10.72
Monthly income ≦30000 70.88 12.12 t = -1.20 0.23 ≧30001 73.06 11.01 Living status Living alone 73.72 8.83 t = 1.08 0.29 Cohabitating 71.44 12.08 Religious beliefs Yes 73.15 10.64 t = 2.55 0.01 No 67.21 13.83 Sleep disturbance Yes 68.96 12.86 t = 2.89 0.004 No 74.00 10.21 Cigarette smoking Yes 71.75 11.97 t = -0.03 0.98 No 71.70 11.53 Regular exercise Yes 71.48 11.92 t = 0.38 0.70 No 72.20 11.39 Disease characteristics
Disease duration (mo) r = 0.2 0.008
Side of lesion Left 71.42 12.22 t = 0.39 0.70 Right 72.19 11.11 Stroke event First 73.02 11.05 t = 2.74 0.007 Recurrent 67.35 12.96 Comorbidity Yes 70.68 11.32 t = 2.87 0.005 No 77.69 12.45
Table 3 Relationships between demographic data, disease characteristics, and acceptance of disability (N = 175) (Continued)
Stroke type
Hemorrhagic 65.84 12.78 t = 1.89 0.06
Ischemic 72.19 11.54
AOD scores. This finding is inconsistent with findings of other studies [35,36], however, this may be partially due to differences in sample size and age distribution of partici-pants. Previous studies all used the Barthel index to evalu-ate patient mobility and to analyze its relationship with depressed mood by surveying small numbers of patients (n≤ 50) [35,36]. Such small sample sizes may provide in-sufficient statistical power in multivariate analysis and thus fail to clarify the true relationships among variables. Fur-thermore, our subjects (≈ 67 years on average) were older than previously studied cases (46.01 and 51.40, respect-ively). It can be argued that with different physical, and possibly cognitive, functioning, the impact of impaired mobility on AOD would be different.
Although the results of this study provide for several im-portant clinical and research implications, a few limitations must be acknowledged. First, the study subjects were re-cruited from a single hospital, which may limit the generalizability of the findings. Future studies should use larger samples, including random or stratified sampling methods of data collection, to improve the sample repre-sentation. Nonetheless, we calculated a required sample size analysis to ensure statistical power before embarking on the study, and thus, the sample size used in this study may be considered satisfactory for exploring the predictors associated with AOD level in stroke patients. Second, since this study used a cross-sectional design, we cannot infer causality from our findings. A longitudinal research design is needed to examine any causal relationships among the factors assessed in this study. Furthermore, there is a need to investigate the relationship between AOD level and
subsequent clinical manifestations. Third, sleep disturbance and religious beliefs were only assessed with a single-item question, and therefore, their psychometric characteristic may be suspect and, accordingly, must be interpreted cau-tiously. Despite these methodological concerns, to our knowledge, this was the first study to assess the level of AOD among Taiwanese stroke patients, a fact which can be used as a future reference in developing the timely thera-peutic regimen.
Conclusion
In conclusion, advances in medical techniques have ex-tended survival of chronically-ill patients; however, cogni-tive, emotional and physical distress, triggered by both condition’s sequelae and its associated treatment modal-ities, may easily disrupt patients’ lives and induce further psychiatric symptoms. This study found that the mean AOD score among Taiwanese stroke patients was 71.72, suggesting a lower level of disability acceptance than that reported in earlier studies. Among stroke patients, those with no religious beliefs, with shorter duration of disease, with recurrent stroke, or with poor ability to perform daily activities, reported lower AODS-R scores. Healthcare pro-viders should consider instituting an appropriate rehabili-tation care procedure for stroke patients, supplemented by a clinically-validated and psychometrically sound assess-ment tool. Actually, it is imperative to help patients better psychologically adapt to their disease and possibly as im-portant as improving the survival rate of patients with the chronic and life threatening disease.
Abbreviations
AOD:Acceptance of disability; AODS-R: Acceptance of disability scale-revised; TDQ: Taiwanese depression questionnaire; SD: Standard deviations; NTD: New Taiwan dollar; DALY: Disability-adjusted life-years. Competing interests
No conflict of interest has been declared by the authors. Authors’ contributions
SYC was responsible for data collection and participated in providing comments on the manuscript drafts. HL contributed to the interpretation of data and providing comments on the final draft of the manuscript. LLT provided administrative support and comments on the manuscript drafts. TYT was responsible for the study conception, design, data analysis, and drafting of the work. All authors read and approved the final manuscript. Acknowledgements
This study was supported by grants from Buddhist Dalin Tzuchi General Hospital (DTCRD101-I-10; DTCRD100(2)-I-08). We thank the co-investigator of this project and the participants who responded our survey.
