Elsevier Editorial System(tm) for The American Journal of Medicine Manuscript Draft
Manuscript Number: 10-396R2
Title: Malignancy in systemic lupus erythematosus: a nationwide cohort study in Taiwan Article Type: Clinical Research Study
Keywords: malignancy; systemic lupus erythematosus; nationwide cohort study; Taiwan Corresponding Author: Dr. Chun-Ying Wu, M.D., Ph.D., M.P.H.
Corresponding Author's Institution: Taichung Veterans General Hospital First Author: Yi-Ju Chen, M.D., Ph.D.
Order of Authors: Yi-Ju Chen, M.D., Ph.D.; Yun-Ting Chang, MD, PhD; Chang-Bi Wang, MS; Chun-Ying Wu, MD, PhD
Abstract: Background: An increased risk of malignancy in patients with systemic lupus erythematosus has been reported, but rarely in Asian populations. We aimed to investigate the relative risk of cancer and to identify high risk group for cancer in lupus patients.
Methods: We conducted a retrospective, nationwide cohort study which included 11,763 lupus patients without prior history of malignancies, utilizing the national health insurance database of Taiwan from 1996 to 2007. Standardized incidence ratios (SIR) of cancers were analyzed.
Results: A total of 259 cancers among lupus patients were observed. An elevated risk of cancer among systemic lupus erythematosus was noted (SIR 1.76, 95% confidence interval [CI], 1.74-1.79), especially for hematoloigc malignancies (SIR 4.96, 95% CI, 4.79-5.14). Younger patients carried a greater risk ratio of cancer than general population and the risk ratio reduced with age. The risk ratio of cancer reduced with time, yet remained elevated than general population. The risk of non-Hodgkin's
lymphoma is greatest (SIR 7.27) among hematologic cancers. Among solid tumors, the risk for cancers of vagina/vulva (SIR 4.76), nasopharynx (SIR 4.18) and kidney (SIR 3.99) were of the greatest. An elevated risk for less common cancers including brain, oropharynx and thyroid glands were also observed.
Conclusions: Lupus patients are at increased risk of cancers and should receive age and gender appropriate malignancy evaluations, with additional assessment for vulva/vagina, kidney,
nasopharynx and hematologic malignancy. Continued vigilance for development of cancers in follow-up is recommended.
Manuscript No.: 10-396R1
Manuscript Title: Malignancy in systemic lupus erythematosus: a nationwide cohort study in Taiwan
Authors: Yi-Ju Chen, Yun-Ting Chang, Chang-Bi Wang, and Chun-Ying Wu
Dear editors and reviewers,
Thank you for offering us more time to do a better revision.
The main problem is about a question proposed by reviewer 2. He reminded us about the start date of observation in our included patients. We responded that all included patients got catastrophic illness certificate after 1997. We assumed the diagnosis date should be close to the issued date. However, when we again checked the count of included patients in each year, we found a triple number of patients at the year of 1997.We then searched for the application date of patients and we found many included subjects applied for the certificate in 1995 and 1996, especially in 1995. Since the NHIRD began in 1995, we though that many patients who were diagnosed earlier began to apply this certificate for medical fee exemption.
Therefore, we decided to exclude those applied for the certificate in 1995, since we did not accurately know how long he or she has been diagnosed with this disease. And we used the application date as the observation start date, and this would be more appropriate for our study design. Therefore, we are sure that each included patient is a newly diagnosed lupus.
The revised manuscript and table are attached and the revised part is highlighted. The major change is a decrease in number of included patients. Although this is a difficult decision, we though it is a more accurate and more appropriate revision for this study.
We are very sorry for this mistake that we should have noticed earlier.
Thanks again for your kindness to offer us this chance for further revision and we are looking forward to still having a positive response from you.
Sincerely,
Yi-Ju Chen, MD, PhD. & Chun-Ying Wu, MD, PhD.
Manuscript No.: 10-396R1
Manuscript Title: Malignancy in systemic lupus erythematosus: a nationwide cohort study in Taiwan
Authors: Yi-Ju Chen, Yun-Ting Chang, Chang-Bi Wang, and Chun-Ying Wu
Dear editors and reviewers,
Thank you for offering us more time to do a better revision.
The main problem is about a question proposed by reviewer 2. He reminded us about the start date of observation in our included patients. We responded that all included patients got catastrophic illness certificate after 1997. We assumed the diagnosis date should be close to the issued date. However, when we again checked the count of included patients in each year, we found a triple number of patients at the year of 1997.We then searched for the application date of patients and we found many included subjects applied for the certificate in 1995 and 1996, especially in 1995. Since the NHIRD began in 1995, we though that many patients who were diagnosed earlier began to apply this certificate for medical fee exemption.
Therefore, we decided to exclude those applied for the certificate in 1995, since we did not accurately know how long he or she has been diagnosed with this disease. And we used the application date as the observation start date, and this would be more appropriate for our study design. Therefore, we are sure that each included patient is a newly diagnosed lupus.
The revised manuscript and table are attached and the revised part is highlighted. The major change is a decrease in number of included patients. Although this is a difficult decision, we though it is a more accurate and more appropriate revision for this study.
