糖尿病患的高血壓治療新趨勢
傅振宗 楊文琴*
佛教慈濟綜合醫院 內科 *藥劑科
摘 要
美國國家腎臟基金會與糖尿病學會將糖尿病患的血壓控制目標定在
130/80mmHg 以下,至於合併腎臟病變,每日蛋白尿排出量大於 1g 病患,則以 125/75mmHg 以下作為控制目標。一般高血壓病患的藥物治療,優先考慮使用利 尿劑與β阻斷劑,但是糖尿病常常合併高血脂,而降血壓藥物會影響血糖和血 脂,因此過去選擇降血壓藥物時,主要是避免血糖和血脂肪惡化,但是目前實證 醫學更重視藥物治療對於大血管病變和小血管病變的影響,尤其是在心血管疾病 與腎臟病變方面,目前美國糖尿病學會建議,如果血壓在 130-139/80-89mmHg 之間,可以先接受最多 3 個月的行為治療,若血壓在 140/90mmHg 以上,就必需 馬上接受藥物治療,有微白蛋白尿或心血管危險因子的病患,第一線藥物以昇壓 素轉化酉每抑制劑 (ACEI ) 優先,至於美國國家腎臟基金會建議,如果血壓超 過 145/90mmHg ( 超過控制目標 15/10mmHg )
以上時,可以考慮合併使用 ACEI 與利尿劑,然後逐漸增加 ACEI 的劑量,若血 壓仍高,則加上長效型鈣離子阻斷劑;倘若仍然無法將血壓控制在目標區,如果 病患心跳每分鐘大於 84 次,可以考慮加上β阻斷劑,如果病患心跳每分鐘小於 84 次,則加上其他族群的鈣離子阻斷劑;至於α阻斷劑可以作為第四線藥物。
關鍵詞:糖尿病 ( Diabetes mellitus )
高血壓治療 ( Antihypertensive treatment )
前言
糖尿病患中大約有 20~60%同時合併有高血壓 1-4,而高血壓是心血管疾病如心 肌梗塞、腦中風與周邊血管疾病等大血管病變的危險因子,由於心血管疾病是糖 尿病患花費最多的併發症,同時也是造成糖尿病患死亡原因的第一位,所佔比例 目前在美國已上升到 86% 5,更何況高血壓也是視網膜病變與腎臟病變兩種小血 管病變的危險因子 6-8,由於糖尿病患容易併發大血管和小血管病變,因此如何 控制糖尿病患的高血壓是非常重要的課題。
高血壓的定義
世界衛生組織/國際高血壓學會 ( WHO/ISH )將正常人的血壓定在 140/90mmHg 以下,對於高血壓則定義為收縮壓大於等於 140mmHg 且/或舒張壓大於等於 90mmHg。1997 年美國監測評估及治療高血壓國家聯合委員會(以下簡稱 JNC) 對
於高血壓的定義也採用 140/90mmHg 以上作為標準 9,並且進一步將血壓在 130/85mmHg 以下定為正常,而將血壓在 130-139/85-89mmHg 稱為正常但偏高,
至於糖尿病患發生心血管疾病的危險性高,因此也有人建議降低正常血壓的標 準,由 130/85mmHg 改為 130/80mmHg,雖然仍沒有共識,但是同意將控制目標 定在 130/80mmHg 以下。
高血壓的盛行率
糖尿病患罹患高血壓的盛行率是同年齡的非糖尿病人的 1.5~3 倍 5,其中第 1 型 糖尿病患常常是在發病後數年,由於併發腎臟病變導致血壓逐漸上升,大約有 30%的第 1 型糖尿病患會發生高血壓 1-2。第 2 型糖尿病患有 20-60%罹患高血 壓,通常在發病時,一部分病患就已合併有高血壓,甚至早在發病前幾年,就已 經有高血壓, 因此它的病理機轉與第 1 型糖尿病患不同,雖然年齡增加或肥胖 都會造成血壓上升,但是將年齡和體重因素控制後,研究仍顯示第 2 型糖尿病患 發生高血壓的危險性是非糖尿病患的 1.5 倍 3。目前認為除了腎臟病變、年齡與 肥胖外,胰島素阻抗和種族差異等其他因素也可能是造成高血壓的原因,由於病 理機轉複雜,因此盛行率差異性大,較難正確預估。
至於台大醫院針對台北市大安區 40 歲以上糖尿病患所做的調查,合併高血壓的 比例為 30.6% 10。通常糖尿病患合併有高血壓的比例和罹患糖尿病的時間成正 比。此外,糖尿病患得到高血壓的年齡也較一般人年輕。
高血壓的診斷與評估
高血壓的診斷必須測量兩次的血壓值都超過 130/85mmHg,而且時間需間隔一周 以上。確定診斷後,應該要測量躺下與立姿的血壓,因為若合併心臟的自主神經 病變時,容易發生姿勢性低血壓,必須特別注意。
身體檢查方面包括身高、體重、周邊循環情形,並且應該注意是否有器官損害或 次發導致高血壓的原因,如視網膜病變、頸動脈雜音、頸靜脈壓上升、心雜音、
