Date 2013/January/6
Type of manuscript: Original article
Manuscript title: Irritable bowel syndrome correlates with increased risk
of Parkinson’s disease in Taiwan
Running head: Irritable bowel syndrome and Parkinson’s disease Authors’ full names:
Shih-Wei Lai, MD1,2; Kuan-Fu Liao, MD and MS 3,4,5; Cheng-Li Lin, MS6,7;
Fung-Chang Sung, PhD, MPH6,7
1School of Medicine, 3Graduate Institute of Integrated Medicine and
6Department of Public Health, China Medical University, Taichung, Taiwan
2Department of Family Medicine, and 7Management Office for Health Data,
China Medical University Hospital, Taichung, Taiwan
4Department of Internal Medicine, Taichung Tzu Chi General Hospital,
Taichung, Taiwan
5Department of Health Care Administration, Central Taiwan University of
Science and Technology, Taichung, Taiwan
The first two authors equally contributed to this study.
Corresponding author:
Fung-Chang Sung, PhD, MPH
Professor, China Medical University, Department of Public Health, No. 91, Hsueh-Shih Road, Taichung City, 404, Taiwan
Phone: 886-4-2206-2295 Fax: 886-4-2201-9901
E-mail: [email protected]
Abstract
Objectives. This study investigated whether an association exists between irritable bowel syndrome (IBS) and the risk of Parkinson’s disease. Methods. This research is a cohort study using the dataset from the Taiwan National Health Insurance program. We identified 17623 patients (aged 40 years or above) with newly diagnosed IBS as the study group and 70492 subjects without IBS as the comparison group from 2000 to 2008. The risk of Parkinson’s disease associated with IBS was estimated. Results. The incidence of Parkinson’s disease in the IBS group was 1.66-fold higher in men (4.53 vs. 2.74 per 1000 person-years) and 1.87-fold higher in women (3.98 vs. 2.13 per 1000 person-years) than that in the comparison group. The multivariate Cox proportional hazard regression analysis revealed that the hazard ratios of Parkinson’s disease associated with IBS were 1.44 (95% CI= 1.24, 1.68) in men and 1.55 (95% CI= 1.33, 1.80) in women compared with the non-IBS group. The sub-analysis demonstrated that constipation subtype or diarrhea subtype was also associated with increased risk of Parkinson’s disease in both genders. Conclusion. IBS is correlated with increased risk of Parkinson's disease in both genders in Taiwan.
Keywords: constipation; diarrhea; irritable bowel syndrome; non-motor; Parkinson’s disease
Introduction
Irritable bowel syndrome (IBS) is a frustrating and common disorder. A systematic review by Lovell et al. has demonstrated that the prevalence of IBS varies from approximately 1.1% to 45.0% worldwide according to the different criteria of defining IBS.1 According to the Rome III criteria,2 the cardinal symptoms include
recurrent abdominal pain or discomfort associated with the onset of either diarrhea predominant, constipation predominant, or mixed types. Although the real
pathophysiology of irritable bowel syndrome remains unclear, the novel pathogenesis mediated by the dysregulation of the brain–gut axis has been proposed.3–5 Various
psychosocial, environmental, or/and genetic factors can influence the brain, which releases numerous neurotransmitters to alter the gastro-intestinal tract motility.3–5
Aside from traditional motor disorders, including resting tremor, cogwheel rigidity, and bradykinesia, non-motor symptoms of Parkinson’s disease have drawn little attention because they are frequently unrecognized and/or under-diagnosed. Among the non-motor symptoms, gastrointestinal symptoms including constipation, and sensory symptoms including abdominal pain are the most common. The prevalence of constipation is about 46.7% to 52.5%, and the prevalence of pain is about 28%. Although the real pathophysiology of non-motor symptoms are not well recognized in clinical practice, the novel pathogenesis involved in neurodegeneration of the brain– gut axis has been proposed. Different potential mechanisms converge in the
degenerative process of the central nervous system and enteric nervous system mediated by the Lewy bodies, Lewy neurites, and other neurological alterations.10–12
Based on the above review, we hypothesize that a relationship exists between IBS and Parkinson’s disease because the brain–gut axis is potentially involved in these two conditions. If a relation exists, more interventions can be performed in these two
conditions. Therefore, we conducted a cohort study to investigate whether an association exists between IBS and Parkinson’s disease in Taiwan.
