行政院國家科學委員會專題研究計畫 成果報告
腦血管疾病之存活及生活品質研究(3/3)
計畫類別: 整合型計畫 計畫編號: NSC91-2314-B-002-132-M56 執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立臺灣大學醫學院神經科 計畫主持人: 鄭建興 共同主持人: 葉炳強,陳思遠 報告類型: 完整報告 處理方式: 本計畫可公開查詢中 華 民 國 92 年 11 月 4 日
腦血管疾病之存活及生活品質研究(3/3)
Survival and Quality of Life after Cerebrovascular Disease (3/3)
目 錄
內 容
頁 次
中文摘要 2-3
英文摘要 4-5
研究背景 6-9
研究目的 10
研究方法 11-13
結果 14-17
討論與結論 18-20
參考文獻 21-25
圖表 26-50
附件 51-59
中文摘要:
關鍵詞:腦血管疾病、腦梗塞、腦出血、存活分析、健康相關生活品質
背景及目的:台灣地區在過去三十多年,腦中風一直是重要的死因之一,也是中老 年人身心障礙的主因。過去台灣地區腦中風的流行病學研究包括了死亡率、發生率與盛 行率等的研究,但缺乏長期的存活分析研究,且健康相關生活品質(Health related quality of life, HRQOL)的研究對於台灣地區主要疾病的腦中風愈形重要。本研究以台大醫院的 腦中風登錄為基礎,探討腦中風的長期存活及即決定因子與腦中風的 HRQOL。 研究方法:台大醫院的腦中風登錄開始於 1995 年 1 月,所有住院或經急診處診治 的急性腦中風病患均包括於登錄之中,每年約有一千名個案進入登錄。腦中風區分為腦 梗塞、腦內出血、蜘蛛網膜下出血及短暫缺血發作。腦梗塞進一步區分為五種亞型:大 動脈粥狀硬化型、小洞腦梗塞、心因性血栓腦梗塞、其他特定原因型及原因未明。腦內 出血則區分為高血壓性腦內出血、其他原因的腦內出血與原因未定的腦內出血。對於每 一個案均標準化登錄腦血管疾病相關危險因子。藉由台大醫院的病歷資料與台灣地區的 死因登錄資料檔,分析 1995 年至 2000 年的所有腦中風登率病患的長期存活情況,並探 討各種不同腦中風形態的存活決定因子。利用 Kaplan-Meier 方法求得 6 個月、1 年、3 年、6 年的腦中風存活率,而 Cox proportional hazard 迴歸分析方法求得存活相關的危險 因子。HRQOL 的測量則以台大醫院腦血管疾病特別門診的腦中風患者,以問卷方式紀 錄 350 至 400 名腦中風患者的基本資料、腦中風形態、危險因子、NIH stroke scale、Barthel index、modified Rankin scale、WHOQOL-BREF Taiwan version、stroke specific QOL 等,
分析不同腦中風形態的 HRQOL、整體 QOL 較中風前差或不變的差別。
研究結果:1995 至 2000 年的台大醫院的腦中風登共有 5024 位初發腦中風(男性 2902 位,女性 2122 位,平均年齡為 62.8+15.6 歲,年齡分佈為 1-100 歲),每一個案平 均追蹤時間(發病至死亡時間或發病至 2000 年 12 月 31 日)為 2.18+1.82 年。初發腦中
風包括 3349 位腦梗塞、1163 位腦內出血、276 位蜘蛛網膜下出血及 236 位短暫缺血發 作。個案追蹤登錄為死亡的比率為腦梗塞(23.3%)、腦內出血(38.1%)、蜘蛛網膜下出 血(42.8%)及短暫缺血發作(9.8%)。比較初發腦中風、初發腦梗塞中風與初發腦內出 血的各形態的存活狀況,均有顯著差異存在,特別是在疾病早期差異非常顯著(p 值均 <0.001)。以 Cox proportional hazard model 決定存活的顯著獨立因子,包括男性、年齡 >65 歲)、無高血壓、糖尿病、缺血性心臟病、心房顫動、腦中風發生於住院時、腦內 出血與蜘蛛網膜下出血等的初發腦中風存活率較低。而對於初發腦梗塞中風病患,年齡 >65 歲、心房顫動、血糖值>140mg/dl、血容積比<36%、腦中風發生於住院時與嚴重頸
動脈狹窄的存活率較低。腦中風的 HRQOL 共有 324 位接受訪查,其中有 257 位為初發 腦梗塞中風患者。針對腦中風患者自行感受整體生活品質是否較中風前差或是不變, SS-QOL 分數(勝算比為 3.3,95%信賴區間為 1.7-6.4,p 值<0.001)、NIH stroke scale(勝 算比為 0.7,95%信賴區間為 0.6-1.0,p 值=0.037)、與 WHOQOL-BREF 分數(勝算比為 1.1,95%信賴區間為 1.0-1.2,p 值=0.011),其它基本資料、中風類型、巴式量表則無顯 著區別能力。
結論:不同型態的腦中風的存活時間有很大的差異,年齡、心臟疾病與中風類型顯 著影響腦中風的存活時間。SS-QOL、NIH stroke scale 與 WHOQOL-BREF 可明顯決定腦 中風患者是否感受整體生活品質因中風有改變。
英文摘要:
Keywords:cerebtrovascular disease, cerebral infarct, cerebral hemorrhage, health related quality of life, survival analysis
Background and Purposes: Stroke is still one of the most important causes of mortality
and morbidity in Taiwan. In past, there was few study concerning about long-term survival
and health related quality of life (HRQOL) of stroke in Taiwan. This study are aimed to
investigate the survival function in stroke and its subtypes and factors related to stroke
survival time; and to analyze HRQOL in different types of stroke.
Subjects and Methods: From January 1995 to December 2000, patients who had acute
stroke occurrence before and during hospitalization at the NTUH were recruited into this
long-term follow-up study. Stroke was categorized into cerebral infarct (CI), cerebral
hemorrhage (CH), subarachnoid hemorrhage (SAH) and transient ischemic attack (TIA). CI
was further categorized into 5 subtypes: large artery atherosclerosis, lacune, cardioembolism,
other specific causes and undetermined. CH was categorized as hypertensive, other secondary
causes, undetermined. Demographic data and stroke related risk factors were recorded in each
patient. Survival time was calculated from the stroke onset to death or till the study endpoint
(31 December 2000). Factors predicting the stroke survival time were assessed. The HRQOL
of stroke patients were assessed in 350-400 patients by the Taiwan version of WHOQOL and
stroke-specific QOL (SS-QOL) questionnaires. Demographic variables and outcome measure
scores were compared between patients rating their overall HRQOL the same as prestroke
versus those with overall HRQOL worse than prestroke.
Results: From 1995 to 2000, there were 5024 first-ever stroke patients (male, 2902;
TIA in 236. Of all, the survival rates at 1 month, 6 months, 1 year, 3 years, and 6 years were
88.2%, 83.1%, 79.9%, 72.0% and 61.9%, respectively. The survival rates of CH and SAH
were lower than CI and TIA. There were significant differences among subtypes of stroke (x2
value by log-rank test = 200.5, p-value < 0.0001); and among subtypes of CI (x2 value by
log-rank test = 172.9, p-value <0.0001). By Cox proportional hazard model, male sex, age >
years, diabetes mellitus, ischemic heart disease, atrial fibrillation, stroke subtypes of CH and
SAH were significantly related to poor survival time in overall first-ever stroke patients. A
total of 324 stroke patients were evaluated. Of these, 257 patients with first-ever cerebral
infarct were analyzed. Independent predictors of good overall HRQOL were the SS-QOL
score (OR, 3.3; 95% CI, 1.7-6.4; p<0.001), NIH stroke scale (OR, 0.7; 95% CI, 0.6-1.0;
p=0.037), and WHOQOL-BREF score (OR, 1.1; 95% CI, 1.0-1.2; p=0.011). Demographic
factors, stroke subtypes, Barthel index, and modified Rankin scale were not associated with
overall HRQOL of stroke
Conclusions: The survival time differed significantly among types of stroke, and
subtypes of CI. Age, cardiac disease and CVD types were the major determinants of survival
time. SS-QOL, NIH stroke scale and WHOQOL-BREF predict patient-reported overall
研究背景:
台灣地區在過去三十多年,腦血管疾病(Cerebrovascular Disease, CVD)一直是重 要的死因之一。1982 之前,CVD 是國人十大死因的第一位,1982 年後仍佔十大死因的 第二位,僅次於癌症(Hung 1993, Chang et al 1993)。根據 2002 年的衛生署死因統計, 台灣地區當年約有 12,009 人死於 CVD(約占當年所有死亡者的 9.46%)。過去二十年台 灣地區對於 CVD 的流行病學研究方法主要可分為:(1)以社區為主的流行病學研究;(2) 以生命統計資料為主的研究;及(3)以醫院為主的流行病學研究。 在以社區為主的 CVD 流行病學研究,主要在探討 CVD 的發生率、盛行率及危險因 子的相對危險性,胡等在台灣四地區所做的 CVD 研究,36 歲以上 CVD 的發生率約為 千分之 3.3,腦梗塞佔 71%,腦出血佔 22%(Hu et al 1992);張等在蘭陽地區的流行病 學研究,45 歲以上 CVD 的發生率約為千分之 4.78,腦梗塞佔 64%,腦出血佔 36%,隨 著年齡的增長 CVD 的發生率明顯上昇(Chang et al 1995)。在 CVD 盛行率研究上,胡 等於 1986 年的研究,36 歲以上 CVD 的盛行率為千分之 16.42,腦梗塞佔 67%,腦出血 佔 14%,蜘蛛網膜下出血佔 4%(Hu et al 1989);李源德教授主持的金山心血管流行病 學研究於 1991 年的結果顯示,CVD 的盛行率為為千分之 21.8(Lee 1992);黃等在 1994 年的台灣多地區的 CVD 盛行率調查研究,台灣地區 CVD 的粗盛行率為千分之 5.95,男 女比為 1.17,兩年累積死亡率為 25.4%(Hwang et al 1997)。以生命統計資料為主的研 究主要依據衛生暑的死因登錄檔,可供分析死因變遷、年齡世代效應等,在張等的死亡 率變遷研究,台灣地區自 1974 年至 1988 年,CVD 的死亡率逐漸下降,腦出血下降驅 勢較腦梗塞更為顯著(Chang and Chen 1993)。而以醫院為主的流行病學研究,主要是以醫院的腦中風登錄為基礎,先有劉醫師於 1980 年的長庚醫院腦中風登錄(Ryu 1986),其後有李醫師的國泰醫院腦中風登錄(Lee 1989),洪教授的大規模台灣地區 26 家醫院腦中風登錄(Hung 1987&1992),1994 年徐
