行政院國家科學委員會專題研究計畫 成果報告
搜尋僵直性脊椎炎相關的克雷白氏菌抗原因子
計畫類別: 個別型計畫
計畫編號: NSC93-2320-B-040-030-
執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 中山醫學大學醫學研究所
計畫主持人: 魏正宗 共同主持人: 賴怡琪
報告類型: 精簡報告
處理方式: 本計畫可公開查詢
中 華 民 國 94 年 10 月 31 日
表 C001 共 1 頁 第 1 頁
行 政 院 國 家 科 學 委 員 會 專 題 研 究 計 畫 申 請 書
一、基本資料: 申請條碼:93WFD2500167
*93WFD2500167*
本 申 請 案 所 需 經 費 ( 單 選 ) A 類(研究主持費及執行計畫所須經費)
計 畫 類 別 ( 單 選 ) 一般型研究計畫
研 究 型 別 個別型計畫
計 畫 歸 屬 生物處
申 請 機 構 / 系 所 ( 單 位 ) 中山醫學大學 醫學系
本 計 畫 主 持 人 姓 名 魏正宗 職 稱 臨床講師 身 分 證 號 碼 *******894
中 文 搜尋僵直性脊椎炎相關的克雷白氏菌抗原因子
本 計 畫 名 稱
英 文 Identification and Characterization of Ankylosing Spondylitis Associated K. pneumoniae Antigens
整 合 型 總 計 畫 名 稱
整 合 型 總 計 畫 主 持 人 身 分 證 號 碼
全 程 執 行 期 限 自民國 93 年 08 月 01 日起至民國 96 年 07 月 31 日
學 門 代 碼 名 稱(如為其他類,請自行填寫學門) 研究學門(請參考本申請書所
附 之 學 門 專 長 分 類 表 填 寫 )
BI 微生物及免疫學
研 究 性 質 基礎研究
本年度申請主持國科會各類研究計畫(含預核案)共 2 件。(共同主持之計畫不予計入) 本件在本年度所申請之計畫中優先順序(不得重複)為第 1 。
本計畫是否為國際合作計畫:否
本計畫是否申請本會吳大猷先生紀念獎:否
本計畫是否申請本會傑出研究獎:否
本計畫是否申請海洋研究船:否
本計畫是否有進行下列實驗:(勾選下列任一項,須附相關實驗之同意文件)
基因重組實驗
計 畫 連 絡 人 姓名: 魏正宗 電話:(公) 04 24739595 # 4714 (宅/手機) 0931 227420 通 訊 地 址 台中市 402 南區建國北路一段 110 號
傳 真 號 碼 04 24637389 E-MAIL: [email protected]
計畫主持人(申請人)簽章: 日期:
表 C002 共 1 頁 第 1 頁
二、申請補助經費:
(一)請將本計畫申請書之第四項(表 C004)、第五項(表 C005)、第六項(表 C006)、第七項(表 C007)、第 八項(表 C008)所列費用個別加總後,分別填入「研究人力費」、「研究設備費」、「其他研究費用」、
「赴國外或大陸地區差旅費」及「出席國際學術會議差旅費」欄內。
(二)管理費為申請機構配合執行本計畫所需之費用,請按上述第(一)點費用總和(不含出席國際學 術會議差旅費及專任助理之雇主應負擔勞健保費)之最高 10%計算後直接填入「管理費」欄。
(三)「國際合作研究計畫差旅費」指若有申請國際合作研究計畫差旅費者,請將表 I002 之「合計」欄 金額填入;本項費用不核列管理費。
(四)「貴重儀器中心使用額度」係將第九項(表 C009)所列使用費用合計數填入。
(五)請依各年度申請博士後研究之名額填入下表。
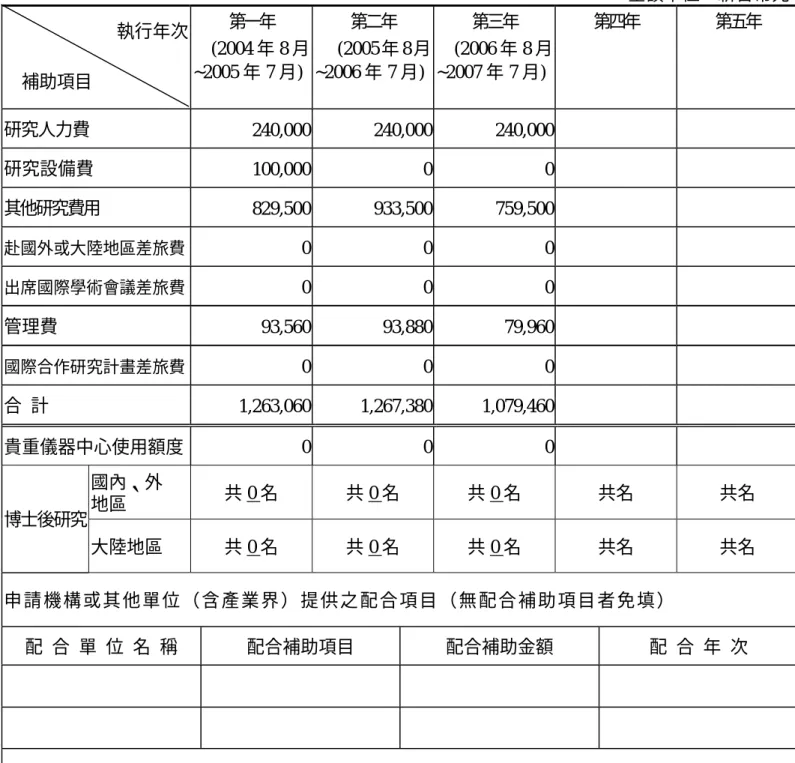
金額單位:新台幣元 執行年次
補助項目
第一年 (2004 年 8 月
~2005 年 7 月)
第二年 (2005 年 8 月
~2006 年 7 月)
第三年 (2006 年 8 月
~2007 年 7 月)
第四年 第五年
研究人力費 240,000 240,000 240,000
研究設備費 100,000 0 0
其他研究費用 829,500 933,500 759,500
赴國外或大陸地區差旅費 0 0 0
出席國際學術會議差旅費 0 0 0
管理費 93,560 93,880 79,960
國際合作研究計畫差旅費 0 0 0
合 計 1,263,060 1,267,380 1,079,460
貴重儀器中心使用額度 0 0 0
國內、外
地區 共 0 名 共 0 名 共 0 名 共名 共名
博士後研究
大陸地區 共 0 名 共 0 名 共 0 名 共名 共名
申 請 機 構 或 其 他 單 位 ( 含 產 業 界 ) 提 供 之 配 合 項 目 ( 無 配 合 補 助 項 目 者 免 填 )
配 合 單 位 名 稱 配合補助項目 配合補助金額 配 合 年 次
配合單位主管簽章(或附相關證明文件):
表 C003 共 1 頁 第 1 頁
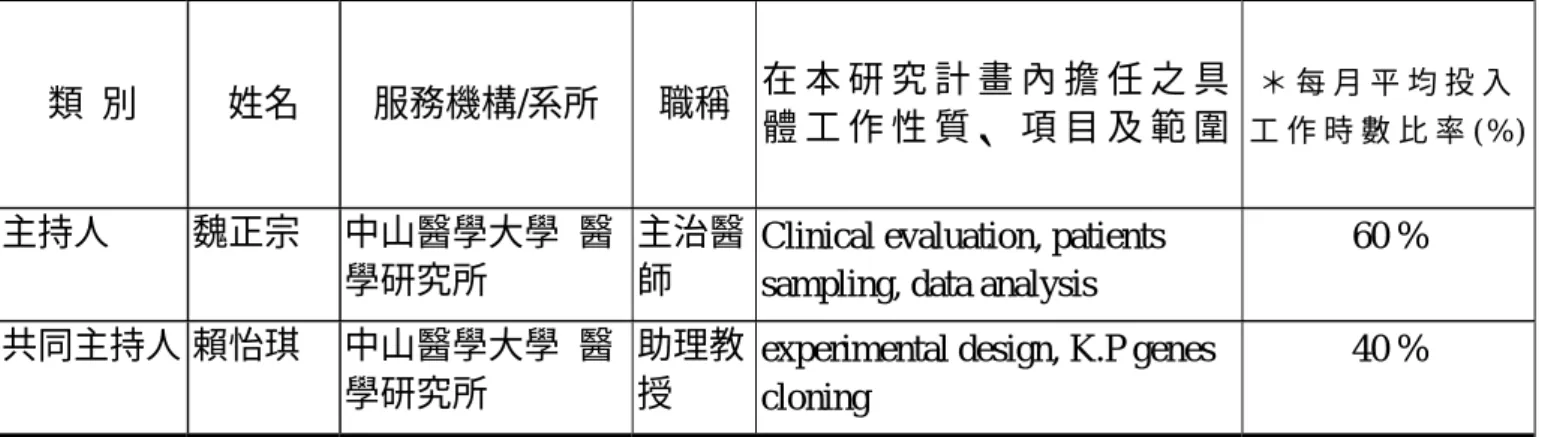
三、主要研究人力:
(一)請依照「主持人」、「共同主持人」、「協同研究人員」及「博士後研究」等類別之順序 分別填寫。
類 別 姓名 服務機構/系所 職稱 在 本 研 究 計 畫 內 擔 任 之 具
體 工 作 性 質 、 項 目 及 範 圍
* 每 月 平 均 投 入 工 作 時 數 比 率 ( % )
主持人 魏正宗 中山醫學大學 醫
學研究所
主治醫 師
Clinical evaluation, patients sampling, data analysis
60 % 共同主持人 賴怡琪 中山醫學大學 醫
學研究所
助理教 授
experimental design, K.P genes cloning
40 %
※註:每月平均投入工作時數比率係填寫每人每月平均投入本計畫工作時數佔其每月全部工作時 間之比率,以百分比表示(例如:50%即表示該研究人員每月投入本計畫研究工作之時數佔 其每月全部工時之百分五十)。
(二)如申請博士後研究,請分年列述博士後研究參與本研究計畫之 1.目的及必備之專長。
2.研究項目。
3.工作份量及其對該計畫之影響程度。
4.工作績效評估準則。
5.若已有人選者,請務必填註人選姓名,並將其個人資料表併同本計畫書送本會。
表 C004 共 2 頁 第1頁
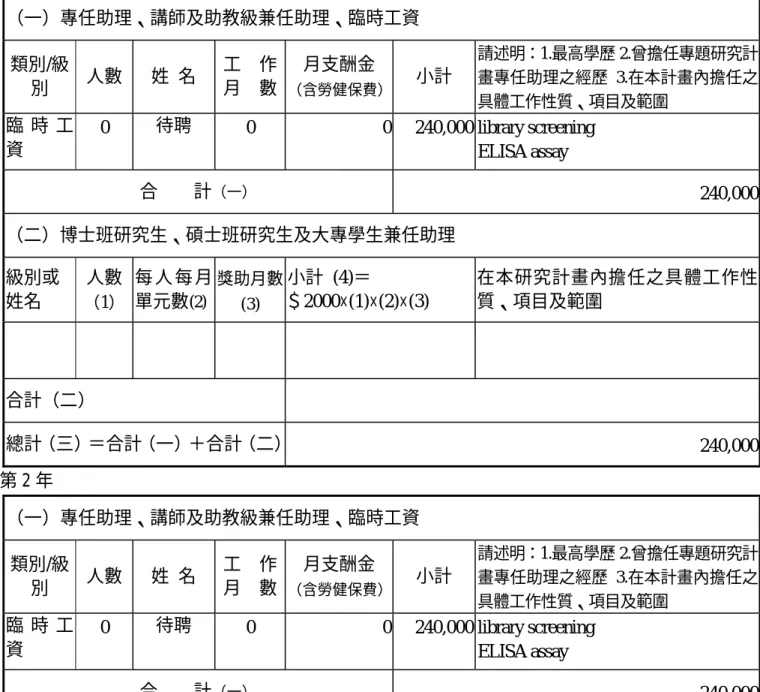
四、研究人力費:
(一) 類別/級別欄請依專任助理(含碩士、學士、三專、五(二)專及高中職)、兼任助理(含博士生、
碩士生、大專學生、講師及助教)及臨時工等填寫。
(二) 專任助理及兼任助理之每月工作酬金標準,不得超過本會補助專題研究計畫助理人員工作 酬金支給標準表之規定。
(三) 九十年以後獲本會碩士論文獎或大專學生研究創作獎者,於本會公布獲獎之日起三年內就 讀國內公私立大專校院博士班或碩士班,並參與本計畫研究工作,申請每月博士班研究獎 助金 28,000 元或碩士班研究助學金 10,000 元部分請務必於級別或姓名欄填列姓名,並檢 附得獎證明影本及學生證正反面影本,以利審核。
(四) 申請專任助理者,除依工作月數填列工作酬金及至多 1.5 個月年終工作獎金外,須另填列
投保勞保及健保之「雇主應負擔之勞、健保費」(可至本會網站下載)。
(五) 請分年列述。
金額單位:新台幣元 第 1 年
(一)專任助理、講師及助教級兼任助理、臨時工資 類別/級
別 人數 姓 名 工 作 月 數
月支酬金
(含勞健保費) 小計
請述明:1.最高學歷 2.曾擔任專題研究計 畫專任助理之經歷 3.在本計畫內擔任之 具體工作性質、項目及範圍
臨 時 工 資
0 待聘 0 0 240,000 library screening
ELISA assay
合 計(一) 240,000
(二)博士班研究生、碩士班研究生及大專學生兼任助理 級別或
