A CAUSAL MODEL OF REHABILITATION RESOURCE USE FOR SUBJECTS
WITH SPINAL CORD INJURY IN TAIWAN
Lyinn Chung,
1Ay-Woan Pan
2and Yen-Ho Wang
3From the1Department of Accounting, Graduate School of Management, Yuan-Ze University, Jung-Li, Taiwan,2School of Occupational Therapy, College of Medicine, National Taiwan University, Taipei, Taiwan,3Department of Physical Medicine
and Rehabilitation, College of Medicine, National Taiwan University, Taipei, Taiwan
Objective: The aim of this study was to construct an adequate causal model of rehabilitation resource use based on a Taiwanese rehabilitation database system.
Design: Cross-sectional analysis of data from a Taiwanese rehabilitation database system.
Subjects: Records from 68 patients (51 men, 17 women; mean age 43 years) with spinal cord injuries were used in the study.
Methods: Path analysis was used to identify a better-fitted model for patients with spinal cord injuries.
Results and conclusion: The results showed that the final causal model fits the data well. The findings also reveal that activities of daily living have the largest total effect on length of stay, whereas subjective well-being and gender have indirect effects on length of stay, mediating through activities of daily living and subjective well-being, respec-tively. The impact of subjective well-being on the length of stay in hospital for patients with spinal cord injuries deserves special attention, as the quality of life issue plays a vital role in rehabilitation of these patients. The influence of subjective well-being on activities of daily living suggests that therapy targeted at improving patients’ subjective well-being is necessary. Additionally, the impact of sexual dysfunction of patients with spinal cord injuries should be investigated further.
Key words: spinal cord injuries, rehabilitation, length of stay, activities of daily living, well-being.
J Rehabil Med 2003; 35: 208–212
Correspondence address: Ay-Woan Pan, 100, No. 7, Chung-Shan S. Road, School of Occupational Therapy, College of Medicine, National Taiwan University, Taipei, Taiwan. Tel: 011 886 2 2312 3456, ext. 6639. Fax: 011 886 2 2371 0614. E-mail: aywoan@ha.mc.ntu.edu.tw
Submitted July 18, 2002; accepted February 10, 2003
INTRODUCTION
Taiwan implemented a national health insurance plan in 1995. Ten medical centres in Taiwan offer medical care for a population of 23 million. They provide professional rehabilita-tion services for people with any type of disability resulting from disease or trauma, as well as more intensive care services. There are also sub-acute rehabilitation institutions, rehabilitation
wards in local hospitals, and nursing homes to provide rehabilitation services. Patients who need rehabilitation receive physical therapy, occupational therapy and speech therapy tailored to their individual needs. The purpose of this study is to develop a model of resources used for inpatient rehabilitation in Taiwan, based on literature reviews and related models (e.g. Anderson’s model of service utilization) (1–5).
The goal of medical rehabilitation is to promote maximal independence in the clients served (6–7). In order to provide effective rehabilitation services, clinicians need to understand factors related to clients’ independence. Rehabilitation services can then be targeted at functions pertinent to clients’ indepen-dence. In the past decade, several studies investigating the predictive factors relevant to rehabilitation outcomes have revealed that age, gender, severity of illness, duration of onset, diagnosis, functions of daily living, cognitive functions and psychological well-being are related to the length of rehabilitation hospitalization (8–11). Other authors (12–17) found that the type of injury may affect the rehabilitation outcome for patients with spinal cord injuries (SCI). Researchers have further indicated that sociability, marital status, occupation and career planning are the factors which affect satisfaction and quality of life for patients with SCI (10–11). As a result, these variables might be important for the adjustment of disease and quality of life for patients with SCI (9–11). Since improving quality of life of patients with SCI would be an ultimate goal of rehabilitation, these factors should be examined for their relationship to quality of life.
Using a database to assess the efficacy of rehabilitation programs is the first step toward the establishment of a feasible model. Experience from western countries indicates that a database system approach can be used to achieve these aims (18–19). However, there is no standard database system available in Taiwan. Therefore, the Taiwanese Rehabilitation Database System (TaRDS) was established to facilitate inter-institution comparisons of the intervention efficacy, to conduct further outcome research and to be a baseline data for health care reimbursement (20–21). It can also provide a consistent database for future use in program evaluation and quality assurance.