Materials and Methods Data sources
We designed a cohort study using the dataset from the Taiwan National Health Insurance. Previous studies have documented the details of the insurance program.13–15
Criteria and definition
This cohort study included two groups. The case group consisted of 17623 patients with newly diagnosed IBS (aged 40 years and older) in 2000 to 2008 (based on the International Classification of Diseases (ICD) 9th Revision, ICD-9 codes 564.1) and the control group consisted of 70492 people without diagnosis of IBS (case: control = 1:4). The case and control groups were matched by gender, age (within 5 years), and index date. The index date was defined as the date of the diagnosis of Parkinson’s disease. The case and control groups were followed up until a subject received a diagnosis of Parkinson’s disease or until December 31, 2010 to determine the incidence of Parkinson’s disease.
Subjects who had a diagnosis of Parkinson’s disease, major psychiatric diseases, (ICD-9 codes 291-293, 294.0, 294.8, 294.9, 295, 296.0, 296.1, 296.4–296.9, 297, and 298), mental retardation (ICD-9 codes 317–319), cancer (ICD-9 codes 140.XX-208.X X), colorectal adenomas (ICD-9 codes 211.3 and 211.4) or inflammatory bowel diseases (ICD-9 codes 555.X and 556.X) before the index date were excluded from the study.
Statistical analysis
Chi-square test and t-test were used to compare the differences between the case group and the control group regarding the baseline co-morbidities in both genders separately. The incidence of Parkinson’s disease was calculated as the number of Parkinson’s disease cases identified during the follow-up divided by the total person-years for each group. Cox proportional hazard models were used to estimate the
hazard ratio (HR) and 95% confidence intervals to evaluate the risk of Parkinson’s disease associated with IBS. All analyses were performed using the SAS software version 9.1 (SAS Institute Inc., Cary, NC), and the statistical significance level was set at two-sided p < 0.05.
Results
Baseline characteristics of the study population
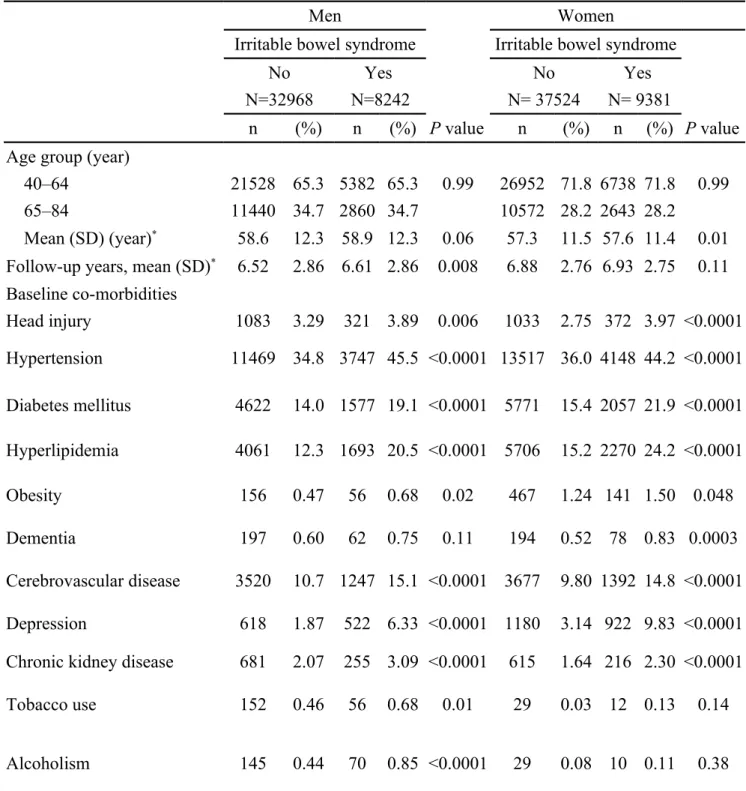
Table 1 demonstrates the baseline co-morbidities between the IBS group and the control group by gender. The IBS group had higher proportions of head injury, hypertension, diabetes mellitus, hyperlipidemia, obesity, cerebrovascular disease, depression, and chronic kidney disease in both genders, with statistical significance. The male cases had higher proportions of tobacco use and alcoholism. The female cases had higher proportion of dementia.