姓名
人數
(1)
每 人 每 月 單元數(2)
獎助月數 (3)
小計 (4)=
$2000×(1)×(2)×(3)
在本研究計畫內擔任之具體工作性 質、項目及範圍
合計(二)
總計(三)=合計(一)+合計(二) 240,000
第 2 年
(一)專任助理、講師及助教級兼任助理、臨時工資 類別/級
別 人數 姓 名 工 作 月 數
月支酬金
(含勞健保費) 小計
請述明:1.最高學歷 2.曾擔任專題研究計 畫專任助理之經歷 3.在本計畫內擔任之 具體工作性質、項目及範圍
臨 時 工 資
0 待聘 0 0 240,000 library screening
ELISA assay
合 計(一) 240,000
表 C004 共 2 頁 第2頁
(二)博士班研究生、碩士班研究生及大專學生兼任助理 級別或
姓名
人數
(1)
每 人 每 月 單元數(2)
獎助月數 (3)
小計 (4)=
$2000×(1)×(2)×(3)
在本研究計畫內擔任之具體工作性 質、項目及範圍
合計(二)
總計(三)=合計(一)+合計(二) 240,000
第 3 年
(一)專任助理、講師及助教級兼任助理、臨時工資 類別/級
別 人數 姓 名 工 作 月 數
月支酬金
(含勞健保費) 小計
請述明:1.最高學歷 2.曾擔任專題研究計 畫專任助理之經歷 3.在本計畫內擔任之 具體工作性質、項目及範圍
臨 時 工 資
0 待聘 0 0 240,000 library screening
ELISA assay
合 計(一) 240,000
(二)博士班研究生、碩士班研究生及大專學生兼任助理 級別或
姓名
人數
(1)
每 人 每 月 單元數(2)
獎助月數 (3)
小計 (4)=
$2000×(1)×(2)×(3)
在本研究計畫內擔任之具體工作性 質、項目及範圍
合計(二)
總計(三)=合計(一)+合計(二) 240,000
表 C005 共 1 頁 第 1 頁
五、研究設備費:
(一) 凡執行研究計畫所需單價在新台幣一萬元以上且使用年限在二年以上之各項儀器、機械 及資訊設備(含各項電腦設施、周邊設備及套裝軟體、程式設計費)等之購置、裝置費 用及圖書館典藏之分類圖書等屬之,此項設備之採購,以與本研究計畫直接有關者為限。
各類研究設備金額請於金額欄內分別列出小計金額。
(二) 設備名稱欄內請填寫儀器、機械、資訊硬體及軟體或圖書等之中文/英文名稱。
(三) 說明欄內請詳細填寫設備之規格、製造廠商、型號及用途,以利審查,若為圖書設備,
則於說明欄內填寫作者姓名、出版社及出版日期。
(四) 購置設備單價在新臺幣二十萬元以上者,須檢附估價單。
(五) 若申請機構及其他機構有提供配合款,請務必註明提供配合款之機構及金額。
(六) 儀器設備單價超過六十萬元(含)以上者,請詳述本項設備之規格與功能(諸如靈敏度、精 確度…等),其他重要特性與重要附件,以及申購本設備對計畫執行之必要性。本項設備 若獲補助,主持人應負維護保養之責,並且在不妨礙個人研究計畫或研究群計畫之工作 下,同意提供他人共同使用,以避免設備閒置。
(七) 請分年列述。
第 1 年 金額單位:新台幣元 經費來源
類別 設備名稱
(中文/英文) 說 明 數 量 單 價 金 額 本會補助
經費需求
提供配合款之機 構名稱及金額 儀器及資
訊設備
蛋白質電泳設 備
1 100,000 100,000 100,000
合 計 100,000 100,000 第 2 年
經費來源
類別 設備名稱
(中文/英文) 說 明 數 量 單 價 金 額 本會補助
經費需求
提供配合款之機 構名稱及金額
合 計 第 3 年
經費來源
類別 設備名稱
(中文/英文) 說 明 數 量 單 價 金 額 本會補助
經費需求
提供配合款之機 構名稱及金額
合 計
表C006 共 3 頁 第 1 頁
六、其他研究費用:
(一) 凡執行研究計畫所需之消耗性器材、化學藥品、電腦使用費、問卷調查費、儀器安裝保 險與運雜費、儀器維護費、印刷與影印費、文具、紙張、郵電費、資料檢索費、國內差 旅費、國內研討會報名費或註冊費(不含學會之年費或入會費)、意外險保險費、論文
發表費(限國科會補助計畫之成果)、人體試驗委員會審查費、受試者禮品費或營養費、
專家諮詢費或出席費、儀器或電腦軟體租用費、物品(使用年限未及二年或金額未達新 台幣一萬元)及其他與研究計畫直接有關之費用等,均可填入本表內。
(二) 說明欄請就該項目之規格、用途等相關資料詳細填寫,以利審查。
(三) 若申請單位有配合款,請於備註欄註明。
(四) 請分年列述。
第 1 年 金額單位:新台幣元
項 目 名 稱 說明 單位 數量 單價 金額 備註
消耗性器材 chemicals set 1 80,000 80,000
消耗性器材 plastic (tips, tubes, plates)
case 20 5,000 100,000 消耗性器材 Western reagents set 5 5,000 25,000
消耗性器材 E. coli expression system
set 1 60,000 60,000 消耗性器材 Restriction enzyme set 10 2,450 24,500 消耗性器材 PCR matrix mixture set 6 10,000 60,000
消耗性器材 colony hybridization membrane
box 20 3,500 70,000 消耗性器材 DNA sequencing Rxn 800 450 360,000
雜支 Domestic travel and symposium attendance
1 10,000 10,000 雜支 Lab maintenance 1 40,000 40,000
合 計 829,500
第2年
項 目 名 稱 說明 單位 數量 單價 金額 備註
表C006 共 3 頁 第 2 頁 消耗性器材 Antibody set 5 10,000 50,000
消耗性器材 Restriction enzyme set 10 2,450 24,500 消耗性器材 PCR matrix mixture set 6 10,000 60,000 消耗性器材 ELISA plates box 20 6,000 120,000 消耗性器材 chemicals set 1 80,000 80,000
消耗性器材 plastic (tips, tubes, plates)
case 20 5,000 100,000 消耗性器材 Western reagents set 5 5,000 25,000
消耗性器材 mice 300 80 24,000
消耗性器材 affinity column set 20 20,000 400,000
雜支 Domestic travel and symposium attendance
1 10,000 10,000 雜支 Lab maintenance 1 40,000 40,000
合 計 933,500
第3年
項 目 名 稱 說明 單位 數量 單價 金額 備註
消耗性器材 Restriction enzyme set 10 2,450 24,500 消耗性器材 PCR matrix mixture set 6 10,000 60,000 消耗性器材 chemicals set 1 80,000 80,000
消耗性器材 plastic (tips, tubes, plates)
case 20 5,000 100,000
消耗性器材 Western reagents set 5 5,000 25,000 消耗性器材 ELISA plates case 20 6,000 120,000
表C006 共 3 頁 第 3 頁 消耗性器材 tissue staining set 1 50,000 50,000