醫師的長庚醫院第二次腦中風登錄(Hsu et al 1995),葉與鄭等於 1995 年於台大醫院開 始腦中風登錄研究(Yip et al 1997a & 1997b, Jeng et al 1998)。以醫院為基礎的腦中風登 錄研究有別於以社區為主的 CVD 流行病學研究,以醫院為主的 CVD 研究雖無法求得發 生率及盛行率及相關危險因子,但醫院可以對 CVD 更深入了解其病程、危險因子、病 變位置及致病機轉、併發症、治療反應、短期疾病致死率、短中期功能預後等,這些多 是社區研究無法達成的,故近 10-20 年醫院腦中風登錄形成 CVD 研究的重要方法之一。 對於 CVD 的死亡率或存活率分析研究,腦中風發生後 30 日致死率於 1980 年長庚 醫院的腦中風登錄為 22.3%(Ryu 1986),1985 年洪教授的 26 家醫院腦中風登錄為 16.8% (Hung 1992),至 1995 年台大醫院的 10.9%(Jeng et al 1998),其中腦梗塞為 5.6%,腦 出血為 24.1%,蜘蛛網膜下出血為 30%。長期的存活率分析主要有洪教授於 1988-1992 共 23910 例腦中風病患登錄研究,一年的存活率為 74.3%,二年為 67.7%,26 家醫院腦 中風登錄可能是急性 CVD 的 30 日死亡率約為 10%-20%(Hung 1992)。 事實上,CVD 不僅是重要的死亡原因,更是中老年人身心障礙的主因。根據榮總 劉醫師等及高雄醫學院劉醫師等在不同地區的研究報告,台灣地區失智症患者之中約有 30%至 40%是為血管性失智症(Liu et al 1995, Liu et al 1998)。CVD 多會遺留下來不等 程度的神經功能障礙,而影響個人日後的日常生活及工作,嚴重的神經功能障礙更需家 人或看護人員的照顧,耗廢許多的醫療及社會資源,對於整個社會及國家都是一個沉重 的負擔,CVD 直接或間接的經濟支出或社會成本耗費甚大。在 1996 年的台灣地區醫院 住院病患分析,CVD 占所有住院病人的 5.1%左右。而根據台大醫院 1997 年的腦中風登 錄,當年的急性 CVD 住院成本分析,每人次的平均住院費用為 19 萬元,佔台大醫院當 年全部住院費用的 3%。根據歐美的研究結果也顯示 CVD 的成本支出逐年提高,美國的 全國 CVD 的成本支出由 1976 年的 73 億美元、1990 年的 246 億美元至 1993 年的估計 的 300 億美元(Dobkin 1995, Taylor et al 1996)。台灣地區尚無較有系統的估算究竟因
CVD 直接或間接的耗費多少國家社會資源,但以 CVD 佔台灣地區如此重要的地位,實 在非常需要去研究了解。 生活品質為多層面的概念(multidimentional concepts),主要包括個人對於生理健 康、心理狀態、社會關係、個人信念、環境等多方面的感受(Ormel et al 1997, WHOQOL Group 1998)。評估某一疾病的影響或是某一治療的效果,現今已不僅考慮死亡率(或 是存活率)、致殘率(身體功能的缺損),尚需考慮對生活品質的影響。對於醫療效性評 估的方法,在近 20 年不斷的研究,健康相關生活品質(Health related quality of life, HRQOL)之理念及測量方法已被提出及接受,作為 HRQOL 基本單位通常用調整品質
後人年(quality adjusted life year, 簡寫為 QALY)來表示(LaPuma & Lawlor 1990, Carr-Hill 1989, Barry 1992, Spiegelhalter et al 1992, Murray & Lopez 1998)。QALY 有好幾種不同的 計量方式,黃教授等於 1996 年提出把 HRQL 直接乘入存活函數中,而 HRQOL 可從目 前尚存活而存活期不同的病人作橫斷面的隨機抽樣調查取得(Hwang et al 1996)。黃等 進一步發展以外插估計 quality adjusted survival 的方法(Hwang et al 1999)。
對於 CVD 的 HRQOL 研究自 1990 年代初期開始發展而漸漸增加(Tengs et al 2001),使用於 HRQOL 的一般性測量工具(generic QOL)包括 MOS 36-item Short Form Health Survey (SF-36)(Ware and Sherbourne 1992)、EuroQol(The EuroQol Group 1990)、 Sickness Impact Profile (SIP)(Bergner et al 1981)、WHOQO(WHOQOL Group 1998)等, 其中只有 WHOQO 是跨文化且依理論基礎發展出來(Carr et al 2001),且能依各國家的 需要發展其本土題目(The WHOQOL-Taiwan Group 2000)。
使用於 CVD 的 HRQOL 的特定疾病測量工具(disease-specific QOL)包括 Frenchay Activities Index (FAI)(Holbrook and Skilbeck 1983)、the 30-iem stroke-adapted SIP
(SA-SIP30)(van Straten et al 1997)、the Niemi QOL scale(Niemi 1988)、the Ferrans and Powers QOL Index-Stroke Version(King 1996)、the Stroke Rehabilitation Outcome Study
(Granger et al 1988)與 the Stroke-specific QOL (SS-QOL)(Williams et al 1999a)。Williams 等的研究顯示 SS-QOL 與神經功能丈受損程度可預測腦中風後的整體 HRQOL,較一般 性測量工具為佳(Williams et al 1999b)。
本研究群自 1995 年起有系統地登錄所有台大醫院急性腦血管疾病住院病患,凡到 院前或住院中發生的腦中風個案均詳細登錄,腦中風登錄研究為”台大醫院中風及腦血 管硬化計劃”(The stroke and cerebral atherosclerosis study of National Taiwan University Hospital,簡稱 SCAN)之一部分(Yip et al 1997a , 1997b; Jeng et al 1994, 1995, 1996, 1998;
Chung et al 1994; Chen et al 1995),關於腦中風登錄研究部份已有數篇研究報告刊登於國 內外雜誌,對於不同型態的腦中風及腦梗塞之相關危險因子及短期 30 日的疾病死亡率 已有完整結果報告,每年約有一千位腦中風病患進入登錄,現仍持續登錄中。期盼建立 起各種不同型態腦中風的長期存活狀況,以外展推估其更長時間的存活狀況;另一方面 則建立腦中風發生之後不同時期的 HRQOL 狀況,最後將二者結合在一起,可得到 CVD 的 quality-adjusted survival 與 QALY。
研究目的:
本研究的目標主要包括兩部份: (一) 追蹤 1995-2000 年的所有腦中風患者,針對不同型態的初發腦中風,求其長期 存活曲線,比較不同型態腦中風探討的存活曲線差異並分析其影響因子。 (二) HRQOL 的測量則以台大醫院腦血管疾病特別門診的腦中風患者,分析不同腦 中風形態的 HRQOL,比較腦中風患者之整體生活品質較中風前差或是沒有改 變的 HRQOL 差別。研究方法:
台大醫院的腦中風登錄開始於 1995 年 1 月,所有住院或經急診處診治的急性腦中 風病患均包括於登錄之中,包括住院前或住院中發生的腦中風均包括在內,每年約有一 千名個案進入登錄。腦中風先區別為初發腦中風與再發腦中風,研究對象將以初發腦中 風為主。腦中風區分為腦梗塞、腦內出血、蜘蛛網膜下出血及短暫缺血發作(Jeng et al 1998)。根據 TOAST classification 方式,腦梗塞進一步區分為五種亞型:大動脈粥狀硬 化型、小洞腦梗塞、心因性血栓腦梗塞、其他特定原因型及原因未明(Adams et al 1993, Johnson et al 1995, Yip et al 1997)。腦內出血則區分為高血壓性腦內出血、其他原因的腦 內出血與原因未定的腦內出血。對於每一個案均標準化登錄腦血管疾病相關危險因子, 包括年齡、性別、高血壓史、糖尿病史、心臟疾病、心房顫動、膽固醇值、三酸甘油脂 值、尿酸值、心電圖結果、頸動脈超音波檢查結果等。 藉由台大醫院的病歷資料與台灣地區的死因登錄資料檔,分析 1995 年至 2000 年的 所有腦中風登率病患的長期存活情況,每一個案平均追蹤時間為發病至死亡時間或發病 至 2000 年 12 月 31 日。利用 Kaplan-Meier 方法求得 1 個月、6 個月、1 年、3 年、6 年 的腦中風存活率。以 log-rank test 與 Wilcoxon test 比較初發腦中風的各形態的存活狀況 有否差異存在。而 Cox proportional hazard 迴歸分析方法探討各種不同腦中風形態的存活 決定因子。HRQOL 的測量則以台大醫院腦血管疾病特別門診的腦中風患者,以問卷方式紀錄
350 至 400 名腦中風患者的基本資料、腦中風形態、危險因子、美國國家衛生院腦中風
評估量表、巴氏量表、modified Rankin scale、台灣簡明版世界衛生組織生活品質問卷、 腦中風特定疾病生活品質問卷等,分析不同腦中風形態的 HRQOL、整體 QOL 較中風前 差或不變的差別。
(1) 美國國家衛生院腦中風評估量表(National Institutes of Health Stroke Scale, NIHSS):
The NIHSS was developed to quantify neurological deficit status in stroke patients and is
based on a scale originally devised at the University of Cincinnati Stroke Center in 1989,
and revised in 1994. The modified NIHSS is a 42-point scale (15 items), with a zero being
a normal scale. The NIHSS has high inter-rater reliability among neurologists, ER
physicians, house officers, and stroke research nurses. It also has been shown and
validated in a large number of studies. The NIHSS is the most commonly used clinical
rating score for acute stroke patients (Brott et al 1989, Lyden et al 1994).
(2) 巴氏量表(Barthel Index, BI):The BI is used to measure the functional disability of persons after stroke. The BI is a widely used functional assessment tool to measure
independence in activities of daily living (ADL) on a 0-100 scale. It scores the
participant’s level of independence in 10 fundamental items of ADL: feeding, grooming,
bowels, bladder, dressing, toilet use, bathing, transfers, walking, and stairs. A higher score
corresponds to a greater independence in ADL and lesser disability. Severe disability is
defined as the BI score < 60; moderate disability, 65-90; mild disability, 95; and
independent in ADL (Mahoney & Barthel 1965, Wade & Collin 1988).
(3) Modified Rankin Scale: This is a 5-point global assessment categorization of patients’
function based on the ability to perform activities of daily life. Scale is ranked from 0=no
symptom to 5=severe disability(Rankin 1957).
(4) 台灣簡明版世界衛生組織生活品質問卷(Taiwanese-adapted WHOQOL-BREF):Both full- and short-form Taiwanese version of WHOQOL questionnaire, i.e., the
WHOQOL-100 and the WHOQOL-BREF, have been developed in Taiwan. Whereas to
used to assess QOL among the CVD patients. Excellent reliability and validity of this
adapted version were reported. The Taiwanese-adapted WHOQOL-BREF comprises 26
items translated from the original WHOQOL-BREF, plus two additional items of local
importance. The first two questions in the Taiwanese-adapted WHOQOL-BREF concern
the overall QOL. The remaining 26 items can be appropriately grouped into 4 major
domains, i.e., physical capacity, psychological well-being, social relationships, and
environment. A range of each domain scores is from 4 to 20. Furthermore, the importance
of each item and domain in relation to the WHOQOL-BREF will be asked with a 5-point
scale to obtain an individualized QOL measure. The importance will be a weighting factor
for each item and domain to obtain individualized domain or item scores for each subject
(The WHOQOL-Taiwan Group 2000; Lin et al 1999, Yao et al 2002).