Incidence of Parkinson’s disease in both genders
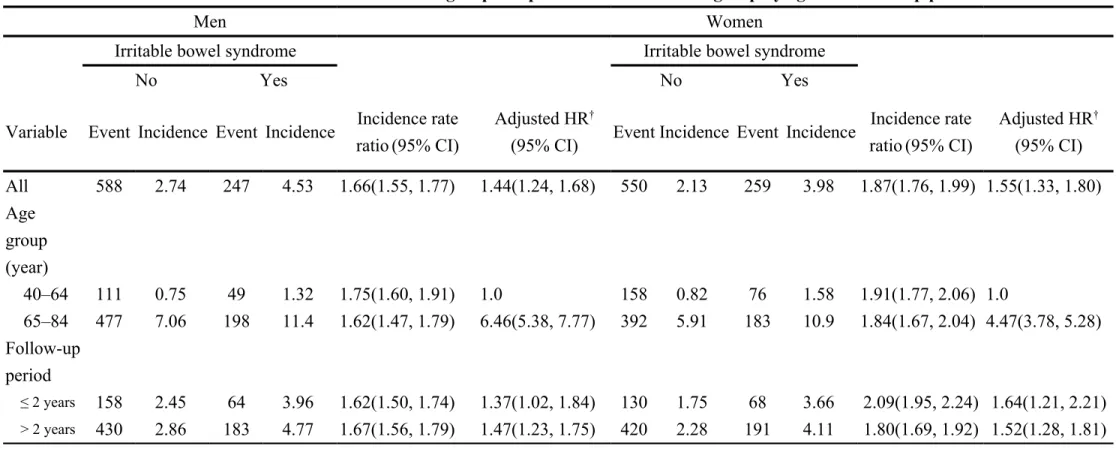
Table 2 shows the gender-specific risk of Parkinson’s disease by duration of follow-up for the IBS and non-IBS grofollow-ups. The incidence of Parkinson’s disease in the IBS group was 1.66-fold higher in men (4.53 vs. 2.74 per 1000 person-years) and 1.87-fold higher in women (3.98 vs. 2.13 per 1000 person-years) than that in the non-IBS group. The multivariate Cox regression analysis revealed that the HRs for Parkinson’s disease associated with IBS were 6.46 (95% CI = 5.38, 7.77) in men aged 65 to 84 and 4.47 (95% CI =3.78, 5.28) in women aged 65 to 84 compared with those aged 40 to 64. The risk of Parkinson’s disease slightly increased after 2 years of follow-up in men and slightly declined after 2 years of follow-up in women.