TaRDS consists of 3 main parts: the patient’s demographic data; the patient’s scores on the Taiwanese Rehabilitation Functional Scale (TaRFS); and related outcome information (20–21). The TaRFS encompasses 3 domains: activities of daily living (ADL); cognitive-social skills (CSS); and subjective well-being (SWB) (22). The integration and progression of these
functions of the patients will empower them to live indepen-dently and satisfactorily in their environment (21). This instrument is supported by its test-retest reliability across times and raters and shows its construct validity (21–22).
The causal model of this study was developed according to literature relevant to the prediction of rehabilitation outcomes (12–17). Four key predictors for rehabilitation service use are proposed in the study. They include personal characteristic variables, ADL, CSS and SWB. These variables were derived due to their extensive use throughout previous research and their theoretical and empirical relevance to the area of concern (23). Length of stay (LOS) was used as the proxy variable for rehabilitation outcome because it is closely related to resource consumption for each client. Moreover, patients usually discharge upon recovery of the functions; therefore, LOS in hospital is a proxy for the rehabilitation outcome.
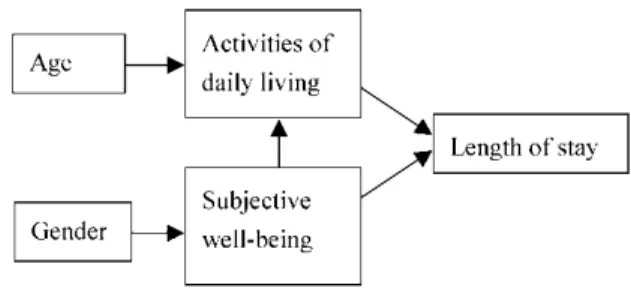
Gender differences influence the level of assistance needed for basic ADL (24). Data from major national surveys confirmed the association between age and disability (24). Hence, we considered age and gender as predicting variables in the model. Others also proposed predictors pertaining to the functional needs of rehabilitation patients. The relationship between the severity of SCI and patients’ functional status was high (9), therefore, functional status of patients was used as predictor for rehabilitation resource use. Functions of the clients include ADL, CSS and SWB. Since the patients with cognitive impairment were not included in the study, CSS was not considered in the model. Basic ADL ability is the most powerful factor in prediction studies (8, 16–17). We thus hypothesized that they will continue to show the predictive validity in explanation of the variance of LOS. Finally, the proposed predictive model for patients with SCI is shown in Fig. 1, showing the relationship among these variables and the directions of correlation. The assumptions for the hypothesized model are as follows:
. Age, gender, ADL and SWB are predictive variables for LOS. . ADL of the patients would directly affect LOS negatively.
Namely, LOS increases as the severity of ADL limitation increases.
. As SWB improves, ADL improves.
. As age increases, ADL decreases.
. Gender is an exogenous variable influencing SWB.
SUBJECTS AND METHODS
SubjectsSixty-eight patients (51 men, 17 women; mean age 43 years) with SCI were recruited from 2 rehabilitation units in university-affiliated hospitals in northern Taiwan. Rated as the first-class medical centres in Taiwan, these hospitals served a variety of patients regardless of diagnoses, severity and complications. Patients admitted to manage the problems of infections or ulcers, as well as those who were diagnosed as having cognitive deficits were excluded from the study.
Procedures
In order to document the outcome of rehabilitation intervention, a reliable functional status measure is needed (25). Since instability of the rater’s ratings will contaminate the data (26), a proper rater training protocol is necessary. This study adapts a training protocol comprising 2 sessions of lecturing and discussion. Each session takes about 3 hours. The contents of the course contain: (i) introduction of the TaRFS background and rating principles; (ii) introduction of the TaRFS item definition and administration instruction; and (iii) pilot testing and feedback. All patients were tested on TaRFS and were interviewed to secure relevant database information at the first week upon admission to the rehabilitation wards.
Instrumentation
The TaRFS was developed based on the consensus that functional status is an important predictor of outcome for inpatient rehabilitation (6, 12– 13). Since the functional status measure encompasses multiple domains (6, 18–19), a multidimensional assessment is needed to obtain a comprehensive view of the patient (6–7). Several related scales used worldwide were reviewed (27–29); of these, the Functional Indepen-dence Measure (FIM) (18), Level of Rehabilitation Scale (LORS) (19), Beck Depression Scale (30), Medical Outcome Study and Short Form 36 (31) were influential in the construction of the TaRFS. The TaRFS
Fig. 1. Initial path model.