消耗性器材 collagen bottle 5 10,000 50,000 消耗性器材 proteomics analysis 10 20,000 200,000
雜支 Domestic travel and symposium attendance
1 10,000 10,000 雜支 Lab maintenance 1 40,000 40,000
合 計 759,500
關鍵詞:僵直性脊椎炎,克雷白氏肺炎菌,IVIAT,HLA-B27 中文摘要:
僵直性脊椎炎(Ankylosing Spondylitis; AS)是一種主要侵襲脊椎的發炎性 疾病。文獻報導以及研究發現 AS 患者血清具有對抗克雷白氏肺炎菌(Klebsiella pneumoniae)的抗體反應,而在 HLA-B27 分子以及細菌抗原之間具有分子相似
(molecular mimicry)片段。在本計畫中我們將建構 IVIAT (In Vivo Inducible Antigen Technology)系統,利用此系統搜尋對 HLA-B27 陽性 AS 病患的血清具有 免疫反應的 K. pneumoniae 抗原。接著再以 Bioinformatics 的軟體工具以及 ELISA 分析這些 K. pneumoniae 抗原對 AS 的免疫反應性以及其抗原特異區域。爲能進 一步了解這些抗原引發的免疫反應在 AS 病程中的重要性,我們將大量表達這些 具有高度免疫反應性的 K. pneumoniae 抗原蛋白,再利用純化所得的蛋白置備特 異的小鼠抗血清。藉由免疫組織染色分析法(immunohistochemical analysis),
這些具有 K. pneumoniae 抗原特異性的小鼠抗血清將可幫助我們找到存在於 AS 患病組織中的自體免疫因子。此外,我們亦會針對 K. pneumoniae 抗原與人類組 織膠原蛋白之間可能存在的交叉反應性(cross-reactivity)進行測試。我們相信 藉由本研究計畫的完成,對於 K. pneumoniae 感染在 AS 疾病進程中所扮演的角 色將有更清楚的了解;而這些在 K. pneumoniae,HLA-B27,以及 AS 患病組織 中彼此共有的 peptide 分子將可提供為開發自體免疫藥物的設計平台。
Keywords:
Ankylosing spondylitis; Klebsiella pneumoniae; IVIAT; HLA-B27Abstract:
Ankylosing spondylitis (AS) is an inflammatory disorder that primarily affects the axial skeleton. Some evidences indicated that Klebsiella pneumoniae might be related to the trigger or pathogenesis of AS. Anti-Klebsiella antibodies and the presence of molecular mimicry between the HLA-B27 molecule and bacterial antigens had been reported. In this project, we will initiate an IVIAT (in vivo
inducible antigen technology)-based approach to identify K. pneumoniae antigens that are immunoreactive to the serum of HLA-B27 positive AS patients. Antigenicity and immunoreactivity of the AS-associated K. pneumoniae antigens identified will be determined using bioinformatics analysis and ELISA assay. The highly AS- responsive K. pneumoniae clones will be selected for large-scale expression and generation of polyclonal antibodies. Tissue-specific antigens present in the infected sites of AS patients that may serve as targets for autoreactive T cells will be identified by immunohistochemical analysis with the generated K. pneumoniae antibodies.
Furthermore, the cross-reactivity between AS-associated K. pneumoniae antigens and human collagens will be examined. The possibly coexisted epitopes present in the K.
pneumoniae antigens, HLA-B27, and infected tissues such as human collagens, will be analyzed using bioinformatics tools. We expect the results obtained from this study will contribute significantly toward the understanding of the pathogenic role of K.
pneumoniae in the development of AS disease. Potential useful peptide targets will be obtained which may lead to the identification of novel anti-autoimmune drugs.
Research Plan
I. Main research results:
The P.I., Dr James Cheng-Chung Wei, is a attending physician and lecturer of Chung Shan medical university. After his training of rheumatology and clinical immunology at Taichung and Kaohsiung veterans general hospital, he went to Royal National Hospital for Rheumatic Diseases (RNHRD) for clinical fellowship under Dr Andrei Calin, the world’s famous master in ankylosing spondylitis (AS) in 2000. In 2001, he went to UCLA rheumatology department as a research fellowship under Dr David Yu to investigate the pathogenesis of spondyloarthropathy. Before present position, he was the chief of family medicine department of Chia Yi veterans hospital.
