Title
A higher incidence rate of acute coronary syndrome following radiation therapy in patients with breast cancer and a history of coronary artery diseases
Names of each author's name and affiliation
Yen-Chien Lee1, Jen-Pin Chuang2, Pi-Ching Hsieh3,Meng-Jiun Chiou4, Chung-Yi Li5,6
1. Department of Oncology, Tainan Hospital, Ministry of Health and Welfare, Tainan, Taiwan, ROC.
2. Department of Surgery, Tainan Hospital, Ministry of Health and Welfare, Tainan, Taiwan, ROC.
3. Department of Health Care Management, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan, ROC.
4. Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan, ROC.
5. Chuang-Yi Li. Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan, ROC. / Department of Public Health, College of Public Health, China Medical University, Taichung, Taiwan, ROC.
Name, address, telephone and fax numbers, and e-mail address of the corresponding author.
Correspondence to: Chung-Yi Li, Ph.D. #1, University Road, Tainan 70101, TAIWAN
TEL: 886-6-2353535 ext.5862, 5863 FAX: 886-6-2359033 E-mail: [email protected]
Word count for the text: 2,710 words. Word count for the abstract: 236 words. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
Abstract
Purpose: This study aims to investigate whether patients with breast cancer and a
history of cardiovascular diseases (CADs) are at an increased incidence of acute coronary syndrome (ACS) after receiving radiation therapy (RT).
Methods: In Taiwan, 5,828 patients who had a history of CAD were newly diagnosed
of breast cancer and received mastectomy between 1999 and 2009. Among these patients, 1,851 also received RT. The study cohort was prospectively followed to the end of 2010 for estimating the incidence of ACS in association with exposure to RT. A Cox proportional hazard model that was adjusted for covariates was used to estimate the hazard ratio (HR) of ACS.
Results: Over the study period, the incident rates of ACS for RT and control patients
were estimated at 1.51 and 1.77 per 100 person-years, respectively. Covariate adjusted regression analysis indicated that the hazard of ACS significantly increased in RT patients at an adjusted HR of 1.48 [95% confidence interval (CI): 1.18–1.87] . Both hypertension and diabetes significantly increased the hazard of ACS in this patient cohort, with adjusted HRs of 3.31 [95% CI: 1.94-5.66] and 1.50 [95% CI: 1.19-1.89], respectively. 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52
Conclusions: This 12-year follow-up study suggested excess of ACS events in
association with RT exposure in patients with breast cancer who had a higher cardiovascular risk. In consideration of the benefit associated with RT, intensive cardiac care should be given to patients with breast cancer and high cardiovascular risk.
Keywords: Breast cancer, Radiation therapy, Acute coronary syndrome, Cardiovascular disease 53 54 55 56 57 58 59 60
Introduction
Breast cancer is the most common type and the leading cause of cancer death among females, accounting for 23% of the total cancer cases and 14% of the total cancer deaths [1]. Radiation therapy (RT) is one of the standard treatments after breast-conserving surgery or total mastectomy with lymph node metastasis [2]. Previous reports have shown that RT after mastectomy or breast conserving surgery reduces two thirds of local recurrence and improves overall survival by 5%–10% [3,4]. However, RT of mediastinal tumors such as lymphoma and seminoma is associated with an elevated risk of cardiac mortality [5,6]. Long-term survivors of Hodgkin’s lymphoma and childhood cancers have twofold to more than sevenfold increased risk for late cardiac deaths after total tumor doses of 30–40 Gy, given in 2 Gy fractions, where a large volume of the heart is included in the irradiated field [7]. In addition, radiation exposure of the heart to an average equivalent single dose of approximately 2 Gy significantly increases the risk of developing ischemic heart disease 10 or more years after irradiation [8], and the risk is progressive [9,10]. Women irradiated for breast cancer were also observed to have increased cardiac mortality [7,11,12], but such observation was not replicated in other studies [13,14].