Table I. Taiwanese Rehabilitation Functional Scale
ADL subscale Cognitive-social subscale Subjective well-being subscale
1. Feeding 1. Orientation 1. Health perception
2. Grooming 2. Problem solving—specific 2. Mood
3. Dressing-Upper body 3. Problem solving—general 3. Influence on social interaction 4. Dressing-Lower body 4. Comprehension 4. Recovery expectation
5. Transfer-chairs 5. Expression 5. Perceived competency
6. Transfer-toilet 7. Toileting 8. Bathing 9. Mobility 10. Stairs
differs from the Barthel Index, FIM and LORS in several aspects: first, items related to bowel and bladder control were not included because these items may represent functions more closely related to physiolo-gical aspects (21); second, the definitions of individual items are designed to suit the customs and rules in Taiwan; third, the SWB subscale was constructed to represent additional dimension of function. The difference between the TaRFS and the FIM can also be found in the references (20–22). Items related to mood, health perception and perceived competency were included (31–33) for the SWB subscale in particular, since there were few functional instruments addressing this issue. In addition to the sampling of related items from these scales, specific cultural background and tools were addressed in the assessment. For example, for the ADL item “feeding”, the use of chopsticks was regarded as one of the abilities to be performed in evaluation; for the item “bathing”, to take a bath on a bench or chair was regarded as acceptable. The item “illness’s influence on social interaction” was included in the SWB subscale since the Chinese perceive “saving face” as an important inherent value (33), and getting ill seemed to be regarded as “losing face” by some families. Consequently, many patients will choose not to disclose their illness and disability to their relatives and friends, and this may have a huge impact on patients’ social interaction. The TaRFS consists of 20 items covering 3 constructs: ADL, CSS and SWB. Each item of the TaRFS is rated on a 7-point rating scale based on suggestions from Streiner and Norman (26). For the ADL and CSS scales, the rating scale ranges from totally dependent (score of 1) to totally independent (score of 7). Occupational therapists rated these 2 scales. For the SWB scale, the range of the scale is from “totally disagree with the statement” (score of 1) to “totally agree with the statement” (score of 7). Patients rated it themselves. The scores of the TaRFS represent the amount of assistance needed for the clients to perform specific activity and the degree of perception on his/her own health and psychological state. Moreover, since actual observation of the perfor-mance could provide accurate information about the patient, the TaRFS was designed to rate patient’s performance by actual observation of patient’s performance within the hospital ward environment (13–15).
The manual provided administration instruction and rating definition. Table I lists the individual items of the TaRFS.
Statistical analyses
Statistical analyses of the study include the descriptive statistics for each variable in the causal model, the computation of correlation coefficients among all variables and the application of path analysis to validate the causal model. Variables used in this study include age, gender, LOS, ADL and SWB. The definition of LOS is the stay duration from admission to discharge during the rehabilitation stage. ADL is the sum of item scores in the ADL subscale. Similarly, SWB is the sum of item scores in the SWB subscale. Path analysis is the generalization of multiple regression. The p-value is set at 0.05 for the overall F statistics and individual T statistics obtained at each step and each path.
Path analysis was introduced by Sewell Wright and popularized by Duncan (35–36). The merits of this method are to interpret linear relationships among a set of variables and to deconstruct the correlation into direct and indirect effect (36). Results of path analysis enable us to determine the effect of predictive variables on LOS and the relative importance of each predictor in the causal model. They are accomplished with standardized path coefficients. A better-fitting model can be obtained through appropriate T-values, p-value ofw2test, and goodness
of fit indices (GFI) (37). All analyses were performed using Statistical Analysis System 6.12 (38) and LISREL 8.3 (39).
RESULTS
The average LOS was 41 days. The correlation matrix for variables used in the causal model can be found in Table II.
Table III shows the regression coefficients and standardized coefficients for initial causal model, which is depicted in Fig. 1. The path (age to ADL) was not significant. The causal relationship between age and ADL was small and not significant. SWB is as important as ADL for patients with SCI in the causal model. In addition, the path (gender to SWB) is marginally
Table II. Correlation matrix among variables in path model Variable Age Gender ADL SWB LOS Age 1.00000
Gender 0.16003 1.00000
ADL 0.21394 0.00788 1.00000
SWB 0.02069 0.21329 0.24294 1.00000
LOS 0.05644 0.04814 0.36716 0.25582 1.00000 ADL = activities of daily living; SWB = subjective well-being; LOS = length of stay.