腹部雜音等。同時應該詢問是否服用藥物,如綜合感冒藥、口服避孕藥、食慾抑 制劑、甲狀腺素等皆可能影響血壓。此外所有新診斷出高血壓的病患還要接受胸 部 X 光檢查、心電圖、尿液分析、尿白蛋白、糖化血色素、血比容、血脂肪、
肌酸酐、鉀鈣離子等檢查,並且使用心臟超音波評估心臟功能及左心室是否有肥 大情形 11。
高血壓治療的目標
對於一般的高血壓病患血壓控制的目標,通常定在 140/90mmHg 以下,研究指出 收縮壓或舒張壓每上升 5mmHg,心血管疾病的發生率會增加 20-30% 12。在 UKPDS(U.K. prospective diabetes study) 與 HOT ( hypertension optimal treatment ) 兩個大型研究結果皆證明積極控制血壓的糖尿病患有較佳的預後,尤其是對於中 風的預防,效果明顯。值得注意的是兩個研究皆將舒張壓的控制目標定為 80 mmHg 以下,其中 UKPDS 研究,積極控制組與對照組的血壓控制分別為小於 150/80 與小於 180/105mmHg;而 HOT 研究,積極控制組與對照組的舒張壓控制 分別為≦80 與≦90mmHg 13-14,其中,積極控制組的糖尿病患,心血管疾病發
生率及死亡率分別比對照組降低 51%與 43%。
由於上述研究都沒有發現以前醫界擔心的所謂 J point,也就是血壓低於某臨界點 時,心血管疾病的危險性反而增加的情形並沒有出現,因此理論上將高血壓患者 的血壓降到正常範圍以下時,發生心血管疾病的危險性會跟著下降,但是將血壓 降得更低,必須花費更多預算,也可能產生更多副作用,實際上也難以施行,因 此在 2000 年底,美國國家腎臟基金會將糖尿病患的血壓控制目標定在
130/80mmHg 以下 15,隔年美國糖尿病學會與 JNC 也以 130/80mmHg 當作糖尿 病患血壓控制的目標。
至於合併腎臟病變,每日蛋白尿排出量大於 1g 病患,不論是糖尿病患或非糖尿 病患則以 125/75mmHg 以下作為控制目標。
高血壓的治療
高血壓的治療包括行為治療與藥物治療,分述如下:
行為治療
行為治療亦稱生活方式治療法,就是以前所謂的非藥物治療。根據 1997 年 JNC 的建議,糖尿病患只要確認血壓大於 130/85mmHg 以上,就需要合併使用藥物與 行為治療。不過美國糖尿病學會在 2002 年建議,如果血壓在 130-139/80-89mmHg 之間,可以先接受最多三個月的行為治療,若血壓在 140/90mmHg 以上,就必需 馬上接受藥物治療 16。行為治療內容包括中等程度限鈉 (每日鈉攝取量小於 2300mg )。根據研究顯示,對於本態性高血壓病患,每日鈉攝取量由 4600mg 降 為 2300mg 時,血壓可以降低 5/2-3mmHg。其他如戒煙、運動、減少飲酒量、攝 取適當的鉀、鈣和鎂離子與維持良好的生活習慣,並建議肥胖病患進行減重,將 體重控制在理想範圍 9。研究顯示,每降低 1 公斤體重,可以降低 1mmHg 平均 動脈壓,並且對血脂肪及血糖也具有改善效果 17。
藥物治療
由於糖尿病合併高血脂的比率相當高,而降血壓藥物會影響血糖的控制和脂蛋白 濃度,因此過去選擇降血壓藥物時,主要是避免血糖和血脂肪惡化,但是目前實 證醫學更重視藥物治療對於大血管病變和小血管病變的影響,尤其是在心血管疾 病與腎臟病變方面,敘述如下:
一、利尿劑 ( Diuretics )
利尿劑分成 thiazide 利尿劑、環利尿劑與留鉀利尿劑三大類。Thiazide 利尿劑會 增加血液中總膽固醇、三酸甘油脂與低密度脂蛋白,對於高密度脂蛋白影響則不 大,它也會促進鉀離子的流失,使胰島素的分泌下降,造成血糖上升,不過最近 也有報告 thiazide 利尿劑可以增加骨質密度。至於環利尿劑如 furosemide 對於血 糖的直接影響較少,主要是透過鉀離子的流失,造成血糖上升。留鉀利尿劑雖不 會造成鉀離子流失,但是對於血脂肪的影響,也值得留意。至於作用在 L-鈣離 子通道的 indapamide,對於血糖與血脂肪的影響較少。
利尿劑的其他副作用還包括電解質不平衡及性功能減退等。雖然利尿劑副作用不 少,但是,實證醫學的研究報告顯示,糖尿病患使用 thiazide 利尿劑,可以降低