We are very sorry for this mistake that we should have noticed earlier.
Thanks again for your kindness to offer us this chance for further revision and we are looking forward to still having a positive response from you.
Sincerely,
Yi-Ju Chen, MD, PhD. & Chun-Ying Wu, MD, PhD.
Malignancy in systemic lupus erythematosus: a nationwide cohort study in Taiwan
Yi-Ju Chen, M.D., Ph.D.,a,b Yun-Ting Chang, M.D., Ph.D.,b,c Chang-Bi Wang, M.S.,d,e Chun-Ying Wu, M.D., Ph.D., M.P.H.b,d,e,f
a
Department of Dermatology, Taichung Veterans General Hospital, Taichung;
b
Faculty of Medicine, National Yang-Ming University, Taipei;
c
Department of Dermatology, Taipei Veterans General Hospital, Taipei
d
Division of Gastroenterology, Department of Internal Medicine, Taichung Veterans General Hospital; Taichung
e
Department of Public Health, China Medical University, Taichung;
f
Department of Life Sciences, National Chung-Hsing University, Taichung, Taiwan
Chen YJ and Chang YT contributed equally to this manuscript
Requests for reprints should be addressed to Chun-Ying Wu, MD, PhD, Division of
Gastroenterology, Department of Internal Medicine, Taichung Veterans General Hospital,
No. 160, Sec. 3, Taichung-Kang Rd. Taichung 407, Taiwan. TEL: +886-4-23592525, ext.
3304, FAX: +886-4-22585686, E-mail: [email protected]
Funding: Grants partly from Taichung Veterans General Hospital, Taichung, Taiwan,
TCVGH-996802C
2
Authorship: All authors had access to the data and a role in writing the manuscript
Article type: Clinical Research Study
Key words: malignancy; systemic lupus erythematosus; nationwide cohort study; Taiwan
Background: An increased risk of malignancy in patients with systemic lupus
erythematosus has been reported, but rarely in Asian populations. We aimed to
investigate the relative risk of cancer and to identify high risk group for cancer in lupus
patients.
Methods: We conducted a retrospective, nationwide cohort study which included 11,763
lupus patients without prior history of malignancies, utilizing the national health
insurance database of Taiwan from 1996 to 2007. Standardized incidence ratios (SIR) of
cancers were analyzed.
Results: A total of 259 cancers among lupus patients were observed. An elevated risk of
cancer among systemic lupus erythematosus was noted (SIR 1.76, 95% confidence
interval [CI], 1.74-1.79), especially for hematoloigc malignancies (SIR 4.96, 95% CI,
4.79-5.14). Younger patients carried a greater risk ratio of cancer than general population
and the risk ratio reduced with age. The risk ratio of cancer reduced with time, yet
remained elevated than general population. The risk of non-Hodgkin’s lymphoma is
greatest (SIR 7.27) among hematologic cancers. Among solid tumors, the risk for cancers
of vagina/vulva (SIR 4.76), nasopharynx (SIR 4.18) and kidney (SIR 3.99) were of the
greatest. An elevated risk for less common cancers including brain, oropharynx and
4
Conclusions: Lupus patients are at increased risk of cancers and should receive age and
gender appropriate malignancy evaluations, with additional assessment for vulva/vagina,
kidney, nasopharynx and hematologic malignancy. Continued vigilance for development
Introduction
A common association between malignancies and autoimmune rheumatic diseases has
been observed, including systemic lupus erythematosus. 1-5 With a better management of
this disease, the survival in lupus has improved in recent decades.6 Yet the mortality and
morbidity of patients with lupus remain higher than general population, not only for
all-cause mortality but also for mortality from cancer. 6-9 Hematologic malignancies,
especially non-Hodgkin’s lymphoma were the most relevant ones in several
population-based cohorts and multicenter clinical cohort studies. 10-16 The results for solid
tumors, however, have not been as consistent. Increased risk of lung, liver, cervix, and
vagina/vulva cancer among lupus has been reported in some studies.12;14;16 To determine
the potential high risk group of patients for cancer screening is ultimate important for
long term prognosis in lupus. Our aim was to investigate the relative risk and specific
types of malignant diseases after the diagnosis of lupus, and to identify the high risk
group for cancer among lupus patients in Taiwanese population based on a nationwide
6
Method
Data sources
This study was based on data from the National Health Insurance Research Database
(NHIRD) released by the National Health Research Institute (NHRI). Taiwan began its
National Health Insurance (NHI) program in 1995 to finance health care for all of its
residents. There are currently >25 million enrollees in the program, representing approximately 99% of Taiwan’s entire population. The database comprises
comprehensive information on insured subjects, such as demographic data, dates of
clinical visits, diagnostic codes, details of prescriptions, and expenditure amounts. This
database has been the source of many epidemiological studies published in peer-reviewed
journals.17-21 International classifications of disease-9 (ICD-9) codes were used to define
diseases during the study period. Personal information including family history, lifestyle
and habits such as smoking and alcohol use was not available from the NHIRD.