Table III. Path analysis for the initial model
Dependent variable Independent variable Standardized coefficient Regression coefficient p-value R2
SWB Gender 0.213 2.828 0.0807 0.045
ADL Age 0.209 0.202
SWB 0.238* 0.710* 0.0003* 0.104
LOS ADL 0.324* 0.483*
SWB 0.177 0.785 0.0006* 0.165
*p-value<0.05,p-value<0.1. ADL = activities of daily living; SWB = subjective well-being; LOS = length of stay.
Table IV. Path analysis for the final model
Dependent variable Independent variable Standardized coefficient Regression coefficient p-value R2
SWB Gender 0.213 2.828 0.0807 0.059
ADL SWB 0.243* 0.722* 0.0003* 0.045
LOS ADL 0.367* 0.547 0.0006* 0.135
*p-value<0.05,p-value<0.1. ADL = activities of daily living; SWB = subjective well-being; LOS = length of stay. Fig. 2. Final path model.
significant. We kept this path because male patients showed a higher variation in SWB score than did female patients (10–11). Fig. 2 shows the revised causal model 2. Table IV shows the result of path analysis for the revised models. ADL is the only direct predictor, which affects LOS. Both SWB and gender affect LOS indirectly through other predictors. The good-fitting models should have GFI>0.9 and AGFI >0.9. Failure to reject the null hypothesis will lead to the conclusion that the revised model fits the data. The results showed GFI = 0.991> 0.9, AGFI = 0.965> 0.8, and p-value = 61% > 5%. It suggests that the revised causal model fit the data well. Table V is the result of a break down of direct, indirect, causal and non-causal components of the path model. SWB and ADL have a strong direct relationship with ADL and LOS, respectively. ADL is the only direct predictor for LOS and has a moderate negative effect on LOS. Namely, LOS increases as ADL deteriorates. This indicates that SWB has a remote relationship with LOS mediated by ADL. Clients with a high (good) SWB score will tend to perform better on ADL, which results in a shorter LOS.
DISCUSSION
This study represents the first attempt to establish a model for understanding the phenomenon of inpatient rehabilitation re-source use in Taiwan. The model can serve as a framework to comprehend the dynamics of the interrelationship among predictors and LOS. The awareness of these relationships can guide the treatment team to focus on those pertinent clinical factors and set up treatment priorities for the patients congruent with the model. The path coefficients used in the current study can be understood as indices of the direct effects of each of the independent variables on the dependent variables. In our model, a unit change in ADL will result in 0.367 units of decrease in LOS. Some of the findings of the initial path model deserved special attention. Firstly, age does not have a significant effect on ADL. Although there is some evidence of the effect of age on functional ability in the literature, no causal relationship was established in the past studies (23). This is probably because the majority of SCI patients are young, thus age does not affect LOS. Secondly, ADL has the largest total effect on LOS. This is consistent with the results from previous studies in the literature (9, 15). It means that the independence of the ability of ADL for patients will affect LOS of the patients. Moreover, the ADL indicator is the most significant predictor on resource use for
patients with SCI; the effect is about 1.4 times the influence of SWB on LOS. The results of the ADL effect on LOS provide evidence that in Asian culture also, the rehabilitation of patients with SCI needs to be targeted at ADL functions as has been shown in western countries.
Thirdly, SWB has direct effects on ADL, indirect effects on LOS and the total effect is 0.256. The impact of SWB on the LOS of the patients deserves special attention from medical practitioners as the quality of life issue plays a vital role in the field of rehabilitation. It might suggest that the improvement of patients’ psychological well-being may pay off in reducing the LOS of the patients. Fourth, the gender effect on SWB is close to statistical significance. When we investigated further for this relationship, we found that male patients showed a higher variation in SWB score (21). We thought that this might indicate the transient nature of their adaptation process since they are uncertain about their prognosis and possible trajectory of the illness. We further found that Asian male patients might experience a further negative effect of the illness on rehabilita-tion outcome (21). This might be explained by the tradirehabilita-tional nature of the male role in Asian society, as the main wage earner and head of the household. In addition to above, the sexual dysfunction of male patients might contribute to the devastating factors of the outcome, which we did not include as a specific factor in the model but which may contribute to the ratings in the SWB subscale.