(5) 腦中風特定疾病生活品質問卷(Stroke-specific quality of life, SS-QOL):The SS-QOL contains 12 domains (energy, family roles, language, mobility, mood, personality, self-care,
social roles, thinking, upper extremity function, vision, and work/productivity) and a total
of 49 items. The SS-QOL had excellent internal reliability, good validity and
結果:
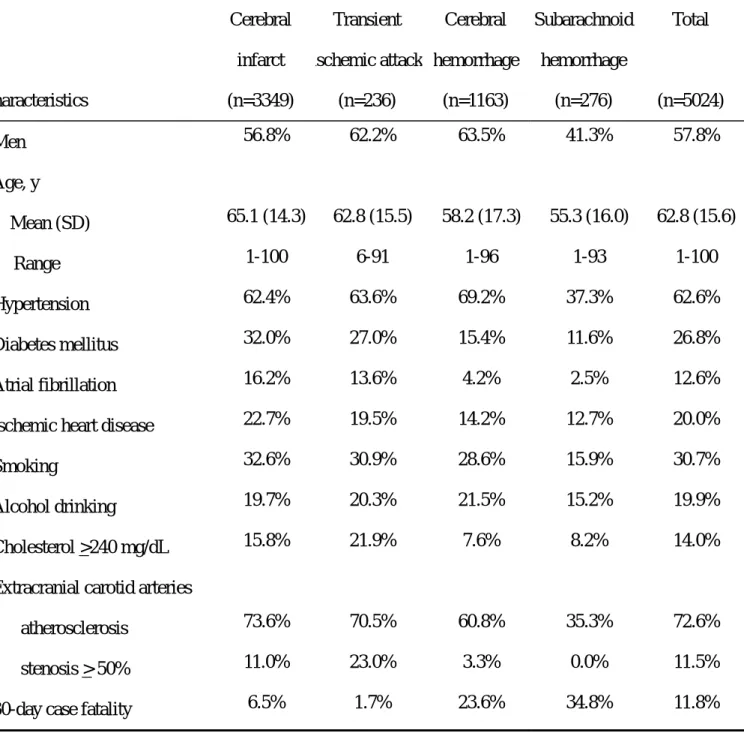
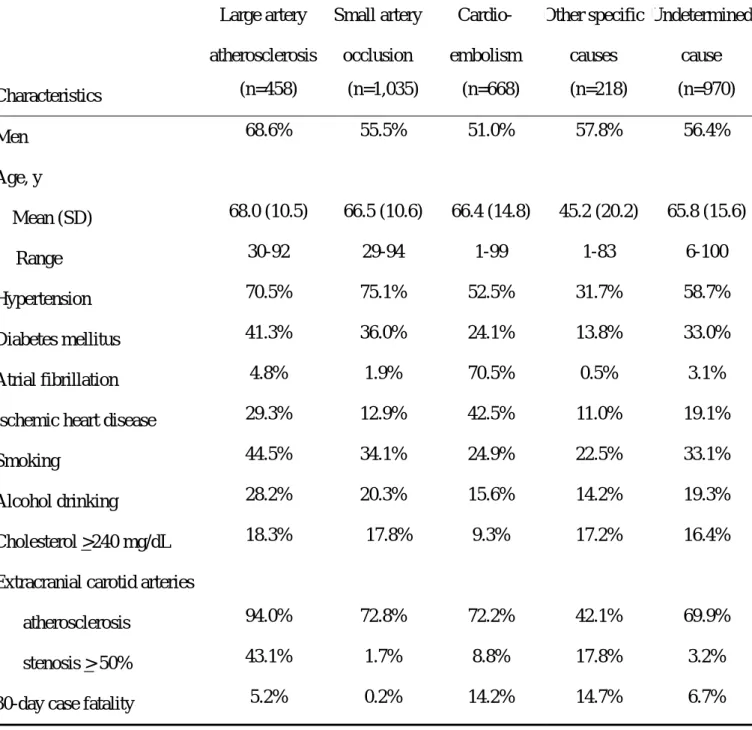
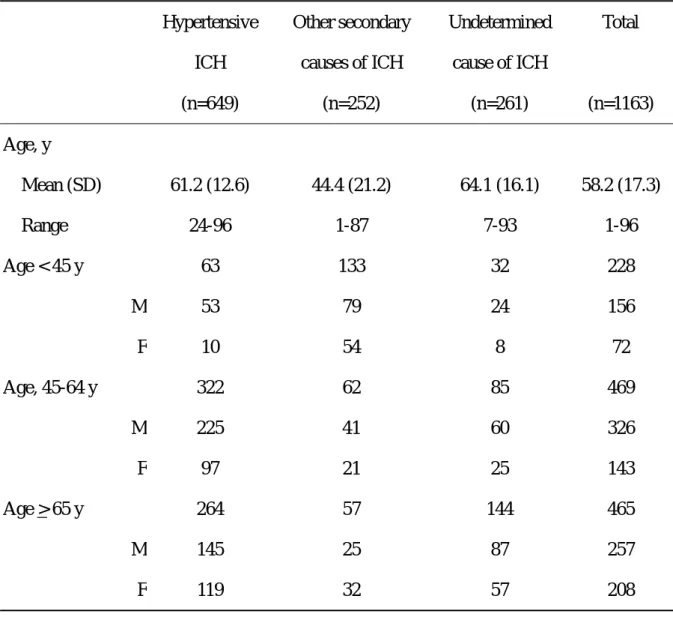
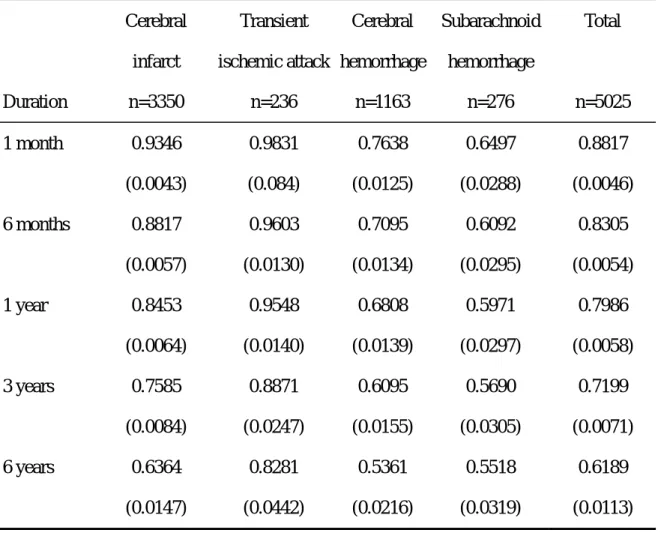
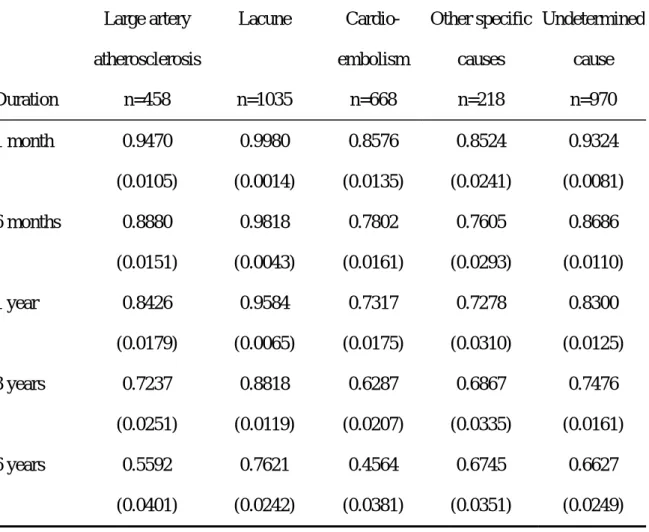
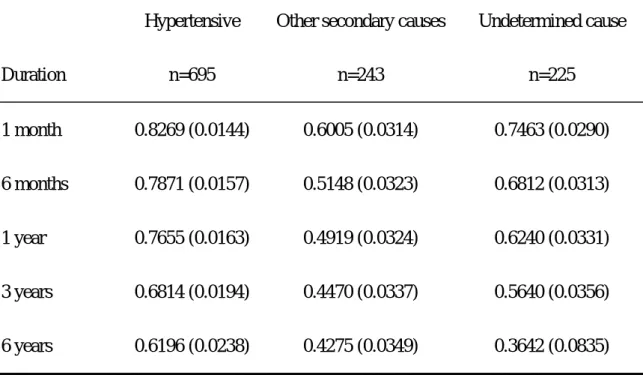
(一)腦中風的存活研究 台大醫院自 1995 年 1 月 1 日至 2000 年 12 月 31 日因急性腦中風所登錄的個案有 6178 位(男性 3619 位,女性 2559 位,平均年齡為 63.8+15.0 歲,年齡分佈為 1-100 歲)。其 中再發腦中風有 1153 位,而初發腦中風有 5024 位(佔 81.3%,男性 2902 位,女性 2122 位,平均年齡為 62.8+15.6 歲,年齡分佈為 1-100 歲),每一個案平均追蹤時間(發病至 死亡時間或發病至 2000 年 12 月 31 日)為 2.18+1.82 年。 表 1 為 5024 位不同型態的初發腦中風患者的基本資料,包括了 3349(66.7%)位 的腦梗塞、1163(23.1%)位的腦內出血、276(5.5%)位的蜘蛛網膜下腔出血及 236(4.7%) 位短暫缺血發作。所有初發腦中風患者的 30 日的短期疾病致死率為 11.8%,腦梗塞為 6.5%、腦內出血為 23.6%、蜘蛛網膜下出血為 34.8%與短暫缺血發作為 1.7%。 表 2 為 3349 位不同型態的初發腦梗塞中風患者的基本資料,包括了 458(13.7%) 位大動脈粥狀硬化型、1035(30.9%)位小動脈腦梗塞、668(19.9%)位心因性血栓腦 梗塞、218(6.5%)位其他特定原因腦梗塞及 970(29.0%)位原因未明的腦梗塞。所有 初發腦中風患者的 30 日的短期疾病致死率以心因性血栓腦梗塞(14.2%)與其他特定原 因腦梗塞(14.7%)最高,而小動脈腦梗塞(0.2%)最低。 表 3 為 1163 位不同型態的初發腦內出血中風患者的資料,包括了 649(55.8%)位 高血壓性腦內出血、252(21.7%)位其他原因的腦內出血與 261(22.4%)位原因未定 的腦內出血。 個案追蹤登錄為死亡的比率為腦梗塞(23.3%)、腦內出血(38.1%)、蜘蛛網膜下腔 出血(42.8%)及短暫缺血發作(9.8%)。表 4 為初發腦中風各形態的存活狀況,以 Kaplan-Meier 方法得到所有初發腦中風病患 1 個月、6 個月、1 年、3 年、6 年的存活比 率為 88.2%、83.1%、79.9%、72.0%與 61.9%。腦內出血與蜘蛛網膜下腔出血的存活比率較低,1 個月的存活率為 76.5%與 65%,6 年的存活率為 53.6%與 55.2%。腦梗塞的 1 個月的存活率雖有 93.5%,但 6 年存活率降至 63.6%,短暫缺血發作的 6 年存活率為 82.8%。比較初發腦中風的各形態的存活狀況,有顯著差異存在(log-rank test 的 x2值為 200.5,p 值為 0.0001;Wilcoxon test 的 x2值為 305.8,p 值為 0.0001;顯示中風發生早期 的差異性更顯著)。 表 5 為初發腦梗塞中風各亞型的存活狀況,心因性血栓腦梗塞的存活比率最低,1 個月的存活率為 85.8%、1 年為 73.2%,6 年為 45.6%。大動脈粥狀硬化型腦梗塞的 6 年 存活率也不高,為 63.6%。小動脈型腦梗塞的存活率最好,1 個月的存活率為 98.3%,6 年為 82.8%。比較初發腦梗塞中風各亞型的存活狀況,有顯著差異存在(log-rank test 的 x2值為 172.9,p 值為 0.0001;Wilcoxon test 的 x2值為 212.4,p 值為 0.0001;顯示中 風發生早期的差異性更顯著)。 表 6 為初發腦出血中風各亞型的存活狀況,高血壓性腦出血、其他原因腦出血與原 因未明腦出血的 1 個月的存活率為 82.7%、60.1%與 74.6%,有顯著差異,而 6 年的存活 率分別為 62%、42.8%與 36.4%,log-rank test 的 x2值為 52.2,p 值為 0.0001;Wilcoxon test 的 x2值為 52.9,p 值為 0.0001;顯示中風發生早期的差異性不特別較晚期顯著。
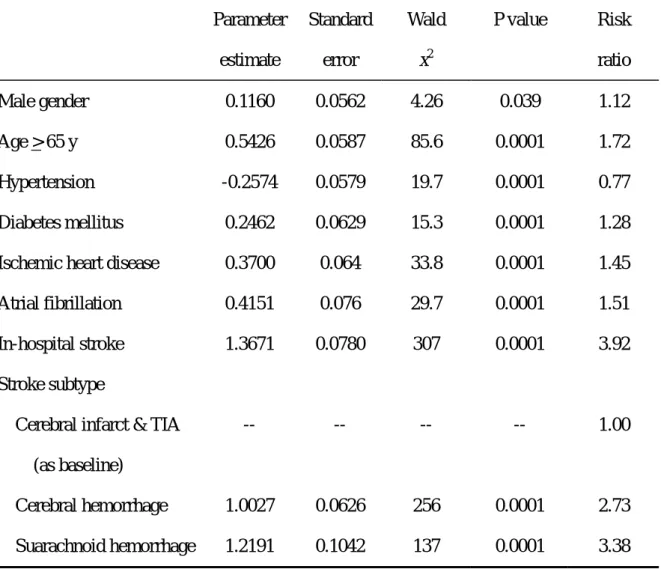
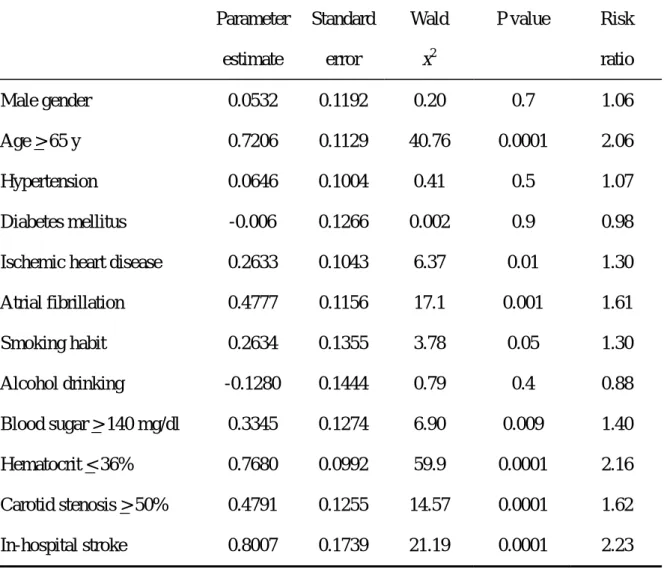
表 7 與表 8 分別為所有初發腦中風與初發腦梗塞中風的 Cox proportional hazard model。對於所有初發腦中風病患,決定存活的顯著獨立因子,包括性別(男性)、年齡 (>65 歲)、血壓(無高血壓)、糖尿病、缺血性心臟病、心房顫動、腦中風發生於住院 時、腦內出血與蜘蛛網膜下腔出血。對於初發腦梗塞中風病患,決定存活的顯著獨立因 子,包括年齡(>65 歲)、心房顫動、血糖值>140mg/dl、血容積比<36%、腦中風發生於 住院時、嚴重頸動脈狹窄(>50%)。 (二)腦中風的生活品質研究
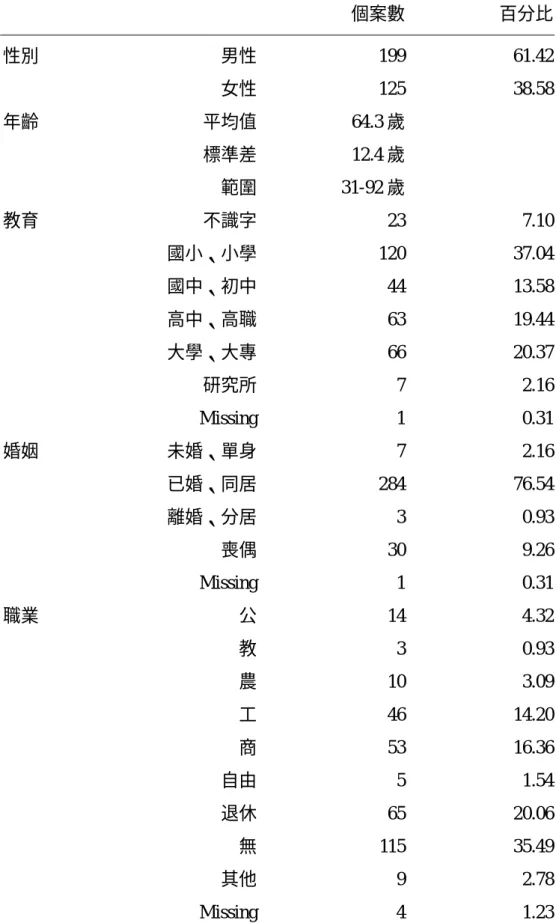
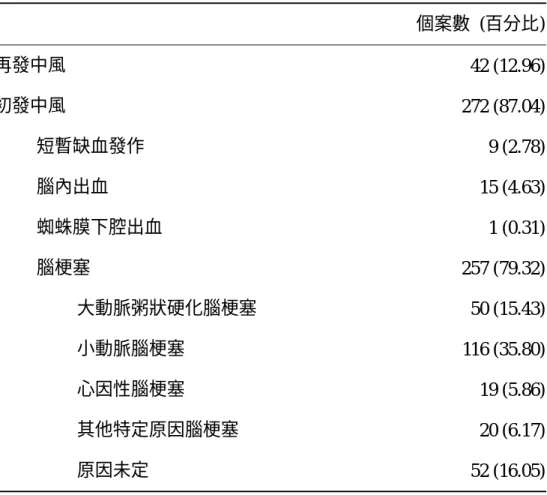
台大醫院腦中風的 HRQOL 研究共有 324 位腦中風患者接受訪查,表 9 為這些腦中 風病患的基本人口學資料。這 324 位腦中風患者有 42(12.96%)位為再發腦中風;而 272(87.04%)位為初發腦中風,包括 257(79.32%)位初發腦梗塞中風與 25 位其它型 態的腦中風患者。初發腦梗塞中風患者包括 50 位大動脈粥狀硬化型、116 位小動脈阻塞 腦梗塞、19 位心因性血栓腦梗塞、20 位其他特定原因腦梗塞及 52 位原因未明的腦梗塞 (表 9)。 表 11 為 257 位初發腦梗塞中風病患的 WHOQOL-BREF 問卷各題目之描述性統計資 料,包括了各分項的回答人數、平均數、標準差、最大與最小值、中數、偏態與峰度等, 平均數愈大表示生活品質愈好。問題的回答度除了第 21 題關於性生活只有 160(62.2%) 位回答,其餘題目均有回答,主要是受訪者大多為高齡的腦中風患者,多數已無性生活, 因此回答率較低。因受訪者大多為高齡、肢體動作較不靈活的腦中風患者,因此問卷的 記錄均幾乎是由固定的一位研究助理負責詢問與填寫。
腦梗塞中風病患的 WHOQOL-BREF 問卷之內部一致性(internal consistency)是以 Cronbach’s α表示,表 12 列出在生理範疇、心理範疇、社會範疇(與加入本土題的社 會範疇)、環境範疇(與加入本土題的環境範疇)的 Cronbach’s α值,介於 0.554 至 0.763, 以生理範疇為最高,整體 WHOQOL-BREF 問卷之內部一致性達到 0.895。 在內容效度方面,以 Pearson correlation 表示之,表 13 列出初發腦梗塞中風病患的 WHOQOL-BREF 問卷各題目與 G1、G4、所屬範疇之相關性,各題目所屬範疇之相關性 相關系數多介於 0.47 至 0.82(p<0.01),但醫療依賴(相關系數=0.24)、飲食(相關系 數=0.23)題目的相關較低。表 14 列出初發腦梗塞中風病患的 WHOQOL-BREF 問卷之 G1、G4、各範疇間之相關。 表 15 列出腦梗塞中風病患的 SS-QOL 問卷各範疇與全部之內部一致性(internal consistency),各範疇內的 Cronbach’s α值介於 0.745 至 0.940,而所有題目之內部一致
