This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon.
Exploring the Impact of Mentoring Functions on Job Satisfaction and
Organizational Commitment of New Staff Nurses
BMC Health Services Research 2010, 10:240 doi:10.1186/1472-6963-10-240 Rhay-Hung Weng (wonhon@mail2000.com.tw)
Ching-Yuan Huang (yuan@mail2000.com.tw) Wen-Chen Tsai (wtsai@mail.cmu.edu.tw)
Li-Yu Chang (jah0795@mail.jah.org.tw) Syr-En Lin (h500@stm.org.tw) Mei-Ying Lee (ming3076@sph.org.tw)
ISSN 1472-6963 Article type Research article Submission date 11 June 2009 Acceptance date 16 August 2010
Publication date 16 August 2010
Article URL http://www.biomedcentral.com/1472-6963/10/240
Like all articles in BMC journals, this peer-reviewed article was published immediately upon acceptance. It can be downloaded, printed and distributed freely for any purposes (see copyright
notice below).
Articles in BMC journals are listed in PubMed and archived at PubMed Central.
For information about publishing your research in BMC journals or any BioMed Central journal, go to http://www.biomedcentral.com/info/authors/
BMC Health Services Research
© 2010 Weng et al. , licensee BioMed Central Ltd.
This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Exploring the impact of mentoring functions on job satisfaction and
organizational commitment of new staff nurses
1
Rhay-Hung Weng 2*Ching-Yuan Huang 3 Wen-Chen Tsai 4 Li-Yu Chang 5
Mei-Ying Lee 6 Syr-En Lin Address:
1
Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, R.O.C. 2 International Business and Trade, Shu-Te University, Taiwan, R.O.C. 3 Health Services Administration, China Medical University, Taiwan, R.O.C. 4 Nursing, Jen-Ai Hospital, Taiwan, R.O.C 5 Nursing, Saint Paul's Hospital, Taiwan, R.O.C. 6 Nursing, St. Martin De Porres Hospital, Taiwan, R.O.C.
E-mail: 1
Rhay-Hung Weng (wonhon@mail2000.com.tw) 2
Ching-Yuan Huang (yuan@mail2000.com.tw) 3
Wen-Chen Tsai (wtsai@mail.cmu.edu.tw) 4
Li-Yu Chang (jah0795@mail.jah.org.tw) 5
Mei-Ying Lee (ming3076@sph.org.tw) 6
Syr-En Lin (h500@stm.org.tw) *
Corresponding author:
Ching-Yuan Huang
Department of International Business and Trade Shu-Te University
No. 59, Hengshan Rd., Yanchao, Kaohsiung County, 82445 Taiwan (R.O.C.) TEL: + 886-929-783601
Abstract
Background
Although previous studies proved that the implementation of mentoring program is beneficial for enhancing the nursing skills and attitudes, few researchers devoted to exploring the impact of mentoring functions on job satisfaction and organizational commitment of new nurses. In this research we aimed at examining the effects of mentoring functions on the job satisfaction and organizational commitment of new nurses in Taiwan’s hospitals.
Methods
We employed self-administered questionnaires to collect research data and select new nurses from three regional hospitals as samples in Taiwan. In all, 306 nurse samples were obtained. We adopted a multiple regression analysis to test the impact of the mentoring functions.
Results
Results revealed that career development and role modeling functions have positive effects on the job satisfaction and organizational commitment of new nurses; however, the psychosocial support function was incapable of providing adequate explanation for these work outcomes.
Conclusion
It is suggested in this study that nurse managers should improve the career development and role modeling functions of mentoring in order to enhance the job satisfaction and organizational commitment of new nurses.
Background
Nurse turnover and turnover intent have received considerable worldwide attention
because of their influence on patient safety and health outcomes. The turnover intent
among new nurses is often higher than that among senior nurses[1]. Nurse turnover in
the first year of practice ranges between 35% and 60%[2]. With the high turnover
incidence among new nurses, it is imperative that retention strategies be effective and
that these strategies be examined closely. When new nurses perform their duties in
hospitals, they often have little or no experience in clinical nursing but they are
required to bear full responsibility of patient care. Owing to limited clinical skills,
experience, and full responsibility of patient care, new nurses would often bear heavy
work pressure. Work pressure and nurse attitudes toward jobs have significant impact
on job satisfaction and organizational commitment among hospital nurses [3-5].
Researches from various countries have confirmed that job satisfaction and
organizational commitment are statistically significant predictors of nurse
absenteeism or turnover, or their intent to quit[1, 6, 7]. Thus, in order to reduce the
nurses’ intent to leave, nurse managers should urgently address the issue of improving
the job satisfaction and organizational commitment of new nurses.
Proenca and Shewchuck[8] indicate that learning and career development
nurses. Mentors play a vital role in providing these opportunities. Moreover, mentors
can facilitate professional socialization of the new nurses in nursing; facilitate their
transition into the workplace and social culture of the organization; and make them
feel welcome in peer groups, with coworkers and the organization[9]. In addition,
mentoring can promote the transfer of knowledge and values that support a hospital’s
mission. Therefore, a mentoring program is seen as a useful approach in improving
the retention of new nurses[10, 11].