He organized the ankylosing spondylitis caring society in Taiwan and had been the president of the society.
Dr Wei’s research interests included clinical and basic researches in ankylosing spondylitis. He conducted the first HLA-B27 subtyping study.(HLA-B27 subtypes in Chinese with ankylosing spondylitis and normal controls. J. of Rheumatology. Vol 25, suppl 54: 27, 1998 Aug.)。 He also find the association of AS with HLA-B60 and B61.(HLA-A, B ANTIGENS IN HLA-B27 NEGATIVE ANKYLOSING
SPONDYLITIS PATIENTS IN TAIWAN. Journal of Rheumatology – Suppl 59:1-62, 2000 Aug, complete paper submitted in 2003)。 In 2001, he and collaborators develop a new immunomagnetic separation (IMS)-sandwich ELISA technique to detect HLA-B27 antigen. (Development of immunomagnetic separation (IMS) - sandwich ELISA for the HLA-B27 antigen detection. J. Immunol Methods. 2001 Aug.)。In 2003, he published a pilot clinical trial on thalidomide in AS patients.
(Thalidomide for Severe Refractory Ankylosing Spondylitis. Journal of
Rheumatology 2003;30:2627-31). He was also invited to write a review article for Clinical & Experimental Rheumatology(Thalidomide in Ankylosing Spondylitis.
Clinical and Experimental Rheumatology. 2002. supp 28, s-158-61)。
Recently, he is working on traditional Chinese medicine trial in AS patients and the validation of some clinical indices in AS.
The co-PI has been working on the pathogenesis of Klebsiella
pneumoniae. Her group is familiar with bacterial genetic analysis techniques and
has established several virulence gene identification approaches, including DNA subtractive hybridization, in vivo expression technology (IVET), and signature- tagged mutagenesis. More than 40 virulence-associated genes have been identified with these techniques. Four articles concerning the results have been published (23-26).
We believe that all these previous experience and efforts will ensure the success of this project.
II. Preliminary study:
1. Collection of AS sera and biopsies
Patients population
Patients in Chung Shan medical university fulfilling the modified New York criteria(1984) for AS were recruited after written informed consent was obtained.
Patients’ seri and tissues from synovium and enthesis were sampled simultaneously with the clinical indices and laboratory tests. Seri and tissue samples were stocked in - 80 degree refrigerators.
Clinical assessments were performed by the same investigator including patient- reported global pain intensity over the past 7 days (recorded using a 100-mm VAS) and patient-reported activity and functional impairment (according to the Bath Ankylosing Spondylitis Disease Activity Index [BASDAI] and Bath Ankylosing Spondylitis Functional Index [BASFI]), Finger to floor test, Schober test, chest expansion test, occipital to wall test, lateral bending test. Laboratory assessment include complete blood count (CBC), liver and renal function, erythrocyte
sedimentation rate (ESR), C-reactive protein (CRP) and immunoglobulin A (IgA) were monitored at each visit of clinical assessments.
Control groups.
Seri samples from healthy normal control and some healthy HLA-B27 carrier subjects were also collected as the control groups.2. Western analysis of AS immunoreactivities against K. pneumoniae. We are interested in the humoral immune responses observed in HLA-B27 positive AS patients that are possibly elicited by the infection of K.
pneumoniae. We performed a preliminary Western analysis by using sera of HLA-B27 positive AS patients as the first antibodies. As shown in Fig. 1, total proteins (30 µg) of the cell lysates prepared from K. pneumoniae CG43
(serotype K2), E. coli XL-1 and S. typhimurium LT2 were separated by SDS- PAGE. After transferred onto PVDF membranes, sera from HLA-B27 positive healthy individuals or from HLA-B27 positive AS patients were added at 4oC for hybridization overnight. Sera from HLA-B27 negative healthy individuals were used as a control in parallel. Alkaline phosphatase (AP)-conjugated anti- human IgG (H+L) antibodies (Promega) were added for another 1 hour at room temperature. AP activity was detected using CDP-Star
chemiluminescence reagent (PerkinElmer) and exposed to a BioMax X-film (Kodak). Since epitopes expressed on the bacterial surface are more likely to be involved in the immune responses, we extracted the extracellular
components of K. pneumoniae CG43 for Western analysis (lane 1; Fig. 1).
Overnight-cultured K. pneumoniae cells (500 µl) was mixed with 100 µl of 1
% Zwittergent 3-14 detergent (Sigma) in 100 mM citric acid (pH 2.0), and incubated at 50°C for 20 min. After centrifugation, 250 µl of the supernatant was transferred to a new tube and extracellular components including capsular polysaccharides were precipitated with 1 ml of absolute ethanol. The pellet was dissolved in 200 µl distilled water.
In comparison with the immunoreactivity of the HLA-B27 negative sera, a significant response to the extracellular components of K. pneumoniae was observed in that of HLA-B27 positive sera either from healthy person or AS patients (as pointed with an arrow in Fig. 1). Except K. pneumoniae, a cross-reactivity to the bacterial lysates of E. coli and S. typhimurium was observed in sera of HLA-B27 positive AS patients. Based on this preliminary result and enormous AS references reported by other groups, we hypothesize that K. pneumoniae has a pathological role in the development of AS disease with an involvement of HLA-B27.
III. Background and Significance:
Ankylosing spondylitis (AS) is the most prominent component of a group of inflammatory arthritides, collectively named as “spondyloarthropathies
(SpAs)”. It is a chronic inflammatory disorder that involves mainly the lumbar spine and sacroiliac joints and less frequently affects the peripheral joints and eye structures such as the uvea. The inflammation can lead to fibrosis and ossification, where bridging spurs of bone known as “syndesmophytes” form, especially at the edges of the intervertebral discs. This form of ossification is primarily seen at the sacroiliac joints and lumbar spine from where it ascends. In extreme cases it can effectively solidify the whole of the vertebrate column. The disease in severe cases can progress to form the classic “bamboo spine” (12). Symptoms of AS first appear most frequently in young men between the ages of 10 and 40. The disease is less common in women, who often have milder symptoms that are more difficult to diagnose.
The causation of AS is largely unknown, but genes and heredity do play a role. The association between AS and HLA-B27 has been well established. The frequency of HLA-B27 in patients with AS ranges from 81 to 96% with control frequencies ranging between 4 and 12%. Rats transgenic for B27 spontaneously develop a chronic inflammatory disease that resembles, both clinically and histologically, the human SpA, while control rats transgenic for HLA-A2 do not develop such an illness (6, 14, 27). The prevalence of AS correlates with the presence of HLA-B27 in all ethnic groups has been studied. African Blacks of unmixed ancestry lack B27 genes and AS is very rare among them. Certain North American Indian tribes who have a high frequency of B27 also have a high prevalence of AS (21). The observations signify the importance of HLA-B27 in the development of AS.
Infections of Klebsiella pneumoniae have been strongly suggested to be a triggering factor of AS. Elevated antibody titers against Klebsiella but not to other microbes could be detected in the sera patients with AS when compared to healthy controls (1, 5, 9, 11, 18, 20, 30, 32). Evidence for molecular mimicry between Klebsiella and HLA-B27 has been shown in several studies (4, 33). An amino-acid sequence homology was identified between HLA-B27 and the K.
pneumoniae nitrogenase reductase enzyme, in that the sequence QTDRED is common to both molecules (28). Rat antisera raised against 16-mer synthetic peptides of K. pneumoniae nitrogenase reductase reacted with synovial biopsies
obtained from HLA-B27 positive AS patients (17). Furthermore, there is extensive evidence to suggest an association between the gut lesions in AS and the coexistence of Klebsiella as the likely triggering agent across the gut mucosa.
HLA-B27 positive individuals, who are suffering from inflammatory bowel disease (IBD) such as Crohn’s disease or ulcerative colitis, have a significantly greater chance of developing AS than HLA-B27 positive individuals not having IBD (34). In a most recent study, patients with AS and Crohn’s disease were found to have elevated levels of IgM, IgG and IgA class-specific antibodies to K.
pneumoniae and to collagens type I, III, IV and V. A positive correlation was observed between K. pneumoniae and collagen antibody levels in these patients (31). These observations support the hypothesis that an important link exists between the infections of Klebsiella and the development of AS.