性高達 Cronbach’s α值為 0.952,顯示 SS-QOL 對於腦梗塞中風有很好的一致性。 表 16 列出不同型態初發腦梗塞中風病患的基本資料,包括年齡、性別、各腦中風 相關危險因子等。表 17 則列出不同型態的初發腦梗塞中風病患的問卷調查距離腦中風 發生時間、NIHSS、BI 與 mRS 分佈。心因性血栓腦梗塞的 NIHSS 與 mRS 分數較其它 型態腦梗塞中風為高,而 BI 則較低,表示心因性血栓腦梗塞的神經功能受損較其它型 態腦梗塞中風為嚴重。小動脈阻塞腦梗塞的 NIHSS 與 mRS 分數則較高,表示神經功能 受損較輕。表 18 為不同型態的初發腦梗塞中風病患的 WHOQOL-BREF 與 SS-QOL 生活 品質結果,各型態的生活品質範疇與總合分數並無顯著差異。表 19 進一步分析小動脈 阻塞腦梗塞(116 位)與非小動脈阻塞腦梗塞(141 位)的 WHOQOL-BREF 與 SS-QOL 的各範疇與總合的生活品質分數,均未顯示有顯著差異。 針對腦中風患者自行感受整體生活品質是否較中風前差(126 位)或是不變(131 位),表 20 列出二者的差異,相對於感受中風後整體生活品質不變的患者,感受整體生 活品質較中風前差的患者的高中(含)以上教育程度較少、NIHSS 與 mRS 分數較高、 BI 則較低(p 值均<0.05),中風類型無明顯相異(p 值=0.89),在 WHOQOL-BREF 與 SS-QOL 的各範疇與總合的生活品質分數均較低。以迴歸分析方式,SS-QOL 分數(勝
算比為 3.3,95%信賴區間為 1.7-6.4,p 值<0.001)、NIH stroke scale(勝算比為 0.7,95% 信賴區間為 0.6-1.0,p 值=0.037)、與 WHOQOL-BREF 分數(勝算比為 1.1,95%信賴區 間為 1.0-1.2,p 值=0.011),其它基本資料、中風類型、巴式量表則無顯著區別能力。若 是以加上本土題的 WHOQOL-BREF 分析,仍然是 SS-QOL 分數、NIH stroke scale、與 WHOQOL-BREF 分數有顯著的區別能力(表 21)。
討論與結論:
不同型態腦中風的存活曲線有明顯的差異,腦中風的一個月疾病致死率以蜘蛛網膜 下腔出血為最高達到 34.8%(約 1/3),其次為腦內出血為 23.6%(約 1/4),腦梗塞僅為 6.5%。中長期的腦中風致死率可以由存活曲線看出腦梗塞與腦內出血漸漸下降,而蜘蛛 網膜下腔出血只在疾病發生後短期的致死率很高,之後則變化不大。中風後 6 年的腦內 出血的存活率已低於蜘蛛網膜下腔出血(53.6%比 55.2%),腦梗塞的存活率也降至 63.6%。此結果主要與中風發病年齡、合併其它疾病的比率、與中風再發生發生有關係。 蛛網膜下腔出血大多是因為腦內的動脈瘤破裂所導致,發生的年齡以在青壯年為最 多,合併其它疾病的比率不高,若蜘蛛網膜下腔出血較嚴重易導致立即致命的危險,有 時來不及或無法救治,而一旦度過了急性期、經手術或栓塞治療,再發生致命蜘蛛網膜 下腔出血的機會就不大,此之所以蜘蛛網膜下腔出血的短期致死率高而長期則變化較 小。腦梗塞與腦內出血則較多發生中老年人口,常合併多種其它疾病,如高血壓、糖尿 病、心臟疾病等,腦梗塞與腦內出血再發生的機會也不低,這些原因導致腦梗塞與腦內 出血的存活曲線隨著時間漸漸下降。 不同型態的腦梗塞中風的存活曲線有明顯的差異,此也是與不同型態的腦梗塞的致 病機轉不同對於腦部的影響也有差異,合併其它疾病的機會也不相同。一個月的疾病致 死率以心因性血栓腦梗塞(14.2%)與其他特定原因腦梗塞(14.7%)為最高,次為大動 脈粥狀硬化型(5.2%),小動脈腦梗塞僅有 0.2%。中長期的存活情形則以心因性血栓腦 梗塞最差,到第 6 年不到 1/2 的存活率(為 45.6%),而大動脈粥狀硬化型也僅稍超過 1/2(為 55.9%),主要的原因可歸為四點:(1)二者所引起的腦梗塞範圍常較廣、神經 症狀常較嚴重,因此直接因腦中風導致死亡的比率也較高;(2)因中風引起的神經症狀 較嚴重,相對發生其它身體併發症(如吸入性肺炎、尿路感染、消化道出血)的機會也 較高;(3)再發腦中風的比例高;(4)合併其它疾病的比例高,二者常合併有冠狀動脈疾病,之後發生心肌梗塞或是突發致死的機會大。 對於所有初發腦中風或是初發腦梗塞中風的決定存活的顯著獨立因子,主要包括包 括性別(男性)、年齡(>65 歲)、糖尿病、心臟疾病(缺血性心臟病與心房顫動)、腦 中風發生於住院時與嚴重頸動脈狹窄(>50%)。長期糖尿病易發生全身大小動脈的病 變,因此之後常因糖尿病併發症而影響存活。腦中風發生於住院時多是已罹患其它較嚴 重疾病(如癌症、感染、或是手術後),因此易影響其之後的存活狀況。高血壓反而不 是中風後的存活的決定因子,主因可能為高血壓發生的腦中風以小動脈腦梗塞最常見, 而小動脈腦梗塞的短中長期的存活情形均優於其它型態的腦中風,因此對於存活的影響 反而不大。 本研究的生活品質問卷訪試對象主要為輕中度的腦中風患者,因此以腦梗塞佔較多 數,之後的分析也以初發腦梗塞中風患者為主。兩份 HRQOL 問卷—WHOQOL-BREF 與 SS-QOL 均有很好的信度與效度,而 SS-QOL 較 WHOQOL-BREF 有更好的內部一致 性。SS-QOL 的發展是依據中風存活者的各層面生活品質所定出來的,包含的題目與範 疇廣,特別是包含了中風後較常發生的語言、上肢功能、認知與視力功能,這些在一般 性的 HRQOL 問卷(如 SF-36、EuroQol、WHOQOL-BREF 等)多不包括,因此評估某 一疾病的 HRQOL 應同時包括一般性的 HRQOL 問卷與特定疾病的 HRQOL 問卷,一般 性的 HRQOL 問卷便於與其他疾病或是大眾相比較,特定疾病的 HRQOL 問卷則利於疾 病長期追蹤時 HRQOL 變化的偵測。對於腦中風患者,特定腦中風的 HRQOL 問卷,如 SS-QOL 也可提供臨床處置的基本參考,如患者的心情與活力範疇的分數低可考慮進一 步判斷是否有中風後憂鬱症,而上肢功能範疇的分數低可考慮是否需要職能治療。 針對腦中風患者自行感受整體生活品質是否較中風前差或是不變,在單變項的比較 時教育程度、NIHSS、mRS、BI、WHOQOL-BREF 與 SS-QOL 的各範疇與總合的生活 品質均有差異,但中風類型、中風至問卷調查時間則無明顯差異。多變項分析則顯示
SS-QOL、NIH stroke scale、與 WHOQOL-BREF 分數有顯著區別能力。其中又以 SS-QOL 區別能力最高。 本研究的限制包括研究的對象非固一中風之後的同一時間評估其 HRQOL,雖然之 後的結果顯示中風至問卷調查時間對於區別 HRQOL 影響不大,主要還是中風後神經功 能受損程度(如 NIHSS)影響較大,但若能長時間追蹤腦中風患者的 HRQOL,應能得 到更有信服力的結果。一般性的 HRQOL 問卷只選取 WHOQOL-BREF 使用,一般國際 上最常使用的 SF-36 若能包括在內當會增加研究的強度。而憂鬱常會影響 HRQOL 結 果,有另一個憂鬱量度的問卷當更能區別是否合併憂鬱而影響 HRQOL,雖然 SS-QOL 已包括了一些憂鬱相關的題目。 本研究的主要結論為不同型態的腦中風的存活時間有很大的差異,年齡、心臟疾病 與中風類型顯著影響腦中風的存活時間。SS-QOL、NIH stroke scale 與 WHOQOL-BREF 可明顯決定腦中風患者是否感受整體生活品質因中風有改變。
參考文獻:
Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic
stroke: definitions for use in a multicenter clinical trial. Stroke 1993;24:35-41.
Barry PP. Age-based rationing of medical care. Geriatrics. 1992; 47:64-7.
Bergner M, Bobbitt RA, Carter WB, Gilson BS. The Sickness Impact Profile: development
and final revision of a health status measure. Med Care. 1981;19:787-805.
Brott TG, Adams HP, Olinger CP, et al. Measurements of acute cerebral infarction: a
clinical examination scale. Stroke. 1989;20:864-70.
Carr AJ, Higgenson IJ. Are quality of life measures patient centered? Br Med J.
2001;322:1357-60.
Carr-Hill R. Assumption of the QALY procedure. Soc Sci Med. 1989; 29:469-77.
Chang CC, Chen CJ. Secular trend of mortality from cerebral infarct and cerebral
hemorrhage in Taiwan, 1974-1988. Stroke. 1993;24:212-8.
Chang SF, Su CL, Chen YZ, et al. Stroke incidence in Ilan Taiwan. J Formos Med Assoc.