Author details
1Department of Nursing, Dalin Tzuchi Hospital, The Buddhist Tzuchi Medical
Foundation, No. 2, Minsheng Rd., Dalin Township, Chiayi 62247, Taiwan.
2Rehabilitation Counseling Program, Portland State University, PO Box 751,
Portland, OR 97207-0751, USA.3Department of Neurology, Dalin Tzuchi Hospital, The Buddhist Tzuchi Medical Foundation, No. 2, Minsheng Rd., Dalin Township, Chiayi 62247, Taiwan.4Department of Medical Research, Dalin Tzuchi Hospital, The Buddhist Tzuchi Medical Foundation, No. 2, Minsheng Rd., Dalin Township, Chiayi 62247, Taiwan.5Department of Nursing, Tzu Chi College of Technology, No. 880, Chien-Kuo Rd. Sec. 2, Hualien 97005, Taiwan.
20 40 60 80
6 months 7-12months 13-24 months 25 months
p<0.05 p=0.08
p=0.17
Figure 1 AODS-R scores among four groups within different disease duration.
Table 4 Multivariate regression analysis predicting AODS-R scores among stroke patients (N = 175)
Variables β coef. t p VIF
Religious beliefs (Yes vs No) 4.61 2.66 <0.01 1.02
Disease duration 0.13 2.34 0.02 1.03
Stroke event (Recurrent vs First) −4.05 −2.32 0.02 1.05
Barthel index 0.22 5.56 <0.01 1.21
【β coefficient with positive values indicate higher level of AOD; negative values reflect lower level of AOD】.
6Department of Environmental and Occupational Health, College of
Medicine, National Cheng Kung University, No. 138, Sheng-Li Rd., Tainan 70428, Taiwan.
Received: 29 June 2013 Accepted: 7 November 2013 Published: 14 November 2013
References
1. World Health Organization: The global burden of disease: 2004 update; 2011. http://www.who.int/healthinfo/global_burden_disease/ GBD_report_2004update_full.pdf.
2. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, et al: Heart disease and stroke statistics–2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee.
Circulation 2009, 119:e1–e161.
3. Ivan CS, Seshadri S, Beiser A, Au R, Kase CS, Kelly-Hayes M, Wolf PA: Demen-tia after stroke: the Framingham Study. Stroke 2004, 35:1264–1268. 4. Koton S, Tanne D, Green MS, Bornstein NM: Mortality and predictors of
death 1 month and 3 years after first-ever ischemic stroke: data from the first National Acute Stroke Israeli Survey (NASIS 2004).
Neuroepidemiology 2010, 34:90–96.
5. Paolucci S: Epidemiology and treatment of post-stroke depression. Neuropsychiatr Dis Treat 2008, 4:145–154.
6. Williams LS, Ghose SS, Swindle RW: Depression and other mental health diagnoses increase mortality risk after ischemic stroke. Am J Psychiatry 2004, 161:1090–1095.
7. Livneh H, Antonak RF: Psychosocial adaptation to chronic illness and disability: a primer for counselors. J Counsel Dev 2005, 83:12–20. 8. Chiang HH, Lai NS, Livneh H, Yeh ML, Tsai TY: Validity and reliability of
Chinese version of acceptance of disability scale-revised. Tzuchi Nurs J 2013, 12:66–76.
9. Attawong T, Kovindha A: The influencing factors of acceptance of disability in spinal cord injuries patients. Nepal J Neurosci 2005, 2:67–70. 10. Groomes DAG, Linkowski DC: Examining the structure of the revised
acceptance disability scale. J Rehabil 2007, 73:3–9.
11. Berglund BA, Mattiasson AC, Nordstrom G: Acceptance of disability and sense of coherence in individuals with Ehlers-Danlos syndrome. J Clin Nurs 2003, 12:770–777.
12. Chen RK, Crewe NM: Life satisfaction among people with progressive disabilities. J Rehabil 2009, 75:50–58.
13. Yeh YH, Lin HC: A questionnaire study of depression related help-seeking behavior among the general public in Taiwan. Formos J Ment Health 2006, 19:125–148.
14. Chang KC, Lee HC, Tseng MC, Huang YC: Three-year survival after first-ever ischemic stroke is predicted by initial stroke sfirst-everity: a hospital-based study. Clin Neurol Neurosurg 2010, 112:296–301.
15. Liao CC, Li TC, Lin RS, Sung FC: Urban and rural difference in prevalence and incidence of stroke in 2000 in Taiwan. Taiwan J Public Health 2006, 25:223–230.