Study subjects with SLE
All enrollees were obtained from the Registry of Catastrophic Illness Database, a
subpart of the NHIRD. The insured who suffer from major diseases can apply for a
applications of catastrophic illness certificates were validated by at least two specialists
based on careful examinations of medical records, laboratory and images studies. Only
those meet the diagnostic criteria of major diseases would be issued a catastrophic illness
certificate. Systemic lupus erythematosus and cancer are statutorily included in the
catastrophic illness category. Both outpatient and inpatient claims of beneficiaries with a
catastrophic illness registry are collected in the catastrophic illness profile and distributed
as a package. The prescription claims of beneficiaries are released in a different dataset
and is not included in current catastrophic illness profile.
The enrollees with SLE (ICD 9 code 710.0) were followed up between January 1,
1996 and December 31, 2005. The observation period ranges from January 1, 1996 to
December 31, 2007 to make sure each enrollee is followed up for at least 2 years.
Application of catastrophic illness certificate of SLE requires a thorough clinical and
laboratory survey which fulfills the diagnostic criteria proposed by American
Rheumatism Association in 1982.22 Patients with other autoimmune diseases such as
RA or Sjogren’s syndrome were excluded. All enrolled SLE patients with prior history
8
As the dataset used in this study consists of de-identified secondary data released to
the public for research purposes, this study was exempt from full review by the
Institutional Review Board.
Identification of cancer cases
We identified the diagnoses of cancers with the records from the Registry of
Catastrophic Illness Patient Database. To apply for a cancer catastrophic illness
certificate, cytological or pathological reports or evidence such as additional laboratory
and image studies supporting the diagnosis of cancer, including tumor marker surveys, X
ray, bone scan, computed tomography scan or magnetic resonance imaging scan, should
be provided. At least two other oncologists will examine the medical records and
laboratory information carefully including images studies. Only those meet the criteria of
diagnoses would be issued the certificates. We did not include those with in-situ
malignancies because in-situ malignant diseases do not qualify for a catastrophic illness
certificate. The diagnostic codes of malignancies were defined as those from 140 to
208.91 in the ICD-9 CM format. We categorized these cancer cases as hematologic
cancers and non-hematologic cancers. Hematologic cancers were subcategorized as
200, 202-203] and Hodgkin’s lymphoma [coded 201]), according to the method of
Cancer Registry in Taiwan.
Cancer risk analysis
All enrolled study subjects were followed up until a first time diagnosis of cancer
(except malignancy in–situ, metastasis or secondary cancers), death, the end of follow-up
in the medical records, or the end of 2007. Standardized incidence ratios (SIR) of cancers
were analyzed. Stratified analyses according to age at diagnosis, gender, and years of
follow-up were conducted.
Statistical analysis
The demographic data of the study population were first analyzed. Follow-up for
each patient with systemic lupus erythematosus began at the date of diagnosis and ended
at the date of censorship, i.e. the date of diagnosis of cancer, death or the end of
follow-up period, and was measured in numbers of years. We examined the association
among lupus and specific cancer types with SIR. SIR was calculated as follows: the
number of cancer cases that arose among lupus patients divided by the expected number
10
cancer rates. Yearly reports of cancer rates were obtained from Taiwan National Cancer
Registry. We pooled the 10-year cancer registry reports of Taiwan from 1997 to 2006 as a
standard.
To assess the age effect on the relative risk for malignancies, we analyzed the
relative risk among those aged between 0-19, 20-39, 40-59, 60-79 years, and more than
80 years at SLE diagnosis. A further analysis was done to evaluate whether the
association of malignancies varied according to the time after lupus diagnoses. We
divided follow-up time into six periods, 1 year or less, between 1 to 2 years, 2-4 years,
4-6 years, 6-8 years and more than 8 years.