The mentoring program is a formal relationship between a senior nurse and junior
nurses of a hospital directed toward the advancement and support of the junior
nurses[2, 9]. It is a useful approach for new nurses as it provides them with effective
and systematic support in the nursing practice, facilitates their professional
development, and enhances the coordination of care within the unique context of
general practice[12]. Tourigny and Pulich[13] argue that apart from the positive
influence on medical care quality, mentoring programs play an important role in
improving the work performance of the new nurses and establishing their attitudes
toward the organizations they work for. Therefore, after the implementation of the
new nurse mentoring program, mentors provide career development advice,
Psychosocial support functions include acceptance, counseling, and friendship.
Friendship is provided by informal interactions at work, and by a willingness to
discuss a variety of topics. Career development functions include sponsorship,
protection, challenging assignments, exposure, and visibility. Exposure and visibility
involve creating opportunities where important decision makers can observe and
appreciate a person’s competence, abilities, and special talents. Career development
functions focus on the organization and the mentee’s career, whereas psychosocial
support functions affect the mentee at a more personal level and extend to other areas
of life[15-17]. Besides, mentees have observed that mentors play a significant role in
shaping their views on how they would act as mentors, thus highlighting the
importance of role modeling. Role modeling is behaving and acting in a way that
others can emulate; a role model displays appropriate attitudes, values, and behaviors
to learn and follow[18-20]. In other words, role modeling functions focus on the fact
that mentees would try to imitate the mentor’s behavior because of their respect for
and trust in the mentors.
Although it has been proven in previous studies that the implementation of a
mentoring program is beneficial in terms of enhancing nursing skills and attitudes,
few researchers have explored the impact of mentoring functions on the job
paper was to examine the effects of the different mentoring functions on the work
outcomes through a survey of new nurses in Taiwan.
Methods
1 Data Source and Analysis
We employed self-administered questionnaires to collect research data. For our
subjects, we selected new nurses from three regional hospitals in Taiwan. In the
course of the study, the participating hospitals facilitated formal meetings with head
nurses, provided contact information on 308 eligible nurses who had been working in
their hospital for two years or less, and gave their full support and coordination in the
conduct of the research. We sent out 308 questionnaires over two months to survey
the new nurses anonymously.
In all, 306 nurse subjects were obtained with an overall valid response rate of 99.35%.
Because all the research data are self-reported and collected through the same
questionnaire during the same period of time, a common method variance (CMV)
may result in a systematic measurement error and may further bias the estimates of
the true relationship between the theoretical constructs[21]. We have adopted some
procedural techniques designed to address the CMV problem. These included
we also used Harman’s one-factor test to check for the presence of CMV in the data.
The Harman’s one-factor test results were as follows: twenty factors had an
eigenvalue greater than 1, and forty-four factors accounted for 97.85% of the variance.
Thus, CMV was not considered a serious threat to this study[21]. After testing for
CMV, reliability, and validity, we conducted a multiple regression analysis to test the
impact of the mentoring functions.
2 Ethical consideration
The ethical issues of this study were reviewed and approved by the ethical committee
of three sample hospitals. During the process of questionnaire collection, we also sent
out informed consent form to 308 eligible nurses to be sure that they agreed to
participate in this survey.
3 Measurement
3.1 Research Variables
Questionnaire items were designed based on existing theoretical constructs and
literature. Three mentoring experts and six nurse managers made some modifications
and the contents of the questionnaires were validated by experts. The five-point Likert
scale (1 = do not agree at all or not satisfied at all; 5 = extremely agree or extremely
the questionnaire was tested by the confirmatory factor analysis.
3.1.1 Mentoring Function: Mentoring function is defined as the sum of the career development function, psychosocial support function, and role
modeling function as perceived by nurses in the mentoring program. The
measuring scales were based on the mentoring function scales proposed by
Scandura[19], Raabe et al.[22], Sosik & Godshalk[20], and Eby et
al[23]. Nine items were prepared, including three items in three dimensions:
career development function, psychosocial support function, and role
modeling function with a Cronbach’s α value of 0.912. The mean value of
the career development function, psychosocial support function, and role
modeling function is 3.49 (SD = 0.64), 3.49 (SD = 0.73), and 3.90 (SD =
0.66), respectively.
3.1.2 Job satisfaction: After referencing literatures on job satisfaction[17, 20, 24, 25], and evaluating the nurses’ work responsibilities and experience, job
satisfaction is defined as the nurses’ overall state of satisfaction. Lankau &
Scandura[24] point out that the Minnesota Satisfaction Questionnaire
(MSQ) is a well-constructed scale for measuring work satisfaction in the
five items with a Cronbach’s α value of 0.865 and a mean of 3.59 (SD =
0.57).
