Endodontic treatment outcome can be assessed by case-control or follow-up epidemiologic studies. Case-control studies evaluate a relatively small number of endodontic treatment and control
cases. The criteria used for assessing success and failure may be different, therefore, endodontic treatment outcomes vary considerably between studies.1Follow-up epidemiologic studies examine
Five-year Follow-up Study of Tooth Extraction
After Nonsurgical Endodontic Treatment in a
Large Population in Taiwan
Shih-Chung Chen,1Ling-Huey Chueh,2Hsin-Ping Wu,3Chuhsing Kate Hsiao3*
Background/Purpose: Nonsurgical retreatment, apical surgery and tooth extraction are three major
unto-ward events following nonsurgical root canal treatment (NSRCT). The purpose of this study was to assess untoward events and total tooth extraction after NSRCT in a large population of dental patients in Taiwan.
Methods: A total of 1,588,217 teeth treated with NSRCT in Taiwan in 2000 were analyzed for the first
untoward event and total tooth extraction over a 5-year follow-up period.
Results: The first untoward event occurred in 192,488 (12.1%) teeth within the first 5 years
post-treatment. Nonsurgical retreatment was performed on 69,273 (36.0%) of these teeth, 4741 (2.5%) received apical surgery, and 118,474 (61.5%) were extracted. In addition, 1,463,312 (92.1%) teeth treated with NSRCT were retained in the oral cavity, and 124,905 (7.9%), including 24,499 (19.6%) anterior teeth, 33,356 (26.7%) premolars, and 67,050 (53.7%) molars were extracted within the 5 years of follow-up. Of these 124,905 teeth, 5869 (4.7%) were extracted after nonsurgical retreatment, 562 (0.4%) after apical surgery, and 118,474 (94.9%) after the first untoward events. There were significantly more molars (54.5% vs. 43.3%) and significantly fewer anterior teeth (19.0% vs. 27.5%) extracted in private clinics than in hospitals (p< 0.001). The overall tooth extraction rate was significantly greater in hospitals (10.0%) than in private clinics (7.7%, p< 0.001). However, tooth extraction procedures were almost evenly distributed over the 5-year follow-up period, with the annual incidence being close to 20%. The overall mean tooth extraction time was significantly greater in private clinics (2.52± 1.43 years) than in hospitals (2.29± 1.50 years, p < 0.001).
Conclusion: We conclude that tooth extraction (61.5%) is the most common of the three untoward
events, and approximately 95% of tooth extractions are performed at the time of the first untoward event. NSRCT is still a valuable dental procedure in Taiwan because of the high rate (92.1%) of tooth retention after 5 years of follow-up. [J Formos Med Assoc 2008;107(9):686–692]
Key Words: general population, root canal treatment, tooth extraction, tooth retention,
untoward events
©2008 Elsevier & Formosan Medical Association
. . . .
1Department of Health, The Executive Yuan, 2Elite Dental Clinic, and 3Department of Public Health, College of Public
Health, National Taiwan University, Taipei, Taiwan.
Received: March 4, 2008 Revised: March 26, 2008 Accepted: April 1, 2008
*Correspondence to: Professor Chuhsing Kate Hsiao, Department of Public Health,
College of Public Health, National Taiwan University, 17 Xu-Zhou Road, Taipei 100, Taiwan.
a very large number of endodontically-treated pa-tients in the general population. There are three examples of this type of study, which use an alter-native approach to evaluate cases of nonsurgical root canal treatment (NSRCT) from the database of a nationwide health insurance organization.2–4 Epidemiologic studies assess a large number of endodontic treatments performed by dentists and endodontists, and their success rate may represent outcomes in the general population.2–4
Epidemiological radiographic surveys have re-ported a relatively lower frequency of high-quality root canal filling ranging from 14% to 65%.5Our previous study evaluated the technical quality of root canal filling in 1085 cases treated with NSRCT, randomly selected from a large represen-tative sample of the Taiwanese population, and found that only 30.3% of the teeth had received good-quality endodontic work.6
In Taiwan, the national health care plan was implemented in March 1995. This plan covers nearly all medical treatments and a portion of den-tal treatments, including surgical and nonsurgi-cal endodontic procedures. The National Health Insurance (NHI) is managed by the Bureau of NHI (BNHI) which insures approximately 21 million individuals from a total population of 22 million. Providers have to make a claim for each treatment to the BNHI, therefore, a large computerized med-ical and dental database for each insured individ-ual has been kept since March 1995. Access to BNHI’s invaluable national data set makes it possi-ble to study the first untoward events, including nonsurgical retreatment, apical surgery and tooth extraction, as well as tooth retention rate following NSRCT.
