Kaohsiung J Med Sci October 2005 • Vol 21 • No 10 475 Epidermoid cysts can be classified as either congenital or
acquired [1]. Congenital types are thought to develop from congenital inclusions of ectodermal tissue during embryologic development, whereas acquired variants are believed to originate through implantation of epithelium, by either surgical or accidental trauma into deeper mesenchymal tissues [1]. Congenital and acquired varieties of epidermoid cysts cannot be differentiated microscopically or histopathologically. In both types, the wall of the keratin-filled cyst is lined by keratinizing stratified squamous epithelium, lacking skin appendages in the cystic wall [1]. Mucoceles are typically the result of traumatic damage to a duct and obstruction to the drainage of a minor salivary gland [2]. Whereas both acquired (implantation-type) epidermoid cysts and mucoceles have been described individually in the literature [1,2], their concomitant occurrence has not yet been documented, either at the same site or at different locations. Herein, we report on an uncom-mon and interesting case of simultaneous epidermoid cyst and mucocele occurrence in the lower labial mucosa.
C
ONCURRENT
E
XTRAVASATION
M
UCOCELE
AND
E
PIDERMOID
C
YST
OF
THE
L
OWER
L
IP
: A C
ASE
R
EPORT
Wen-Chen Wang,Li-Min Lin, Yee-Hsiung Shen,1 Yu-Ju Lin, and Yuk-Kwan Chen
Departments of Oral Pathology and 1Oral and Maxillofacial Surgery, Kaohsiung Medical University Chun-Ho Memorial Hospital, School of Dentistry, College of Dental Science,
Kaohsiung Medical University, Kaohsiung, Taiwan.
An uncommon case of concurrent extravasation mucocele and epidermoid cyst in the lower lip of a 13-year-old boy is described. To our knowledge, there is no other report of such a concurrence, neither at the same site nor at different locations, involving these two lesions in the oral mucosa.
Key Words: epidermoid cyst, lip, mucocele (Kaohsiung J Med Sci 2005;21:475–9)
Received: May 4, 2005 Accepted: June 23, 2005 Address correspondence and reprint requests to: Dr. Yuk-Kwan Chen, Department of Oral Pathology, School of Dentistry, College of Dental Science, Kaohsiung Medical University, 100 Shih-Chuan 1st Road, Kaohsiung, Taiwan.
E-mail: [email protected]
C
ASEP
RESENTATIONA 13-year-old boy presented to the Oral and Maxillofacial Surgery Department of our institution, complaining of a painless, non-tender swelling over the left lower lip that had been present for approximately 1 year (Figure 1). The patient’s medical and family history were unremarkable, and, other than his habitual lower-lip biting, he was in good health. On clinical examination, the lesion was found to be a soft, non-tender, fluctuant, round submucosal swelling, approximately 1 cm in diameter. No submental or submandibular lymph nodes were palpable.
Figure 1. A dome-shaped swelling is noted over the left lower lip of the
W.C. Wang,L.M. Lin, Y.H. Shen, et al
The clinical findings were suggestive of an extravasation mucocele over the lower lip, and differential diagnoses included an epidermoid cyst, a minor salivary gland tumor, a lipoma or a lymphoid nodule. The lesion was completely removed by excisional biopsy, via a horizontal incision in the lower labial mucosa, while under local anesthesia. The specimen was sent to the Oral Pathology Department for histopathologic examination.
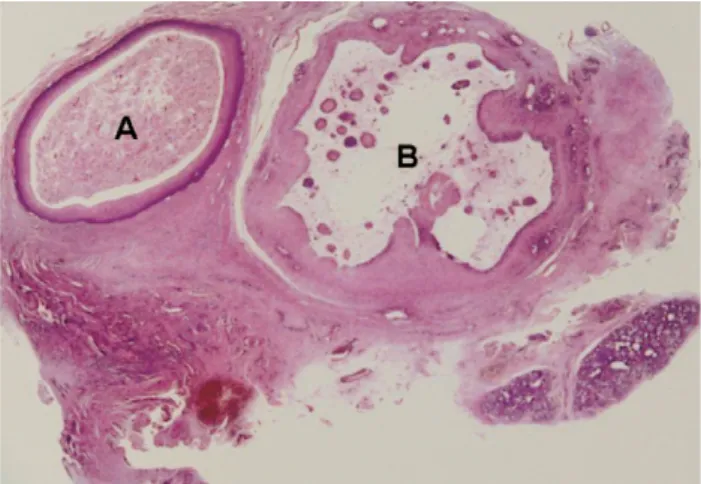
The lesion was found to contain two cystic cavities on low power microscopic examination (Figure 2). One of the
cavities was a fibrous-walled cyst, completely lined by keratinizing stratified squamous epithelium and with no skin adenexae evident in the cystic wall (Figure 3A). Immunohistochemical staining revealed that the lumen was filled with degenerating parakeratin (Figure 4A) and a histologic diagnosis of epidermoid cyst was made. Microscopic examination of the other cavity of the lesion identified a luminal area containing mucin, as demonstrated by mucicarmine histochemical staining (Figure 4B), and chronic inflammatory cells surrounded by a rim of granulation tissue (Figure 2). No true epithelial lining was observed (Figure 3B). Some minor salivary gland acini were also found (Figure 2). A histologic diagnosis of extravasation mucocele was made. Thus, the final diagnosis was one of an epidermoid cyst and concomitant mucocele of the lower lip. Furthermore, the epidermoid cyst was observed to be on the far side of the extravasation mucocele from the minor salivary gland acini (Figure 2). No recurrence was noted 2 years after total excision.