心血管疾病之併發症,例如 SHEP ( systolic hypertension in the elderly program ) 研 究顯示,罹患高血壓的 60 歲以上糖尿病老人服用低劑量 thiazide 利尿劑組與對 照組比較 ,心血管疾病的發生情形可以降低 34%(p< 0.05) ,而且相較於非糖尿 病患,降壓結果受益更多 18。
臨床上利尿劑的使用必須考慮病患腎功能,如果腎絲球過濾速率<60ml/min 時,
thiazide 利尿劑效果不佳,此時應該改為環利尿劑,也有建議肌酸酐大於 1.3mg/dL 時改用環利尿劑,即使目前還沒有大型研究證實環利尿劑對心血管疾病或腎臟病 變有益。
二、β阻斷劑(β-blockers)
β阻斷劑包括非心臟選擇性(例如 propranolol )、心臟選擇性 ( 例如 atenolol、
metoprolol ) 、具內在交感活性 ( ISA, 例如 acebutolol ) 與具β及α雙重阻斷劑 ( 例如 labetalol ) 等四大類。以非心臟選擇性阻斷劑為例,糖尿病患使用應注意 的副作用包括:
(一)透過抑制β2 接受器,降低胰島素分泌,造成血糖上升。
(二)β2 阻斷劑會降低升糖素的分泌,同時周邊組織對於葡萄糖的利用增加,結 果會延長低血糖的發作時間。
(三)發生低血糖的症狀是經由交感神經的興奮產生,若使用β阻斷劑則相關的症 狀例如心悸、顫抖等不會出現,病患較不易早期察覺低血糖的發生。
(四)低血糖發作時,服用β阻斷劑的病患,由於β交感神經被抑制,則α交感神 經會相對的亢奮,使得血管收縮,造成血壓急速上升,容易發生腦溢血。
(五)β阻斷劑除了會使三酸甘油脂上升、高密度脂蛋白濃度下降,只有具內在交 感活性的β阻斷劑不會影響血脂肪的代謝。
(六)β阻斷劑會降低四肢血管的流量,所以手腳冰冷或合併周邊血管疾病的病 患,最好不要使用。
此外,氣喘、慢性阻塞性肺病、心臟傳導障礙、心臟衰竭以及性機能低下者使用 β阻斷劑時皆應小心。由於上述缺點,所以糖尿病患使用時顧忌較多,要小心使 用,應採用有心臟選擇性的β阻斷劑,以低劑量使用較不會影響病患。此外,以 前使用β阻斷劑時,較偏向不會影響血脂肪的具內在交感活性的 acebutolol,不 過近來認為具交感活性,心跳反而增加,對心血管疾病有不利影響。
實證醫學的研究報告顯示,糖尿病患使用β阻斷劑時,副作用並沒有引起太大問 題,在心血管疾病與腎臟病變方面反而有些正面評價,例如使用 atenolol 於第 1 型與第 2 型的糖尿病腎病變病患,都可以減緩腎臟惡化的速度 19-21,而在 UKPDS-HDS ( UKPDS-hypertension in diabetes study )
研究也證實在降低糖尿病相關的大血管與小血管病變方面,β阻斷劑的效果和昇 壓素轉化酉每抑制劑 ( 以下簡稱 ACEI ) 不相上下,而且心肌梗塞死亡率降低 25% 22。在副作用方面,UKPDS 研究顯示使用β阻斷劑組的病患產生四肢冰冷、
間歇性跛行、支氣管痙攣機率高,所以遵囑性較差,至於低血糖的發生率並不如 預期多。
由於罹患心肌梗塞的病患,使用β阻斷劑的死亡率較低,建議罹患心肌梗塞的糖 尿病患可以考慮使用β阻斷劑 22-23。
三、α阻斷劑(α blockers)
α阻斷劑例如 prazosin 是屬於αl 阻斷劑。使用 prazosin 可增加胰島素敏感性,
而且可降低膽固醇、三酸甘油脂及增加高密度脂蛋白。但是初期使用容易發生姿 勢性低血壓,所以糖尿病患有神經病變或姿勢性低血壓時應特別注意。不過有攝 護腺肥大的男性病患,使用α阻斷劑可以減緩症狀。
實證醫學方面,ALLHAT ( antihypertensive and lipid-lowering treatment to prevent heart attack trial ) 研究報告顯示,使用α阻斷劑會增加心血管疾病的發生機率,
尤其是發生心臟衰竭的危險性較高,因此研究進行一半就提早結束 24。目前α 阻斷劑不是糖尿病患的第一選擇。
四、鈣離子阻斷劑(calcium channel blockers;簡稱 CCB)
鈣離子阻斷劑可以分成 dihydropyridine calcium channel blockers ( 簡稱 DCCB )、