Association between Parkinson’s disease, IBS, and other co-morbidities
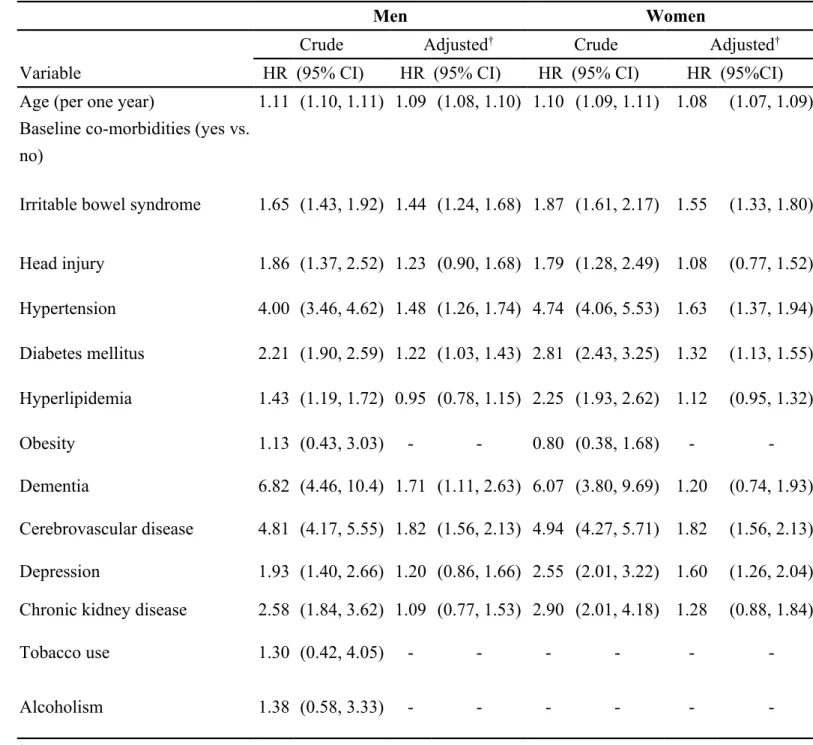
The multivariate Cox proportional hazard regression analysis revealed that the HRs of Parkinson’s disease associated with IBS were 1.44 (95% CI= 1.24, 1.68) in men and 1.55 (95% CI= 1.33, 1.80) in women compared with the non-IBS group (Table 3). Age, hypertension, diabetes mellitus, and cerebrovascular disease were also
significantly associated with Parkinson’s disease in both genders (Table 3). Sub-analysis of the association between Parkinson's disease and IBS subtypes As a reference of the non-IBS group, the sub-analysis revealed that the HRs of
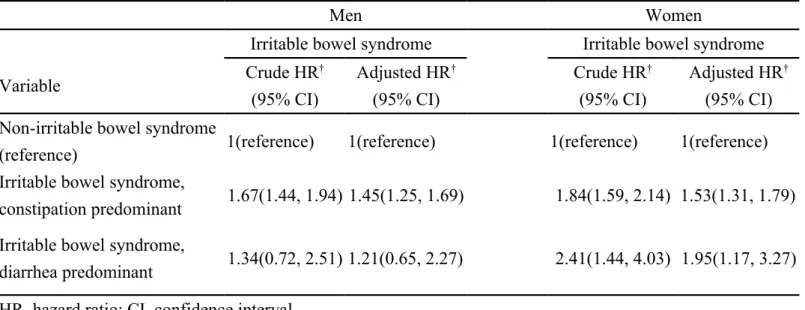
Parkinson’s disease were 1.45 in male patients with constipation predominant (95% CI= 1.25, 1.69), 1.21 in male patients with diarrhea predominant (95% CI= 0.65, 2.27), 1.53 in female patients with constipation predominant (95% CI= 1.31, 1.79), and 1.95 in female patients with diarrhea predominant (95% CI= 1.17, 3.27) (Table 4).
Discussion
This research is a pilot study, with no relevant studies to compare it with. The overall risk of Parkinson’s disease increased to 1.4-fold in men and 1.6-fold in women with IBS. Although constipation can be a non-motor symptom of Parkinson’s disease, in our further analysis, constipation predominant or diarrhea predominant can be associated with increased risk in both genders, except for male diarrhea predominant that did not reach statistical significance. A close association, albeit not causal, exists between IBS and Parkinson’s disease. Although this study demonstrates that the subjects diagnosed with IBS preceded the clinical diagnosis of Parkinson’s disease, due to an observational study, we cannot differentiate whether IBS actually belongs to the non-motor symptoms of Parkinson’s disease or only the side effects of the drugs for the treatment of the symptoms associated with the preclinical undiagnosed stage of Parkinson’s disease or is a unique event that coincidences with Parkinson’s disease. However, previous studies have shown that colonoscopy biopsies can demonstrate the Lewy pathology in the submucosal plexus of the colon in patients with Parkinson’s disease. This finding partially explains the pathophysiology of gastrointestinal symptoms even prior to the development of motor symptoms of Parkinson’s disease and provides valuable evidence that Lewy pathology of the colon can be used as a reliable early biomarker of Parkinson’s disease.18 We also found that the risk of
Parkinson’s disease associated with IBS is higher in older patients. Based on the Rome III criteria,2 only after the exclusion of inflammatory, metabolic, anatomic or
neoplastic cause can IBS be diagnosed by clinical features. Furthermore, routine colonoscopy biopsies should be recommended for patients with clinically suspected IBS to determine whether Lewy pathology or other lesions can be detected, especially in those aged 65 or older. Therefore, these patients cannot be misdiagnosed.