Some studies reported that excess cardiovascular morbidity and mortality are only 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78
associated with left breast irradiation [15,16], whereas others reported no such difference [13,17-19]. In addition, previous studies reported that inner-quadrant tumors with RT had higher risk of cardiovascular mortality than outer-quadrant tumors after irradiation [17]. Several reviews have investigated the relationship between RT associated with breast cancer and cardiovascular mortality, but the results remain inconclusive [2,20-22].
In this study, we aimed to investigate whether RT is associated with a higher incidence of acute coronary syndrome (ACS) in patients with breast cancer and a history of coronary artery disease (CAD). These patients are essentially a subgroup with higher cardiovascular risk. To the best of our knowledge, the risk of ACS in this high-risk segment of patients with breast cancer has never been investigated.
79 80 81 82 83 84 85 86 87 88 89 90
Patients and Methods
Data Sources
The data analyzed in this study were retrospectively retrieved from the claims of the National Health Insurance Research Database (NHIRD) provided by the National Health Insurance Administration (NHIA), Ministry of Health and Welfare of Taiwan. The NHIRD provided all inpatient and ambulatory medical claims for around 99% of Taiwanese people [23]. The NHIRD covered all inpatient and outpatient claims and medical orders, as well as the information on health care providers, including medical institutions and health care workers. The identification numbers of all health care providers are encrypted to ensure privacy. To ensure the accuracy of claim files, the NHIA performs expert reviews quarterly on a random sample for every 50 to 100 ambulatory and inpatient claims [24]. In Taiwan, the NHIA issues major illness/injury certificates to all patients who suffer from malignant neoplasm, and these patients are exempt from copayment to the NHI if they are admitted for the illness associated with the related malignancy. A major illness/injury certificate can be issued only when the cancer diagnosis is pathologically confirmed. To ensure the accuracy of the diagnosis of malignant neoplasm, we enrolled only those patients with breast cancer by using major illness/injury certificates for the particular admissions or ambulatory cares. 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108
Access to research data has been granted by the Review Committee of the National Health Research Institutes. The research protocol has also obtained the IRB approval from Taipei City Hospital (TCHIRB-1020408-E).
Study cohort
On the basis of the NHIRD report, a total of 84,657 patients with breast cancer were newly diagnosed (as per the International Classification of Disease, 9th
Revision, Clinical Modification, ICD-9-CM code 174.0 to 174.9) between January 1, 1999 and December 31, 2010.We searched the medical claims of all breast cancer patients between 1997 and 2010 to identify those who had a history of coronary artery disease (CAD) ( ICD-9-CM code: 410.XX to 414.XX or ICD-9-CM procedure codes: 36.00-36.06 and 36.10-36.19) prior to breast cancer diagnosis. Breast cancer patients who had specific diagnostic codes of ACS including angina (413.9), acute myocardial infarction (AMI) (410.XX), and intermediate syndrome (411.1) or ACS-related procedures, including coronary artery bypass graft, stent insertion, or percutaneous coronary intervention were excluded, resulting in 6,484 p atients with first-ever breast cancer diagnosis and had a history of CAD (excluding ACS) included in the study cohort. Exclusion of patients with prior specific diagnosis of ACS was to ensure that any ACS diagnosed after RT was an incident event. We further excluded 875 patients 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 126
who received no breast surgery and 327 patients who underwent RT (medical order codes: 36011B, 36012B, 36012BA, 36012BB, and 36012BC) at >1 year after breast cancer diagnosis. Finally, 5,282 patients were left in the analysis. Among the study patients, 1,851 had received RT within 1 year after breast surgery (RT group), and 3,431 received no RT. Finally, 5,282 patients were left in the analysis. Among the study patients, 1,851 had received RT within 1 year after breast surgery (RT group), and 3,431 received no RT (control group).