benzothiazepines 及 phenylalkylamines,後面兩類合稱 non-dihydropyridine calcium channel blockers ( 簡稱 NDCCB)。NDCCB 的作用和 DCCB 不同,DCCB 舒張血 管作用較強,會產生心跳加快、頭痛、臉潮紅與水腫現象,而 NDCCB 在抑制心 房室傳導作用較強,舒張血管作用則較 DCCB 弱。報告顯示鈣離子阻斷劑會抑 制胰島素的分泌,但臨床上並沒有太大意義。
(一) DCCB
雖然 Syst-Eur ( Systolic Hypertension in Europe trial ) 及 HOT 研究證實 DCCB 可 以降低糖尿病患老人得到心血管疾病的機率,但是這些研究對象大都合併使用 ACEI 與β阻斷劑,因此難以單獨對 DCCB 進行評估 14,25,不過在 ABCD ( appropriate blood pressurecontrol in diabetes ) 與 FACET
( fosinipril versus amlodipine cardiovascular randomized events trials ) 研究中都顯 示 ACEI 降低心血管疾病的效果大於 DCCB 26-27。進一步的次族群分析結果也 顯示 DCCB 降低心肌梗塞與心臟病方面的功效比利尿劑、β阻斷劑或 ACEI 差 28 ,而在 PREVENT ( prospective randomized evaluation of the vascular effects of norvasc trial ) 研究結果雖然使用 amlodipine 病患可以降低住院率,但降低心血管 疾病死亡率並沒有意義 29。而 Furberg 等人回溯性分析更指出短效的 nifedipine 用於降低血壓反而會增加心血管疾病的死亡率,因此不建議使用短效 DCCB 於 降血壓 30。至於預防中風方面,DCCB 成效與 ACEI 不相上下。
在糖尿病腎病變方面,使用 DCCB 雖然可以減低肌酸酐清除率下降的速度,但 是效果比 ACEI 差 31,而短效的 nifedipine 甚至於會增加糖尿病腎病變患者的蛋 白尿情形 32。
整體而言,對於 DCCB 是否可以減少心血管疾病及代謝方面的影響目前仍有爭 議,目前美國心臟學會建議使用 DCCB 於慢性穩定型心絞痛病患,效果佳 33。
(二) NDCCB
目前對於 NDCCB 的觀點是雖然舒張血管作用較弱,降壓效果比 DCCB 差,但
是可以降低交感神經活性,抑制心房室傳導,使心跳減慢,而且可以降低血小板 的活性,減少栓塞的形成,故 NDCCB 較 DCCB 更能預防心血管疾病的發生,
由於早上 6-10 點是發生心血管疾病的顛峰時間,因此在晚上使用長效型的 NDCCB ( COER verapamil,最大作用時間為 6-12 小時),如此即可在隔天早上顯 現出最大作用的效果,來預防心血管疾病的發生。
此外,NDT ( nordic diltiazem trial ) 研究顯示使用 NDCCB 比使用利尿劑 /β阻斷 劑發生腦中風的危險性明顯降低 34。NDCCB 也可以延緩腎臟病變惡化,具備 保護腎臟的功能 35-37,尤其是和 ACEI 合併使用,效果比單一使用好,因此糖 尿病患選擇鈣離子阻斷劑時,以 NDCCB 為優先考慮對象。
由於 NDCCB 與 DCCB 是作用在 L-鈣離子通道不同的位置上,因此兩者也可以 合併使用於高血壓的病患。
五、昇壓素轉化酉每抑制劑 (Angiotensin-converting enzyme inhibitors;ACEI):
ACEI 通常不會影響血糖值或血脂肪,僅有少數病例報告 captopril 及 enalapril 曾 經引起低血糖。主要副作用包括乾咳、血管神經性水腫、高血鉀與急性腎臟衰竭 等,臨床上如果有下列情況時,容易發生急性腎臟衰竭,應該避免使用,包括 (1) 病患的平均動脈壓不足以維持腎臟灌流壓(2)體液容積不足(3)使用血管收縮的藥 物 ( 包括 NSAID、cyclosporin 等 ) (4)有腎血管疾病包括腎動脈狹窄或小腎動脈 有瀰漫性動脈硬化等。急性腎臟衰竭常發生於使用初期,必須小心監測腎功能,
如果使用前肌酸酐<2mg/dL,而使用後上升 0.5mg/dL 以上或使用前肌酸酐
>2mg/dL,使用後上升 1.0mg/dL 以上時,就必須停止使用 ACEI 38。
有些病患使用第一代的藥物 captopril 後,發生蛋白尿與小便酮體檢查偽陽性現 象,造成困擾。不過實證醫學的大型研究報告顯示,ACEI 可以降低發生腦中風、
冠心病、心臟衰竭的機率,也可以降低心血管疾病與發生心肌梗塞後的死亡率,
此外對腎臟有保護作用,除非特殊考量,一般使用為首選藥物。敘述如下:
(一)對心血管病變的影響
根據 UKPDS 的研究顯示使用 ACEI (captopril) 或使用β阻斷劑 ( atenolol ) 嚴格 控制血壓的糖尿病患與非嚴格控制血壓的對照組比較,糖尿病相關的心血管疾病 ( total diabetes-related end point ) 降低 24%,糖尿病相關的死亡率降低 32%,中 風的危險性降低 44% 13,22。而 CAPPP (captopril prevention project ) 則是證實使 用 ACEI 發生心血管死亡率、心肌梗塞、腦中風的情形比使用利尿劑/β阻斷劑 低 39。
STOP-Hypertenion 2 trial 研究結果顯示,使用傳統抗血壓的藥物包括利尿劑或β 阻斷劑治療的病患和使用較新的藥物包括 ACEI 或鈣離子阻斷劑的病患,兩組在 心血管疾病的發生情形與預後並沒有差異,不過在 STOP-Hypertention-2 的次族 群分析研究結果顯示使用 ACEI 比 DCCB (felodipine 或 isradipine ) 有較低的心肌 梗塞發生率 40。
目前的研究證實急性腦梗塞初期,使用 ACEI ( perindopril ) 控制血壓並不會降低
腦部病變部位的血流量 41-42,而其他傳統降壓藥和 CCB 則可能影響血流量。
綜合以上結論︰ACEI 降低心血管疾病的發生與心肌梗塞後的死亡率皆優於其他 降壓藥物。推測機轉可能包括維持內皮細胞的完整,抑制 endothelin 釋放、促進 纖維溶解與釋放一氧化氮(NO )、prostacyclin 等血管舒張物質。
(二)對腎臟病變的影響
有關第 1 型糖尿病的研究證實 ACEI ( captopril)使用於已發生蛋白尿(尿液白蛋白
>500mg /24h ) 的糖尿病患 43,可以延緩腎臟病變繼續惡化的速度,其作用機轉 和降血壓的作用沒有關連,而是 ACEI 本身同時具備保護腎臟的功能。
至於第 2 型糖尿病的 UKPDS-HDS 也證實使用 ACEI 或β阻斷劑積極控制血壓的 病患比使用其他降壓藥物治療,在包括腎臟與視網膜病變的發生情形降低 37%,
而 6 年內發生白蛋白尿的危險性降低 29% 13。
由以上的大型研究報告可知 ACEI 用於第 1 型與第 2 型糖尿病可以延緩腎臟病變 繼續惡化的速度,證實 ACEI 除了降低血壓外,對腎臟也有保護功能。至於腎臟 功能正常時,是否可以用 ACEI 來預防腎臟病變的發生呢?雖然目前
MICRO-HOPE (Heart Outcomes Prevention Evaluation ) 研究顯示 ACEI ( ramipril ) 可以降低微白蛋白尿的發生,但是沒有統計上的意義 44,未來仍然有待大型研 究證實。
總而言之,ACEI 除了控制血壓外,也使用於心臟衰竭、糖尿病與非糖尿病之腎 臟病變,是罹患高血壓的糖尿病患首選藥物。
六、昇壓素接受器阻斷劑(Angiotension receptor blockers;ARB)
ARB 發生乾咳、高血鉀、血管神經性水腫與急性腎臟衰竭的機率皆較 ACEI 低。
研究證實 ARB 也可以延緩腎臟病變繼續惡化的速度,其作用機轉和降血壓的作 用沒有關連 45-46,亦即同時具有降壓與保護腎臟的功能。在降低血壓及尿白蛋 白方面,合併使用 ARB 與 ACEI 較單獨使用其中任何一種效果佳。不過 ARB 在 降低心血管疾病的成效,仍然有待未來大型研究證實 47-48。
如何選擇高血壓藥物
心血管疾病是造成糖尿病患死亡原因的第一位,因此使用降血壓藥物治療必須注 意對心血管疾病的影響,目前市面上使用的降血壓的藥物,每一類大約可以降低 血壓 10-15/5-10mmHg,因此使用降血壓藥物治療的相關研究大都顯示能降低心 血管疾病的發生情形,至於那一種藥物是較佳的選擇呢?