The SAS statistical package (SAS System for Windows, version 9.1; SAS Institute,
Cary, North Carolina) and SPSS statistics (SPSS statistics for window, version 15.0;
SPSS Incorporation, Chicago, Illinois) were used to perform the statistical analysis of the
Results
We identified a total of 11,763 patients with systemic lupus erythematosus who did
not have previous malignancies. The demographic data of study subjects are presented in
Table 1. A total of 259 cancers (2.2%) were identified after diagnosis of lupus. An
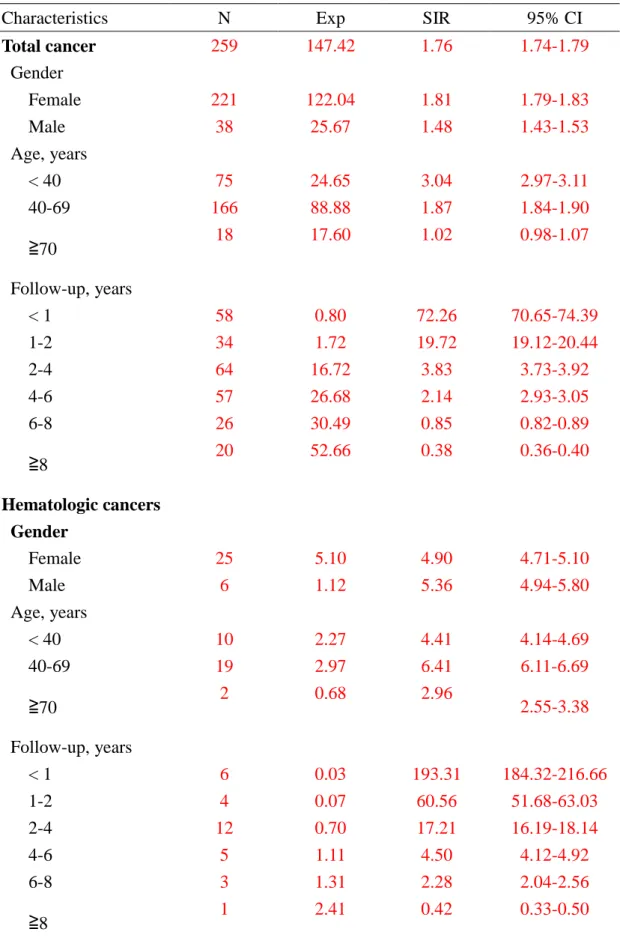
elevated overall cancer risk in lupus patients was observed (Table 2). Women had a
slightly higher risk than men. The risk ratio of cancer is greater in lupus patients younger
than 40 years when compared with subjects of similar ages in general population, and the
risk ratio reduced with age. (Table 2)
Comorbid malignant diseases in systemic lupus erythematosus were mostly detected
following the first year of diagnosis. The risk ratios gradually reduced with time. After 8
years of observation, the SIR of malignancies was even lower than general population.
(Table 2) An elevated risk for hematologic malignancies in lupus patients was observed,
especially in male patients. (Table 2) Middle-aged patients (aged 40-69 years) carried the
greatest risk ratio for hematologic cancers. (Table 2)
Of all comorbid malignant diseases, 31 cases (11.97%) were hematologic
malignancies, including 24 cases of non-Hodgkin’s lymphomas and 7 cases of leukemias.
No Hodgkin’s lymphoma was observed in our cohort. The risks for hematologic cancers
12
Among hematologic cancers, the risk for non-Hodgkin’s lymphoma (including other
lymphosarcoma, reticulosarcoma, multiple myeloma and other immunoproliferative
neoplasms) is greatest. The risk of leukemias, to a lesser extent, is also elevated. (Table 3)
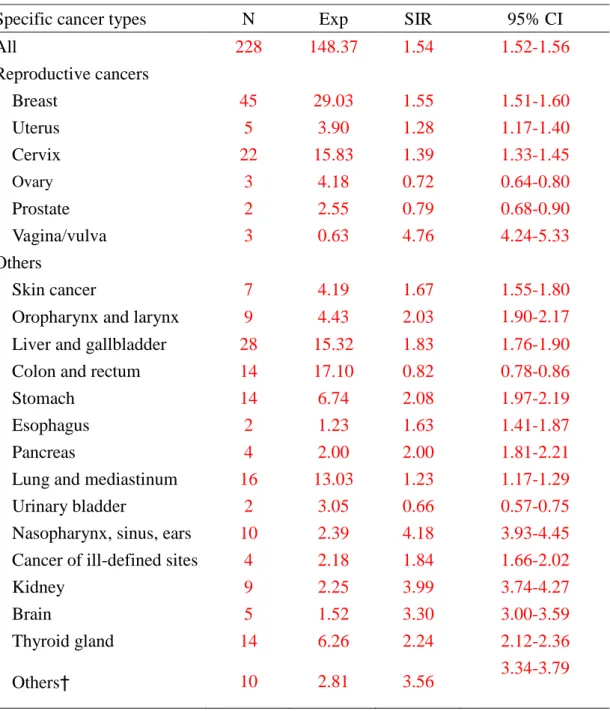
Lupus patients also carried an increased risk for non-hematologic malignancies.
(Table 4) The most relevant cancers were originating from female genitalis, such as vulva
and vagina and cervix. A decreased risk of prostate and ovary cancer was observed
compared to general population. (Table 4)
Other associated cancers were presented in Table 4, including cancers of kidney,
Discussion
It has been accepted nowadays that systemic lupus erythematosus is at increased risk
of certain cancers. Different cohort studies produced various estimates of the cancer risk
of lupus patients; however, the risk of specific cancer types was inconclusive. 16;23-27 Most
cancer cases in our cohort were detected within the first 2 years after diagnosis.
Aggressive surveillance for cancer during that period may have resulted in a detection
bias. When cancer cases observed in the first 2 years were excluded, a sustained elevated
risk existed among lupus patients until 8 years of follow-ups, indicating a true link
between these two diseases.