Some limitations exist in this dataset. First, we cannot obtain the colonoscopy findings in patients with suspected IBS if they have not undergone colonoscopy. Second, other non-motor symptoms that preceded IBS cannot be found in this dataset. We conclude that IBS correlates with increased risk of Parkinson’s disease in Taiwan, but further studies are needed to clarify this issue.
Funding
This study was supported in part by grants from the Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH 101-TD-B-111-004), the Cancer Research Center of Excellence (DOH 101-TD-C-111-005), and the National Science Council (NSC 100-2621-M-039-001). The funding agencies did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgements
The authors thank the National Health Research Institute in Taiwan for providing the insurance claims data.
Specific author contributions:
Shih-Wei Lai: (1) substantially contributed to the conception of this article; (2) planned and conducted the study; (3) initiated the draft of the article and critically revised the article.
Kuan-Fu Liao: (1) participated in data interpretation; (2) critically revised the article. Cheng-Li Lin: (1) conducted data analysis; (2) critically revised the article.
Fung-Chang Sung: (1) substantially contributed to the concept and design, as well as data acquisition; (2) critically revised the article.
Conflict of Interest Statement
References
1. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol 2012;10:712-21 e4.
2. Appendix A Rome III Diagnostic Criteria for Functional
Gastrointestinal Disorders. [cited in 2013 January, http://www.romecriteria.org. 3. Mach T. The brain-gut axis in irritable bowel syndrome--clinical aspects. Med Sci Monit 2004;10:RA125-31.
4. Ohman L, Simren M. New insights into the pathogenesis and pathophysiology of irritable bowel syndrome. Dig Liver Dis 2007;39:201-15.
5. Katiraei P, Bultron G. Need for a comprehensive medical approach to the neuro-immuno-gastroenterology of irritable bowel syndrome. World J Gastroenterol
2011;17:2791-800.
6. Chaudhuri KR, Healy DG, Schapira AH. Non-motor symptoms of Parkinson's disease: diagnosis and management. Lancet Neurol 2006;5:235-45.
7. Poewe W. Non-motor symptoms in Parkinson's disease. Eur J Neurol 2008;15 Suppl 1:14-20.
8. Chaudhuri KR, Martinez-Martin P, Schapira AHV, et al. International
multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson's disease: The NMSQuest study. Mov Disord
2006;21:916-23.
9. Martinez-Martin P, Schapira AHV, Stocchi F, et al. Prevalence of nonmotor symptoms in Parkinson's disease in an international setting; Study using nonmotor symptoms questionnaire in 545 patients. Mov Disord 2007;22:1623-9.
10. Natale G, Pasquali L, Paparelli A, Fornai F. Parallel manifestations of
neuropathologies in the enteric and central nervous systems. Neurogastroenterol Motil 2011;23:1056-65.
11. Cersosimo MG, Benarroch EE. Pathological correlates of gastrointestinal dysfunction in Parkinson's disease. Neurobiol Dis 2012;46:559-64.
12. Ferrer I, Lopez-Gonzalez I, Carmona M, Dalfo E, Pujol A, Martinez A. Neurochemistry and the non-motor aspects of PD. Neurobiol Dis 2012;46:508-26. 13. Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, Sung FC. Polypharmacy
correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore) 2010;89:295-9.