3.1.3 Organizational commitment: Organizational commitment refers to the belief in and acceptance of organizational goals and values such that nurses
are willing to make considerable efforts to achieve them, and are willing to
remain with the organization[21, 25-27]. The Organization Commitment
Questionnaire (OCQ) developed by Mowday et al.[28] is accepted as the
most widely used unidimensional measure of organizational commitment. It
contains three dimensions: value commitment, effort commitment, and
retention commitment[26]. Therefore, we developed a total of six items
with a Cronbach’s α value of 0.913 based on the OCQ and a mean of 3.40
(SD = 0.63).
3.2 Control Variables
We used sample source, mentee’s age[24, 29], mentee’s gender[24], mentee’s
education level[24], mentee’s nursing experience[24, 30], mentor’s nursing ladder[20,
30], mentoring period[24, 29], and frequency of interactions with the mentor[24, 29,
30] as control variables in our regression models. Previous literatures have
organizational commitment. Frequency of interactions with the mentor was defined as
the mentee’s perceived degree of frequency rate of interaction with mentor per month.
With respect to the measurement method, the five-point scale (1 = Seldom;
2=Sometimes;3= Normally;4= Usually;5 = Always) was used. Nursing experts
involved in the study suggested that the factors “mentor had been trained for
mentoring” and “mentor had the experience of mentoring” affect the work outcome of
the new nurses in the mentoring program. Therefore, we included these two factors as
control variables in the follow-up regression.
3.3 Measure Validity and Reliability
All measures were subjected to a confirmatory factor analysis (CFA) using the AMOS
6.0 to test for unidimensionality, and convergent and discriminant validity[31]. Since
job satisfaction does not include different dimensions, this study divided the five
items of this construct into two composite indicators: the average value for the odd
number items is named “job satisfaction 1,” and the average value for the even
number items is named “job satisfaction 2.”After the CFA analysis, this model
generated acceptable fit indices (χ2/df = 2.535; GFI = 0.969; AGFI = 0.931; RMR =
0.010; CFI = 0.988; NFI = 0.981; RFI = 0.967; IFI = 0.989; TLI = 0.980; RMSEA =
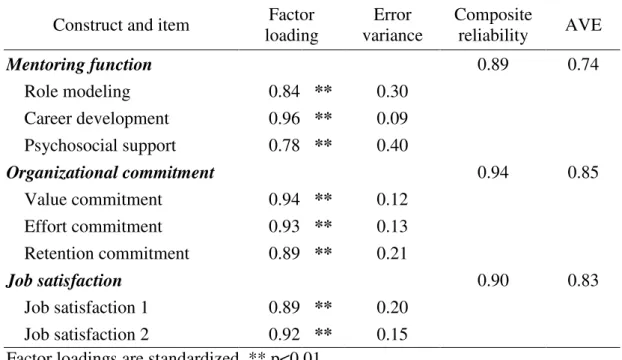
0.071). Table 1 show that the minimum value of the composite reliability of all the
This indicates that every research construct possesses good internal consistency. In
addition, Table 1 shows that the factor loadings of all the research construct items
reach statistically significant levels. This indicates that the measurement model has
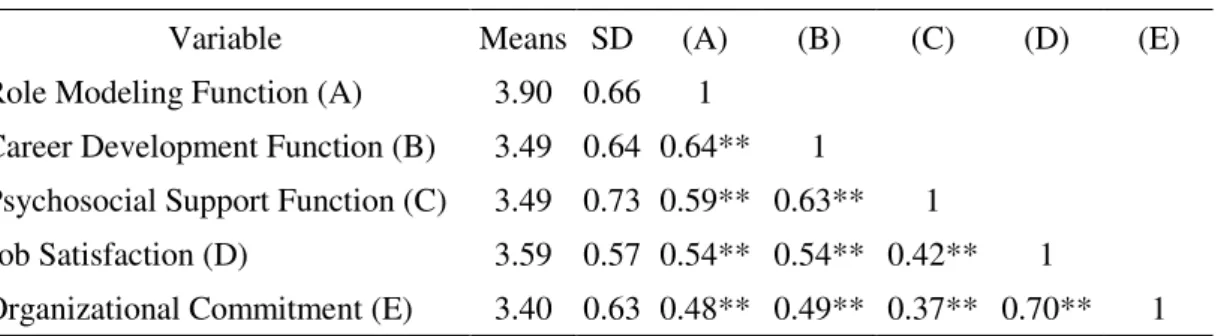
good convergent validity[32]. The CFA results also showed that the square roots of all
the AVE values of every research construct are higher than the pairwise correlation
coefficients; the correlation coefficients between mentoring function and
organizational commitment, between mentoring function and job satisfaction, and
between organizational commitment and job satisfaction are 0.54, 0.63, and 0.75,
respectively. This also shows that the measurement model of all the research
constructs had good discriminate validity[32].