根據 JNC 的建議,一般高血壓病患如果收縮壓與舒張壓皆高於標準,可以優先 考慮使用利尿劑與β阻斷劑;獨立收縮型高血壓的病患,則以利尿劑或 NDCCB 為第一線藥物。至於世界衛生組織的建議則是利尿劑、β阻斷劑、鈣離子阻斷劑、
α阻斷劑、ACEI 或 ARB 都可以當做高血壓病患治療的第一線藥物。
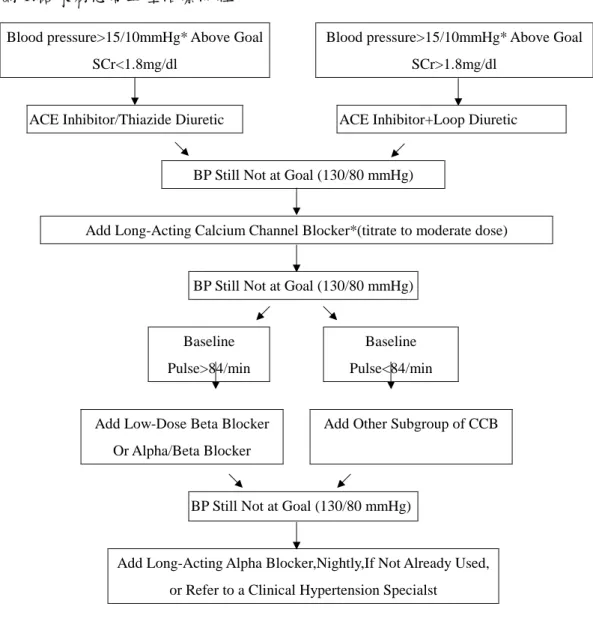
對於罹患高血壓的糖尿病患,美國糖尿病學會建議,對於微白蛋白尿或心血管危 險因子的病患,第一線藥物以 ACEI 為優先,若有罹患心肌梗塞,則使用β阻斷 劑,至於美國國家腎臟基金會在 2000 年建議,如果血壓超過 145/90mmHg ( 超過控制目標 15/10mmHg ) 以上時,可以考慮合併使用 ACEI 與利尿劑 ( 肌
酸酐≧1.3mg/dL 時,改用環利尿劑 ),然後逐漸增加 ACEI 的劑量,如果血壓仍 未達到 130/80mmHg,則加上長效型 NDCCB;倘若仍然無法將血壓控制在目標 區,若病患心跳每分鐘大於 84 次,可以考慮加上低劑量β阻斷劑,如果病患心 跳每分鐘小於 84 次,則加上其他族群的 CCB ( 圖一)。至於α阻斷劑可以作為 第四線藥物。如果使用 ACEI 發生無法忍受之副作用,也可以考慮改用 ARB 藥 物。當血壓控制不錯時,則可以考慮將 ACEI 和利尿劑改成單一錠劑,提高病人 服藥的遵囑性。
結論
糖尿病患者應該定期測量血壓,雖然 JNC 在 1997 年建議只要確認血壓大於 130/85mmHg 以上,就需要合併使用藥物與行為治療,不過美國糖尿病學會在 2002 年建議如果血壓在 130-139/80-89mmHg 之間,可以先接受最多 3 個月的行 為治療,若血壓在 140/90mmHg 以上,就必需馬上接受藥物治療。當然藥物的選 擇必須根據每位病患的個別差異來考量,包括耐受性、合併症、個人喜好、價錢 等等因素。血壓控制的目標定在 130/80mmHg 以下,至於合併腎臟病變,每日蛋 白尿排出量大於 1g 病患,則為 125/75mmHg 以下。通常達到治療目標需要合併 使用兩種以上的藥物,當血壓控制不錯時,則可以考慮將 ACEI 和利尿劑改成合 併的單一錠劑,以提高病人服藥的遵囑性。
參考文獻
1.Nishimura R, LaPorte RE, Dorman JS, Tajima N, Becker D, Orchard TJ. Mortality trends in type 1 diabetes: the Allegheny County (Pennsylvania) Registry 1965-1999.
Diabetes Care 2001; 24: 823-7.
2.Mathiesen ER, Ronn B, Jensen T, Storm B, Deckert T. Relationship between blood pressure and urinary albumin excretion in development of microalbuminuria. Diabetes 1990; 39: 245-9.
3.Hypertension in Diabetic Study (HDS): prevalence of hypertension in newly presenting type 2 diabetic patients and the association with risk factors for cardiovascular and diabetic complications. J Hyperten 1993; 11: 309-17.
4.Nelson RG, Bennett PH, Beck GJ, et al. Development and progression of renal disease in Pima Indians with non-insulin-dependent diabetes mellitus. N Engl J Med 1996; 335:1636-42.
5.Wingard DL, Barrett-Connor E. Heart disease and diabetes. In Diabetes in America.
Washington, DC, U.S. Govt. Printing Office; 1995; 429-48.
6.Hasslacher C, Sted W, Wahl P, Ritz E. Blood pressure and metabolic control as risk factors for nephropathy in type I (insulin-dependent) diabetes. Diabetologia 1985; 28:
6-11.
7.Knuiman MW, Welborn TA, McCann VJ, Stanton KG, Constable IJ. Prevalence of diabetic complications in relation to risk factors. Diabetes 1986; 35: 1332-9.
8.Kannel WB. An overview of risk cardiovascular disease. In Prevention of Coronary
Disease, Practical Management of Risk Factors. Kaplan, Neward, Stanler, Eds.
Philadelphia, WB Sauders, Co; 69-83.
9.Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure: The Sixth Report of the Joint National Committee on
Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC VI).
Arch Int Med 1997; 157: 2413-46.