Follow-up and ascertainment of ACS events
All study participants were followed from the date of breast cancer diagnosis to the date of the following 3 events whichever came first, i.e., incidence of ACS, death, and end-of-follow-up (i.e., December 31, 2010).The occurrence of ACS was determined by a discharge diagnosis of unstable angina (ICD-9 CM code: 413.9), acute
myocardial infarction (AMI) (ICD-9 CM code, 410.XX), intermediate syndrome (ICD-9 CM code: 411.1), or ACS-related procedures, including coronary artery bypass graft, stent insertion, or percutaneous coronary intervention [25]. The ACS-related procedures were determined by the following ICD-9-CM procedure codes: coronary artery intervention (360.0 to 363.9), percutaneous coronary dilatation (one vessel: 33076B, two vessels: 33077B, and three vessels: 33078B) and implantation of 127 128 129 130 131 132 133 134 135 136 137 138 139 140 141 142 143 144
heart assist system (376.0 to 376.7).
Statistical Analysis
We first compared the characteristics between RT and non-RT groups. A Cox proportional hazard model with adjustment for covariates was conducted to assess the independent effect of RT on the incidence of ACS. In the regression model, the follow-up period was calculated as the time interval between date of breast cancer diagnosis to the date of the following 3 events whichever came first, i.e., incidence of ACS, death, and end-of-follow-up (i.e., December 31, 2010). The assumption of proportionality for the Cox model was graphically examined and verified. We also constructed a life table that demonstrates the ACS-free survival rates for each of the two study groups.
The covariates considered in the multiple regression model included age, sex, and co-morbidities known to pose risk to cardiovascular disease, including
hypertension (ICD-9-CM codes: 401.0 to 405.99), diabetes (ICD-9-CM codes: 250.xx), and hyperlipidemia (ICD-9-CM codes: 272.xx). The analyses were
performed with SAS (ver. 9.3, The SAS Institute, Cary, NC.), and a two-side p< 0.05 was considered statistically significant.
145 146 147 148 149 150 151 152 153 154 155 156 157 158 159 160 161
Results
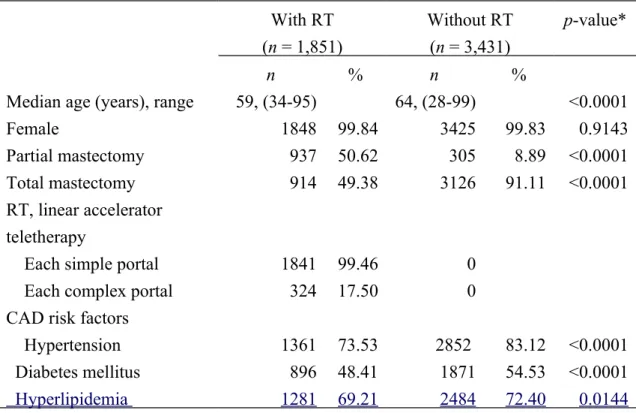
The characteristics of patients are shown in Table 1. There were 1,851 patients had received radiation therapy within 1 year after breast cancer diagnosis. None of them had ever received radiation therapy before breast cancer diagnosis and 288 out of 1,851 patients had received radiation therapy in one year after breast cancer diagnosis as well. The RT group comprised patients who were younger and had a lower percentage of total mastectomy than the non-RT group. The percentages of hypertension, diabetes, and h yperlipidemia were also lower in the RT group than in the non-RT group.
After a maximum of 12 years of follow-up, 110 patients with RT and 266 patients without RT experienced ACS events, with an incidence rate of 1.51 and 1.77 per 100 person-years, respectively (Table 2). The cumulative ACS-free rate for the RT group was estimated at 0.6528 after the follow-up period. The corresponding figure for the non-RT group was lower, at 0.6160 (Table 3).
The multiple regression indicated that the patients with RT were significantly associated with an increased hazard of ACS, with an adjusted HR of 1.48 (95% confidence interval (CI): 1.18–1.87). It also indicated that both hypertension and diabetes were associated with significantly increased hazards of ACS events, with an 162 163 164 165 166 167 168 169 170 171 172 173 174 175 176 177 178 179
adjusted HR of 3.31 (95% CI: 1.94–5.66) and 1.50 (95% CI: 1.19–1.89), respectively. (Table 2) We also noted that approximately 25% (305 out of 1242 patients) of patients did not receive RT after partial mastectomy.