Results
The mean age of the sample was 26.83 (SD = 3.87). Thirty-five percent of the sample
had earned a Bachelor of Science degree or higher in nursing and seventy percent of
the new nurses had nursing experience of more than one year. The mean period of the
mentoring program was 3.97 (SD = 2.43), and the frequency rate of interaction
between the mentors and mentees was 3.60 (SD = 0.86). In particular, most mentors
earned the level III of the nursing ladder or higher (69.93%), had been trained for
mentoring (62.09%), and had prior mentoring experience (83.66%) (Table 2). Besides,
During the survey period, we found that all the hospitals that were part of the study
have an existing formal program that required mentors to give guidance and
assistance to new staff nurses for at least two months. We found that the new staff
obtained clinical guidance and mentor assistance for nearly four months, during which
interaction with their mentors was frequent. Nursing managers usually assigned senior
nurses—who had achieved the level III of the nursing ladder or higher—as mentors to
guide the new staff nurses. Besides, mentors often not only had to be trained for
mentoring but also usually had to have mentoring experience. Training program for
mentoring in Taiwan is often designed for mentors. The types of this program include
classes, seminar, workshop, or conference. The topics of all types of this program are
related to the mentor’s role and responsibilities, the mentor’s communication skills,
the mentor’s clinical evaluation ability, mentor’s case teaching ability, mentor’s
teaching evaluation and feedback, medical ethics and laws, or mentor’s experience
sharing. Therefore, there were some requirements related to the mentor’s
qualifications and these not only focused on clinical expertise but also placed
importance on the mentoring abilities and experiences of senior nurses who wanted to
be mentors.
Overall, the current mentoring program for new staff nurses actually works as
the effects of the career development, psychosocial support, and role modeling
functions on them. Of these three functions, the level of the role modeling function as
perceived by the mentees is the highest (mean = 3.90) as compared with the levels of
the career development and psychosocial support functions, which are relatively
lower (mean = 3.49). Thus, the mentors who served as senior nurses actually
produced a role modeling effect on the new nurses; however, the mentees perceived
relatively limited functions that concerned the psychological and development of new
nurses (including career development and psychosocial support functions). We should
focus on this finding and view it as a critical issue that requires our efforts to improve
in the future.
Before conducting the multiple regression analysis, we adopted the Kolmogorov-
Smirnov test to examine the residual normality of the regression models. The result of
the Kolmogorov-Smirov test showed that the residual normality of each regression
model was acceptable (p > 0.05). Besides, the residual analysis plot showed that our
regression models did not violate the assumptions of linearity and homogeneity. We
also assessed the multicollinearity of the models by examining the variance inflation
factor (VIF) and found that all VIF values for independent variables were less than 7.
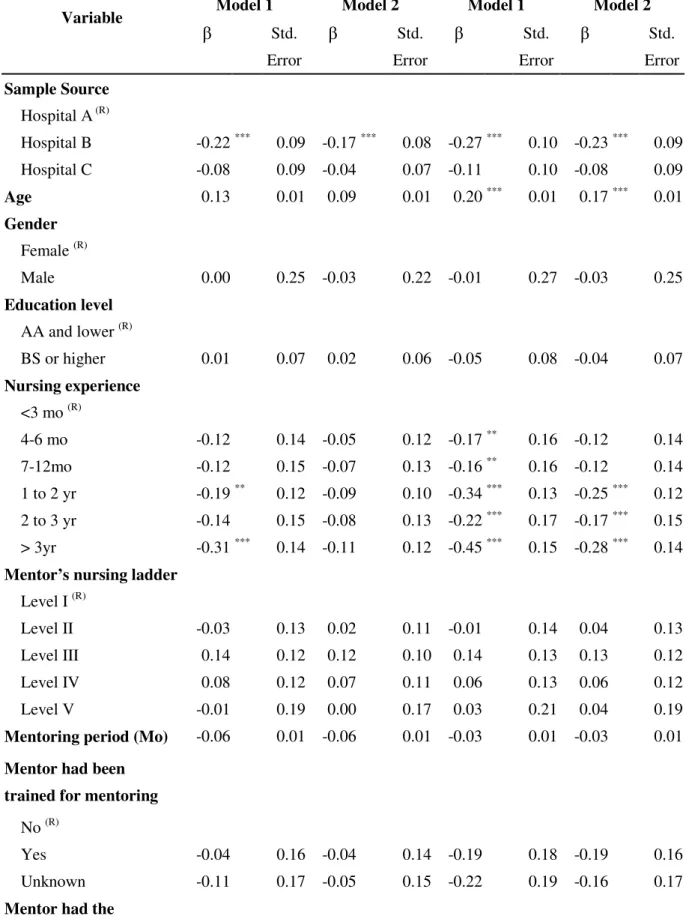
Table 4 shows the results of our multi-regression analysis for job satisfaction. The
result of Model 1 indicates that three control variables—sample source, nursing
experience, and frequency of interaction with the mentor—would significantly affect
job satisfaction. After including the variables of the mentoring functions, only the
career development function (β = 0.31) and the role modeling function (β = 0.30)
were found to be significantly and positively related to job satisfaction; however, the
coefficient of the psychosocial support function was not significant (Model 2). The
results of the regression analysis for organizational commitment showed that four
control variables—sample source, nursing experience, mentor had prior mentoring
experience, and frequency of interactions with the mentor—would have a significant
influence on organizational commitment (Model 1). After including the variables of
the mentoring functions, we also found that the impact of the career development
function (β = 0.28) and the role modeling function (β = 0.26) on organizational
commitment is significantly positive, but the coefficient of the psychosocial support
function is not significant (Model 2).