16. Lee HC, Chang KC, Lan CF, Hong CT, Huang YC, Chang ML: Factors associated with prolonged hospital stay for acute stroke in Taiwan. Acta Neurol Taiwan 2008, 17:17–25.
17. Cohen J: A power primer. Psychol Bull 1992, 112:155–159.
18. Lee Y, Yang MJ, Lai TJ, Chiu NM, Chau TT: Development of the Taiwanese depression questionnaire. Chang Gung Med J 2000, 23:688–694. 19. Chao HL, Tsai TY, Livneh H, Lee HC, Hsieh PC: Patients with colorectal
cancer: relationship between demographic and disease characteristics and acceptance of disability. J Adv Nurs 2010, 66:2278–2286. 20. Richardson A, Adner N, Nordström G: Persons with insulin-dependent
dia-betes mellitus: acceptance and coping ability. J Adv Nurs 2001, 33:758–763. 21. Luengo-Fernandez R, Gray AM, Rothwell PM: Costs of stroke using
patient-level data: a critical review of the literature. Stroke 2009, 40:e18–e23. 22. Langhorne P, Coupar F, Pollock A: Motor recovery after stroke: a
systematic review. Lancet Neurol 2009, 8:741–754.
23. Wolf SL, Winstein CJ, Miller JP, Uswatte G, Morris D, Giuliani C, Light KE, Nichols-Larsen D, EXCITE Investigators: Effect of constraint-induced move-ment therapy on upper extremity function 3 to 9 months after stroke: the EXCITE randomized clinical trial. JAMA 2006, 296:2095–2104. 24. Miller EL, Murray L, Richards L, Zorowitz RD, Bakas T, Clark P, Billinger SA,
American Heart Association Council on Cardiovascular Nursing and the
Stroke Council: Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke patient: a scientific statement from the American Heart Association. Stroke 2010, 41:2402–2448.
25. Levin J: Religion and mental health: theory and research. Int J Appl Psychoanal Stud 2010, 7:102–115.
26. Coruh B, Ayele H, Pugh M, Mulligan T: Does religious activity improve health outcomes? A critical review of the recent literature. Explore 2005, 1:186–191.
27. Chung KH, Lin HC: Methods of suicide among cancer patients: a nationwide population-based study. Suicide Life Threat Behav 2010, 40:107–114.
28. Poynter B, Shuman M, Diaz-Granados N, Kapral M, Grace SL, Stewart DE: Sex differences in the prevalence of post-stroke depression: a systematic review. Psychosomatics 2009, 50:563–569.
29. Andersen G, Vestergaard K, Riis J, Lauritzen L: Incidence of post-stroke depression during the first year in a large unselected stroke population determined using a valid standardized rating scale. Acta Psychiatr Scand 1994, 90:190–195.
30. Barton J: Stroke and rehabilitation: Psychological perspectives. In The Oxford Handbook of Rehabilitation Psychology. Edited by Kennedy P. Oxford: Blackwell Science; 2012:235–247.
31. Ay H, Arsava EM, Rosand J, Furie KL, Singhal AB, Schaefer PW, Wu O, Gonzalez RG, Koroshetz WJ, Sorensen AG: Severity of leukoaraiosis and susceptibility to infarct growth in acute stroke. Stroke 2008, 39:1409–1413. 32. Schneider JA, Wilson RS, Cochran EJ, Bienias JL, Arnold SE, Evans DA,
Bennett DA: Relation of cerebral infarctions to dementia and cognitive function in older persons. Neurology 2003, 60:1082–1088.
33. Samsa GP, Bian J, Lipscomb J, Matchar DB: Epidemiology of recurrent cerebral infarction: a medicare claims–based comparison of first and recurrent strokes on 2-year survival and cost. Stroke1999, 30:338–349. 34. van de Port IG, Kwakkel G, Bruin M, Lindeman E: Determinants of
depression in chronic stroke: a prospective cohort study. Disabil Rehabil 2007, 29:353–358.
35. Cassidy E, O'Connor R, O'Keane V: Prevalence of post-stroke depression in an Irish sample and its relationship with disability and outcome follow-ing inpatient rehabilitation. Disabil Rehabil 2004, 26:71–77.
36. Srivastava A, Taly AB, Gupta A, Murali T: Post-stroke depression: prevalence and relationship with disability in chronic stroke survivors. Ann Indian Acad Neurol 2010, 13:123–127.
doi:10.1186/1471-2377-13-175
Cite this article as: Chiu et al.: Acceptance of disability and its predictors among stroke patients in Taiwan. BMC Neurology 2013 13:175.
Submit your next manuscript to BioMed Central and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit