Traumatic Left Main Coronary Artery Dissection with Acute Myocardial Infarction after
Chest Contusion
Keng-Yi Wu
1,2, and Jou-Hong Lai
11
Department of Cardiology, Department of Internal Medicine,
Taichung Armed-Forces General Hospital, Taichung, Taiwan, Republic of China;
2
Division of Cardiology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China
Abstract
Blunt chest contusion can rarely induce coronary artery dissection with myocardial infarction. Clin- ical symptoms, electrocardiography, and serial cardiac enzyme evaluations are necessary in patients with thoracic trauma. Angioplasty or bypass surgery is chosen according to the lesion characteristics and associ- ated complications. Here, we report a case of a dissected flap from the left main coronary artery to the left anterior descending coronary artery in a 63-year-old man with acute myocardial infarction secondary to blunt chest trauma during a traffic accident. (J Intern Med Taiwan 2016; 27: 261-266)
Key Words: Chest contusion, Coronary artery dissection, Myocardial infarction
Background
Acute myocardial infarction can be caused by atherosclerosis, dissection, thromboembolism, vasculitis, congenital abnormality or procedure- related.
1Thoracic injury often causes subcutane- ous ecchymosis, rib fracture or pneumothorax.
2However, coronary artery injury rarely occurs as a consequence of trauma. Moreover, left main coro- nary artery dissection secondary to blunt trauma is particularly rare. We report a case of traumatic left main coronary artery dissection complicated with acute myocardial infarction in a 63-year-old man involved in a traffic accident.
Case Presentation
A 63-year-old man, a heavy smoker, had no history of comorbidities such as hypertension, dia- betes or coronary artery disease. The patient was involved in a road traffic accident while driving a motor vehicle at a speed of 70 kilometer/per hour.
In response to the impact, the patient directly hit the handle bar with chest contusion, and fall down then. So, he was brought to our emergency depart- ment with alert consciousness state, multiple abra- sion wounds of trunk and deformity of right lower limb. On arrival, he presented stable vital signs and blood pressure of 119/72 mmHg, heart rate of 68
Reprint requests and correspondence:Dr. Jou-Hong Lai
Address:Division of Cardiology, Taichung Armed Forces General Hospital, and Basic Science, Central Taiwan University of Science and Technology, No.348, Section 2, Chung-shan Road, Taiping 41168, Taichung, Taiwan, Republic of China
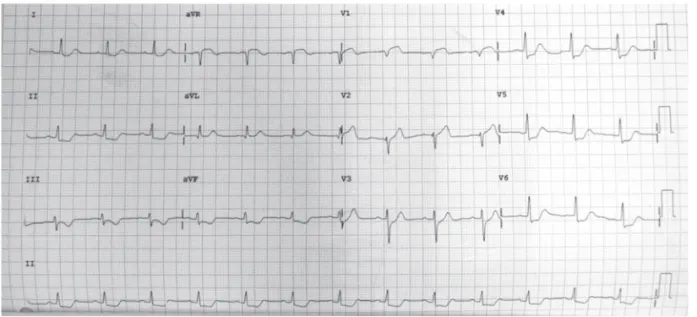
beats/min, respiratory rate of 20 breaths/min, and Glasgow Coma Scale Score of 15. Physical exam- ination revealed multiple facial abrasion injuries, deformities of nasal bone and right lower leg and ecchymosis injury over the anterior chest wall. No other significant or abnormal findings such as rib fracture, pneumothorax or subcutaneous emphy- sema were observed on a chest radiograph. Initial electrocardiography revealed normal sinus rhythm without ST-T segment change (Fig. 1). Abdomi- nal computed tomography (CT) and brain CT did not show intra-abdominal haemorrhage, abdomi-
nal aortic aneurysm or intra-cranial haemorrhage.
After completion of preliminary protocols, includ- ing blood laboratory tests, imaging studies, and fluid supplementation, the patient admitted for external fixation operation of right leg deform- ity. However, the patient gradually developed chest tightness without tearing, ripping sensation but presented a drop in blood pressure (54/42 mmHg).
Follow-up electrocardiography (ECG) revealed dif- fused ST-T segment depression across all leads, rather than elevation in the aVR lead (Fig. 2). Blood laboratory test showed creatinine kinase level of
Figure 1. Normal electrocardiogram initially.
Figure 2. ST segment elevation in the aVR and V1 leads with diffuse ST segment down-sloping in the other leads.
78.6 U/L (normal range, 25–192 U/L), an MB frac- tion of 77.6 U/L (normal range, 0–23 U/L), a Tro- ponin-I level of 0.13 ng/mL (normal range, <0.4 ng/
mL) 3 hours later after the accident. But there was no available echocardiography screen at that time.
However, the patient had typical angina manifes- tation and dynamic ECG changing, we arranged emergent coronary artery angiography examination.
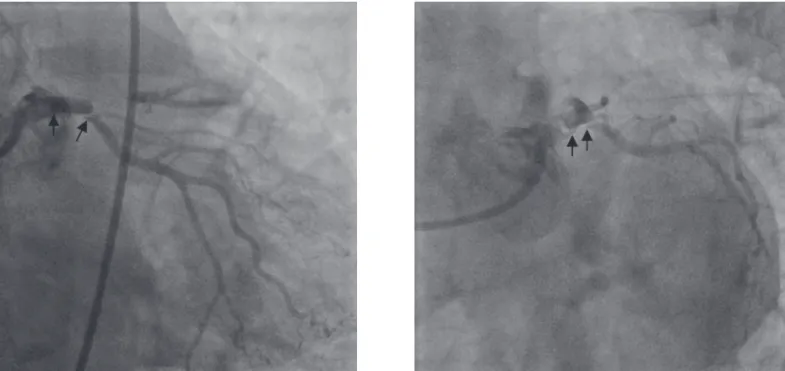
Intra-aortic balloon pump and vasopressors were also used to sustain cardiac function and arterial blood pressure. Emergent coronary artery angiog- raphy showed a small dissected flap over the proxi- mal part of left main coronary artery (LMCA) with minimizing blood flow in left anterior descending coronary artery (LAD) but good distal run-off in left circumflex coronary artery (LCX) was found initially (Fig. 3). After repeat testing with contrast medium injection, we identified minimal compro- mised antegrade blood flow in LCX. So, an iatro- genic extended dissected flap was highly suspected via following coronary artery angiograghy (Fig. 4).
We immediately deployed a 3.5 × 33 mm bare metal stent stent (BMS) and a 3.0 × 30 mm BMS from the proximal part of LMCA to the proximal part of LAD and to the proximal LCX sequentially with
Cullotte technigue. So, well distal coronary artery blood flow in left coronary artery after the proce- dure was achieved (Fig 5). The patient also got the improved angina symptom and stable vital sign after emergent coronary artery stenting.
Then, the patient underwent the procedure of open reduction with internal fixation operation of the fractured leg on the 8th day of hospitaliza- tion. Anti-coagulants and anti-platelet agents were administered on the 10
thday, with no evidence of bleeding during hospitalization. The patient was discharged on the 20th days with normal left ven- tricular function.
Discussion
Blunt chest wall injury is often encountered in the emergency department. Although cardiac injury has rarely been reported in association with chest trauma, it can lead to lethal conditions such as cardiac rupture or coronary artery dissection. Trau- matic coronary artery dissection was first described by Kohli et al. in 1988.
1The mechanism of dissection included intimal tearing with intraluminal throm- bosis or coronary artery spasm, with direct injury or deceleration effects. The most common clinical
Figure 3. The dissected flap from LMCA to proximal LAD with compromised antegrade blod flow (arrow).
symptom of myocardial infarction is chest pain, but it should be differentiated from musculoskeletal injuries, pneumothorax, cardiac rupture, pericardial tamponade, and cardiac arrhythmia.
2According to the anatomy of the coronary artery, the left ante- rior descending coronary artery is the most com- monly affected vessel (71.4%), followed by the right
coronary artery (19%), left main coronary artery (6.4%), and circumflex coronary artery (3.2%). At times, two vessels may be involved.
3There are few reported cases of a dissected flap from the left main to the left ascending coronary artery.
4,5Apart from lethal conditions, early detection of traumatic myocardial infarction in the emergency department is very important. The Eastern Associa- tion for the Surgery of Trauma guidelines recom- mend that echocardiography should be reserved for patients who present with hypotension or other unstable conditions, even if there are no initial abnormalities on electrocardiograms or in cardiac enzyme levels.
6,7,8In addition, in our case, manual injection of contrast may further extend the dissected flap to the distal vessel.