The underlying mechanisms linking malignancies and lupus remained unclear. There
is no clear explanation regarding the inflammatory nature of lupus or the
immunosuppressive treatment in association with malignancies. Bernatsky et al., has
firstly explored the relationship between cancer and exposures of medication and other
risk factors in lupus patients.28 Their study indicated older age, disease activity and
tobacco exposure were associated with an increased cancer risk in systemic lupus
erythematosus. The relationship between immunosuppressive drugs and cancers may
vary considerably with different type of cancers. For example, increased cancer rates
14
linked to treatment with drugs including cyclophosphamide, azathioprine, and
methotrexate in some reports. 29-32 An increased risk of hematologic malignancies was
observed after at least 5 years of immunosuppressice drug exposure.28 However, a recent
nested case control study focusing on the association between non-Hodgkin’s lymphoma
and lupus indicated that it is the hematologic aberrations (leuco-/thrombocytopenia, or
hematoloigc anemia), sicca symptoms, or recurrent pneumonias predict the prognosis
among lupus patients. It also indicated that use of azathioprine and cyclophosphamide did
not increase the risk of non-Hodgkin’s lymphoma. 33 Several case series have indicated
an increased risk of bladder cancer among lupus patients because of the treatment with
cyclophosphamide. 29-32 We were not able to examine this association since we did not
have treatment information on these patients. Nevertheless, the finding of a gradual
reduction of cancer risk ratios during observation in our lupus patients implied that
cancer risk is not completely explained by cumulative toxicity of immunosuppressive
drugs.
The finding of younger lupus patients bearing greater risk ratio of cancer has not
been reported until recently. 34 Our study is the first regarding the age effect and cancer
risk of lupus patients in Asian populations. Since malignant diseases generally increase
cancer cases among aged patients makes the difference in incidence non-significant
between elderly lupus patients and elderly subjects from the general population. The
relationship between severity of lupus and malignant diseases may be another plausible
explanation. Previous reports have indicated that the majority of severe cases of systemic
lupus erythematosus occur in younger women, particularly women other than
non-Hispanic whites. 35 In addition, younger patients with severe disease may be treated
with more aggressively with immunosuppressive agents, which may also lead to an
increased risk of cancer.
Increased mortality risk due to cancer in lupus, especially non-Hodgkin’s lymphoma
and lung cancer, has been demonstrated.7 A poorer prognosis in lupus patients
complicated with non-Hodgkin’s lymphoma has been reported.36 However, it is unknown
if this is related to more aggressive histological subtypes on diagnosis,13;14 delayed cancer
diagnosis, or others.
Most of the data from previous cohort studies suggested a three to fourfold risk of
hematologic malignancies, especially non-Hodgkin’s lymphoma in lupus than general
population. 8;12 Comparable to previous studies, our results demonstrated an even higher
risk of non-Hodgkin’s lymphoma (SIR 7.27) and to a lesser extent, leukemia (SIR 2.64)
16
have indicated an increased proportion of the aggressive diffuse large B cell
lymphomas.12;37;38 The risk of large B cell lymphoma among lupus was also significantly
elevated than general population.34 We did not subcategorize our non-Hodgkin’s
lymphoma patients by subtypes because standardized cancer estimates by specific
lymphoma subtypes in Taiwan were not available.
A common association of hematologic malignancies, especially non-Hodgkin’s
lymphoma, in patients with autoimmune diseases has been observed for decades. Shared
eiopathogeneic factors and genetic predisposition commonly in both autoimmune
diseases and lymphomas included uncontrolled B cell proliferation,39 defected
apoptosis,40 oncogene translocation36 and aberrant Epstein-Barr virus expression41.
Chronic lymphocyte activation related to autoimmune diseases has been proposed to be a
possible underlying mechanism.6;37;42-44
An increased risk of various solid tumors was observed in our lupus patients. In
addition to commonly reported lung and hepatobiliary cancers, an elevated risk for
certain rare cancers was observed, such as kidney (SIR 3.99), nasopharynx, sinus or ears
(SIR 4.28), brain (SIR 3.30) and thyroid (SIR 2.24) in lupus patients. The findings of
increased risks of these rarer cancers highlighted the power of our present study to detect
An elevated risk of vagina/vulva (SIR 4.76) and cervix cancers (SIR 1.39) was
observed in our lupus patients. Only few studies have mentioned about the high
prevalence of vagina/vulva cancer in lupus patients.14;34 An increased prevalence of
human papillomavirus in women with lupus may be a possible explanation for the
elevated risk of these two cancer types. 45;46 A decreased risk of some hormone-sensitive
malignancies such as breast and endometrial cancers was described in some cohort
study;12;34 on the contrary, except for the cancers of prostate and ovary, we demonstrated
an elevated risk of breast and uterus cancers.
There are several limitations in our present study. First, we did not have personal
information of patients, such as life style, body mass index, smoking and alcohol use,
family history of malignancy, or the information of systemic treatment which may
contribute to cancer risk. Second, misclassification of diseases may happen based on
administrative database of NHIRD in Taiwan. To minimize the possible bias, we enrolled
the patients from the catastrophic illness profile in which only those with definite
diagnoses would be included. Finally, most lupus patients undergo regular physical and
laboratory check-ups for many years. A surveillance bias may contribute to some of the
increased frequency of cancer in these patients.