1995;94:30-6.
Chang SF, Su CL, Hung TP. Epidemiological study of cerebrovascular disease in the
Taiwan area: current status. J Formosan Med Assoc. 1993;92:S112-20.
Chen CC, Chung MY, Jeng JS, et al. A scoring system for evaluation of the extent of
extracranial carotid atherosclerosis with B-mode imaging. Acta Neurol Sin.
1995;4:19-33.
Chung MY, Jeng JS, Yip PK, et al. Study on blood lipids, lipoproteins and apolipoproteins
in different types of ischemic stroke. Acta Neurol Sin. 1994;3:194-9.
Dobkin B. The economic impact of stroke. Neurology 1995;45(suppl 1):S6-S9.
Granger CV, Hamilton BB, Gresham GE. The Stroke Rehabilitation Outcome Study, part I: general description. Arch Phys Med Rehabil. 1988;69:506-9.
Holbrook M, Skilbeck CE. An activities index for use with stroke patients. Age Ageing.
Hsu WC, Chen ST, Chang HS, et al. The Chang Gang Stroke Registry: 1994. Acta Neurol
Sin 1995;4:171-9.
Hu HH, Chu FL, Chiang N, et al. Prevalence of stroke in Taiwan. Stroke. 1989;20:858-63.
Hu HH, Sheng WY, Chu FL, et al. Incidence of stroke in Taiwan. Stroke. 1992;23:1237-41.
Hung TP and Study Group on Stroke. Epidemiology and Clinical Profiles of Stroke in
Taiwan: Report of a Stroke Registry of 26 Teaching Hospitals in Taiwan, 1985. Taipei:
Department of Health, R.O.C., 1987 [In Chinese; English abstract]
Hung TP and Study Group on Stroke. Prospective Survey and Registry of Stroke in Taiwan
Area, Taipei: Department of Health, R.O.C., 1992 [In Chinese; English abstract]
Hung TP. Cerebrovascular disease in the Taiwan Area: past, present and future. J Formos
Med Assoc. 1993;92:S103-11.
Hunt SM, McKenna SP, McEwen J, et al. A quantitative approach to perceived health status:
a validation study. J Epidemiol Community Health. 1980;34:281-6.
Hwang JS, Tsao JY, Wang JD. Estimation of expected quality adjusted survival by
cross-sectional survey. Stat Med. 1996;15:93-102.
Hwang JS, Wang JD. Monte Carlo estimation of extrapolation of quality-adjusted survival
for follow-up studies. Stat Med. 1999;18:1627-40.
Hwang ZS, Chiang TL, Lee TK. Stroke prevalence in Taiwan: findings from the 1994
National health Interview Survey. Stroke. 1997;28:1579-1584.
Jeng JS, Chung MY, Yip PK, et al. Extracranial carotid atherosclerosis and vascular risk
factors in different types of ischemic stroke in Taiwan. Stroke. 1994;25:1989-93.
Jeng JS, Lee TK, Chang YC, et al. Misdiagnosis of acute cerebrovascular disease
(SCAN-V). Acta Neurol Taiwan. 1998;7:185-194.
Jeng JS, Lee TK, Chang YC, et al. Subtypes and mortality of stroke: a hospital-based stroke
registry in Taiwan (SCAN-IV). J Neurol Sci. 1998;156:220-6.
Jeng JS, Yip PK, Chung MY, et al. Extracranial carotid artery atherosclerosis in 1014
Jeng JS, Yip PK, Chung MY, et al. Lipoprotein (a) as a risk factor for cortical infarction and
carotid atherosclerosis. Cerebrovasc Dis. 1996;6 (suppl 2):95.
Johnson CJ, Kittner SJ, McCarter RJ, et al. Interrater reliability of an etiologic
classification of ischemic stroke. Stroke 1995;26:46-51.
King RB. Quality of life after stroke. Stroke. 1996;27:1467-72.
LaPuma J, Lawlor EF. Quality-adjusted life-years: ethical implications for physicians and
policy-makers. J Am Med Assoc. 1990;263:2917-21.
Lin MR, Yao KP, Hwang JS, Wang JD. Scale descriptor selection for Taiwan-version of
questionnaire of World Health Organization quality of life. Chin J Public Health (Taipei).
1999;18(4):262-70.
Liu CK, Lai CL, Tai CT, et al. Incidence and subtypes of dementia in southern Taiwan.
Impact of socio-demographic factors. Neurology. 1998;50:1572-9.
Liu HC, Lin KN, Lee TE, et al. Prevalence and subtypes of dementia in Taiwan: a
community of 5297 individuals. J Am Geriatr Soc. 1995;43:144-9.
Lyden P, Brott G, Tiley B, et al. NINDS TPA Stroke Study Group. Improved reliability of
the NIH stroke scale using video training. Stroke. 1994;25:2220-6.
Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Maryland State Med J.
1965; 14: 61-68.
Murray CJL, Lopez AD. Global comparative assessment in the health sector: Disease
burden, expenditures and intervention packages. Collected reprints from the Bulletin of
the World Health Organization (WHO). Geneva: WHO, 1994. also in: WHO (World
Health Organization). World Health Report 1998. Geneva: WHO,1998.
Niemi ML, Laaksonen R, Kotila M, Waltimo O. Quality of life 4 years after stroke. Stroke. 1988;19:1101-7.
Ormel J, Lindenberg S, Steverink N, Vonkorff M. Quality of life and social production
function: a framework for understanding health effects. Soc Sci Med. 1997;45:1051-63.
Rankin J. Cerebral vascular accidents in patients over the age of 60: prognosis. Scott Med J.
Ryu SJ. The Chang Gung stroke registry-1980. Chang Gung Med J. 1986;9:204-16.
Spiegelhalter DJ, Gore SM, Fitzpatrick R, Fletcher AE, Jones DR, Cox DR. Quality of life
measure in health care. III: resource allocation. Br Med J. 1992;305:1205-9.
Taylor TN, Davis PH, Torner JC, et al. Lifetime cost of stroke in the United States. Stroke.
1996;27:1469-66.
Tengs TO, Yu M, Luistro E. Health-related quality of life after stroke. A comprehensive
review. Stroke. 2001;32:964-972.
The EuroQol Group. EuroQol: a new facility for the measurement of health related quality
of life. Health Policy. 1990;16:199-208.
The WHOQOL-Taiwan Group. Introduction to the Development of the WHOQOL-Taiwan
Version. Chinese J Pub Health. 2000;19:315-24
The World Bank. World Development Report 1993: Investing in health. Oxford, U.K.:
Oxford University Press, 1993.
van Straten A, de Haan RJ, Limburg M, et al. A stroke-adapted 3—item version of the Sickness Impact Profile to assess quality of life (SA-SIP30). Stroke. 1997;28:2155-61.
Wade DT, Collin C. The Barthel ADL index: A standard measure of physical disability. Int
Disabil Studies. 1988; 10: 64-67.
Ware JE, Sherbourne CD. The MOS 36-Item Short Form Health Survey (SF-36), I:
conceptual framework and item selection. Med Care. 1992;30:473-83.
WHOQOL Group. Development of the World Health Organization WHOQOL-BREF
quality of life assessment. Psychol Med. 1998;28:551-8.
Williams LS, Weinberger M, Harris LE, Biller J. Measuring quality of life in a way that is
meaningful to stroke patients. Neurology. 1999b;53:1839-43.
Williams LS, Weinberger M, Harris LE, Clark DO, Biller J. Development of a
stroke-specific quality of life scale. Stroke. 1999a;30:1362-9.
Yao G, Chung CW, Yu CF, Wang JD. Development and verification of validity and
2002;101:342-351.
Yip PK, Jeng JS, Lee TK, et al. Subtypes of ischemic stroke: A hospital-based stroke
registry in Taiwan (SCAN-IV). Stroke. 1997a;28:2507-12.
Yip PK, Jeng JS, Ng SK, et al. The Stroke and Cerebral Atherosclerosis Study of National
Taiwan University Hospital (SCAN): background and methodology. Acta Neurol Taiwan.
1997b;6:300-8.
主持人李源德: 金山社區急性心臟血管病調查5年先驅研究—八十一年度報告 (DOH81-TD-027)。台北 : 中華民國行政院衛生署,1992。
圖表:
表 1. Clinical Characteristics of 5,025 First-ever Stroke Patients From 1995-2000 NTUH
Stroke Registry Cerebral infarct Transient ischemic attack Cerebral hemorrhage Subarachnoid hemorrhage Total Characteristics (n=3349) (n=236) (n=1163) (n=276) (n=5024) Men 56.8% 62.2% 63.5% 41.3% 57.8% Age, y Mean (SD) 65.1 (14.3) 62.8 (15.5) 58.2 (17.3) 55.3 (16.0) 62.8 (15.6) Range 1-100 6-91 1-96 1-93 1-100 Hypertension 62.4% 63.6% 69.2% 37.3% 62.6% Diabetes mellitus 32.0% 27.0% 15.4% 11.6% 26.8% Atrial fibrillation 16.2% 13.6% 4.2% 2.5% 12.6%
Ischemic heart disease 22.7% 19.5% 14.2% 12.7% 20.0%
Smoking 32.6% 30.9% 28.6% 15.9% 30.7%
Alcohol drinking 19.7% 20.3% 21.5% 15.2% 19.9%
Cholesterol >240 mg/dL 15.8% 21.9% 7.6% 8.2% 14.0%
Extracranial carotid arteries
atherosclerosis 73.6% 70.5% 60.8% 35.3% 72.6%
stenosis > 50% 11.0% 23.0% 3.3% 0.0% 11.5%
表 2. Clinical Characteristics of 3,350 First-ever Cerebral Infarct Patients From 1995-2000
NTUH Stroke Registry
Large artery Small artery Cardio- Other specific Undetermined
atherosclerosis occlusion embolism causes cause
Characteristics (n=458) (n=1,035) (n=668) (n=218) (n=970) Men 68.6% 55.5% 51.0% 57.8% 56.4% Age, y Mean (SD) 68.0 (10.5) 66.5 (10.6) 66.4 (14.8) 45.2 (20.2) 65.8 (15.6) Range 30-92 29-94 1-99 1-83 6-100 Hypertension 70.5% 75.1% 52.5% 31.7% 58.7% Diabetes mellitus 41.3% 36.0% 24.1% 13.8% 33.0% Atrial fibrillation 4.8% 1.9% 70.5% 0.5% 3.1%
Ischemic heart disease 29.3% 12.9% 42.5% 11.0% 19.1%
Smoking 44.5% 34.1% 24.9% 22.5% 33.1%
Alcohol drinking 28.2% 20.3% 15.6% 14.2% 19.3%
Cholesterol >240 mg/dL 18.3% 17.8% 9.3% 17.2% 16.4%
Extracranial carotid arteries
atherosclerosis 94.0% 72.8% 72.2% 42.1% 69.9%
stenosis > 50% 43.1% 1.7% 8.8% 17.8% 3.2%
表 3. Age and Sex Distribution of Cerebral Hemorrhage: 1995-2000 1st-ever Stroke at NTUH Hypertensive ICH Other secondary causes of ICH Undetermined cause of ICH Total (n=649) (n=252) (n=261) (n=1163) Age, y Mean (SD) 61.2 (12.6) 44.4 (21.2) 64.1 (16.1) 58.2 (17.3) Range 24-96 1-87 7-93 1-96 Age < 45 y 63 133 32 228 M 53 79 24 156 F 10 54 8 72 Age, 45-64 y 322 62 85 469 M 225 41 60 326 F 97 21 25 143 Age > 65 y 264 57 144 465 M 145 25 87 257 F 119 32 57 208
表 4. Survival analysis in different types of first-ever stroke Cerebral infarct Transient ischemic attack Cerebral hemorrhage Subarachnoid hemorrhage Total Duration n=3350 n=236 n=1163 n=276 n=5025 1 month 0.9346 (0.0043) 0.9831 (0.084) 0.7638 (0.0125) 0.6497 (0.0288) 0.8817 (0.0046) 6 months 0.8817 (0.0057) 0.9603 (0.0130) 0.7095 (0.0134) 0.6092 (0.0295) 0.8305 (0.0054) 1 year 0.8453 (0.0064) 0.9548 (0.0140) 0.6808 (0.0139) 0.5971 (0.0297) 0.7986 (0.0058) 3 years 0.7585 (0.0084) 0.8871 (0.0247) 0.6095 (0.0155) 0.5690 (0.0305) 0.7199 (0.0071) 6 years 0.6364 (0.0147) 0.8281 (0.0442) 0.5361 (0.0216) 0.5518 (0.0319) 0.6189 (0.0113)
表 5. Survival analysis in different subtypes of first-ever cerebral infarct Large artery atherosclerosis Lacune Cardio- embolism Other specific causes Undetermined cause Duration n=458 n=1035 n=668 n=218 n=970 1 month 0.9470 (0.0105) 0.9980 (0.0014) 0.8576 (0.0135) 0.8524 (0.0241) 0.9324 (0.0081) 6 months 0.8880 (0.0151) 0.9818 (0.0043) 0.7802 (0.0161) 0.7605 (0.0293) 0.8686 (0.0110) 1 year 0.8426 (0.0179) 0.9584 (0.0065) 0.7317 (0.0175) 0.7278 (0.0310) 0.8300 (0.0125) 3 years 0.7237 (0.0251) 0.8818 (0.0119) 0.6287 (0.0207) 0.6867 (0.0335) 0.7476 (0.0161) 6 years 0.5592 (0.0401) 0.7621 (0.0242) 0.4564 (0.0381) 0.6745 (0.0351) 0.6627 (0.0249)