14. Lai SW, Su LT, Lin CH, Tsai CH, Sung FC, Hsieh DP. Polypharmacy increases the risk of Parkinson's disease in older people in Taiwan: a population-based study. Psychogeriatrics 2011;11:150-6.
carcinoma in diabetic patients and risk reduction associated with anti-diabetic therapy: a population-based cohort study. Am J Gastroenterol 2012;107:46-52.
16. Lebouvier T, Neunlist M, Bruley des Varannes S, et al. Colonic biopsies to assess the neuropathology of Parkinson's disease and its relationship with symptoms. PLoS One 2010;5:e12728.
17. Pouclet H, Lebouvier T, Coron E, et al. A comparison between rectal and colonic biopsies to detect Lewy pathology in Parkinson's disease. Neurobiol Dis 2012;45:305-9.
18. Cersosimo MG, Benarroch EE. Autonomic involvement in Parkinson's disease: pathology, pathophysiology, clinical features and possible peripheral biomarkers. J Neurol Sci 2012;313:57-63.
Table 1. Age and baseline comorbidities between IBS group and non-IBS group by gender
Men Women
Irritable bowel syndrome Irritable bowel syndrome
No Yes No Yes
N=32968 N=8242 N= 37524 N= 9381
n (%) n (%) P value n (%) n (%) P value
Age group (year)
40–64 21528 65.3 5382 65.3 0.99 26952 71.8 6738 71.8 0.99
65–84 11440 34.7 2860 34.7 10572 28.2 2643 28.2
Mean (SD) (year)* 58.6 12.3 58.9 12.3 0.06 57.3 11.5 57.6 11.4 0.01
Follow-up years, mean (SD)* 6.52 2.86 6.61 2.86 0.008 6.88 2.76 6.93 2.75 0.11
Baseline co-morbidities Head injury 1083 3.29 321 3.89 0.006 1033 2.75 372 3.97 <0.0001 Hypertension 11469 34.8 3747 45.5 <0.0001 13517 36.0 4148 44.2 <0.0001 Diabetes mellitus 4622 14.0 1577 19.1 <0.0001 5771 15.4 2057 21.9 <0.0001 Hyperlipidemia 4061 12.3 1693 20.5 <0.0001 5706 15.2 2270 24.2 <0.0001 Obesity 156 0.47 56 0.68 0.02 467 1.24 141 1.50 0.048 Dementia 197 0.60 62 0.75 0.11 194 0.52 78 0.83 0.0003 Cerebrovascular disease 3520 10.7 1247 15.1 <0.0001 3677 9.80 1392 14.8 <0.0001 Depression 618 1.87 522 6.33 <0.0001 1180 3.14 922 9.83 <0.0001 Chronic kidney disease 681 2.07 255 3.09 <0.0001 615 1.64 216 2.30 <0.0001
Tobacco use 152 0.46 56 0.68 0.01 29 0.03 12 0.13 0.14
Alcoholism 145 0.44 70 0.85 <0.0001 29 0.08 10 0.11 0.38 Chi-square test and *t-test comparing subjects with irritable bowel syndrome and non-irritable bowel
Table 2. Hazard ratios of Parkinson's disease for the IBS group compared with the non-IBS group by age and follow-up period
Men Women
Irritable bowel syndrome Irritable bowel syndrome
No Yes No Yes
Variable Event Incidence Event Incidence Incidence rate ratio(95% CI)
Adjusted HR†
(95% CI) Event Incidence Event Incidence
Incidence rate ratio(95% CI) Adjusted HR† (95% CI) All 588 2.74 247 4.53 1.66(1.55, 1.77) 1.44(1.24, 1.68) 550 2.13 259 3.98 1.87(1.76, 1.99) 1.55(1.33, 1.80) Age group (year) 40–64 111 0.75 49 1.32 1.75(1.60, 1.91) 1.0 158 0.82 76 1.58 1.91(1.77, 2.06) 1.0 65–84 477 7.06 198 11.4 1.62(1.47, 1.79) 6.46(5.38, 7.77) 392 5.91 183 10.9 1.84(1.67, 2.04) 4.47(3.78, 5.28) Follow-up period ≤ 2 years 158 2.45 64 3.96 1.62(1.50, 1.74) 1.37(1.02, 1.84) 130 1.75 68 3.66 2.09(1.95, 2.24) 1.64(1.21, 2.21) > 2 years 430 2.86 183 4.77 1.67(1.56, 1.79) 1.47(1.23, 1.75) 420 2.28 191 4.11 1.80(1.69, 1.92) 1.52(1.28, 1.81)
Incidence: per 1000 person-years
Table 3. Cox model estimated hazard ratios and 95% confidence intervals of Parkinson’s disease associated with IBS and covariates
Men Women
Crude Adjusted† Crude Adjusted†
Variable HR (95% CI) HR (95% CI) HR (95% CI) HR (95%CI)
Age (per one year) 1.11 (1.10, 1.11) 1.09 (1.08, 1.10) 1.10 (1.09, 1.11) 1.08 (1.07, 1.09) Baseline co-morbidities (yes vs.