180 181 182
Discussion
This cohort study demonstrated that patients with breast cancer and a history of CAD had a 1.49-fold higher incidence of ACS after RT. Such increased incidence was independent of patient age and co-morbid diabetes, hypertension, and
hyperlipidemia. Older age, diabetes, and hypertension were also associated with increased incidence of ACS in breast cancer survivors. Diabetes was associated with 1.52 higher incidence of ACS, which is similar to previous Framingham Heart Study results [26]. These findings suggested that RT may pose equal contribution as
diabetes to the incidence of ACS in patients with breast cancer and a CAD history, which warrants careful administration of RT.
Several previous studies showed that radiation may increase cardiovascular morbidity and mortality [11,12,16,27]. Clarke et al. [3] conducted a meta-analysis of randomized trials that assessed the effects of RT in patients with early-stage breast cancer on local cancer recurrence and 15-year survival; they reported 1.27 excess mortality of heart disease from radiation exposure and 4.4% increase in overall survival. In addition, Cuzick et al. [28] found an excess risk of CAD associated with exposure of left breast to radiation. Paszat et al. [29] also reported a significantly higher risk of AMI associated with RT to the left breast, with an HR of 1.96 among 184 185 186 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201
patients aged ≥60 years. The strengths of the study by Paszat et al. included
adjustment for history of smoking and knowledge of anterior internal mammary node radiation status. Although we were unable to account for the role of smoking in our analysis, the prevalence of smoking among women in Taiwan is considered low (<5%) [30].
Darby et al. reported that the risk of ischemic heart disease increases within the first 5 years after RT for women with breast cancer and that the risk persists into the third decade after RT [16]. Our study showed similar results where the ACS event rate dramatically increased from 1.1 per 1,000 person-years in the first 2 years after RT to 18.8 and 47.0 per 1,000 person-years in 2 to 4 years and 4 to 6 years after RT, respectively.
Despite the above similarities, our results contradict with findings from several previous studies. Darby et al. [31] analyzed the SEER data and reported excess mortality of AMI and other ischemic heart disease associated with exposure to radiation on the left-sided breast tumor during 1973 to 1982, but no such findings were obtained after 1983. They reported that the standardized cardiac mortality ratio after RT for early breast cancer decreased from 1.20 in 1983 to 0.96 in 2001 [31]. Vallis et al. [13] also compared the potential cardiovascular effect from radiation 202 203 204 205 206 207 208 209 210 211 212 213 214 215 216 217 218 219
exposure between left-sided versus right-sided breast cancer. They concluded no evidence for excess AMI after RT at 10.2 years of follow-up. Comparison of study findings between our study and previous ones is difficult because of dissimilarity in eligibility of study patients. Previous studies focused on various types of heart
diseases, such as diseases of pulmonary circulation and acute rheumatic fever, before breast cancer diagnosis [3]. The present study primarily focused on the history of CAD in patients with breast cancer. Besides, most previous studies assessed the risk of heart disease from exposure to RT in general patients with breast cancer
[3,10,12,13,23,27,29]. The present study focused on a subgroup of breast cancer patients who are believed to be at a greater risk of ACS. This subgroup of patients was frequently encountered during daily clinic practices because of the high
prevalence of CAD [32], and concern over these patients is of particular imperative.
We unexpectedly found that approximately 25% (305 out of 1,242 patients) of patients with breast cancer did not receive RT after partial mastectomy. Breast cancer surgery followed by RT decreases local recurrence by a magnitude from 39.2% to 14.3% after a 20 year follow-up period as compared with operation alone [33] and is now considered to be a standard therapy. Tuttle et al. [34] reported that omission of RT significantly increases from 1992 (15.5%) to 2007 (25.0%); RT has also been associated with increased disease-free and overall survivals. The reason for not 220 221 222 223 224 225 226 227 228 229 230 231 232 233 234 235 236 237 238
receiving RT for such a large number of patients remains unknown. One possible reason might be the fear of patients from being at a higher risk of cardiovascular disease. Our study suggests an excess incidence of ACS in breast cancer patients with a CAD history, which could compromise, at least to some extent, the benefit of RT after breast cancer surgery.