表 6. Survival analysis in different subtypes of first-ever cerebral hemorrhage
Hypertensive Other secondary causes Undetermined cause
Duration n=695 n=243 n=225 1 month 0.8269 (0.0144) 0.6005 (0.0314) 0.7463 (0.0290) 6 months 0.7871 (0.0157) 0.5148 (0.0323) 0.6812 (0.0313) 1 year 0.7655 (0.0163) 0.4919 (0.0324) 0.6240 (0.0331) 3 years 0.6814 (0.0194) 0.4470 (0.0337) 0.5640 (0.0356) 6 years 0.6196 (0.0238) 0.4275 (0.0349) 0.3642 (0.0835)
表 7. Proportional hazard model for first-ever stroke Parameter estimate Standard error Wald x2 P value Risk ratio Male gender 0.1160 0.0562 4.26 0.039 1.12 Age > 65 y 0.5426 0.0587 85.6 0.0001 1.72 Hypertension -0.2574 0.0579 19.7 0.0001 0.77 Diabetes mellitus 0.2462 0.0629 15.3 0.0001 1.28
Ischemic heart disease 0.3700 0.064 33.8 0.0001 1.45
Atrial fibrillation 0.4151 0.076 29.7 0.0001 1.51
In-hospital stroke 1.3671 0.0780 307 0.0001 3.92
Stroke subtype
Cerebral infarct & TIA
(as baseline)
-- -- -- -- 1.00
Cerebral hemorrhage 1.0027 0.0626 256 0.0001 2.73
表 8. Proportional hazard model for first-ever cerebral infarct patients Parameter estimate Standard error Wald x2 P value Risk ratio Male gender 0.0532 0.1192 0.20 0.7 1.06 Age > 65 y 0.7206 0.1129 40.76 0.0001 2.06 Hypertension 0.0646 0.1004 0.41 0.5 1.07 Diabetes mellitus -0.006 0.1266 0.002 0.9 0.98
Ischemic heart disease 0.2633 0.1043 6.37 0.01 1.30
Atrial fibrillation 0.4777 0.1156 17.1 0.001 1.61 Smoking habit 0.2634 0.1355 3.78 0.05 1.30 Alcohol drinking -0.1280 0.1444 0.79 0.4 0.88 Blood sugar > 140 mg/dl 0.3345 0.1274 6.90 0.009 1.40 Hematocrit < 36% 0.7680 0.0992 59.9 0.0001 2.16 Carotid stenosis > 50% 0.4791 0.1255 14.57 0.0001 1.62 In-hospital stroke 0.8007 0.1739 21.19 0.0001 2.23
Survival Distribution in First-ever and Recurrent Stroke ~ 1995 to 2000 NTUH Stroke Registry
Year
First-ever stroke
Recurrent stroke
圖一、初發與再發腦中風的存活曲線圖
Survival Distribution in Subtypes of Cerebrovascular Diseases ~ 1995 to 2000 NTUH Stroke Registry
Year TIA CI CH SAH
圖二、不同類型初發腦中風的存活曲線圖
Year
Survival Distribution in Subtype of Cerebral Infarct ~ 1995-2000 NTUH Stroke Registry
Large artery atherothrombosis Lacune Cardioembolism Other determined causes Undetermined causes
圖三、不同類型初發腦梗塞中風的存活曲線圖
YearSurvival Distribution in Subtype of Cerebral Hemorrhage ~ 1995-2000 NTUH Stroke Registry
Hypertensive
Undetermined
Secondary causes
表 9:腦中風病患(324 位)生活品質研究受訪者人口學資料 個案數 百分比 性別 男性 199 61.42 女性 125 38.58 年齡 平均值 64.3 歲 標準差 12.4 歲 範圍 31-92 歲 教育 不識字 23 7.10 國小、小學 120 37.04 國中、初中 44 13.58 高中、高職 63 19.44 大學、大專 66 20.37 研究所 7 2.16 Missing 1 0.31 婚姻 未婚、單身 7 2.16 已婚、同居 284 76.54 離婚、分居 3 0.93 喪偶 30 9.26 Missing 1 0.31 職業 公 14 4.32 教 3 0.93 農 10 3.09 工 46 14.20 商 53 16.36 自由 5 1.54 退休 65 20.06 無 115 35.49 其他 9 2.78 Missing 4 1.23
表 10:腦中風病患(324 位)之中風型態分佈 個案數 (百分比) 再發中風 42 (12.96) 初發中風 272 (87.04) 短暫缺血發作 9 (2.78) 腦內出血 15 (4.63) 蜘蛛膜下腔出血 1 (0.31) 腦梗塞 257 (79.32) 大動脈粥狀硬化腦梗塞 50 (15.43) 小動脈腦梗塞 116 (35.80) 心因性腦梗塞 19 (5.86) 其他特定原因腦梗塞 20 (6.17) 原因未定 52 (16.05)
表 11、257 位初發腦梗塞中風病患的 WHOQOL-BREF 問卷各題目之描述統計資料 題號 層面 回答人數 平均數 Median 標準差 SD 最小值 Minimum 最大值 Maximum 中數 Median 偏態 Skewness 峰度 Kurtosis 1 綜合生活品質 257 3.39 0.73 1 5 4 -0.64 0.36 2 綜合健康 257 2.95 0.87 1 5 2 0.13 -1.57 3 疼痛不適 257 3.86 0.96 1 5 4 -0.78 -0.13 4 醫療依賴 257 2.16 0.63 1 5 2 3.59 12.39 5 正面感覺 257 2.81 0.94 1 5 3 -0.12 -0.85 6 個人信仰 257 3.08 0.91 1 5 3 -0.23 -0.52 7 思考學習記憶 257 3.11 0.94 1 5 4 -0.39 -0.91 8 身體安全保障 257 3.59 0.85 1 5 4 -1.59 1.55 9 物理環境 257 3.79 0.58 1 4 4 -2.91 8.21 10 活力 257 2.96 0.95 1 5 2 0.04 -1.25 11 身體意像 257 3.70 0.71 1 5 4 -1.91 3.80 12 財務資源 257 3.41 0.86 1 5 4 -0.93 -0.17 13 資訊技能 257 3.71 0.66 1 5 4 -1.75 2.52 14 娛樂休閒 257 3.04 1.04 1 5 4 -0.27 -1.37 15 活動能力 257 3.35 0.93 1 5 4 -1.06 -0.50 16 睡眠 257 3.40 0.86 1 5 4 -0.65 -0.78 17 日常活動 257 3.18 0.86 1 5 4 -0.40 -0.92 18 工作能力 257 3.04 0.86 1 5 4 -0.22 -1.12 19 自尊 257 3.33 0.88 1 5 4 -0.69 -0.88 20 個人關係 257 3.66 0.72 1 5 4 -1.50 1.36 21 性生活 160 2.82 0.95 1 4 2 0.60 -1.38 22 社會支持 257 3.52 0.79 1 5 4 -1.17 0.20 23 家居環境 257 3.85 0.47 1 5 4 -2.98 10.51 24 社會照護 257 3.87 0.47 1 5 4 -2.66 10.33 25 交通 257 3.83 0.57 1 5 4 -2.48 6.49 26 負面感覺 257 3.27 0.99 1 5 4 -0.57 -0.77 27 被尊重 257 3.70 0.67 1 5 4 -2.06 4.18 28 飲食 257 3.79 0.64 1 5 4 -0.85 1.86
表 12、257 位初發腦梗塞中風病患的 WHOQOL-BREF 問卷之內部一致性 範 疇 Cronbach’s α D1 生理 0.763 D2 心理 0.733 D3 社會 0.554 D3(TW)社會 0.615 D4 環境 0.667 D4(TW)環境 0.671 24 題 (不含 G1、G4 與本土題) 0.881 26 題 (含 G1 與 G4,但不含本土題) 0.892 28 題 (含 G1、G4 與本土題) 0.895
表 13、257 位初發腦梗塞中風病患的 WHOQOL-BREF 問卷各題目與 G1、G4、 所屬範疇之相關性 題號 層面 與 G1 與 G4 與所屬範疇1 與所屬範疇 (TW)2 1 綜合生活品質 1.00 0.40 -- --2 綜合健康 0.40 1.00 -- --3 疼痛不適 0.38 0.47 0.66 --4 醫療依賴 0.11* 0.02* 0.24 --5 正面感覺 0.45 0.37 0.75 --6 個人信仰 0.43 0.29 0.75 --7 思考學習記憶 0.36 0.32 0.71 --8 身體安全保障 0.27 0.25 0.57 0.55 9 物理環境 0.15 0.16 0.47 0.45 10 活力 0.29 0.34 0.71 --11 身體意像 0.33 0.29 0.59 --12 財務資源 0.49 0.22 0.67 0.67 13 資訊技能 0.34 0.18 0.58 0.59 14 娛樂休閒 0.28 0.21 0.63 0.61 15 活動能力 0.23 0.31 0.69 --16 睡眠 0.22 0.22 0.49 --17 日常活動 0.33 0.43 0.82 --18 工作能力 0.39 0.46 0.81 --19 自尊 0.42 0.55 0.71 --20 個人關係 0.29 0.22 0.77 0.60 21 性生活 0.09* 0.07* 0.76 0.68 22 社會支持 0.21 0.10* 0.76 0.62 23 家居環境 0.25 0.11* 0.48 0.47 24 社會照護 0.25 0.16 0.50 0.49 25 交通 0.27 0.20 0.53 0.52 26 負面感覺 0.24 0.28 0.60 --27 被尊重 0.30 0.20 0.36 0.48 28 飲食 0.32 0.19 0.23 0.41 1未含本土題之範疇 2含本土題之範疇 除 * 外所有之相關係數皆 p<0.05
表 14、257 位初發腦梗塞中風病患的 WHOQOL-BREF 問卷之 G1、G4、各範疇間之相關 G1 G4 D1 生理 D2 心理 D3 社會3(TW)社會 D4 環境 4(TW)環境 G1 1.00 G4 0.40 1.00 D1 生理 0.41 0.51 1.00 D2 心理 0.54 0.51 0.65 1.00 D3 社會 0.26 0.17 0.33 0.46 1.00 D3(TW)社會 0.25 0.16 0.41 0.45 0.65 1.00 D4 環境 0.52 0.34 0.51 0.60 0.40 0.44 1.00 D4(TW)環境 0.55 0.36 0.51 0.61 0.41 0.44 0.98 1.00 D3(TW)與 D4(TW)含本土題之範疇 所有之相關係數皆 p<0.01
表 15、257 位初發腦梗塞中風病患的 SS-QOL 問卷之內部一致性 範 疇 Cronbach’s α D1 自我照顧 0.839 D2 視力 0.829 D3 語言 0.937 D4 行動 0.940 D5 工作能力 0.908 D6 上肢功能 0.906 D7 思考 0.813 D8 個性 0.838 D9 心情 0.745 D10 家庭角色 0.778 D11 社會角色 0.907 D12 活力 0.887 總合 0.952
表 16、257 位初發腦梗塞中風病患的基本資料 腦梗塞中風亞型 大動脈粥狀 硬化狹窄 小動脈 阻塞 心因性 梗塞 其它特定 原因 原因未定 (n=50) (n=116) (n=19) (n=20) (n=52) 年齡(歲) 平均 67.7 + 10.7 65.3 + 10.8 65.5 + 11.7 49.1 + 9.6 64.5 + 13.1 範圍 46 - 86 35 - 86 38 - 87 36 - 67 36 - 89 性別 男性 33 66 13 12 34 女性 17 50 6 8 18 教育 不識字 2 11 0 1 4 小學 18 46 6 4 21 中學 17 37 6 14 15 大學、研究所 13 21 7 1 14 婚姻 未婚、單身 0 1 1 1 1 已婚、同居 43 105 17 19 44 離婚、分居 1 0 0 0 0 喪偶 6 9 1 0 7 抽煙習慣 27 42 4 9 27 飲酒習慣 6 23 2 5 6 高血壓 39 101 9 6 32 糖尿病 16 43 4 2 4 冠心症 9 5 1 0 2 心房顫動 2 3 16 0 0 高膽固醇 18 36 1 5 12 高三酸甘油脂 12 30 4 5 5 高尿酸 9 25 4 4 8 嚴重頸動脈狹窄 22 1 0 2 1 合併癌症 3 1 1 4 1 除了年齡,其它項目數字為個數(百分比)。