no)
Irritable bowel syndrome 1.65 (1.43, 1.92) 1.44 (1.24, 1.68) 1.87 (1.61, 2.17) 1.55 (1.33, 1.80)
Head injury 1.86 (1.37, 2.52) 1.23 (0.90, 1.68) 1.79 (1.28, 2.49) 1.08 (0.77, 1.52) Hypertension 4.00 (3.46, 4.62) 1.48 (1.26, 1.74) 4.74 (4.06, 5.53) 1.63 (1.37, 1.94) Diabetes mellitus 2.21 (1.90, 2.59) 1.22 (1.03, 1.43) 2.81 (2.43, 3.25) 1.32 (1.13, 1.55) Hyperlipidemia 1.43 (1.19, 1.72) 0.95 (0.78, 1.15) 2.25 (1.93, 2.62) 1.12 (0.95, 1.32) Obesity 1.13 (0.43, 3.03) - - 0.80 (0.38, 1.68) - -Dementia 6.82 (4.46, 10.4) 1.71 (1.11, 2.63) 6.07 (3.80, 9.69) 1.20 (0.74, 1.93) Cerebrovascular disease 4.81 (4.17, 5.55) 1.82 (1.56, 2.13) 4.94 (4.27, 5.71) 1.82 (1.56, 2.13) Depression 1.93 (1.40, 2.66) 1.20 (0.86, 1.66) 2.55 (2.01, 3.22) 1.60 (1.26, 2.04) Chronic kidney disease 2.58 (1.84, 3.62) 1.09 (0.77, 1.53) 2.90 (2.01, 4.18) 1.28 (0.88, 1.84)
Tobacco use 1.30 (0.42, 4.05) - - -
-Alcoholism 1.38 (0.58, 3.33) - - -
-†Adjusted HR: adjusted for age, head injury, hypertension, diabetes mellitus, hyperlipidemia, dementia,
Table 4. Hazard ratios and 95% confidence interval for Parkinson’s disease associated with subtypes of IBS
Men Women
Irritable bowel syndrome Irritable bowel syndrome
Variable Crude HR † (95% CI) Adjusted HR† (95% CI) Crude HR† (95% CI) Adjusted HR† (95% CI) Non-irritable bowel syndrome
(reference) 1(reference) 1(reference) 1(reference) 1(reference)
Irritable bowel syndrome,
constipation predominant 1.67(1.44, 1.94) 1.45(1.25, 1.69) 1.84(1.59, 2.14) 1.53(1.31, 1.79) Irritable bowel syndrome,
diarrhea predominant 1.34(0.72, 2.51) 1.21(0.65, 2.27) 2.41(1.44, 4.03) 1.95(1.17, 3.27) HR, hazard ratio; CI, confidence interval
†Adjusted HR: adjusted for age, head injury, hypertension, diabetes mellitus, hyperlipidemia, dementia,