Mediastinal radiation could be broadly separated into three parts, namely,
extensive (Hodgkin disease), variable (e.g., non-Hodgkin lymphoma and lung cancer), and tangential (breast cancer). The mechanisms by which long-term RT interacts with cardiovascular system are largely unknown [7]. Certain cytokines and growth factors have been implicated to play roles [35]. RT exerts detrimental effects on systolic and diastolic cardiac function at 4 to 6 weeks after RT [36]. Other studies reported that radiation for breast cancer is linked to narrowing of the coronary arteries [37,38] or cardiac perfusion defects 6 months later [39]. Novel techniques have been studied to decrease the radiation dosage to the heart, including end-inspiration-gated
radiotherapy [40] or other respiratory maneuvers [41]. An increasing trend was also observed for omission of the internal mammary field, which presumably increases the dose to the heart [42]. Experimental evidence showed that radiation doses >2 Gy, in combination with elevated cholesterol levels, might initiate atherosclerosis and 239 240 241 242 243 244 245 246 247 248 249 250 251 252 253 254 255 256
doses <5 Gy are not associated with significantly increased risk of cardiovascular morbidity [31, 43]. Modern radiotherapy, especially with deep inspiration breath–hold techniques, can reduce the averaged doses over the whole heart from 3 Gy to 17 Gy[21] to < 2Gy [44].
To the best of our knowledge, this study is the first to investigate the incidence of ACS in patients with breast cancer and a history of CAD. The strengths of our study included a large and representative study sample. The claim data-based population study also had minimal chance for loss to follow-up of the study sample.
Nevertheless, some limitations should be noted. First, we ascertained the ACS events from medical claims, which could under-report the incidence of ACS because some patients who developed first-time ACS events might die before they can be sent to emergency rooms. Such under-report may occur to both patients with or without RT, and such non-differential misclassification would lead to an underestimation rather than overestimation of HR. Second, we used solely diagnostic codes to determine ACS, which may entail, at least to some extent, certain degrees of information bias. Again, the chance of over- or under-ascertainment of ACS is likely to be similar in both RT and non-RT groups (i.e., non-differential), which would bias the relative risk estimate toward the null, and should not be a valid argument for the observed positive association of RT with incidence of ACS. Third, we were unable to completely adjust 258 259 260 261 262 263 264 265 266 267 268 269 270 271 272 273 274 275 276
for some important risk factors for ACS such as exercise, smoking, and overweight, which are not available from medical claims. Fourth, we could not evaluate the cardiovascular effects associated with trade and doses of radiation because details about the irradiated volume, such as internal mammary lymph nodes and anterior boost volume to the left breast, were not be available from medical claims. We also did not separately assess the effect of RT on left- and right-sided breast cancer. Fifth, we could not obtain information on cancer staging from medical claims. However, most of our study samples are believed to be early-stage breast cancer patients, who normally require surgery. Moreover, chemotherapy may cause premature menopause, which might consequently increase the incidence of CAD. Failure to include the specific chemotherapy drugs in the analyses also warrants further investigation.
In summary, this study involving nearly 12 years of follow-up noted an excess of ACS events in patients who had a history of CAD and received RT for breast cancer. Careful management of RT in this high-risk segment of patients with breast cancer should be evaluated for the potential survival benefit.
277 278 279 280 281 282 283 284 285 286 287 288 289 290 291 292 293
Disclaimers:
The authors declare no conflict of interest. Manuscript has not been and will not be a podium or poster meeting presentation.
294
295 296
Acknowledgments
This study was supported by a grant from Taiwan National Scientific Council (NSC101-2314-B-006-076-MY3).
297
298 299
References
1. Jemal A, Bray F, Center MM et al (2011) Global cancer statistics. CA Cancer J Clin 61:69-90.
2. Rutqvist LE, Rose C, Cavallin-Stahl E (2003) A systematic overview of radiation therapy effects in breast cancer. Acta Oncol 42:532-545.
3. Clarke M, Collins R, Darby S et al (2005) Effects of radiotherapy and of
differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet 366:2087-2106.