With the exception of the path from gender to SWB, all paths are statistically significant in the final causal model. The GFI suggest that the revised causal model fits the data well. ADL has the largest total effect on LOS. Because SWB has the second largest total effect on LOS, the impact of SWB on the LOS of the patients deserves special attention from medical practitioners. Furthermore, intervention therapy for helping patients to cope with the disease stage should be considered. The final causal model indicates that ADL, SWB and gender predict LOS for the SCI patients. The current path model offers rehabilitation professionals a careful way to design treatment plans for clients with SCI or to refer them to programs that are more appropriate. The consideration of these factors in the reimbursement system of the National Health Insurance Plan could further facilitate the achievement of rehabilitation outcomes for clients with SCI.
As Taiwan is trying to revise the reimbursement system of National Health Insurance, the results of this study offer the following possible directions: (i) they support the trend to establish function-related groups for the reimbursement system
Table V. Breakdown of the total effects
Bivariate relationship Total Direct effect Indirect effect Causal effects Non-causal effects
(Gender, SWB) 0.213 0.213 0 0.213 0 (Gender, ADL) 0.008 0 0.052 0.052 0.06 (Gender, LOS) 0.048 0 0.019 0.019 0.029 (SWB, ADL) 0.243 0.243 0 0.243 0 (SWB, LOS) 0.256 0 0.089 0.089 0.167 (ADL, LOS) 0.367 0.367 0 0.367 0
due to significant contribution of ADL in the causal model (40); (ii) the standardized regression coefficients in the model can be utilized as a basis for assessing relative weight for different predictors; and (iii) the contribution of SWB in the model suggests that payment for rehabilitation counselling for psycho-social aspects may pay off in the long term for patients with SCI. Note the 2 limitations of this study. First, patients with SCI may have problems with sexual function; however, this perspective was not investigated in detail. Second, the sample was too small to divide clients into different severity or sub-diagnostic groups so that in-depth results for subgroups were not available.
In summary, the contribution of the current study to clinical practice is the provision of scientific data of various predictors on resource use in patients with SCI, and a reminder of the influence of SWB in the proposed model. The validation of the model with different sets of patient records should be considered in future studies.
ACKNOWLEDGEMENTS
This study was supported and sponsored by the Department of Health of the Republic of China, and National Health Research Institute. Grant No. DOH86-HR-634, DOH87-HR-634, DOH88-HR-634
REFERENCES
1. Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Memorial Fund Quarterly/Health and Society 1973; 51: 95–121.
2. Andersen R, Kravits J, Andersen OW. Equity in health services: empirical analyses in social policy. Cambridge MA: Ballinger; 1975. 3. Andersen R, Aday L. Access to medical care in the US: realized and
potential. Med Care 1978; 16: 533–546.
4. Dutton DB. Explaining the low uses of health services by the poor: costs, attitudes, or delivery systems? Am Sociol Rev 1978; 43: 348– 368.
5. Dutton D. Patterns of ambulatory health care in five different delivery systems. Med Care 1979; 17: 221–241.
6. Clark F, Azen SP, Zemke R, Jackson J, Carlson M, Mandel D, et al. Occupational therapy for independent-living older adults: a randomized controlled trial. JAMA 1997; 278: 1321–1325. 7. Crewe NM, Dijkers M. Functional assessment. In: Cushman LA,
Scherer MJ, eds. Psychological assessment in medical rehabilitation. Washington DC: American Psychological Association; 1994: 101– 140.
8. Stineman MG, Williams SV. Predicting inpatient rehabilitation length of stay. Arch Phys Med Rehabil 1990; 71: 881–887. 9. Post MWM, Witte LPD, VanAsbeck FWA, Dijk AJ, Schrijvers AJP.
Predictors of health status and life satisfaction in spinal cord injury. Arch Phys Med Rehabil 1998; 78: 395–402.
10. Hampton NZ, Marshall A. Culture, gender, self-efficacy, and life satisfaction: a comparison between American and Chinese people with spinal cord injury. J Rehabil 2000; 66: 21–28.
11. Chase BW, Cornille TA, English RW. Life satisfaction among persons with spinal cord injuries. J Rehabil 2000; 66: 14–20. 12. Harada ND, Sofaer S, Kominski G. Functional status outcomes in
rehabilitation: Implications for prospective payment. Med Care 1993; 31: 345–357.
13. Heinemann AW, Linacre JM, Wright BD, Hamilton BB, Granger CV. Predication of rehabilitation outcomes with disability measures. Arch Phys Med Rehabil 1994; 75: 133–143.