Two large epidemiologic studies using a long follow-up period have found very high tooth re-tention rates (94–97%) among a large number of NSRCT cases collected from an insurance company database.2,3These results motivated our group to study the first untoward events and tooth retention rate over a 5-year follow-up period for 1,557,547 teeth treated with NSRCT in Taiwan in 1998. We found that the first untoward events occurred in 159,680 (10.3%) of these teeth during the 5-year
follow-up period. Moreover, a high 5-year tooth retention rate of 92.9% was observed.4Here, we have further assessed the first untoward events and tooth retention rate over a 5-year follow-up period for 1,588,217 teeth that were treated with NSRCT in 2000. We compared the types of teeth extracted between hospitals and private clinics. Tooth extraction rates and mean extraction times were compared between six different regions of Taiwan, and between hospitals and private clinics in six different regions. In addition, the distribu-tion of total tooth extracdistribu-tion cases in each of the five follow-up periods was studied and compared between six different regions of Taiwan.
Methods
We analyzed the initial NSRCT cases completed in 2000 from a pool of 21 million individuals in-sured by the NHI plan since March 1995. Details of 1,588,217 NSRCT procedures claimed in 2000 were collected by searching the database for the specific BNHI procedure codes, 90001C, 90002C and 90003C, which represent NSRCT performed in teeth with one, two, or three or more root canals, respectively. These 1,588,217 NSRCT proce-dures were principally performed by dentists and endodontists, and occasionally by other dental specialists.
The following information was also collected for each NSRCT procedure: tooth identification number, date of completion of endodontic proce-dure, and patient age. To ensure personal privacy, patient data, including identification number, gender and medical records, were not released by the BNHI. Each NSRCT tooth was followed for a continuous period of 5 years from the comple-tion date of the endodontic procedure in 2000. A maximum of 25 related subsequent treatment codes and dates were collected. Of particular in-terest was evaluation of the first and last proce-dures, including untoward events, defined as nonsurgical retreatment, apical surgery and tooth extraction, in two prior epidemiological studies,2,3 for each tooth within the 5-year follow-up period.
The occurrence of untoward events was analyzed by searching the database for the BNHI proce-dure codes, 90001C, 90002C, 90003C, 90015C, 92030C, 92031C, 92032C, 90010C, 92013C and 92014C. The BNHI does not provide codes for non-surgical retreatment. Therefore, a second appear-ance of the codes 90001C, 90002C and 90003C for the same tooth represented nonsurgical retreat-ment for a tooth with one, two, or three or more root canals, respectively. Procedure 90015C, for root canal enlargement and debridement, also belongs to the nonsurgical retreatment category. Procedures 92030C, 92031C and 92032C are the codes for apicoectomy in maxillary and mandibu-lar anterior teeth, premomandibu-lars and momandibu-lars, respec-tively; and 90010C is the code for root-end filling. The item for apical surgery included both apicoec-tomy (92030C, 92031C, 92032C) and root-end filling (90010C). The BNHI codes for simple and complicated tooth extraction were 92013C and 92014C, respectively.