K. pneumoniae is present as a saprophyte in the human nasopharynx and intestinal tract. It is an important nosocomial pathogen, causes suppurative infection, pneumonia, urinary tract infection and septicemia, occurring
particularly in immunocompromised individuals (7) and has a high fatality rate if untreated. Several virulence factors have been found important in the
pathogenesis of K. pneumoniae, including capsular polysaccharides (3),
lipopolysaccharides (8), adhesins, iron acquisition systems, and several secreted toxins. Despite of these, much of the pathogenesis events in K. pneumoniae are present unclear. In view of the importance of Klebsiella infections with the aetiopathogenesis of AS, we propose to initiate an IVIAT (in vivo inducible antigen technology)-based approach (10, 15, 16) that will lead to the
identification of K. pneumoniae antigens involved in the development of AS disease.
IV. Specific aims:
The study is to be completed in three years. The goal of this project is to identify and characterize the causative K. pneumoniae factors that are involved in the pathogenesis of ankylosing spondylitis (AS). The specific aims are listed chronologically as follows.
The first year
1. Construction of an inducible expression genomic DNA library of K.
pneumoniae
2. Screening for AS-associated K. pneumoniae genes
The second year
1. Bioinformatic analysis of AS-associated K. pneumoniae genes 2. Expression and purification of K. pneumoniae antigens
3. Determination of AS immunoreactivity to the associated K. pneumoniae antigens
4. Generation and purification of reactive AS antibodies against K. pneumoniae antigens
The third year
1. Determination of the cross-reactivity between the AS-associated K.
pneumoniae antigens and putative AS factors
(1) Immunohistochemical analysis of AS synovial tissues.
(2) Immunoreactivity analysis with human collagens.
2. Identification of immunodominant peptides of AS-reactive K. pneumoniae antigens
V. Research design and methods:
We here describe our tentative approaches stepwise as follows.
The first year
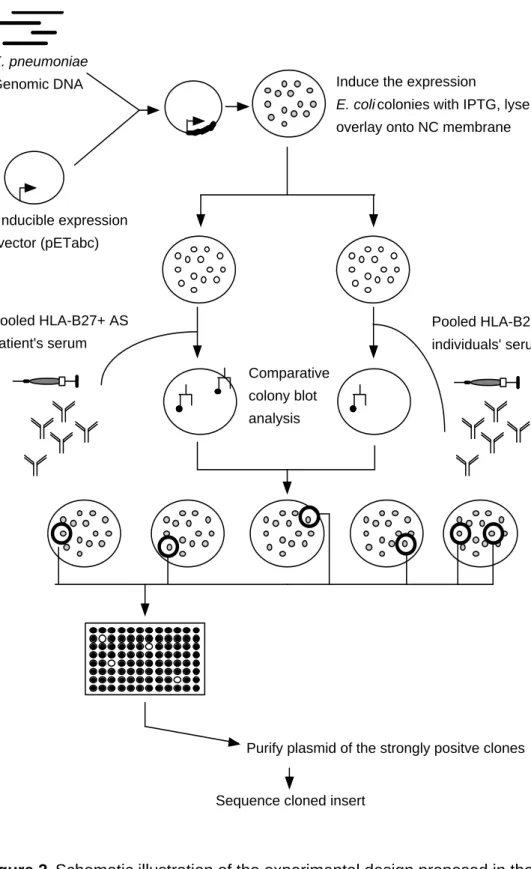
1. Screening for AS-associated K. pneumoniae antigens by using an IVIAT- based approach. In vivo induced antigen technology (IVIAT) is a novel method designed to screen microbial genes that are expressed during an actual human infections rather than in an animal model (15). IVIAT is highly effective and has allowed many infection-associated microbial genes to be identified (10, 16). Based on the IVIAT approach, we will use pooled sera from HLA-B27 positive AS patients to probe K. pneumoniae genes that
specifically expressed in the development of AS disease. The experimental scheme is shown in Fig. 2.
(1) Construction of an inducible expression library of K. pneumoniae.
An inducible expression library of K. pneumoniae will be generated as follows. K. pneumoniae genomic DNA will be purified by a
conventional sodium dodecyl sulfate (SDS)-protease method, partially digested with Sau3AI, and separated by electrophoresis with a low- melting-point agarose gel (Amersham). DNA fragments of ca. 0.5 to 1.0 kb will be cut from the agarose gel and extracted by using the QIAEX II gel extraction kit (Qiagen). The purified DNA inserts will be ligated into the pET30abc expression vectors (Novagen), which will have been cut by BamHI and treated with shrimp alkaline phosphatase (Roche). The resulting ligation mixture will be electroporated into electrocompetent DH5α cells (Gibco-BRL). The transformants will be spread onto LB agar plates containing 50 µg/ml of kanamycin. After overnight incubation, colonies on the plates will be scraped and frozen at –70oC until use. An aliquot of the resulting library will be grown in LB broth, and plasmids will be isolated. The isolated plasmid library DNA will be subsequently electroporated into the expression host E. coli BL21(DE3) (Novagen).
(2) Screening for AS-associated K. pneumoniae genes with sera from HLA-B27 positive AS patients. As illustrated in Fig. 1, the K.
pneumoniae expression library constructed in E. coli BL21(DE3) will be plated onto BHI agar plates containing 50 µg/ml of kanamycin at a density of ca. 1000 colonies per plate. The colonies will be replica plated onto two BHI agar plates with supplement of kanamycin and 1 mM IPTG (isopropyl-β-D-thiogalactopyranoside) to induce the expression of inserted DNA fragments. The colonies will be exposed to chloroform vapors to partially lyse the bacteria and the exposed proteins will be adsorbed onto overlaid HyBond nitrocellulose membranes (Amersham).
The membranes will be carefully removed and saturated with a 5% skim milk solution in phosphate-buffered saline (PBS) containing 0.5%
Tween 20. Comparative colony Western blot analysis will be performed
with the pooled serum of HLA-B27 positive AS patients and the HLA- B27 negative healthy control, respectively as the primary antibody.
Peroxidase-conjugated rabbit antihuman immunoglobulin G (IgG), IgA and IgM (Promega) will be used as the secondary antibody. The positive signals will be detected by using an enhanced chemiluminescence (ECL) and Hyperfilm ECL (Amersham). Reactive clones, which are positive in the blotting with AS sera and negative in the control blotting by parallel, will be collected and retested for reactivity by another round of colony immunoblot analysis. Each colony of the resulting reactive clones will be grown overnight in 96-well culture plates and then replica plated onto BHI agar plates containing kanamycin with or without IPTG. Only the clones showing strong positively at the secondary screening will be regarded to contain putative AS-associated antigens. Inserted DNAs in the positive clones will be sequenced.
The second year
2. Characterization of AS-associated K. pneumoniae antigens. By using bioinformatics analysis and ELISA assay, we will determine the antigenicity and immunoreactivity of the K. pneumoniae genes identified in the first year.
The experimental scheme is shown in Fig. 3.
(1) Bioinformatics analysis of AS-associated K. pneumoniae genes. The nucleotide sequences of the AS-associated K. pneumoniae genes will be analyzed in GenBank database and the genomic sequence database of K.
pneumoniae MGH78578 provided by Washington University with the BLAST programs (2). Based on the homology searches, these AS- associated genes will be assigned to a gene cluster using a microbial genome classification system. Amino acid sequences of the putative AS- associated K. pneumoniae antigens will be deduced and used for a computer analysis of probable antigenic sites. Regions with a high antigenicity index according to Jameson and Wolf (19) and a high probability of containing turns based on secondary structure predictions (13) will be identified.
(2) Determination of the immunoreactivity of the identified K.
pneumoniae antigens with AS patient sera. Levels of IgG, IgA and IgM antibodies of AS patients to each of the putative K. pneumoniae antigens will be evaluated by ELISA assay. These putative AS- associated K. pneumoniae genes will be expressed and purified by affinity chromatography with the His-Bind resin (Novagen). These purified K. pneumoniae antigen proteins will be coupled covalently to 96-well assay plates at 1 µg/well. Sera collected from AS patients will be diluted and incubated for 1.5 h at room temperature. Sera from healthy individual will be introduced to serve as the controls. After washing, 100 µl of anti-human class-specific IgG, IgA, or IgM
conjugated to peroxidase will be added. After incubation, plates will be washed, and bound antibodies will be detected with 3,3-5,5- tetramethyl- benzidine and read at a wavelength of 450 nm. All sera will be tested in triplicate, and the results will be averaged. Differences in
immunoglobulin class levels against the various K. pneumoniae antigens in the serum samples of AS patients will be assessed by comparing the proportion in each group having OD units greater than the 95%
confidence limits for the population of controls (one-tailed test) using the χ2 test, with Yates correction (significance will be taken at P < 0.05).