Discussion
Bahniuk[33] and Allen[34] have proven that the mentoring program enhances the job
satisfaction of the mentees. During the mentoring process, mentors would often assign
and skills, provide career guidance, support the advancement of job position, help in
resolving task-related problems, and further promote their overall growth. In this way,
mentees improve their knowledge and skills and have a clear picture about their
career development and position advancement [35-37]. The knowledge and
experience exchange and learning opportunities in the mentorship were found to
increase the mentees’ sense of confidence toward their job, decrease their anxiety for
the future, satisfy their career development needs and further create a high level of job
satisfaction [7, 19, 38]. All the above mentioned benefits for mentees primarily stem
from the career development function. Furthermore, McNeese-Smith & Nazarey[39]
had used content analysis to analyze the interview data of 30 nurses. They found that
apart from personal factors, the learning opportunities provided by the organization
are critical factors that have a highly positive relationship with organizational
commitment. In addition to providing a number of learning opportunities, mentoring
programs also provide insight into the hospital systems and regulations; create room
for performance feedbacks, discussions, and feedback friendship and offer the
necessary clinical support. These career-related functions are vital for establishing a
sense of organizational identity and organizational belonging. The organizational
commitment of mentees is positively related to their sense of organizational identity
organizational commitment that connects organizational practices and specific job
characteristics to the emotions and cognitions of employees. He found that an
individual’s perceptions of organizational support are key emotional and cognitive
processes that mobilize commitment in the workplace. Overall, study results have
proven a significant positive relationship between career development function and
job satisfaction or organizational commitment of new staff nurses.
We also found a significant positive relationship between role modeling function and
job satisfaction or organizational commitment of new nurses. As a result of the trust
and respect for the mentors, the mentees can try to imitate the mentor’s behavior in
mentorship (role modeling) and can then upgrade their expertise and skills[13, 41, 42].
Besides, the mentees’ perception of such mentoring relationships as trustful and
respectful will be beneficial for the mentees in improving their workplace experience,
perceptions, and future expectations. Therefore, if mentoring programs produced role
modeling functions, they could effectively improve the expertise and skills of new
nurses. In addition, it would facilitate the mentee’s adaptation to nursing jobs and
nursing environments. If new staff nurses adapt well to their nursing jobs and nursing
environments, they will have higher job satisfaction and few complaints against the
hospitals, invest more effort and initiative in their work, and further strengthen their
role modeling function in the mentorship, it indicates that mentors have more referent
power for mentees. In such conditions, there are fewer conflicts between mentors and
mentees when the former guide the latter. The decline in conflicts is positively related
to the growing improvement in the relationship between the mentors and mentees and
in the learning effects from the mentorship. In addition, the mentees’ commitment to
their organizations would further strengthen and improve the mentor-mentee
relationship and increase the benefits of mentoring [10, 43].
Conclusion
This cross-sectional study examined the influence of career development,
psychosocial support, and role modeling functions on the job satisfaction and
organizational commitment of new staff nurses.
The results indicated that the development of mentoring programs for new staff nurses
in Taiwan has reached a mature state and that the interactions between new nurses and
their mentors are frequent, useful, and enduring. To serve as mentors, nurse managers
assigned senior nurses who had been trained for mentoring, had previous mentoring
experience, and had at least achieved the level III of the nursing ladder. In addition,
mentoring programs for new nurses are indeed capable of generating the role
that mentors do exhibit a higher degree of nursing knowledge and technical
capabilities; thus, the role modeling function appears to be significant in the
mentoring process. However, it is likely that nursing mentors are not concerned about
the psychosocial needs (for example, high praise from their mentors and the
establishment of friendship in the workplace) and career anxieties or directions of new
nurses. Therefore, the psychosocial support and career development functions, as
perceived by new nurses, appear to be lower in Taiwan. Despite being perceived to be
relatively lower by the new nurses, these two functions positively influence their job
satisfaction and organizational commitment. If nurse managers want to improve the
mentoring programs for new staff nurses, they should encourage mentors towards the
direction of lending psychosocial support, providing directions on career development,
giving opportunities for self-expression and promotion, and assigning challenging
tasks that provide more learning opportunities for the new nurses. Effective mentoring
will reinforce the job satisfaction of the new nurses and their commitment to the
hospital.
In addition, the results of this study show that the role modeling function provided by
mentors will positively influence the job satisfaction and organizational commitment
of new staff nurses. If the nursing mentors can exhibit a high degree of nursing
benchmarks, it will facilitate the mentee’s adaptation to their jobs and workplaces and
will further enhance their job satisfaction and improve their organizational
commitment. Therefore, while selecting senior nurses as mentors for new nurses,
nurse managers should carefully consider their expertise and abilities. Besides
expertise and abilities, nursing managers should reinforce the mentor’s professional
attitudes about nursing care and assist in improving their mentoring abilities in order
to strengthen the role modeling functions of the mentoring programs.