18
nationwide cohort study of cancer and lupus conducted in Asian population. Younger
lupus patients are at greatest risk to develop certain cancers when compared with that in
general population. In addition to a high prevalence of hematologic cancers especially
non-Hodgkin’s lymphoma, an increased risk of several less common cancers, such as
vagina/vulva, kidney, nasopharynx, urinary bladder, brain and thyroid gland were also
observed. We therefore suggest a thorough history taking, physical and laboratory
examinations for these rare cancers in all lupus patients. Although most cancers were
detected within the early course of observation, we suggest a continuous cancer screening
Acknowledgement
This study is based in part on data from the National Health Insurance Research Database
provided by the Bureau of National Health Insurance, Department of Health and
managed by the National Health Research Institute. The interpretation and conclusions
contained herein do not represent those of the Bureau of National Health Insurance,
20
Reference List
(1) Racanelli V, Prete M, Minoia C, Favoino E, Perosa F. Rheumatic disorders as paraneoplastic syndromes. Autoimmun Rev 2008;7:352-358.
(2) Varoczy L, Gergely L, Zeher M, Szegedi G, Illes A. Malignant
lymphoma-associated autoimmune diseases--a descriptive epidemiological study. Rheumatol Int 2002;22:233-237.
(3) Zintzaras E, Voulgarelis M, Moutsopoulos HM. The risk of lymphoma development in autoimmune diseases: a meta-analysis. Arch Intern Med 2005;165:2337-2344.
(4) Bernatsky S, Boivin JF, Joseph L et al. Race/ethnicity and cancer occurrence in systemic lupus erythematosus. Arthritis Rheum 2005;53:781-784.
(5) Bernatsky S, Ramsey-Goldman R, Clarke A. Malignancy and autoimmunity. Curr Opin Rheumatol 2006;18:129-134.
(6) Moss KE, Ioannou Y, Sultan SM, Haq I, Isenberg DA. Outcome of a cohort of 300 patients with systemic lupus erythematosus attending a dedicated clinic for over two decades. Ann Rheum Dis 2002;61:409-413.
(7) Bernatsky S, Boivin JF, Joseph L et al. Mortality in systemic lupus erythematosus. Arthritis Rheum 2006;54:2550-2557.
(8) Tarr T, Gyorfy B, Szekanecz E et al. Occurrence of malignancies in Hungarian patients with systemic lupus erythematosus: results from a single center. Ann N Y Acad Sci 2007;1108:76-82.
(9) Nossent J, Cikes N, Kiss E et al. Current causes of death in systemic lupus erythematosus in Europe, 2000--2004: relation to disease activity and damage accrual. Lupus 2007;16:309-317.
(10) Ragnarsson O, Grondal G, Steinsson K. Risk of malignancy in an unselected cohort of Icelandic patients with systemic lupus erythematosus. Lupus 2003;12:687-691.
incidence in a Swedish cohort of patients with systemic lupus erythematosus. Scand J Rheumatol 2002;31:66-71.
(12) Bernatsky S, Boivin JF, Joseph L et al. An international cohort study of cancer in systemic lupus erythematosus. Arthritis Rheum 2005;52:1481-1490.
(13) Pettersson T, Pukkala E, Teppo L, Friman C. Increased risk of cancer in patients with systemic lupus erythematosus. Ann Rheum Dis 1992;51:437-439.
(14) Mellemkjaer L, Andersen V, Linet MS, Gridley G, Hoover R, Olsen JH. Non-Hodgkin's lymphoma and other cancers among a cohort of patients with systemic lupus erythematosus. Arthritis Rheum 1997;40:761-768.
(15) Abu-Shakra M, Gladman DD, Urowitz MB. Malignancy in systemic lupus erythematosus. Arthritis Rheum 1996;39:1050-1054.
(16) Cibere J, Sibley J, Haga M. Systemic lupus erythematosus and the risk of malignancy. Lupus 2001;10:394-400.
(17) Wu CY, Wu MS, Kuo KN, Wang CB, Chen YJ, Lin JT. Effective reduction of gastric cancer risk with regular use of nonsteroidal anti-inflammatory drugs in Helicobacter pylori-infected patients. J Clin Oncol 2010;28:2952-2957.
(18) Wu CY, Kuo KN, Wu MS, Chen YJ, Wang CB, Lin JT. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology 2009;137:1641-1648.
(19) Huang YL, Chen YJ, Lin MW et al. Malignancies associated with
dermatomyositis and polymyositis in Taiwan: a nationwide population-based study. Br J Dermatol 2009.
(20) Chang YT, Chen TJ, Liu PC et al. Epidemiological study of psoriasis in the national health insurance database in Taiwan. Acta Derm Venereol
2009;89:262-266.
(21) Chen YJ, Wu CY, Huang YL, Wang CB, Shen JL, Chang YT. Cancer risks of dermatomyositis and polymyositis: a nationwide cohort study in Taiwan. Arthritis Res Ther 2010;12:R70.
22
(22) Tan EM, Cohen AS, Fries JF et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1982;25:1271-1277.
(23) Ramsey-Goldman R, Clarke AE. Double trouble: are lupus and malignancy associated? Lupus 2001;10:388-391.