3. Generation and purification of AS-reactive antibodies
(1) Generation of polyclonal antibodies for AS-associated K.
pneumoniae antigens. The AS-associated K. pneumoniae antigens that present a strong immunoreactivity to the AS sera will be selected to generate polyclonal antibodies for further studies. Female BALB/c mice (six to eight weeks of age) will be immunized with the following
schedule. The mice will receive 25 µg of K. pneumoniae antigen i.p. on days 0 and 14 and pristine on days 3 and 17; on day 21 blood samples will be taken for assessing the course of immunization. At day 28, the mice will be given a third i.p. dose of K. pneumoniae antigen, and on day 31, they will be injected i.p. with a nonsecreting myeloma cell line. On day 42, ascites fluid will be collected and pooled. Immunoglobulins will
be purified by 50% saturation with ammonium sulfate (22). Whether the generated K. pneumoniae antibodies will cross-react with the infected tissue of AS patients will be subsequently assessed.
(2) Purification of K. pneumoniae reactive antibodies from AS sera by affinity chromatography. For a comparative analysis of K.
pneumoniae-associated immune response elicited in an actual AS patient, we will purify the antibodies from pooled AS sera by using
chromatography on immobilized K. pneumoniae antigens. The purified K. pneumoniae proteins that show strongly reactivity to AS sera (2 mg) will be coupled to 0.3 g of CH-Sepharose 4B (Pharmacia) in 0.1 M Na2HCO3/NaH2CO3 (pH 8.0) containing 0.5 M NaCl. Chromatography will be carried out at room temperature at a flow rate of 0.2 ml/min.
Protein-A-purified antibodies obtained from AS sera, will be applied to the column for 2 h. The fraction not bound by the column will be saved for analysis. The column will be washed extensively with PBST (PBS/
0.05% Tween-20) followed by the same buffer supplemented with 0.35 M NaCl. During elution of bound antibodies with 0.1 M glycine- HCl, pH 2.5, fractions of 0.2 ml will be collected and immediately neutralized with 10 µl 2 M Tris buffer and subsequently dialyzed against PBS.
The third year
Determination of cross-reactivity between the AS-associated K.
pneumoniae antigens and the putative AS factors. Possession of HLA- B27 has been strongly associated with the development of AS. Despite intensive research, the pathogenic role of HLA-B27 and its relevance with Klebsiella infection remain unclear. To understand the underlying
mechanism of this cross-reactivity, we will (i) identify the tissue-specific antigen that the antibody raised against K. pneumoniae will deposit by using an immunohistochemical analysis of the synovial tissue from HLA-B27+ AS patients; (ii) evaluate the immunoreactivity of AS-associated K. pneumoniae antibodies to human collagens.
(1) Immunohistochemical analysis. The biopsy specimens of synovial tissue (ST) have been collected from AS patients and frozen at –80oC.
Cryostat sections will be prepared and mounted on glass slides. The serial sections will be stained with the polyclonal antibodies generated against K. pneumoniae antigen or with the purified antibodies from AS patients. For control sections, the primary antibodies will be omitted or irrelevant mouse antibodies will be applied. Staining will be performed based on a three-step immunoperoxidase method (29). After the slides warmed to room temperature and air-dried, the sections will be washed between all steps with PBS. All incubations will be carried out at room temperature. The primary antibodies will be diluted in PBS-1% BSA.
The HRP-conjugated secondary antibodies will be diluted in PBS-1%
BSA supplemented with 10% normal human serum (NHS) as blocking serum. Endogenous peroxidase activity will be inhibited using 0.1%
sodium azide and 0.3% hydrogen peroxide in PBS. The primary
antibodies will be incubated for 1 h. HRP-conjugated goat anti-mouse or goat anti-human antibody will be added for 30 min, followed by
incubation with HRP-conjugated swine anti-goat antibody for another 30 min. HRP activity will be detected with hydrogen peroxide as substrate and amino ethylcarbazole (AEC) as dye.
(2) Examination of the cross-reactivity with human collagens. Since a correlation between IgM and IgG antibodies against K. pneumoniae and collagen types I, III and IV has been reported (31), we will examine whether the K. pneumoniae reactive antibodies that generated and purified in the second year will crossly react with the human collagens.
Collagen types I, II, III and IV will be purchased from Sigma and dissolved in NaHCO3 (0.1 M) containing with NaCl (0.5 M) to a final concentration of 1 mg/ml. Flat-bottomed 96-well plates will be coated with 200 µl of collagen solution and incubated overnight at 4oC.
Polyclonal antibodies generated from BALB/c mice or purified from AS patient sera will be added and incubated for 1.5 h at room temperature.
After washing, 100 µl of anti-mouse or anti-human class-specific IgG, IgA, or IgM antibody conjugated with peroxidase will be added for
another 1 h. After incubation, plates will be washed, and bound antibodies will be detected and read at a wavelength of 450 nm.
Identification of cross-reactive peptides of the AS-associated K.
pneumoniae antigens. Currently the management of patients with AS includes two main approaches. The first one involves the use of one or more of non-steroid anti-inflammatory drugs (NSAIDs) that are mainly used to alleviate the pain and reduce the associated inflammation. The second approach involves physiotherapy and postural education to prevent the stiffness and deformities which are the main sequelae occurring in this disease. However, the use of NSAIDs is considered as non-specific
measures, as they could not reverse or even halt the damaging pathological process of the disease. Furthermore, these drugs have various undesirable side effects. The use of other therapeutic measures to eliminate the K.
pneumoniae infection or to reduce the level of autoantibodies will be beneficial for the AS patients. For this reason, we will identify the immunodominant region of the identified AS-reactive K. pneumoniae antigens that might bind to HLA-B27. It will provide candidate peptide sequences that can be served as a template for a selective immunotherapy by blocking or antagonizing the HLA-B27 interaction with autoreactive T cell clones.
VI. Anticipated results and achievements:
We anticipate achieving two major contributions through the study.
First, although the IVIAT is not a brand new technology, the application of IVIAT in screening for cross-reactive bacterial antigens in an autoimmune disease is a new approach. The IVIAT system developed in this study can be considered as a platform and will be useful for future analysis of other autoimmune disease associated microbial factors, such as Proteus or Mycobacterium with rheumatic arthritis (RA), Chlamydia trachomatis with spondyloarthropathies (SpA), or certain viral infections with systemic lupus erythematosus (SLE). Second, through the IVIAT analysis, we anticipate to
identify 20-30 genes that putatively associated with the pathogenesis of AS.
By determining their cross-reactivity with AS factors, potential useful peptide targets will be obtained which may lead to the identification of novel anti- autoimmune drugs.
VII. Reference:
1. Ahmadi, K., C. Wilson, H. Tiwana, A. Ebringer, S. Shanmuganathan, and A. Binder. 1998. Antibodies to Klebsiella pneumoniae nitrogenase reductase in patients with ankylosing spondylitis. Ann Rheum Dis 57:441.
2. Altschul, S. F., W. Gish, W. Miller, E. W. Myers, and D. J. Lipman. 1990.
Basic local alignment search tool. J Mol Biol 215:403-10.
3. Arakawa, Y., R. Wacharotayankun, T. Nagatsuka, H. Ito, N. Kato, and M.
Ohta. 1995. Genomic organization of the Klebsiella pneumoniae cps region responsible for serotype K2 capsular polysaccharide synthesis in the virulent strain Chedid. J Bacteriol 177:1788-96.
4. Baines, M., A. Ebringer, H. Avakian, D. Samuel, and D. C. James. 1990.
The use of enzyme immunoassay (EIA) and radiobinding assay to investigate the cross-reactivity of Klebsiella antigens and HLA B27 in ankylosing spondylitis patients and healthy controls. Scand J Rheumatol 19:341-9.