The first subsequent procedure for each NSRCT tooth was analyzed to disclose whether any untoward event occurred after the comple-tion of NSRCT. In addicomple-tion, the total number and incidence of each untoward event for all NSRCT teeth were calculated. The last related procedure for each NSRCT tooth was used to calculate how many teeth were extracted, and in turn, to deter-mine the percentage of teeth retained after comple-tion of the full 5-year follow-up period. Patient outcome criteria were applied blindly because the dentists submitting claims were not aware that the data would be used for future endodontic out-come analysis. At the end of the follow-up period in 2005, about 99% of the patients remained in the same NHI plan, which indicated very modest losses from the patient pool.
The number of extracted anterior teeth, pre-molars and pre-molars were counted and compared between hospitals and private clinics using the χ2test. Tooth extraction rates were compared be-tween six different regions (Taipei, north, cen-tral, south, Kaoping and east regions) of Taiwan, and between hospitals and private clinics in each of the six regions of Taiwan, using the χ2 test.
Distribution of total tooth extractions in each of the 5 follow-up years in the six different regions of Taiwan was analyzed. Finally, the mean tooth extraction times after completion of NSRCT were compared between the six different regions of Taiwan by analysis of variance (ANOVA), and be-tween hospitals and private clinics in each of the six regions by Student’s t test. A p value of less than 0.05 was considered statistically significant for all tests.
Results
A total of 1,588,217 teeth treated with NSRCT in 2000 were evaluated. First untoward events oc-curred in 192,488 (12.1%) teeth during a 5-year follow-up period. Nonsurgical retreatment was performed for 69,273 (36.0%) of these teeth, 4741 (2.5%) received apical surgery, and 118,474 (61.5%) were extracted. At the end of the follow-up period, 124,905 (7.9%) teeth were extracted, which yielded a 5-year tooth retention rate of 92.1% for all NSRCT teeth. Of these 124,905 teeth, 5869 (4.7%) were extracted after nonsurgi-cal retreatment, 562 (0.4%) after apinonsurgi-cal surgery, and 118,474 (94.9%) at the first untoward event (Table 1).
A total of 124,905 teeth, including 24,499 (19.6%) anterior teeth, 33,356 (26.7%) premolars, and 67,050 (53.7%) molars were extracted. In both hospitals and private clinics, there was a trend where more molars than anterior teeth or pre-molars were extracted. There were significantly more molars (54.5% vs. 43.3%) and significantly fewer anterior teeth (19.0% vs. 27.5%) extracted in the private clinics than in hospitals (p< 0.001, Table 2).
There was a significant difference in the tooth extraction rate between six different regions of Taiwan (p< 0.001, χ2test). The east region had the highest tooth extraction rate (10.4%) and the Taipei region had the lowest (7.5%, Table 3). The overall tooth extraction rate was significantly greater in hospitals (10.0%) than in private clinics (7.7%, p< 0.001). The individual tooth extraction
Table 1. Relationship between total number of follow-up cases and the first untoward events after completion of nonsurgical endodontic treatment*
All teeth
First untoward events
Total Nonsurgical retreatment Apical surgery Extraction
Extraction cases (n= 124,905) 5869 (4.7) 562 (0.4) 118,474 (94.9) 124,905 (100.0) Non-extraction cases (n= 1,463,312) 63,404 (93.8) 4179 (6.2) 0 (0) 67,583 (100.0) Total follow-up cases (n= 1,588,217) 69,273 (36.0) 4741 (2.5) 118,474 (61.5) 192,488 (100.0)
*Data presented as n (%).