4. Veronesi U, Cascinelli N, Mariani L et al (2002) Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 347:1227-1232.
5. Adams MJ, Lipsitz SR, Colan SD et al (2004) Cardiovascular status in long-term survivors of Hodgkin's disease treated with chest radiotherapy. J Clin Oncol 22:3139-3148.
6. De Bruin ML, Sparidans J, van't Veer MB et al (2009) Breast cancer risk in female survivors of Hodgkin's lymphoma: lower risk after smaller radiation volumes.J Clin Oncol 27:4239-4246.
7. Stewart FA, Seemann I, Hoving S et al (2013) Understanding radiation-induced cardiovascular damage and strategies for intervention. Clin Oncol 25:617-624. 8. Schultz-Hector S, Trott KR (2007) Radiation-induced cardiovascular diseases: is
the epidemiologic evidence compatible with the radiobiologic data? Int J Radiat Oncol Biol Phys 67:10-18.
9. Martinou M, Gaya A (2013) Cardiac complications after radical radiotherapy. SeminOncol40:178-185.
10. Darby SC, Ewertz M, McGale P et al (2013) Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med 368:987-998. 11. Bouillon K, Haddy N, Delaloge S et al (2011) Long-term cardiovascular mortality 301 302 303 304 305 306 307 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328
after radiotherapy for breast cancer. J Am Coll Cardiol 57:445-452.
12. Carpeggiani C, Rossi G, Landi P et al (2015) Long-term outcome and medical radiation exposure in patients hospitalized for cardiovascular disease. Int J Cardiol 195:30-36.
13. Vallis KA, Pintilie M, Chong N et al (2002) Assessment of coronary heart disease morbidity and mortality after radiation therapy for early breast cancer. J Clin Oncol 20:1036-1042.
14. Wang W, O'Connell D, Stuart K et al (2011) Analysis of 10-year cause-specific mortality of patients with breast cancer treated in New South Wales in 1995. J Med Imaging Radiat Oncol 55:516-525.
15. Borger JH, Hooning MJ, Boersma LJ et al (2007) Cardiotoxic effects of tangential breast irradiation in early breast cancer patients: the role of irradiated heart volume. Int J Radiat Oncol Biol Phys 69:1131-1138.
16. Correa CR, Das IJ, Litt HI et al (2008) Association between tangential beam treatment parameters and cardiac abnormalities after definitive radiation treatment for left-sided breast cancer. Int J Radiat Oncol Biol Phys 72:508-516.
17. Bouchardy C, Rapiti E, Usel M et al (2010) Excess of cardiovascular mortality among node-negative breast cancer patients irradiated for inner-quadrant tumors. Ann Oncol 21:459-465.
18. Park CK, Li X, Starr J, Harris EE (2011) Cardiac morbidity and mortality in women with ductal carcinoma in situ of the breast treated with breast conservation therapy. Breast J 17:470-476.
19. Uehlinger NB, Beyeler F, Weiss J et al (2010) Organ transplantation in Switzerland: impact of the new transplant law on cold ischaemia time and organ transports. Swiss Med Wkly 140:222-227.
20. Rutqvist LE, Lax I, Fornander T et al (1992) Cardiovascular mortality in a
randomized trial of adjuvant radiation therapy versus surgery alone in primary breast cancer. Int J Radiat Oncol Biol Phys 22:887-896.
329 330 331 332 333 334 335 336 337 338 339 340 341 342 343 344 345 346 347 348 349 350 351 352 353 354 355 356 357
radiotherapy. Cancer Treat Reviews 33:578-593.
22. Woodward WA, Strom EA, McNeese MD et al (2003) Cardiovascular death and second non-breast cancer malignancy after postmastectomy radiation and doxorubicin-based chemotherapy. Int J Radiat Oncol Biol Phys 57:327-335. 23. Lu JF, Hsiao WC (2003) Does universal health insurance make health care
unaffordable? Lessons from Taiwan. Health affairs 22:77-88.