5. Blankenberg-Sprenkels, S. H., M. Fielder, T. E. Feltkamp, H. Tiwana, C.
Wilson, and A. Ebringer. 1998. Antibodies to Klebsiella pneumoniae in Dutch patients with ankylosing spondylitis and acute anterior uveitis and to Proteus mirabilis in rheumatoid arthritis. J Rheumatol 25:743-7.
6. Brewerton, D. 1974. The inherited antigen (HL-A 27) and arthritis. Rep Rheum Dis 55: 423-5.
7. Carpenter, J. L. 1990. Klebsiella pulmonary infections: occurrence at one medical center and review. Rev Infect Dis 12:672-82.
8. Ciurana, B., and J. M. Tomas. 1987. Role of lipopolysaccharide and
complement in susceptibility of Klebsiella pneumoniae to nonimmune serum.
Infect Immun 55:2741-6.
9. Collado, A., J. Gratacos, A. Ebringer, T. Rashid, A. Marti, R. Sanmarti, and J. Munoz-Gomez. 1994. Serum IgA anti-Klebsiella antibodies in
ankylosing spondylitis patients from Catalonia. Scand J Rheumatol 23:119-23.
10. Deb, D. K., P. Dahiya, K. K. Srivastava, R. Srivastava, and B. S.
Srivastava. 2002. Selective identification of new therapeutic targets of Mycobacterium tuberculosis by IVIAT approach. Tuberculosis (Edinb) 82:175-82.
11. Ebringer, A., N. L. Cox, I. Abuljadayel, M. Ghuloom, S. Khalafpour, T.
Ptaszynska, F. Shodjai-Moradi, and C. Wilson. 1988. Klebsiella antibodies in ankylosing spondylitis and Proteus antibodies in rheumatoid arthritis. Br J Rheumatol 27 Suppl 2:72-85.
12. Ebringer, A., and C. Wilson. 2000. HLA molecules, bacteria and autoimmunity. J Med Microbiol 49:305-11.
13. Garnier, J., D. J. Osguthorpe, and B. Robson. 1978. Analysis of the accuracy and implications of simple methods for predicting the secondary structure of globular proteins. J Mol Biol 120:97-120.
14. Hammer, R. E., S. D. Maika, J. A. Richardson, J. P. Tang, and J. D.
Taurog. 1990. Spontaneous inflammatory disease in transgenic rats expressing HLA-B27 and human beta 2m: an animal model of HLA-B27- associated human disorders. Cell 63:1099-112.
15. Handfield, M., L. J. Brady, A. Progulske-Fox, and J. D. Hillman. 2000.
IVIAT: a novel method to identify microbial genes expressed specifically during human infections. Trends Microbiol 8:336-9.
16. Hang, L., M. John, M. Asaduzzaman, E. A. Bridges, C. Vanderspurt, T. J.
Kirn, R. K. Taylor, J. D. Hillman, A. Progulske-Fox, M. Handfield, E. T.
Ryan, and S. B. Calderwood. 2003. Use of in vivo-induced antigen technology (IVIAT) to identify genes uniquely expressed during human infection with Vibrio cholerae. Proc Natl Acad Sci U S A 100:8508-13.
17. Husby, G., N. Tsuchiya, P. L. Schwimmbeck, A. Keat, J. A. Pahle, M. B.
Oldstone, and R. C. Williams, Jr. 1989. Cross-reactive epitope with Klebsiella pneumoniae nitrogenase in articular tissue of HLA-B27+ patients with ankylosing spondylitis. Arthritis Rheum 32:437-45.
18. Isenberg, D. A., R. Feldman, C. Dudeney, F. Konikoff, D. Jones, A.
Ebringer, and Y. Shoenfeld. 1987. A study of antipolynucleotide antibodies,
anti-Klebsiella (K30) antibodies and anti-DNA antibody idiotypes in ankylosing spondylitis. Br J Rheumatol 26:168-71.
19. Jameson, B. A., and H. Wolf. 1988. The antigenic index: a novel algorithm for predicting antigenic determinants. Comput Appl Biosci 4:181-6.
20. Khalafpour, S., A. Ebringer, I. Abuljadayel, and M. Corbett. 1988.
Antibodies to Klebsiella and Proteus microorganisms in ankylosing spondylitis and rheumatoid arthritis patients measured by ELISA. Br J Rheumatol 27 Suppl 2:86-9.
21. Khan, M. A. 1996. Spondyloarthropathies-spondylarthropathies. Curr Opin Rheumatol 8:267-8.
22. Kurpisz, M., S. K. Gupta, D. L. Fulgham, and N. J. Alexander. 1988.
Production of large amounts of mouse polyclonal antisera. J Immunol Methods 115:195-8.
23. Lai, Y. C., G. T. Lin, S. L. Yang, H. Y. Chang, and H. L. Peng. 2003.
Identification and characterization of KvgAS, a two-component system in Klebsiella pneumoniae CG43. FEMS Microbiol Lett 218:121-6.
24. Lai, Y. C., H. L. Peng, and H. Y. Chang. 2001. Identification of genes induced in vivo during Klebsiella pneumoniae CG43 infection. Infect Immun 69:7140-5.
25. Lai, Y. C., H. L. Peng, and H. Y. Chang. 2003. RmpA2, an activator of capsule biosynthesis in Klebsiella pneumoniae CG43, regulates K2 cps gene expression at the transcriptional level. J Bacteriol 185:788-800.
26. Lai, Y. C., S. L. Yang, H. L. Peng, and H. Y. Chang. 2000. Identification of genes present specifically in a virulent strain of Klebsiella pneumoniae. Infect Immun 68:7149-51.
27. Schlosstein, L., P. I. Terasaki, R. Bluestone, and C. M. Pearson. 1973.
High association of an HL-A antigen, W27, with ankylosing spondylitis. N Engl J Med 288:704-6.
28. Schwimmbeck, P. L., D. T. Yu, and M. B. Oldstone. 1987. Autoantibodies to HLA B27 in the sera of HLA B27 patients with ankylosing spondylitis and Reiter's syndrome. Molecular mimicry with Klebsiella pneumoniae as
potential mechanism of autoimmune disease. J Exp Med 166:173-81.
29. Tak, P. P., P. A. van der Lubbe, A. Cauli, M. R. Daha, T. J. Smeets, P. M.
Kluin, A. E. Meinders, G. Yanni, G. S. Panayi, and F. C. Breedveld. 1995.
Reduction of synovial inflammation after anti-CD4 monoclonal antibody treatment in early rheumatoid arthritis. Arthritis Rheum 38:1457-65.
30. Tani, Y., H. Tiwana, S. Hukuda, J. Nishioka, M. Fielder, C. Wilson, S.
Bansal, and A. Ebringer. 1997. Antibodies to Klebsiella, Proteus, and HLA- B27 peptides in Japanese patients with ankylosing spondylitis and rheumatoid arthritis. J Rheumatol 24:109-14.
31. Tiwana, H., R. S. Natt, R. Benitez-Brito, S. Shah, C. Wilson, S. Bridger, M. Harbord, M. Sarner, and A. Ebringer. 2001. Correlation between the immune responses to collagens type I, III, IV and V and Klebsiella
pneumoniae in patients with Crohn's disease and ankylosing spondylitis.
Rheumatology (Oxford) 40:15-23.
32. Trull, A. K., R. Ebringer, G. S. Panayi, D. Colthorpe, D. C. James, and A.
Ebringer. 1983. IgA antibodies to Klebsiella pneumoniae in ankylosing spondylitis. Scand J Rheumatol 12:249-53.
33. Welsh, J., H. Avakian, P. Cowling, A. Ebringer, P. Wooley, G. Panayi, and R. Ebringer. 1980. Ankylosing spondylitis, HLA-B27 and Klebsiella. I.
Cross-reactivity studies with rabbit antisera. Br J Exp Pathol 61:85-91.