Limitations and future research suggestions
Since this study has a cross-sectional design, it has certain empirical limitations with
regard to the verification of the relationship between research constructs. Therefore, it
is suggested that future researchers use a study with a longitudinal design to further
consider the impact of mentoring functions on job satisfaction and organizational
commitment. In addition, we used Harman’s one-factor test to assess the seriousness
of common method biases. Although test results indicated that CMV was not
considered a serious threat to this study, we suggest that if future researchers can
overcome the data-collection and time-limitation problems, they can try to use the
temporal, proximal, psychological, or methodological separation of measurement to
Furthermore, this study only surveyed new staff nurses of Taiwan’s hospitals;
therefore, the findings cannot be generalized to other countries. Future researchers
may collect samples from different countries and continue to test the assumptions of
this research. Finally, future researchers can continue to investigate from different
perspectives in order to explore the influential factors and the impact of these factors
on the different dimensions of work outcomes (such as patient safety performance)
and further strengthen the integrity of the theory of mentorship in nursing.
Competing Interests
The author(s) declare that they have no competing interests.
Authors’ Contributions
WRH conceived of the study and made substantial contributions to study design, data
acquisition, and data analysis and result interpretation. He also took responsibility for
drafting and revising the manuscript. HJY performed the statistical analysis, assisted
in interpreting the results and writing the manuscript. TWC was involved in designing
the study, interpreting the analysis results and providing many important directions for
literature review and discussion. CLY, LMY, and LSE took responsibility for data
collection, participated in the data analysis and contributed to discussions. All authors
Appendix.1 Construct Measurement Items Mentoring Function
Career development
The mentor gave me many important assignments that provided me with
opportunities to learn nursing skills, for example, case analysis.
The mentor provided me with many suggestions about career development and
highlighted the relevant concerns.
The mentor gave me a lot of information about position advancement
opportunities.
Psychosocial support
I would discuss my private concerns and problems with my mentor.
I actually see my mentor as my “real” friend.
After work, I still kept in touch with my mentor.
Role modeling function
I tried to adapt my mentor’s behavior.
I really respect and admire my mentor’s nursing expertise and skills.
I really respect and admire my mentor for her mentoring expertise and skills.
Job Satisfaction
With regard to the sense of achievement while finishing my jobs, I feel…….
With regard to the performance feedbacks, I feel…….
With regard to whether my salary and welfare are commensurate with the
workload, I feel…….
With regard to the interactions with my coworkers, I feel…….
Organizational Commitment
Effort commitment
I am willing to put in extra efforts for my hospital.
I am willing to make an all-out effort to keep up with the hospital’s development.
Value commitment
I feel a sense of pride in doing my job at this hospital.
My current work environment is the ideal one, which I always hoped to work in.
Retention commitment
Even though there are better opportunities outside, I will not leave this hospital.
I have strong commitment to continue providing my services at this hospital until
retirement.
Acknowledgements
This study was supported by a grant from the National Science Council in Taiwan
References
1. Beecroft PC, Dorey F, Wenten M: Turnover intention in new graduate
nurses: A multivariate analysis. J Adv Nurs 2008, 62:41-52.
2. Halfer D, Graf E, Sullivan C: The organizational impact of a new graduate
pediatric nurse mentoring program. Nurs Econ 2008, 26:243-249.
3. Lu H, While AE, Barriball KL: Job satisfaction among nurses: A literature
review. International Journal of Nursing Studies 2005, 42:211-227.
4. Chu CI, Hsu HM, Price JL: Job satisfaction of hospital nurses: An
empirical test of a causal model in Taiwan. Int Nurs Rev 2003, 50:176-182.
5. Brief AP, Aldag RJ: Antecedents of organizational commitment among
hospital nurses. Work and Occupations 1980, 7:210-221.
6. Lee TY, Tzeng WC, Lin CH, Yeh ML: Effects of a preceptorship
programme on turnover rate, cost, quality and professional development.
J Clin Nurs 2009, 18:1217-1225.
7. Salt J, Cummings G, Profetto-McGrath J: Increasing retention of new
graduate nurses: A systematic review of interventions by healthcare organizations. J Nurs Adm 2008, 38:287-296.
8. Proenca EJ, Shewchuck: Organizational tenure and the perceived
importance of retention factors in nursing homes. Health Care Manag Rev
1997, 22:65-73.
9. Beecroft PC, Santner S, Lacy ML, Kunzman L, Dorey F: New graduate
nurses' perceptions of mentoring: Six-year programme evaluation. J Adv
Nurs 2006, 55:736 -747.
10. Andrews M, Wallis M: Mentorship in nursing: A literature review. J Adv Nurs 1999, 29:201-207.
11. Greene MT, Puetzer M: The value of mentoring: A strategic approach to
retention and recruitment. J Nurs Care Qual 2002, 17:63-70.