24. Insurance. BoNH Regulations governing contracting and management of National Health Insurance medical care institutions. .
http://www.nhi.gov.tw/English/webdata/webdata.aspx?
menu=11&menu_id=295&WD_ID=295&webdata_id=3284 Accessed
September 4, 2014.
25. Berenson K, Ogbonnaya A, Casciano R et al (2010) Economic consequences of ACS-related rehospitalizations in the US. Curr Med Res Opin 26:329-336. 26. Wilson PW, D'Agostino RB, Levy D et al (1998) Prediction of coronary heart
disease using risk factor categories. Circulation 97:1837-1847.
27. Hooning MJ, Botma A, Aleman BM et al (2007) Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J Natl Cancer Inst 99:365-375. 28. Cuzick J, Stewart H, Rutqvist L et al (1994) Cause-specific mortality in long-term
survivors of breast cancer who participated in trials of radiotherapy. J Clin Oncol 12:447-453.
29. Paszat LF, Vallis KA, Benk VM et al (2007) A population-based case-cohort study of the risk of myocardial infarction following radiation therapy for breast cancer. Radiother Oncol 82:294-300.
30. Tsai YW, Tsai TI, Yang CL et al (2008) Gender differences in smoking behaviors in an Asian population. J Women Health 17:971-978.
31. Darby SC, McGale P, Taylor CW et al (2005) Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol 6:557-565. 359 360 361 362 363 364 365 366 367 368 369 370 371 372 373 374 375 376 377 378 379 380 381 382 383 384 385 386 387
32. McGovern PG, Pankow JS, Shahar E et al (1996) Recent trends in acute coronary heart disease--mortality, morbidity, medical care, and risk factors. The
Minnesota Heart Survey Investigators. N Engl J Med 334:884-890. 33. Fisher B, Anderson S, Bryant J et al (2002) Twenty-year follow-up of a
randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 347:1233-1241.
34. Tuttle TM, Jarosek S, Habermann EB et al (2012) Omission of radiation therapy after breast-conserving surgery in the United States: a population-based analysis of clinicopathologic factors. Cancer 118:2004-2013.
35. Basavaraju SR, Easterly CE (2002) Pathophysiological effects of radiation on atherosclerosis development and progression, and the incidence of
cardiovascular complications. Med Phy 29:2391-2403.
36. Dogan SM, Bilici HM, Bakkal H et al (2012) The effect of radiotherapy on cardiac function. Coron Artery Dis 23:146-154.
37. No authors listed (2012) Radiation for breast cancer is linked to narrowing of the coronary arteries. Harv Womens Health Watch 19:6-7.
38. Correa CR, Litt HI, Hwang WT et al (2007) Coronary artery findings after left-sided compared with right-left-sided radiation treatment for early-stage breast cancer. J Clin Oncol 25:3031-3037.
39. Hardenbergh PH, Munley MT, Bentel GC et al (2001) Cardiac perfusion changes in patients treated for breast cancer with radiation therapy and doxorubicin: preliminary results. Int J Radiat Oncol Biol Phys 49:1023-1028.
40. Korreman SS, Pedersen AN, Josipovic M et al (2006) Cardiac and pulmonary complication probabilities for breast cancer patients after routine end-inspiration gated radiotherapy. Radiother Oncol 80:257-262.
41. Chen MH, Cash EP, Danias PG et al (2002) Respiratory maneuvers decrease irradiated cardiac volume in patients with left-sided breast cancer.J CardiovascMagnReson 4:265-271. 388 389 390 391 392 393 394 395 396 397 398 399 400 401 402 403 404 405 406 407 408 409 410 411 412 413 414 415 416
paradox! J Cancer Res and Ther 3:190-192.
43. Tukenova M, Guibout C, Oberlin O et al (2010) Role of cancer treatment in long-term overall and cardiovascular mortality after childhood cancer. J Clin Oncol 28:1308-1315.
44. Borst GR, Sonke JJ, den Hollander S et al (2010) Clinical results of image-guided deep inspiration breath hold breast irradiation. Int J Radiat Oncol Biol Phys 78:1345-1351. 418 419 420 421 422 423 424 425
Table 1. Characteristics of patients with breast cancer and with or without RT within one year after operation.