34. Wright, V. 1978. Seronegative polyarthritis: a unified concept. Arthritis Rheum 21:619-33.
Figures:
72
33 24
11 kDa
1 2 3 4 1 2 3 4 1 2 3 4
HLA-B27(-) healthy
HLA-B27(+) healthy
HLA-B27(+) AS patient
Figure 1. Western analysis. The extracellular components of K.
pneumoniae (lane 1) and the t otal cell lysates of K. pneumoniae (lane 2), E. coli XL-1 (lane 3) and S. typhimurium LT2 (lane 4) (30 ug/per lane) were separated by 12.5% SDSŠPAGE and transferred onto PVDF
membranes. The membranes were hybridized with serum samples diluted at 1:2000. Representative results from three independent experiments were shown. Panel a: sera from HLA-B27 negative healthy; panel b: HLA- B27 positive healthy; panel c: HLA-B27 positive AS patients. Arrows indicate a specific antigenic response against K. pneumoniae .
(a) (b) (c)
K. pneumoniae Genomic DNA
Inducible expression vector (pETabc)
Induce the expression
E. coli colonies with IPTG, lyse and overlay onto NC membrane
Pooled HLA-B27+ AS patient's serum
Pooled HLA-B27- healthy individuals' serum
Comparative colony blot analysis
Purify plasmid of the strongly positve clones
Sequence cloned insert
Figure 2. Schematic illustration of the experimental design proposed in the first year.
表C013 共 1 頁 第 1 頁
十三、近三年內執行及申請中之研究計畫
(向本會新申請之研究計畫不得與曾執行或其他申請中之研究計畫重複)
計畫名稱
(本會補助者請註明編號)
計畫內擔
任之工作 起迄年月 補助或委託機構 申請(執行)情形
生物處專題計畫主持人近五年研究成果統計、獲研究計畫補助及獎勵情形(表 A)
(修正:92/08/28)
主持人姓名:
_魏 正 宗_
申請機關系所:_中山醫學大學過敏免疫風濕科_
___計畫名稱:
___ 搜尋僵直性脊椎炎相關的克雷白氏菌抗原因子 ___________
(一)請依照個人資料表所列之研究成果提供五年內(1999.1.1 迄今)已發表或被接受發表於 SCI、
SSCI、EI 或其他之期刊論文(發表在有編輯委員會且有同儕審查制度定期發行之學術期刊)、
研討會論文(有刊載出論文全文者)、專書及專書論文、專利及技術移轉等資料填寫於下表:
研究成果* 總篇(件)數 作者順序
SCI 期刊論文 3 1. 第一作者論文 1 篇
2. 非第一作者之通訊作者論文 篇
3. 非第一或通訊作者之其他序位作者論文 2 篇 SSCI 期刊論文
1. 第一作者論文 篇
2. 非第一作者之通訊作者論文 篇
3. 非第一或通訊作者之其他序位作者論文 篇 EI 期刊論文
1. 第一作者論文 篇
2. 非第一作者之通訊作者論文 篇
3. 非第一或通訊作者之其他序位作者論文 篇 加重計分之國內優良
期刊論文 (見附件 2-3)
1. 第一作者論文 篇
2. 非第一作者之通訊作者論文 篇
3. 非第一或通訊作者之其他序位作者論文 篇 其他學術期刊論文
(上述四類以外之期刊論文) 7 1. 第一作者論文 5 篇
2. 非第一作者之通訊作者論文 篇
3. 非第一或通訊作者之其他序位作者論文 2 篇
其他著作 1.研討會論文(有刊載出論文全文者) 篇 2.專書、專書論文 . 篇 3.專利或技轉 件 4.其他 篇(件)
*SCI (Science Citation Index)、SSCI (Social Science Citation Index)、及 EI (Engineering Index)期刊目錄,可就近至 各大學醫學院圖書館、國科會科學技術資料中心或上網(網址:http://www.isinet.com)檢索或查詢。上述 SCI、
SSCI 及 EI 期刊目錄以2002 年之版本為準。
(二)請填寫申請人近五年來獲得本會研究補助及獎勵情形。
主持本會之專題研究計畫件數 (共同及協同主持人不列入計算)
獲得本會之研究獎勵費類別【請選填下列獎別號碼】
□傑出□甲種□乙種□吳大猷□其他(請填名稱)
1. 89 年度 1 期(88.1.1∼88.12.31 ) 件 1. 88 年度(88.1.1∼88.12.31)獲得___________
2. 89 年度 2 期(89.1.1∼89.12.31) 件 2. 89 年度(89.1.1∼89.12.31)獲得___________
3. 90 年度(90.1.1∼90.12.31) 件 3. 90 年度(90.1.1∼90.12.31)獲得___________
4. 90 年度(91.1.1∼91.12.31) 件 4. 91 年度(91.1.1∼91.12.31)獲得___________
5. 92 年度(92.1.1∼迄今) 件 5. 92 年度(92.1.1 迄今) 獲得__________
註:國科會一般甲、乙種研究獎勵費89 學年度
以後停辦。
主持人簽名:
年 月 日8
生物處專題計畫主持人研究表現指數 (RPI) 統計表 (表 B )
(修正:92/08/28)
主持人姓名:____魏 正 宗_____ 申請機關系所:___中山醫學大學過敏免疫風濕科_
計畫名稱:
_____
搜尋僵直性脊椎炎相關的克雷白氏菌抗原因子______________
研究年資(請打9):□滿五年以上(至多 15 篇) □滿四年(至多 12 篇) □滿三年(至多 10 篇)
□滿二年(至多 8 篇) 9滿一年(至多 6 篇) □未滿一年(至多 4 篇)
代表性研究成果一欄表(填表前請先詳閱第四至第六頁之填表說明及範例)
序號
研究 成果 分類
五年內代表性研究成果名稱及相關發表資料 (期刊名稱及發表年代;卷數:起迄頁數)
論文 性質 分類
(C) 刊登 雜誌 分類 排名 (J)
作者 排名 加權 分數 (A)
分數 C×J×A 1 J.CC. Wei, T.W. Chan, H-S. Lin, F. Huang, C-T. Chou.
Thalidomide for Severe Refractory Ankylosing Spondylitis.
Journal of Rheumatology 2003;30:2627-31(SCI)
3 5 5 75 75
2 F Huang, JCC Wei, M Breban. Thalidomide in Ankylosing Spondylitis. Clinical and Experimental Rheumatology. 2002.
supp 28, s-158-61. (SCI)
3 4 3 S01 36
3 Chou CT, Tsai YF, Liu J, Wei JC, Liao TS, Chen ML, Liu LY.
Development of immunomagnetic separation(IMS)- sandwich ELISA for the HLA-B27 antigen detection. J. Immunol Methods.
2001. 255(1-2):15-22. (SCI)
3 4 0.5 S02 6
4 魏正宗. 2003/12. 抗腫瘤壞死因子製劑 臺灣醫界,2003, 46(12):699-704
1 1 6 S04 6
5 魏正宗.食物與關節炎的關係. 基層醫學 2001 16:270-3 1 1 6 S05 6
6 魏正宗.魚油的證據醫學. 基層醫學 2002.17:270-3. 1 1 6 S06
6
7 魏正宗.血清陰性脊椎關節病變.當代醫學 2001. 28:674-8 1 1 6 S07
6
8 簡志弘 魏正宗.自體免疫性肝炎. 中華民國風濕病雜誌
2000.15(1), 29-32.
1 1 5 S08 5
9 魏正宗, 莊家銘..血管硬化新指標--同胱胺酸. 基層醫學 2003.
17:300-2.
1 1 5 5
8
10 蔡宗宏, 魏正宗. .紅斑狼瘡病患常見之感染. 基層醫學 2002.
17:246-51.
1 1 5 5
序號
研究 成果 分類
五年內代表性研究成果名稱及相關發表資料 (期刊名稱及發表年代;卷數:起迄頁數)
論文 性質 分類
(C) 刊登 雜誌 分類 排名 (J)
作者 排名 加權 分數 (A)
分數 C×J×A
11 S11
12 S12
13 S13
14 S14
15 S15
積 分
(S16=S01+S02+S03+..+S14+S15) S16 146研究表現指數(RPI)【(積分×100)/指標上限滿分 =(S16×100)/指標
12.9主持人姓名:__________________ 申請機關系所:_________________________
計畫名稱:
__________________________________________________
序號
研究 成果 分類
五年內代表性研究成果名稱及相關發表資料 (期刊名稱及發表年代;卷數:起迄頁數)
論文 性質 分類
(C) 刊登 雜誌 分類 排名 (J)
作者 排名 加權 分數 (A)
分數 C×J×A
11 S11
8
12 S12
13 S13
14 S14
15 S15