10.Tai TY, Chuang LM, Chen CJ, Lin BJ. Link between hypertension and diabetes mellitus epidemiological study of Chinese adults in Taiwan. Diabetes Care 1991; 14:
1013-20.
11.Arauz-Pacheco, parrott MA, Raskin P. The treatment of hypertension in Adult patients with diabetes. Diabetes Care 2002; 25: 134-47.
12.MacMahon S, Peto R, Cutler J, et al. Blood pressure, stroke, and coronary heart disease. Part 1. Prolonged difference in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990; 335: 765-74.
13.UK Prospective Diabetes Study Group: Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ 1998; 317: 703-13.
14.Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin on patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomized trial. Lancet 1998; 351:
1755-62.
15.Bakris GL, Williams M, Dworkin L, et al. Special Report: Preserving renal function in adults with hypertension and diabetes: A consensus approach. Am J Kidney Dis 2000; 36: 646-61.
16.Treatment of hypertension in adults with diabetes. American Diabetes Association.
Diabetes Care 2002; 25: 199-201
17.Staessen J, Fagard R, Lijnen P, Amery A. Body weight, sodium intake and blood pressure. J Hyperten 1989; 7: S19-23.
18.Curb JD, Pressel SL, Cutler JA, et al. Effect of diuretic-based antihypertensive treatment on cardiovascular disease risk in older diabetic patients with isolated systolic hypertension: Systolic Hypertension in the Elderly Program Cooperative Research Group. JAMA 1996; 276: 1886-92.
19.Nielsen FS, Rossing P, Gall MA, Skott P, Smidt UM, Parving HH. Long-term effect of lisinopril and atenolol on kidney function in hypertensive NIDDM subjects with diabetic nephropathy. Diabetes 1997; 46: 1182-8.
20.De Cesaris R, Ranieri G, Filitti V, Andriani A, Bonfantino MV. Effects of atenolol and enalapril on kidney function in hypertensive diabetic patients. J Cardiovasc Pharmacol 1993; 22: 208-14.
21.Elving LD, de Nobel E, van Lier HJ, Thien T. A comparison of the hypotensive effects of captopril and atenolol in the treatment of hypertension in diabetic patients. J Clin Pharmacol 1989; 29: 316-20.
22.UK Prospective Diabetes Study Group: Efficacy of atenolol and captopril in reducing the risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. BMJ 1998; 317: 713-20.
23.Goldstein S. Beta-blockers in hypertensive and coronary heart disease. Arch Intern Med 1996; 156: 1267-76.
24.Messerli FH. Implications of discontinuation of doxazosin arm of ALLHAT: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Lancet 2000; 355: 863-4.
25.Tuomilehto J, Rastenyte D, Birkenhager WH, et al. Effects of calcium channel blockade in older patients with diabetes and systolic hypertension. NEJM 1999; 340:
677-84.
26.Estacio RO, Jeffers BW, Gifford N, Schrier RW. Effect of blood pressure control on diabetic microvascular complications in patients with hypertension and type 2 diabetes. Diabetes Care 2000; 23: B54-64.
27.Tatti P, Paahron M, Byington RP, DiMauro P, Strollo G, Strollo F. Outcome results of fosinopril versus amlodipine cardiovascular events randomized trial (FACET) in patients with hypertension and NIDDM. Diabetes Care 1998; 21: 597-603.
28.Blood Pressure Lowering Treatment Trialist's Collaboration: Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomized trials. Lancet 2000; 356: 1944-55.
29.Pitt B, Byington RP, Furberg CD, et al. Effect of amlodipine on the progression of atherosclerosis and the occurrence of clinical events. Circulation 2000; 102: 1503-10.
30.Furberg CD, Psaty BM, Meyer JV. Nifedipine: dose-related increase in mortality in patients with coronary heart disease. Circulation 1995; 92: 1326-31.
31.Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the
angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 2001; 345: 851-60.
32.Melbourne Diabetic Nephropathy Study Group. Comparison between perindopril and nifedipine in hypertensive and normotensive diabetic patients with
microalbuminuria. BMJ 1991; 302: 210-6.
33.Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/ American Heart Association task force on practice guidelines
(committee on management of patients with chronic stable angina). J Am Coll Cardiol 1999; 33: 2092-7.
34.Hansson L, Hedner T, Lund-Johansen P, et al. Randomized trial of effects of calcium antagonists compared with diuretics and beta-blockers on cardiovascular mortality in hypertension: the Nordic Diltiazem Study. Lancet 2000; 356: 359-64.
35.Bakris GL. Effects of diltiazem or lysinopril on massive proteinuria associated with diabetes mellitus. Ann Intern Med 1990; 112: 707-8.
36.Bakris GL, Mangrum A, Copley JB, Vicknair N, Sadler R. Effect of calcium channel or beta-blockade on the progression of diabetic nephropathy in African Americans. Hypertension 1997; 29: 744-50.