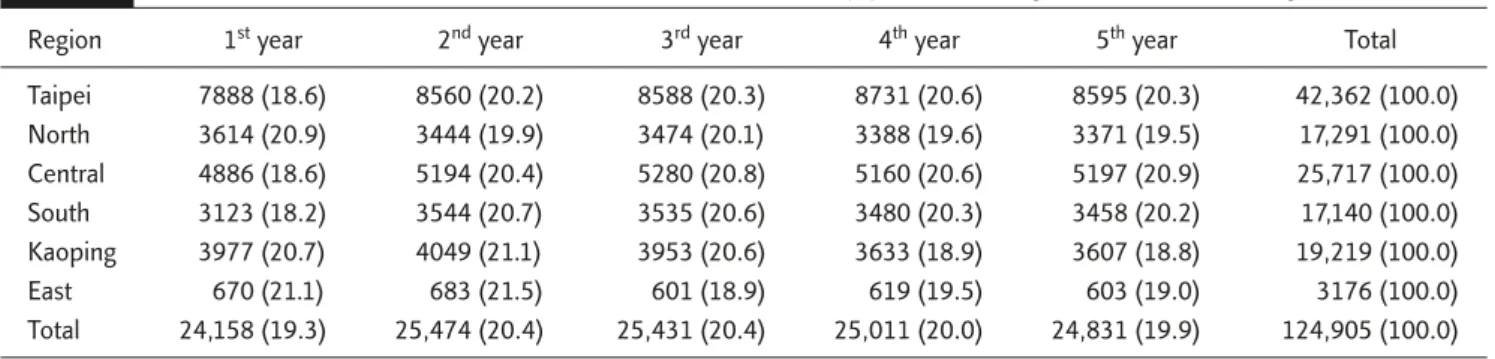
rate in all six regions of Taiwan was also signifi-cantly greater in hospitals than in private clinics (Table 3). However, tooth extraction procedures were nearly evenly distributed over the follow-up of 5 years, with the annual incidence being close to 20%. This trend was similar in each of the six different regions of Taiwan (Table 4).
A significant difference in the mean tooth ex-traction time was found between the six different regions of Taiwan (p< 0.001, ANOVA). Kaoping and east regions had the lowest mean tooth ex-traction time (2.44± 1.44 and 2.44 ± 1.45 years, respectively), whereas Taipei had the highest (2.54±1.43 years, Table 5). The overall mean tooth
Table 2. Comparison of the number of extracted anterior teeth, premolars and molars between hospitals and private clinics*
All teeth Anterior teeth Premolars Molars χ2test
Hospital type p< 0.001
Hospital 8529 (100.0) 2348 (27.5) 2490 (29.2) 3691 (43.3)
Private clinic 116,376 (100.0) 22,151 (19.0) 30,866 (26.5) 63,359 (54.5)
Total 124,905 (100.0) 24,499 (19.6) 33,356 (26.7) 67,050 (53.7)
*Data presented as n (%).
Table 3. Tooth extraction rates in six different regions of Taiwan according to hospital type*
All teeth Taipei region North region Central region South region Kaoping region East region Total Hospitals Extracted teeth 2429 1488 1973 809 1464 366 8529 Total teeth 25,903 15,216 18,441 9551 13,117 3159 85,387 Extraction rate 9.4% 9.8% 10.7% 8.5% 11.2% 11.6% 10.0% p† < 0.001 < 0.001 < 0.001 0.026 < 0.001 0.026 < 0.001 Private clinics Extracted teeth 39,933 15,803 23,744 16,331 17,755 2810 116,376 Total teeth 538,589 206,951 299,835 208,341 221,811 27,303 1,502,830 Extraction rate 7.4% 7.6% 7.9% 7.8% 8.0% 10.3% 7.7% Overall Extracted teeth 42,362 17,291 25,717 17,140 19,219 3176 124,905 Total teeth 564,492 222,167 318,276 217,892 234,928 30,462 1,588,217 Extraction rate 7.5% 7.8% 8.1% 7.9% 8.2% 10.4% 7.9%
Table 4. Distribution of tooth extraction cases in each of the 5 follow-up years according to the six different regions of Taiwan*
Region 1styear 2ndyear 3rdyear 4thyear 5thyear Total
Taipei 7888 (18.6) 8560 (20.2) 8588 (20.3) 8731 (20.6) 8595 (20.3) 42,362 (100.0) North 3614 (20.9) 3444 (19.9) 3474 (20.1) 3388 (19.6) 3371 (19.5) 17,291 (100.0) Central 4886 (18.6) 5194 (20.4) 5280 (20.8) 5160 (20.6) 5197 (20.9) 25,717 (100.0) South 3123 (18.2) 3544 (20.7) 3535 (20.6) 3480 (20.3) 3458 (20.2) 17,140 (100.0) Kaoping 3977 (20.7) 4049 (21.1) 3953 (20.6) 3633 (18.9) 3607 (18.8) 19,219 (100.0) East 670 (21.1) 683 (21.5) 601 (18.9) 619 (19.5) 603 (19.0) 3176 (100.0) Total 24,158 (19.3) 25,474 (20.4) 25,431 (20.4) 25,011 (20.0) 24,831 (19.9) 124,905 (100.0) *Data presented as n (%).