表 17、257 位不同型態的初發腦梗塞中風病患的問卷調查距離腦中風發生時間、NIHSS、 BI 與 mRS 分佈 腦梗塞中風亞型 大動脈粥狀 硬化狹窄 小動脈 阻塞 心因性 梗塞 其它特定 原因 原因未定 (n=50) (n=116) (n=19) (n=20) (n=52) 問 卷 調 查 距 離 腦 中 風發生時間(年) 平均 2.61 + 2.86 3.03 + 3.58 2.31 + 1.64 2.69 + 3.85 3.53 + 3.70 範圍 0.2 – 12.0 0.1 – 22.0 0.5 – 6.2 0.1 – 14.0 0.2 – 17.0 NIHSS 平均 1.48 + 1.81 0.99 + 1.55 2.89 + 3.25 1.90 + 2.05 1.06 + 1.38 範圍 0 – 7 0-12 0-11 0-7 0-6 Barthel index 平均 1.58 + 1.07 1.18 + 0.95 1.74 + 1.28 1.55 + 1.19 1.17 + 1.08 範圍 0 - 4 0 - 4 0 - 4 0 - 4 0 - 4 Modified Rankin scale 平均 93.9 + 16.9 97.3 + 10.0 86.6 + 30.3 95.8 + 12.2 96.5 + 11.2 範圍 10 - 100 20 - 100 10 - 100 50 - 100 40 – 100
表 18、257 位不同型態的初發腦梗塞中風病患的生活品質結果 腦梗塞中風亞型 大動脈粥狀 硬化狹窄 小動脈 阻塞 心因性 梗塞 其它特定 原因 原因未定 (n=50) (n=116) (n=19) (n=20) (n=52) WHOQOL-BREF G1 3.4 + 0.7 3.4 + 0.8 3.6 + 0.7 3.0 + 0.8 3.4 + 0.7 G4 3.0 + 0.8 3.0 + 0.9 3.0 + 0.9 2.5 + 0.6 3.0 + 0.9 D1 生理 12.1 + 2.4 12.7 + 2.2 12.4 + 2.3 12.3 + 2.2 12.8 + 2.0 D2 心理 12.6 + 2.7 13.0 + 2.5 13.2 + 2.4 12.0 + 2.7 13.0 + 2.2 D3 社會 13.3 + 3.0 13.8 + 2.6 13.4 + 2.4 12.3 + 2.2 13.9 + 2.1 D3(TW)社會 11.9 + 2.5 12.6 + 2.4 12.9 + 2.2 13.3 + 2.5 13.1 + 2.0 D4 環境 14.5 + 1.5 14.6 + 1.6 14.7 + 1.4 14.0 + 2.3 14.8 + 1.4 D4(TW)環境 14.6 + 1.4 14.6 + 1.5 14.6 + 1.4 13.9 + 2.0 14.9 + 1.3 SS-QOL D1 自我照顧 4.4 + 0.9 4.5 + 0.8 4.0 + 1.4 4.4 + 0.9 4.5 + 0.9 D2 視力 4.7 + 0.5 4.8 + 0.5 4.8 + 0.4 4.4 + 1.0 4.7 + 0.5 D3 語言 4.6 + 0.9 4.8 + 0.6 4.3 + 0.9 4.7 + 0.6 4.6 + 0.6 D4 行動 4.0 + 1.1 4.1 + 1.0 3.5 + 1.4 4.1 + 1.2 4.3 + 1.1 D5 工作能力 3.6 + 1.5 4.0 + 1.3 3.6 + 1.8 3.7 + 1.5 3.9 + 1.4 D6 上肢功能 4.4 + 1.1 4.5 + 0.9 3.8 + 1.6 4.5 + 0.9 4.5 + 1.1 D7 思考 3.0 + 1.5 3.2 + 1.6 2.9 + 1.4 2.7 + 1.4 3.2 + 1.4 D8 個性 3.1 + 1.6 3.2 + 1.6 3.3 + 1.6 3.0 + 1.5 3.2 + 1.6 D9 心情 3.5 + 1.4 3.6 + 1.5 3.7 + 1.6 3.3 + 1.6 3.5 + 1.5 D10 家庭角色 3.5 + 1.4 3.6 + 1.5 3.7 + 1.6 3.3 + 1.6 3.5 + 1.5 D11 社會角色 1.7 + 1.2 2.2 + 1.5 2.2 + 1.6 2.3 + 1.7 2.0 + 1.4 D12 活力 3.4 + 1.5 3.1 + 1.6 3.1 + 1.5 2.4 + 1.5 3.1 + 1.6 總合 3.7 + 0.8 3.8 + 0.8 3.6 + 1.0 3.6 + 1.0 3.7 + 0.8
表 19、257 位不同型態的初發腦梗塞中風病患的生活品質結果 小動脈阻塞 非小動脈阻塞 P 值 (n=116) (n=141) 年齡(歲) 65.3 + 10.8 63.6 + 13.1 0.25 男性 66 (56.9) 92 (65.2) 0.11 高中(含)以上教育程度 43 (37.1) 63 (44.7) 0.15 NIHSS 1.0 + 1.6 1.6 + 2.0 0.01 Barthel index 97.3 + 10.0 94.2 + 17.1 0.07
Modified Rankin scale 1.2 + 1.0 1.5 + 1.1 0.04
問卷調查距離腦中風發生 時間(年) 3.0 + 2.9 3.6 + 3.2 0.80 WHOQOL-BREF G1 3.4 + 0.8 3.4 + 0.7 0.45 G4 3.0 + 0.9 2.9 + 0.9 0.48 D1 生理 12.7 + 2.2 12.4 + 2.2 0.33 D2 心理 13.0 + 2.5 12.8 + 2.5 0.41 D3 社會 13.8 + 2.6 13.7 + 2.5 0.81 D3(TW)社會 12.6 + 2.4 12.7 + 2.3 0.83 D4 環境 14.6 + 1.6 14.5 + 1.5 0.89 D4(TW)環境 14.6 + 1.5 14.6 + 1.5 0.78 總合 54.0 + 7.3 53.4 + 6.7 0.47 總合(TW) 52.9 + 7.1 52.4 + 6.6 0.55 SS-QOL D1 自我照顧 4.5 + 0.8 4.4 + 1.0 0.21 D2 視力 4.8 + 0.5 4.7 + 0.6 0.33 D3 語言 4.8 + 0.6 4.6 + 0.8 0.042
D4 行動 4.1 + 1.0 4.0 + 1.2 0.86 D5 工作能力 4.0 + 1.3 3.7 + 1.5 0.20 D6 上肢功能 4.5 + 0.9 4.4 + 1.1 0.26 D7 思考 3.2 + 1.6 3.0 + 1.5 0.24 D8 個性 3.2 + 1.6 3.2 + 1.6 0.71 D9 心情 3.6 + 1.5 3.5 + 1.5 0.40 D10 家庭角色 3.6 + 1.5 3.5 + 1.5 0.39 D11 社會角色 2.2 + 1.5 2.0 + 1.4 0.22 D12 活力 3.1 + 1.6 3.1 + 1.6 0.93 總合 3.8 + 0.8 3.7 + 0.9 0.19
表 20、257 位不同型態的初發腦梗塞中風病患的生活品質結果 整體的生活品質 較中風前差 整體的生活品質與 中風前差不多 P 值 (n=126) (n=131) 年齡(歲) 64.4 + 12.9 64.3 + 11.3 0.92 男性 75 (59.5) 83 (63.4) 0.61 高中(含)以上教育程度 44 (34.9) 62 (47.3) 0.038 NIHSS 2.0 + 2.3 0.6 + 0.9 <0.001 Barthel index 91.8 + 19.6 99.2 + 3.8 <0.001
Modified Rankin scale 1.8 + 1.1 0.9 + 0.8 <0.001
問卷調查距離腦中風發生 時間(年) 2.7 + 3.4 3.2 + 3.42 0.18 腦梗塞中風類型 大動脈粥狀硬化狹窄 27 (21.4) 23 (17.6) 0.89 小動脈阻塞 53 (42.1) 63 (48.1) -- 心因性梗塞 10 (7.9) 9 (6.9) -- 其它特定原因 10 (7.9) 10 (7.6) -- 原因未定 26 (20.6) 26 (19.8) -- WHOQOL-BREF G1 3.1 + 0.8 3.6 + 0.6 <0.001 G4 2.6 + 0.7 3.3 + 0.9 <0.001 D1 生理 11.4 + 2.1 13.7 + 1.6 <0.001 D2 心理 11.7 + 2.6 13.9 + 1.7 <0.001 D3 社會 12.9 + 2.8 14.5 + 2.0 <0.001 D3(TW)社會 11.9 + 2.4 13.3 + 2.1 <0.001 D4 環境 14.0 + 1.7 15.0 + 1.3 <0.001
D4(TW)環境 14.1 + 1.6 15.1 + 1.2 <0.001 總合 50.1 + 7.4 57.1 + 4.3 <0.001 總合(TW) 49.2 + 7.1 56.0 + 4.5 <0.001 自我生活品質分數* 64.2 + 14.5 72.9 + 11.7 <0.001 SS-QOL D1 自我照顧 4.1 + 1.1 4.8 + 0.5 <0.001 D2 視力 4.6 + 0.7 4.9 + 0.3 <0.001 D3 語言 4.5 + 0.9 4.9 + 0.4 <0.001 D4 行動 3.5 + 1.2 4.5 + 0.7 <0.001 D5 工作能力 3.1 + 1.5 4.6 + 0.8 <0.001 D6 上肢功能 4.0 + 1.3 4.8 + 0.5 <0.001 D7 思考 2.6 + 1.5 3.6 + 1.4 <0.001 D8 個性 2.7 + 1.6 3.6 + 1.5 <0.001 D9 心情 2.9 + 1.4 4.2 + 1.3 <0.001 D10 家庭角色 2.9 + 1.4 4.2 + 1.3 <0.001 D11 社會角色 1.5 + 1.1 2.6 + 1.6 <0.001 D12 活力 2.7 + 1.6 3.5 + 1.5 <0.001 總合 3.3 + 0.8 4.2 + 0.6 <0.001 *自我生活品質分數量分為 0 至 100 分
表 21、Independent predictors of overall HRQOL the same as prestroke OR 95% CI P value Regression 1 SS-QOL score* 3.31 1.72, 6.37 <0.001 NIHSS score† 0.74 0.55, 0.98 0.037 WHOQOL-BREF score* 1.10 1.02, 1.19 0.011 Regression 2 SS-QOL score* 3.54 1.80, 6.98 <0.001 NIHSS score† 0.72 0.53, 0.96 0.027 WHOQOL-BREF Taiwan version score* 1.08 1.00, 1.17 0.043
*Higher SS-QOL and WHOQOL scores indicate better health-related quality of life.
†Lower NIHSS score indicates less impairment.
OR = odds ratio; SS-QOL = stroke-specific quality of life; NIHSS = NIH stroke scale;
<附件一>
美國國家衛生研究院中風評量表(NIHSS) 評估日期: 西元__ 年 月 日 項 目 評 分 指 標 分數 警覺 0 嗜睡 1 木僵 2 1a.意識程度 昏迷 3 正確回答二項指令 0 正確回答一項指令 1 1b.意識程度,回答問題 (問年齡及出生月份) 二者皆回答不正確 2 正確服從二項指令 0 正確服從一項指令 1 1c.意識程度,遵從命令 (閉眼、握拳) 二者皆不正確 2 正常 0 部分凝視麻痺 1 2.凝視 強迫性偏移或完全癱瘓 2 視野正常 0 部分同側偏盲 1 完全同側偏盲 2 3.視野 兩側偏盲(全盲) 3 動作正常 0 輕微癱瘓 1 局部癱瘓 2 4.顏面麻痺 完全癱瘓 3 無傾斜 0 有傾斜 1 稍可對抗重力 2 右 上 肢 右 下 肢 左 上 肢 左 下 肢 不能對抗重力 3 不能移動 4 5-8.肢體運動功能 (重複每隻手臂及腿) 無法測試 X 沒有出現 0 一肢失調 1 9.肢體運動失調 (只有出現時才計分) 二肢失調 2 正常 0 局部喪失 1 10.感覺(用針刺) 嚴重喪失 2 無失語症 0 輕-中度失語 1 嚴重失語 2 11.語言 完全失語 3 正常發音 0 輕-中度構音困難 1 無法理解的或更差 2 12.構音障礙 未經試驗的 X 無疏忽 0 部分疏忽 1 13.疏忽/不注意 完全疏忽 2 總 分<附件二>
Modified Rankin Scale
□ 第 0 級 No symptoms at all
□ 第 1 級
No significant disability despite symptoms
Able to carry out all usual duties and activities
□ 第 2 級
Slight disability
Unable to carry out all previous activities, but able to look after own affairs without assistance
□ 第 3 級
Moderate disability
Requiring some help, but able to walk without assistance
□ 第 4 級
Moderately severe disability
Unable to walk without assistance, and unable to attend to own bodily needs
□ 第 5 級
Severe disability
Bedridden, incontinence, and requiring constant nursing care and attention