With RT (n = 1,851) Without RT (n = 3,431) p-value* n % n %
Median age (years), range 59, (34-95) 64, (28-99) <0.0001
Female 1848 99.84 3425 99.83 0.9143
Partial mastectomy 937 50.62 305 8.89 <0.0001
Total mastectomy 914 49.38 3126 91.11 <0.0001
RT, linear accelerator teletherapy
Each simple portal 1841 99.46 0
Each complex portal 324 17.50 0
CAD risk factors
Hypertension 1361 73.53 2852 83.12 <0.0001
Diabetes mellitus 896 48.41 1871 54.53 <0.0001
Hyperlipidemia 1281 69.21 2484 72.40 0.0144
* Based on Wilcoxon rank sum test or Pearson’s 2 test 426
427
428 429
Table 2. Incidence rate and HRs of acute coronary syndrome for in relation to radiation and covariates.
Variables n Person-years Incidence rate a Adjusted HR b p-value
Estimate 95% CI Estimate 95% CI Radiation No 266 15070.36 1.77 1.56-1.99 1.00 Yes 110 7269.62 1.51 1.24-1.82 1.48 1.18-1.87 0.0007 Hypertension No 15 4425.98 0.39 0.19-0.56 1.00 Yes 361 17913.99 2.02 1.81-2.23 3.31 1.94-5.66 <.0001 Diabetes mellitus No 112 10334.92 1.08 0.89-1.30 1.00 Yes 264 12005.05 2.20 1.94-2.48 1.50 1.19-1.89 0.0005 Hyperlipidemia No 66 5968.26 1.11 0.86-1.41 1.00 Yes 310 16371.72 1.89 1.69-2.12 1.02 0.77-1.35 0.8845 Age (years) <50 21 3555.38 0.59 0.37-0.90 1.00 50 - <65 116 9681.89 1.20 0.99-1.44 1.62 1.01-2.60 0.0045 ≧ 65 239 9102.70 2.63 2.30-2.98 3.45 2.17-5.47 <.0001 Total 376 22339.97 1.68 1.52-1.86
a No. of cases per 100 p-y
b Estimated from the Cox model that simultaneously included radiation, hypertension, diabetes mellitus, and age in the model. 430
431
432 433
Table 3. Cumulative event-free rate of patients with breast cancer who received RT. Follow-up (years) Radiation No radiation No. of ACS Event rate Cumulative event-free rate No. of ACS Event rate Cumulative event-free rate 0–2 2 0.0011 0.9989 3 0.0009 0.9989 2–4 28 0.0188 0.9801 57 0.0207 0.9782 4–6 35 0.0470 0.9341 60 0.0358 0.9432 6–8 28 0.0798 0.8595 63 0.0664 0.8806 8–10 12 0.0870 0.7848 52 0.1135 0.7806 10–12 5 0.1613 0.6582 31 0.2109 0.6160 434 435 436 437
Exclusion:
1. 875 patients who received no breast surgery
2. 327 patients who underwent radiation therapy (RT) at >1 y after breast cancer diagnosis
Patients with first-ever breast cancer diagnosis from Jan 1, 1999 to Dec 31, 2010 n = 84,657
Patients with breast cancer who received RT within one year after
breast surgery, n = 1,851
Patients with breast cancer who received no RT after breast surgery,
n = 3,431
Followed to the end of 2010
Patients admitted for acute coronary syndrome
n=110
Patients admitted for acute coronary syndrome
n=266
Study cohort, n=5,282 Inclusion:
Those with a history of coronary artery disease (CAD), but not acute coronary syndrome (ACS)
n=15,580
Patients with first-ever breast cancer diagnosis from Jan 1, 1999 to Dec 31, 2010 and had a history
of CAD, n=6,484 n=15,580 438 439 440 441 442 443 444 445 446 447 448 449 450 451 452 453 454 455 456 457 458 459
Figure 1. Flow chart of selection and follow-up of study participants. 460