extraction time was 2.50± 1.44 years after com-pletion of NSRCT for all teeth, and was signifi-cantly greater in private clinics (2.52± 1.43 years) than in hospitals (2.29± 1.50 years, p < 0.001). Furthermore, the individual mean tooth extrac-tion time in each of the six regions of Taiwan was also significantly greater in private clinics than in hospitals (Table 5).
Discussion
Recently, an epidemiological model with a very large sample size was used to evaluate endodon-tic treatment outcome.2,3 In this type of study, tooth retention becomes an evaluative criterion for the clinical outcome of NSRCT. Three recent studies have evaluated tens of thousands to more than one million NSRCT cases.2–4Lazarski et al reported that 94.4% of NSRCT teeth remained
functional over an average follow-up period of 3.5 years.2Salehrabi and Rotstein found that 97% of teeth were retained in the oral cavity 8 years after initial NSRCT.3Our recent study showed that 92.9% of 1,557,547 teeth treated in Taiwan in 1998 were retained in the oral cavity 5 years after NSRCT.4The 5-year tooth retention rate of 92.1% in the present study was comparable to that (92.9%) in our recent study.4Other follow-up in-vestigations by Friedman and Mor revealed that 91–97% of endodontically treated teeth remained functional over time.1 The results of the above studies indicate a high tooth retention rate of > 91% after NSRCT. It appears reasonable to con-clude that NSRCT is a valuable dental procedure because of the high tooth retention rate.
Epidemiologic studies also provide some in-formation on the group of teeth experiencing an untoward event. Here, we found that 61.5% of the 192,488 teeth with the first untoward event Table 5. Mean tooth extraction times after completion of nonsurgical endodontic treatment in six different regions of Taiwan
according to hospital type
Mean tooth extraction time± standard deviation (yr) Hospital type
Taipei region North region Central region South region Kaoping region East region Total Hospitals 2.35± 1.51 2.18± 1.52 2.31± 1.51 2.30± 1.47 2.24± 1.48 2.41± 1.43 2.29± 1.50 (n= 2429) (n= 1488) (n= 1973) (n= 809) (n= 1464) (n= 366) (n= 8529) p* < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 0.709 < 0.001 Private clinics 2.55± 1.43 2.49± 1.44 2.54± 1.43 2.55± 1.42 2.45± 1.44 2.44± 1.45 2.52± 1.43 (n= 39,933) (n= 15,803) (n= 23,744) (n= 16,331) (n= 17,755) (n= 2810) (n= 116,376) Overall 2.54± 1.43 2.46± 1.45 2.52± 1.44 2.53± 1.42 2.44± 1.44 2.44± 1.45 2.50± 1.44 (n= 42,362) (n= 17,291) (n= 25,717) (n= 17,140) (n= 19,219) (n= 3176) (n= 124,905)
were extracted during the 5-year follow-up pe-riod. This result was comparable to the corre-sponding result (65.5%) of our previous study.4 Lazarski et al reported that 59% of 4212 teeth that suffered a first untoward event were ex-tracted over a minimum follow-up interval of 2 years.2 Salehrabi and Rotstein also demon-strated that 73.5% of 57,361 teeth with the first untoward events were extracted.3 All four of these studies indicate that tooth extraction is the most common initial untoward event following NSRCT.