14. Hosek S, Kane R, Carney M. Charges and outcomes for rehabilitative care: Implications for the prospective payment system. Santa Monica: The RAND Corporation; 1986.
15. Rondinelli RD, Murphy JR, Wilson DH, Miller CC. Predictors of functional outcome and resources utilization in inpatient rehabilita-tion. Arch Phys Med Rehabil 1991; 72: 447–453.
16. McGinnis GE, Osberg JS, Dejong G, Seward ML, Branch LG. Predicting charges for inpatient medical rehabilitation using severity, diagnostic related groups, age, and function. Am J Public Health 1987; 77: 826–829.
17. Rondinelli RD, Murphy JR, Wilson DH, Miller CC. Predictors of functional outcome and resources utilization in inpatient rehabilita-tion. Arch Phys Med Rehabil 1991; 72: 447–453.
18. Guide for the Use of the Uniform Data Set for Medical Rehabilitation (Adult FIMSM), Version 4.0. Buffalo: State Uni-versity of New York at Buffalo; 1995.
19. Formations in health care Inc. The LORS American data system (LADS): the national inpatient rehabilitation program evaluation system. Chicago Ill: Formations in Health Care Inc.; 1992. 20. Pan AW, Chung L, Huang Y, Chern J. The development of
Taiwanese rehabilitation database system. J Occup Ther Assoc R.O.C. 2000; 18: 47–58.
21. Pan AW, Chern J, Chung L, Lai J. Inter-rater and test-retest reliability of the Taiwanese rehabilitation functional scale. Occup Ther Int 2001; 8: 168–183.
22. Pan AW, Chung L, Tseng MH. Development and validation of a rehabilitation functional scale. Formos J Med 2001; 5: 389–400. 23. Pan AW. Model of rehabilitation resource use—a new approach.
Unpublished PhD dissertation, University of Illinois at Chicago; 1994.
24. LaPlante MP. The need for assistance in basic life activities. In: Thompson-Hoffman S, Storck IF., eds. Disability in the United States, New York: Springer Publishing Company; 1991: 73–106. 25. Ottenbacher KJ, Mann WC, Granger CV, Tomita M, Hurren D,
Charvat B. Inter-rater agreement and stability of functional assessment in the community-based elderly. Arch Phys Med Rehabil 1994; 75: 1297–1301.
26. Streiner DL, Norman GR. Health measurement scales: a practical guide to their development and use. New York: Oxford University Press; 1989.
27. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md Stat Med J 1965; 14: 61–65.
28. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffee MW. Studies of illness in the aged: The index of ADL: a standardized measure of biological and psychosocial function. JAMA 1963; 185: 914–919. 29. Bowling A. Measuring health: a review of quality of life
measure-ment scales. Buckingham: Open University Press; 1997.
30. Beck AT, Steer RA, Brown GK. BDI-II Manual. San Antonio TX: The Psychological Corporation; 1996.
31. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 health survey: manual and interpretation guide. Boston, MA: New England Medical Center, Health Institute; 1993.
32. Van Den Bos GAM, Triemstra AHM. Quality of life as an instrument for need assessment and outcome assessment of health care in chronic patients. Qual Health Care 1999; 8: 247–252. 33. Research team for WHOQQOL-Chinese version. Manual of WHO
questionnaire on quality of life-Chinese version. National Taiwan University, Department of Psychology, Taiwan, 1999.
34. Duncan OD. Path analysis: Sociological examples. Am J Sociol. 1996; 72: 1–16.
35. Wright S. Path coefficients and path regressions: alternative or complementary concepts? Biometrics 1960; 16: 189–202. 36. Pedhazur EJ. Multiple regression and behavioral science. Orlando
FL: Harcourt Brace Co.; 1982.
37. Subhash S. Applied multivariate techniques. New York: Springer Publishing Company; 1995.
38. SAS Institute Inc. SAS user’s guide: statistics, version 6.12 edition. Cary, NC: SAS Institute, Inc.; 1990.
39. LISREL 8. User’s Reference Guide, version 8 edition. Chicago IL: Scientific Software International, Inc.; 1996.
40. Stineman MG, Escarce JJ, Goin JE, Hamilton BB, Granger CV, Williams SV. A case mix classification system for medical rehabilitation. Med Care 1994; 32: 366–379.