(24) Ramsey-Goldman R, Mattai SA, Schilling E et al. Increased risk of malignancy in patients with systemic lupus erythematosus. J Investig Med 1998;46:217-222. (25) Sweeney DM, Manzi S, Janosky J et al. Risk of malignancy in women with
systemic lupus erythematosus. J Rheumatol 1995;22:1478-1482.
(26) Abu-Shakra M, Gladman DD, Urowitz MB. Malignancy in systemic lupus erythematosus. Arthritis Rheum 1996;39:1050-1054.
(27) Nived O, Bengtsson A, Jonsen A, Sturfelt G, Olsson H. Malignancies during follow-up in an epidemiologically defined systemic lupus erythematosus inception cohort in southern Sweden. Lupus 2001;10:500-504.
(28) Bernatsky S, Joseph L, Boivin JF et al. The relationship between cancer and medication exposures in systemic lupus erythaematosus: a case-cohort study. Ann Rheum Dis 2008;67:74-79.
(29) Gibbons RB, Westerman E. Acute nonlymphocytic leukemia following short-term, intermittent, intravenous cyclophosphamide treatment of lupus nephritis. Arthritis Rheum 1988;31:1552-1554.
(30) Lishner M, Hawker G, Amato D. Chronic lymphocytic leukemia in a patient with systemic lupus erythematosus. Acta Haematol 1990;84:38-39.
(31) Meyerson HJ, Farhi DC, Rosenthal NS. Transient increase in blasts mimicking acute leukemia and progressing myelodysplasia in patients receiving growth factor. Am J Clin Pathol 1998;109:675-681.
(32) Vasquez S, Kavanaugh AF, Schneider NR, Wacholtz MC, Lipsky PE. Acute nonlymphocytic leukemia after treatment of systemic lupus erythematosus with immunosuppressive agents. J Rheumatol 1992;19:1625-1627.
non-Hodgkin's lymphoma cases in a national Swedish systemic lupus erythematosus cohort: a nested case-control study. Ann Rheum Dis 2007;66:1627-1632.
(34) Parikh-Patel A, White RH, Allen M, Cress R. Cancer risk in a cohort of patients with systemic lupus erythematosus (SLE) in California. Cancer Causes Control 2008;19:887-894.
(35) Alarcon GS, Calvo-Alen J, McGwin G, Jr. et al. Systemic lupus erythematosus in a multiethnic cohort: LUMINA XXXV. Predictive factors of high disease activity over time. Ann Rheum Dis 2006;65:1168-1174.
(36) Bernatsky S, Ramsey-Goldman R, Rajan R et al. Non-Hodgkin's lymphoma in systemic lupus erythematosus. Ann Rheum Dis 2005;64:1507-1509.
(37) Smedby KE, Hjalgrim H, Askling J et al. Autoimmune and chronic inflammatory disorders and risk of non-Hodgkin lymphoma by subtype. J Natl Cancer Inst 2006;98:51-60.
(38) Lofstrom B, Backlin C, Sundstrom C, Ekbom A, Lundberg IE. A closer look at non-Hodgkin's lymphoma cases in a national Swedish systemic lupus
erythematosus cohort: a nested case-control study. Ann Rheum Dis 2007;66:1627-1632.
(39) Efremidis A, Eiser AR, Grishman E, Rosenberg V. Hodgkin's lymphoma in an adolescent with systemic lupus erythematosus. Cancer 1984;53:142-146. (40) Xu Y, Wiernik PH. Systemic lupus erythematosus and B-cell hematologic
neoplasm. Lupus 2001;10:841-850.
(41) Poole BD, Templeton AK, Guthridge JM, Brown EJ, Harley JB, James JA. Aberrant Epstein-Barr viral infection in systemic lupus erythematosus. Autoimmun Rev 2009;8:337-342.
(42) Chow WH, Gridley G, Mellemkjaer L, McLaughlin JK, Olsen JH, Fraumeni JF, Jr. Cancer risk following polymyositis and dermatomyositis: a nationwide cohort study in Denmark. Cancer Causes Control 1995;6:9-13.
24
immune-modulating medications as risk factors for non-Hodgkin's lymphoma: a case-control study. Am J Epidemiol 2005;162:1153-1161.
(44) Zintzaras E, Voulgarelis M, Moutsopoulos HM. The risk of lymphoma development in autoimmune diseases: a meta-analysis. Arch Intern Med 2005;165:2337-2344.
(45) Tam LS, Chan AY, Chan PK, Chang AR, Li EK. Increased prevalence of squamous intraepithelial lesions in systemic lupus erythematosus: association with human papillomavirus infection. Arthritis Rheum 2004;50:3619-3625. (46) Nath R, Mant C, Luxton J et al. High risk of human papillomavirus type 16 infections and of development of cervical squamous intraepithelial lesions in systemic lupus erythematosus patients. Arthritis Rheum 2007;57:619-625.