The frequency of apical surgery after NSRCT was 15% and 16.4% in the studies of Lazarski et al2and Salehrabi and Rotstein,3respectively, with both rates higher than the 2.5% and 2.7% demonstrated in our present and previous stud-ies,4respectively. In the USA, endodontics is one of the American Dental Association’s recognized specialties. Lazarski et al found that approximately 70% of all apical surgery following NSRCT is per-formed by endodontists in the USA.2In Taiwan, apical surgery is considered a high-level technique that is always taught in postgraduate courses, and therefore, it is performed mostly by endodontists or oral surgeons. Thus, global differences in en-dodontic training may contribute to differences in the rates of apical surgery versus tooth extraction. In this study, more molars than anterior teeth or premolars were extracted in hospitals and pri-vate clinics. Our previous study evaluated the technical quality of NSRCT in Taiwan and showed that significantly more molars have poor en-dodontic work compared to that of anterior teeth and premolars in both hospitals and private clin-ics.6This might explain why more molars than anterior teeth or premolars were extracted in the present study. In Taiwan, more well-trained en-dodontists work in hospitals than in private clin-ics, which results in a higher percentage of teeth receiving good endodontic work being found in hospitals rather than in private clinics.6Easier en-dodontic cases are treated in private clinics rather than in hospitals, and the majority of difficult or failed endodontic cases are referred to hospitals for treatment. Moreover, dentists may feel more
comfortable performing apical surgery in the anterior regions than in the premolar or molar areas because of better visibility and easier access in the former. The above-mentioned reasons par-tially explain why there were significantly more molars and significantly fewer anterior teeth ex-tracted in private clinics than in hospitals, why the overall tooth extraction rate was significantly greater in hospitals than in private clinics, and why the overall mean tooth extraction time after completion of NSRCT was significantly greater in private clinics than in hospitals.
The nonsurgical-retreatment frequency was 36%, which was comparable to that (31.7%) of our previous study,4but higher than that deter-mined by Lazarski et al2 (26%) and Salehrabi and Rotstein (10.1%).3There are several explana-tions for this finding. First, approximately 70% of the teeth treated with NSRCT in Taiwan were either inadequately filled or incompletely obtu-rated, as evaluated by radiographic surveys.6 When performing prosthodontic work on im-properly treated teeth, the dentist may favor non-surgical retreatment in order to improve the prognosis. Second, nonsurgical retreatment is covered by the NHI in Taiwan; therefore, patients may initially prefer this conservative treatment modality. Third, compared to their US counter-parts, dentists in Taiwan may lack the training necessary for apical surgery, so are more likely to perform nonsurgical retreatment.
In conclusion, tooth extraction (61.5%) is the most common procedure among the three first untoward events. Approximately 95% of tooth extraction procedures are performed at the first untoward event, and the remaining 5% are per-formed after initial nonsurgical retreatment or apical surgery. NSRCT is still a valuable dental procedure because of the high rate (92.1%) of tooth retention 5 years after NSRCT in Taiwan.
Acknowledgments
The authors extend their thanks to the BNHI in Taiwan for the help provided during the study.
This research was supported by grant DOH95-HI-1001 from the Department of Health, Executive Yuan, Taiwan.
References
1. Friedman S, Mor C. The success of endodontic therapy— healing and functionality. J Calif Dent Assoc 2004;32: 493–503.
2. Lazarski MP, Walker WA, Flores CM, et al. Epidemiologi-cal evaluation of the outcomes of nonsurgiEpidemiologi-cal root canal
treatment in a large cohort of insured dental patients.
J Endod 2001;27:791–6.
3. Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod 2004;30:846–50.
4. Chen SC, Chueh LH, Hsiao CK, et al. An epidemiological study of tooth retention after nonsurgical endodontic treatment in a large population in Taiwan. J Endod 2007; 33:226–9.
5. Eriksen HM, Kirkevang LL, Petersson K. Endodontic epi-demiology and treatment outcome: general considera-tions. Endod Topics 2002;2:1–9.
6. Chueh LH, Chen SC, Lee CM, et al. Technique quality of root canal treatment in Taiwan. Int Endod J 2003;36:416–22.