9Therefore, we should detect the dis- sected flap in the coronary artery before invasive therapy. So, coronary computed tomography (CTA) may play a diagnostic role in coronary artery dis- section in the emergency department; however, it is expensive and provides suboptimal radiographic images and causes an increase in heart rate. Intra- vascular ultrasound (IVUS) enables qualitative and
Figure 4. The extended dissected flap from LMCA to proximal LCX with compromised distal flow (arrow) after repeatintra-coronary contrast medium testing.
Figure 5. Good left coronary artery distal run-off was achieved after Cullotte stenting (arrow).
quantitative evaluation of the dissected coronary artery and provides useful information for deter- mining a suitable strategy for the evaluation of a dissected flap before repeat testing with contrast medium injection and for the prevention of such iat- rogenic complications.
10Anti-coagulants and anti-platelet agents should be used after stent implantation. However, physi- cians should adjudge the risk of haemorrhage and stent thrombosis in these kinds of patients. Throm- bolysis is not advised because of the risk of bleeding from associated injuries.
11,12In our patient, clopi- dogrel and aspirin were administered 2 days after reduction and fixation of the limb fracture, and there were no obvious complications at the 3-month follow-up.
Conclusion
Early recognition of this clinical entity via screening electrocardiogram in the emergency department and taking advanced management of emergent coronary angiography with stent place- ment could result in a favorable outcome, like our case.
References
1. Kohli S, Saperia GM, Waksmonski CA, Pezzella S, Singh JB.
Coronary artery dissection secondary to blunt chest trauma.
Cathet Cardiovasc Diagn 1988;15:179-83.
2. Chang YC, Wang CH, Han YY, Ko WJ, Lee YC. Successful treatment of traumatic coronary artery dissection with angio- graphic stenting. Am J Emerg Med 2010; 28: 113.e1-113.e4.
3. Hobelmann A, Pham JC, Hsu EB. Case of the month: Right coronary artery dissection following sports-related blunt trauma. Emerg Med J 2006; 23: 580-3.
4. Lai CH, Ma T, Chang TC, Chang MH, Chou P, Jong GP. A case of blunt chest trauma induced acute myocardial infarc- tion involving two vessels. Int Heart J 2006; 47: 639-43.
5. Lin YL, Yu CH. Acute myocardial infarction caused by coro- nary artery dissection after a blunt chest trauma. Intern Med 2011; 50: 1969-71.
6. Altekin RE, Er A, Oktay C, Baktir AO, Yanikoglu A, Yalcin- kaya AS, Kavasog ME. Acute anterior myocardial infarction after being struck on the chest by a soccer ball. Hong Kong J Emereg Med 2011; 18: 120-4.
7. James MM, Verhofste M, Franklin C, Beilman G, Goldman C.
Dissection of the left main coronary artery after blunt thoracic trauma: Case report and literature review. World J Emerg Surg 2010; 5: 21.
8. Keith Clancy, MD, Catherine Velopulos, MD, Jaroslaw W.
Bilaniuk, MD, et al. Screening for blunt cardiac injury: An Eastern Association for the Surgery of Trauma practice man- agement guidelineTrauma Acute Care Surg 2012; 73(suppl 4): s301-6
9. Antoniades D, Apostolakis S, Tzoras S, Lazaridis K. Iatro- genic right coronary artery dissection distal to a total occlu- sion: a case report. Cases Journal 2009; 2: 6797.
10. Bjørnstad JL, Pillgram-Larsen J, Tønnessen T. Coronary artery dissection and acute myocardial infarction following blunt chest trauma. World J Emerg Surg 2009; 4: 14.
11. Chun JH, Lee SC, Gwon HC, et al. Left main coronary artery dissection after blunt chest trauma presented as acute ante- rior myocardial infarction: assessment by intravascular ultra- sound: a case report. J Korean Med Sci 1998; 13: 325-7.
12. D Leong, M Brown. Blunt traumatic dissection of the proxi- mal left anterior descending artery. Emerg Med J 2006;23:e67 doi:10.1136/emj.2006.041426.
創傷性左冠狀動脈主幹枝剝離併急性心肌梗塞
吳耿逸1,2 賴昭宏1
1國軍台中總醫院 心臟內科
2國防醫學院三軍總醫院 心臟內科
摘 要