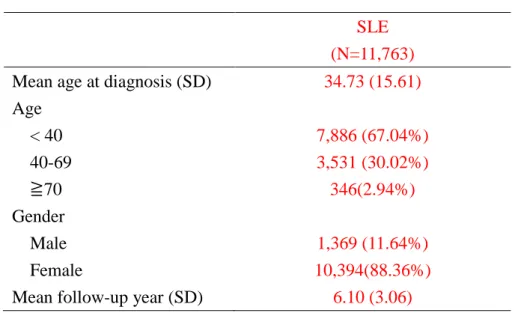
Table 1. Demographic data of SLE patients
SLE (N=11,763) Mean age at diagnosis (SD) 34.73 (15.61) Age < 40 7,886 (67.04%) 40-69 3,531 (30.02%) ≧70 346(2.94%) Gender Male 1,369 (11.64%) Female 10,394(88.36%)
Mean follow-up year (SD) 6.10 (3.06)
Table 2. Standardized incidence ratios (SIRs) and 95% confidence intervals (95% CIs) of cancers, according to age, gender, duration of follow-ups in SLE.
Characteristics N Exp SIR 95% CI
Total cancer 259 147.42 1.76 1.74-1.79 Gender Female 221 122.04 1.81 1.79-1.83 Male 38 25.67 1.48 1.43-1.53 Age, years < 40 75 24.65 3.04 2.97-3.11 40-69 166 88.88 1.87 1.84-1.90 ≧70 18 17.60 1.02 0.98-1.07 Follow-up, years < 1 58 0.80 72.26 70.65-74.39 1-2 34 1.72 19.72 19.12-20.44 2-4 64 16.72 3.83 3.73-3.92 4-6 57 26.68 2.14 2.93-3.05 6-8 26 30.49 0.85 0.82-0.89 ≧8 20 52.66 0.38 0.36-0.40 Hematologic cancers Gender Female 25 5.10 4.90 4.71-5.10 Male 6 1.12 5.36 4.94-5.80 Age, years < 40 10 2.27 4.41 4.14-4.69 40-69 19 2.97 6.41 6.11-6.69 ≧70 2 0.68 2.96 2.55-3.38 Follow-up, years < 1 6 0.03 193.31 184.32-216.66 1-2 4 0.07 60.56 51.68-63.03 2-4 12 0.70 17.21 16.19-18.14 4-6 5 1.11 4.50 4.12-4.92 6-8 3 1.31 2.28 2.04-2.56 ≧8 1 2.41 0.42 0.33-0.50
Table 3. SIR of hematopoietic malignancies in SLE in Taiwan
Cancer types N Exp SIR 95% CI
All 31 6.25 4.96 4.79-5.14
Leukemia 7 2.65 2.64 2.45-2.84
Hodgkin’s lymphoma 0 - - -
Non-Hodgkin’s lymphoma
and others* 24 3.30 7.27 6.98-7.57
N, observed number; Exp, expected number; SIR, standardized incidence ratio; CI, confidence interval.
*Others include lymphosarcoma, reticulosarcoma, multiple myeloma and other immunoproliferative neoplasms.
Table 4. SIRs of non-hematologic malignancies and specific cancer types in systemic lupus erythematosus (SLE) in Taiwan
N, observed number; Exp, expected number; SIR, standardized incidence ratio; CI, confidence interval.
†Other tumors include malignancies of salivary glands, intestine, retroperitoneum, bone, cartilage, and connective tissue.
Specific cancer types N Exp SIR 95% CI
All 228 148.37 1.54 1.52-1.56 Reproductive cancers Breast 45 29.03 1.55 1.51-1.60 Uterus 5 3.90 1.28 1.17-1.40 Cervix 22 15.83 1.39 1.33-1.45 Ovary 3 4.18 0.72 0.64-0.80 Prostate 2 2.55 0.79 0.68-0.90 Vagina/vulva 3 0.63 4.76 4.24-5.33 Others Skin cancer 7 4.19 1.67 1.55-1.80
Oropharynx and larynx 9 4.43 2.03 1.90-2.17
Liver and gallbladder 28 15.32 1.83 1.76-1.90
Colon and rectum 14 17.10 0.82 0.78-0.86
Stomach 14 6.74 2.08 1.97-2.19
Esophagus 2 1.23 1.63 1.41-1.87
Pancreas 4 2.00 2.00 1.81-2.21
Lung and mediastinum 16 13.03 1.23 1.17-1.29
Urinary bladder 2 3.05 0.66 0.57-0.75
Nasopharynx, sinus, ears 10 2.39 4.18 3.93-4.45
Cancer of ill-defined sites 4 2.18 1.84 1.66-2.02
Kidney 9 2.25 3.99 3.74-4.27
Brain 5 1.52 3.30 3.00-3.59
Thyroid gland 14 6.26 2.24 2.12-2.36
Clinical significance
1. Systemic lupus erythematosus carries an elevated risk of various cancers,
especially non-Hodgkin’s lymphoma, cancers of vagina/vulva, nasopharynx and
kidney.
2. The risk ratio of cancer in systemic lupus erythematosus was greatest among
those younger than 40 years old; and the risk ratio decreased with age.
3. The risk ratio of cancer in systemic lupus erythematosus was greatest within the
first year after diagnosis, and remained elevated than general population until 8
years of observation.