D
ISCUSSIONSkin appendages in the cyst’s connective tissue wall seen on microscopic examination are what distinguish dermoid cysts from epidermoid cysts. The reported lesions of epidermoid cyst do not have the skin appendages [2]. Epidermoid and dermoid cysts of the head and neck constitute only about 7% of all such cysts.
Some (25%) of these head and neck cysts develop in the floor of the mouth, with the remainder generally found in the tongue, lips, palate and jaws [3,4]. Epidermoid cysts of
Figure 2. A low power photomicrograph shows the specimen and the two
cystic lesions (A and B). Lesion A is a fibrous-walled cyst, completely lined by keratinizing stratified squamous epithelium, whereas lesion B has a lumen containing mucus and chronic inflammatory cells that are surrounded by a rim of granulation tissue. Note that lesion A is located on the far side of lesion B, from the minor salivary gland acini. Some ingrowth of the wall into the lumen of lesion B is also shown (hematoxylin & eosin, =10).
Figure 3. (A) No skin adenexae are present in the cystic wall of cystic lesion A. The lumen is filled with degenerating parakeratin (hematoxylin
& eosin, =100); (B) no true epithelial lining is observed in the cystic lesion B. The lumen contains mucus and chronic inflammatory cells (hematoxylin & eosin, =100).
traumatic origin are typically reported on the palms, fingers and soles [5]. Only a small number of cases with authentic evidence of trauma have been described in oral and perioral soft tissues, namely, four in the mouth floor [6–9], four in the lower lip [1,6,10,11], and one in the tongue [12]. All of the previously reported cases exhibited a firm, fluctuating swelling and were predominantly in males [1,6–12].The present case was, therefore, generally in keeping with previously reported cases [1,6–12].
Extravasation mucoceles are usually the result of traumatic damage to a duct and obstruction to the drainage of a minor salivary gland [13]. They typically present as a dome-shaped mucosal swelling and are common in children, owing to their likelihood of experiencing trauma [13]. The lower lip is the most common site, accounting for at least 75% of presentations. Less common sites include the buccal mucosa, anterior ventral tongue and mouth floor [13].The findings of our patient were quite consistent with previous reports in the literature.
Whereas both acquired epidermoid cysts and extravasation mucoceles have been described individually in the literature [1,13], their concomitant occurrence, either at the same site or different locations, has not to our knowledge been previously documented. As both entities share a common traumatic etiology, nothing would prevent both types of lesions to occur simultaneously. In our patient, it was unclear whether the two lesions developed simultaneously or if one preceded the other.
Microscopically, the epidermoid cyst was located on the far side of the extravasation mucocele from the minor salivary gland acini, and hence it appears likely that the length of duct between the mucocele and the surface of the oral mucosa was the origin of the epidermoid cyst.
Figure 4. (A) Immunohistochemical staining shows that the lumen of the epidermoid cyst is filled with parakeratin (avidin–biotin–peroxidase
complex, =100); (B) the luminal area of extravasation mucocele shows the presence of mucin (mucicarmine, =100).
Furthermore, there were ingrowths of the wall into the lumen of the extravasation mucocele, suggesting that the wall has limited the spread of mucus, and reduced the size of the ductal lumen. This supports the suggestion of an absence of mucus in the proximal duct section.
If the wall of an extravasation mucocele completely prevents the flow of mucus along this part of the duct, the epithelial lining of the duct could conceivably proliferate and develop an epidermoid cyst. A related phenomenon has been shown by Harrison [14], who described the squamous metaplasia of the length of a duct associated with mucocele. Therefore, based on the aforementioned microscopic findings, it seems reasonable to predict that the extravasation mucocele would have been formed prior to the epidermoid cyst.
From observation during excisional biopsy and examination of the excised gross specimen, both lesions had no connection to the skin of the chin area. This point of view was further confirmed on multiple sections of the specimen. Therefore, we were confident that the epidermoid cyst had developed along the duct, between the mucocele and the surface of the lower lip mucosa.
R
EFERENCES1. Ettinger RL, Manderson RD. Implantation keratinizing epidermoid cysts. Oral Surg Oral Med Oral Pathol 1973;36: 225–30.
2. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and
Maxillofacial Pathology. Phildadelphia: WB Saunders, 2002;
31–3.
3. Brown CA, Baker RD. Dermoid cyst: Report of a case. J Oral
W.C. Wang,L.M. Lin, Y.H. Shen, et al
4. Rontal E, Adams GL, Boies LR. Cysts in the floor of the mouth.
Minn Med 1971;54:829–31.
5. Epstein WL, Kligman AM. Epithelial cysts in buried human skin. Arch Dermatol 1957;76:437–45.
6. Sanchez Torres J, Higa TT. Epidermoidal cysts in the oral cavity. J Oral Surg 1970;30:592–600.
7. Kelln EE. Oral epidermal cysts and probable histogenesis.
Oral Surg Oral Med Oral Pathol 1965;19:359–64.
8. Zielinski DE. Epidermoid cyst: report of a case. J Am Dent
Assoc 1972;84:153–5.
9. De Ponte FS, Brunelli A, Marchetti E, Bottini DJ. Sublingual
epidermoid cyst. J Craniofac Surg 2002;13:308–10.
10. Papanayotou PH, Kayavis JG. Epidermoid implantation cyst of the lower lip: report of a case. J Oral Surg 1977;35:585–6. 11. Kuroyanagi K, Kawabata T, Tooi M. Epidermoid cyst of the
upper lip: report of a case. Bull Tokyo Dent Coll 1973;14:95–8. 12. Akerson H, Milford ML. Epidermoid cyst of the tongue:
report of a case. J Oral Surg 1974;32:117–20.
13. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and
Maxillofacial Pathology. Philadelphia: WB Saunders, 2002:
389–91.