37.Bakris GL, Copley JB, Vicknair N, Sadler R, Leurgrans S. Calcium channel
blockers versus other antihypertensive therapies on progression of NIDDM associated nephropathy. Kidney Int 1996; 50: 1641-50.
38.Schoolwerth AC, Sica DA, Ballermann BJ, Wilcox CS. Renal considerations in angiotensin converting enzyme inhibitor therapy: a statement for healthcare
professionals from the Council on the Kidney in Cardiovascular Disease and the Council for High Blood Pressure Research of the American Heart Association.
Circulation 2001; 104: 1985-91.
39.Hansson L, Lindhol LH, Niskanen L, et al: Effect of angiotensin-
converting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomized trial. Lancet 1999; 353: 611-6.
40.Hansson L, Lindholm L, Ekborn T, et al. Randomized trial of old and new
antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity the Swedish Trial in Old Patients with Hypertension-2 study. Lancet 1999; 354: 1751-6.
41.Waldemar G, Vorstrup S, Andersen AR, et al. Angiotensin-converting enzyme inhibition and regional cerebral blood flow in acute stroke. J Cardiovasc Pharmacol 1989; 14: 722-9.
42.Dyker AG, Grosset DG, Lees KR. Perindopril reduces blood pressure but not cerebral blood flow in patients with recent cerebral ischemic stroke. Stroke 1997; 28:
580-3.
43.Lewis EJ, Hunsicker LG, Bain RP, Rohde RE: The effect of angiotensin-converting enzyme inhibition on diabetic nephropathy. N Engl J Med 1993; 329: 1456-62.
44.Heart Outcomes Prevention Evaluation Study Investigators: Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE
study and MICRO-HOPE substudy. Lancet 2000; 355: 253-9.
45.Parving HH, Lehnert H, Brochner-Mortensen J, Gomis R, Andersen S, Arner P.
The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 2001; 345: 870-8.
46.Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001; 345: 861-9.
47.Ruilope LM, Aldigier JC, Ponticelli C, et al. Safety of the combination of valsartan and benazepril in patients with chronic renal disease. European Group for the
Investigation of Valsartan in Chronic Renal Disease. J Hypertens 2000; 18: 89-95.
48.Russo D, Pisani A, Balletta MM, et al. Additive antiproteinuric effect of converting enzyme inhibitor and losartan in normotensive patients with IgA nephropathy. Am J Kidney Dis 1999; 33: 851-6.
New Trend in Antihypertensive Treatment in Diabetes Mellitus
Chen-Chung Fu, and Wen-Chin Yang*
Department of Internal Medicine, *Department of Pharmacy Buddhist Tzu Chi General Hospital, Hualien, Taiwan
New treatment guideline published by the National Kidney Foundation and American Diabetic Association advise physicians to lower the blood pressure of patients with diabetes to <130/80mmHg and even lower blood pressures levels -- less than 125/75 mm Hg for people who have proteinuria of greater than 1 g per day and renal
insufficiency regardless of etiology. Although some antihypertensive medications have impacts on the patients' blood sugar and lipids, the evidence-based medicine put more focuses on reducing the morbidity and mortality from macrovascular
(congestive heart failure, coronary artery disease, and stroke) and microvascular complications (nephropathy, neuropathy, and retinopathy). If the patient has a blood pressure above 145/90mmHg, starts treatment with low dose of an
angiotensin-converting enzyme inhibitor and add a thiazide diuretic if necessary, then increasing the dosage of the ACE inhibitor, as needed. If blood pressure is still not controlled, add a nondihydropyridine calcium channel blocker is recommended. If the blood pressure goal is still not achieved, a beta blocker or other subgroup of calcium channel blocker can be added depending on the heart rate of the patient. Finally, once the goal of blood pressure is achieved, switch to a fixed-dose multi-drug combination of either an ACE inhibitor and a diuretic, to help facilitate patient compliance. (J Intern Med Taiwan 2002;13:215-224)
圖 1.糖尿病患高血壓治療流程
Blood pressure>15/10mmHg* Above Goal SCr<1.8mg/dl
Blood pressure>15/10mmHg* Above Goal SCr>1.8mg/dl
ACE Inhibitor/Thiazide Diuretic ACE Inhibitor+Loop Diuretic
BP Still Not at Goal (130/80 mmHg)
Add Long-Acting Calcium Channel Blocker*(titrate to moderate dose)
BP Still Not at Goal (130/80 mmHg)
Baseline Pulse>84/min
Baseline Pulse<84/min
Add Low-Dose Beta Blocker
Or Alpha/Beta Blocker
Add Other Subgroup of CCB
BP Still Not at Goal (130/80 mmHg)
Add Long-Acting Alpha Blocker,Nightly,If Not Already Used, or Refer to a Clinical Hypertension Specialst
*If BP goal achieved converted to fixed combinations(ACEI/CCB or an ACEI/diuretic)
圖一:糖尿病患高血壓治療流程