12. Gibson T, Heartfield M: Mentoring for nurses in general practice: An
Australian study. J Interprof Care 2005, 19:50-62.
13. Tourigny L, Pulich M: A critical examination of formal and informal
14. McCloughen A, O'Brien L: Development of a mentorship programme for
new graduate nurses in mental health. Int J Ment Health Nurs 2005, 14:276-284.
15. Ragins BR, Cotton J: Mentor functions and outcomes: A comparison of
men and women in formal and informal mentoring relationships. J Appl
Psychol 1999, 84:529-550.
16. Scandura TA: Mentorship and career mobility: An empirical investigation. J Org Behav 1992, 13:169-174.
17. Scandura TA: Mentoring and organizational justice: An empirical
investigation. J Vocat Behav 1997, 51:58-69.
18. Kram KE: Mentoring at work: Developmental relationships in
organizational life. Glenview, IL: Scott, Foresman; 1985.
19. Scandura TA, Williams EA: An Investigation of the moderating effects of
gender on the relationships between mentorship initiation and protégé perceptions of mentoring functions. J Vocat Behav 2001, 59:342-363.
20. Sosik JJ, Godshalk VM: Leadership styles, mentoring functions received,
and job-related stress: A conceptual model and preliminary study. J Org
Behav 2000, 21:365-390.
21. Podsakoff P, Organ D: Self-reports in organizational research: Problems
and prospects. J Manag 1986, 12:531-544.
22. Raabe B, Beehr TA: Formal mentoring versus supervisor and coworker
relationships: Differences in perceptions and impact. J Org Behav 2003, 24:271-293.
23. Eby LT, Lockwood AL, Butts M: Perceived support for mentoring: A
multiple perspectives approach. J Vocat Behav 2006, 68:267-291.
24. Lankau MJ, Scandura TA: An investigation of personal learning in
mentoring relationships: content, antecedents, and consequences. Acad
Manag J 2002, 45:779-790.
25. Laschinger HK, Finegan J, Shamian J: The impact of workplace
empowerment, organizational trust on staff nurses' work satisfaction and organizational commitment. Health Care Manag Rev 2001, 26:7-23.
organizational commitment. Hum Resour Manag Rev 1991, 1:61-89.
27. Payne SC, Huffman AH: A longitudinal examination of the influence of
mentoring on organizational commitment and turnover. Acad Manag J
2005, 48:158-168.
28. Mowday RT, Steers RM, Porter LW: The measurement of organizational
commitment. J Vocat Behav 1979, 14:224-247.
29. Godshalk VM, Sosik JJ: Aiming for career success: The role of learning
goal orientation in mentoring relationships. J Vocat Behav 2003, 63:417-437.
30. Day R, Allen TD: The relationship between career motivation and
self-efficacy with protégé career success. J Vocat Behav 2004, 64:72-91.
31. Bollen KA: Structural equations with latent variables. New York: John Wiley & Sons; 1989.
32. Fornell C, Larcker DF: Evaluating structural equation models with
unobservable variables and measurement error. J Mark Res 1981, 48:39-50.
33. Bahniuk MH, Dobos J, Kogler Hill SE: The impact of mentoring, collegial
support, and information adequacy on career success: A replication. J Soc
Behav Pers 1990, 5:431-451.
34. Allen TD, Russell JEA, Maetzke SB: Formal peer mentoring: Factors
related to protégés satisfaction and willingness to mentor others. Group
Organization Manag 1997, 22:488-507.
35. Fawcett DL: Mentoring--what it is and how to make it work. Association of Operating Room Nurses 2002, 75:950-954.
36. Gibson T, Heartfield M: Mentoring for nurses in general practice: An
Australian study. Journal of Interprofessional Care 2005, 19:50-62.
37. Tourigny L, Pulich M: A critical examination of formal and informal
mentoring among nurses. The Health Care Manager 2005, 24:68-76.
38. Underhill CM: The effectiveness of mentoring programs in corporate
settings: A meta-analytical review of the literature. J Vocat Behav 2006, 68:292-307.
organizational commitment among nurses / practitioner application. J
Healthc Manag 2001, 46:173-187.
40. Fang SR: An emperical study on relationship value, relationship quality
and loyalty for retailing bank industry. J Manag 2002, 19:1097-1130.
41. Scandura TA, Williams EA: Mentoring and transformational leadership:
The role of supervisory career mentoring. J Vocat Behav 2004, 65:448-468.
42. Wanberg CR, Welsh ET, Hezlett SA: Mentoring research : A review and
dynamic process model. Hum Resour Manag 2003, 22:39-124.
43. Donaldson SI, Ensher EA, Grant-Vallone EJ: Longitudinal examination of
mentoring relationships on organizational commitment and citizenship behavior. J Career Development 2000, 26:233-249.
Tables
Table 1 Assessment of Convergent and Discriminant Validity (n=306) Construct and item Factor
loading Error variance Composite reliability AVE Mentoring function 0.89 0.74 Role modeling 0.84 ** 0.30 Career development 0.96 ** 0.09 Psychosocial support 0.78 ** 0.40 Organizational commitment 0.94 0.85 Value commitment 0.94 ** 0.12 Effort commitment 0.93 ** 0.13 Retention commitment 0.89 ** 0.21 Job satisfaction 0.90 0.83 Job satisfaction 1 0.89 ** 0.20 Job satisfaction 2 0.92 ** 0.15 Factor loadings are standardized. ** p<0.01.
Table 2 Frequencies and Percentages on Selected Respondent Characteristics (n=306)
Variable Frequency % Variable Frequency %
Sample Source Mentor’s nursing ladder
Hospital A 81 26.47 Level I 31 10.13
Hospital B 108 35.29 Level II 61 19.93
Hospital C 117 38.24 Level III 119 38.89
Sex Level IV 83 27.12
Female 301 98.37 Level V 12 3.92
Male 5 1.63 Mentor had been trained for
mentoring
Education level No 14 4.58
AA and lower 199 65.03 Yes 190 62.09
BS or higher 107 34.97 Unknown 102 33.33
Nursing experience Mentor had the experience
of mentoring <3 mo 32 10.46 No 13 4.25 4-6 mo 31 10.13 Yes 256 83.66 7-12mo 27 8.82 Unknown 37 12.09 1 to 2 yr 94 30.72 2 to 3 yr 24 7.84 > 3yr 98 32.03
Table 3 Means, Standard Deviation and Correlation Matrix for Research Constructs
Variable Means SD (A) (B) (C) (D) (E)
Role Modeling Function (A) 3.90 0.66 1
Career Development Function (B) 3.49 0.64 0.64** 1
Psychosocial Support Function (C) 3.49 0.73 0.59** 0.63** 1
Job Satisfaction (D) 3.59 0.57 0.54** 0.54** 0.42** 1
Organizational Commitment (E) 3.40 0.63 0.48** 0.49** 0.37** 0.70** 1 ** p < .05
Table 4 Results of multiple regression analysis a (n=306)
Job Satisfaction Organizational Commitment
Model 1 Model 2 Model 1 Model 2
Variable β Std. Error β Std. Error β Std. Error β Std. Error Sample Source Hospital A (R) Hospital B -0.22 *** 0.09 -0.17 *** 0.08 -0.27 *** 0.10 -0.23 *** 0.09 Hospital C -0.08 0.09 -0.04 0.07 -0.11 0.10 -0.08 0.09 Age 0.13 0.01 0.09 0.01 0.20 *** 0.01 0.17 *** 0.01 Gender Female (R) Male 0.00 0.25 -0.03 0.22 -0.01 0.27 -0.03 0.25 Education level AA and lower (R) BS or higher 0.01 0.07 0.02 0.06 -0.05 0.08 -0.04 0.07 Nursing experience <3 mo (R) 4-6 mo -0.12 0.14 -0.05 0.12 -0.17 ** 0.16 -0.12 0.14 7-12mo -0.12 0.15 -0.07 0.13 -0.16 ** 0.16 -0.12 0.14 1 to 2 yr -0.19 ** 0.12 -0.09 0.10 -0.34 *** 0.13 -0.25 *** 0.12 2 to 3 yr -0.14 0.15 -0.08 0.13 -0.22 *** 0.17 -0.17 *** 0.15 > 3yr -0.31 *** 0.14 -0.11 0.12 -0.45 *** 0.15 -0.28 *** 0.14
Mentor’s nursing ladder
Level I (R)
Level II -0.03 0.13 0.02 0.11 -0.01 0.14 0.04 0.13
Level III 0.14 0.12 0.12 0.10 0.14 0.13 0.13 0.12
Level IV 0.08 0.12 0.07 0.11 0.06 0.13 0.06 0.12
Level V -0.01 0.19 0.00 0.17 0.03 0.21 0.04 0.19
Mentoring period (Mo) -0.06 0.01 -0.06 0.01 -0.03 0.01 -0.03 0.01
Mentor had been trained for mentoring
No (R)
Yes -0.04 0.16 -0.04 0.14 -0.19 0.18 -0.19 0.16
Unknown -0.11 0.17 -0.05 0.15 -0.22 0.19 -0.16 0.17
Mentor had the
No (R)
Yes 0.11 0.17 -0.02 0.15 0.25 ** 0.19 0.14 0.17
Unknown 0.10 0.19 0.02 0.17 0.24 ** 0.21 0.18 0.19
Frequency of interacting
with the mentor 0.23
*** 0.04 -0.02 0.04 0.21 *** 0.04 0.00 0.04 Mentoring function Role modeling 0.31 *** 0.06 0.26 *** 0.07 Career development 0.30 *** 0.06 0.28 *** 0.07 Psychosocial support 0.05 0.05 0.03 0.06 R2 0.15 0.39 0.18 0.36 Adj.R2 0.09 0.34 0.12 0.30 F Change 2.47 *** 36.81 *** 3.13 *** 25.55 *** a
Standardized regression coefficients are shown in the table ** p < .05;*** p <.01; (R) reference group