IIN NT TR RO OD DU UC CT TIIO ON N
Nasopharyngeal carcinoma (NPC) is a common cancer in Southeast Asia, including Southern China, Hong Kong, Taiwan, Singapore, and Malaysia [1-4], where large populations of ethnic Chinese are gathered.
The age-adjusted annual incidence rate varied from 3/10
55to 60/10
55[4,5]. Genetic vulnerability, diet, environmental factors and viral infections have been associated with the high risk of NPC [5-7]. Among these, Epstein-Barr virus
(EBV) infection has been suggested to contribute most substantially to the development of NPC. Not only EBV gene products are detected in NPC cells [6-9], but also serum IgA and IgG to EBV antigens are elevated in these patients [1-4,8-11]. EBV serology, virology, pathology, immunology and molecular biology were therefore used for determining the disease management [6-12].
Several researchers have studied the correlation between serum antibody titer to EBV with prognosis. Nonetheless, the results have not been consistent [2-4,8-11]. The discrepancy could be due in part to the limited application capacity of the respective EBV antigen, and in part to the fact that the B
Ba ac ck kg gr ro ou un nd d.. Elevated serum IgA to Epstein-Barr virus (EBV) antigens was frequently found in patients with nasopharyngeal carcinoma (NPC). Recent evidence indicated that EBV in NPC patients could be a mixture of latent and active infections.
M
Me etth ho od dss.. In this longitudinal study, we therefore used six EBV antigens from both latent and acute phases of infection to evaluate NPC patients. Immunosensitivity was determined using enzyme-linked immunosorbent assay, and immunospecificity was assessed using immunoblot.
R
Re essu ullttss.. Levels of serum IgA to EBV in NPC patients were significantly higher than the levels in the healthy control subjects. Persistent high IgA titer or the aberrant increase of IgA level indicated a high risk of disease recurrence and early distant metastasis.
C
Co on nc cllu ussiio on nss.. Disease progression of NPC was proceeded by the increase of IgA titer to EBV antigens. Measurement of serum IgA to a panel of EBV antigens from both latent and acute viral infections could, therefore, provide a predictive index for NPC response. (Mid Taiwan J Med 2001;6:7-13)
K
Ke ey y w wo or rd ds s
ELISA, Epstein-Barr virus, nasopharyngeal carcinoma, prognosis, western blot
Serum Responses to the Combination of Epstein-Barr Virus Antigens in Patients
With Nasopharyngeal Carcinoma in a Follow-up Study
Ming-Hsui Tsai, Chang-Fang Chiu 1 , Kuan-Chih Chow 2
Department of Otolaryngology,
1Section of Hematology/Oncology, Department of Internal Medicine, and
2Department of Medical Research, China Medical College Hospital, Taichung, Taiwan, R.O.C.
Received : December 1, 2000. Revised : January 10, 2001.
Accepted : January 10, 2001.
Address reprint requests to : Kuan-Chih Chow, Department of
Medical Research, China Medical College Hospital, No 2,
Yuh-Der Road, Taichung 404, Taiwan, R.O.C.
virus in the cancer cells may not be latent alone [1-4,9-11]. In this study, we used six EBV- encoded proteins that were expressed at different phases of virus infection to appraise serum IgA levels to determine the clinical care of NPC patients.
P
PA AT TIIE EN NT TS S A AN ND D M ME ET TH HO OD DS S Patients
From June 1980 through July 1992, 314 patients with newly diagnosed NPC were enrolled in this study. All patients for whom at least one follow-up examination or death was documented were pathologically confirmed as having NPC. Patients were followed until June 1997. Clinical staging was classified by the UICC system. Sera from 340 healthy donors with equivalent distribution of age and gender were collected as the healthy control for comparison [1]. The protocol was approved by the ethics committee of our hospital, and written informed consent was obtained from each patient. Sera and peripheral blood cells were collected from patients at the time of diagnosis. Following cessation of treatment, collections of sera and peripheral blood cells were continued during follow-up, four times at three-month interval during the first year, and then at six-month interval after the second year. The total dose for irradiation was 70 74 Gy (2 Gy/fraction, 5 fractions/week) at the nasopharynx region. When the patient had cervical lymph node involvement, 65 74 Gy was given in the neck areas. Patients with local recurrence were irradiated by external beam irradiation, and those with distant metastatsis were treated with chemotherapy consisting of cisplatin and 5-fluorouracil based regimens. After treatment, all patients were followed as designated by protocol. A single- blind procedure was followed to carry out enzyme-linked immunosorbent assay (ELISA), immunoblotting, in situ hybridization (ISH) and polymerase chain reaction (PCR) [1].
Immunoblot Analysis and EBV Signal Amplification
Construction of the plasmids, purifi- cation of the EBV antigens and sensitization of the ELISA plate have been described previously [1]. Immunoblot analysis and EBV signal amplification were performed as reported previously, and the respective sensitivity of immunoblotting was 98.1% and specificity was 93.3% [1]. Briefly, six purified recombinant proteins, DNA binding protein (DBP), early antigen diffused (EA-D), EBNA-1, EBV-specific DNA polymerase (EDP), thymi- dine kinase (TK) and EBV BZLF-1 replication activator (ZEBRA), were mixed and subjected to a one-well SDS-PAGE. Proteins were then electroblotted onto a nitrocellulose membrane, and the membrane was sectioned into thin strips containing all six proteins. A thin strip was incubated with serum from one patient. A positive reaction was identified using alkaline phosphatase-conjugated goat anti-human IgA (1:3000 dilution) and chromogen nitro blue tetrazolium with 5-bromo-4-chloro-3-indolyl phosphate (Sigma, St. Louis, Missouri). For EBV signal amplification, cellular DNA extracted from each patient's WBC fraction was subjected to 40 cycles of PCR. Two sets of primers that were specific to the Bam HI L region and BamHI W region of EBV were used, respectively. The amplified product was then resolved in a 2.5% agarose-ethidium bromide gel [1].
R
RE ES SU UL LT TS S
The initial clinical characteristics of the NPC patients are summarized in Table 1. The average age of the male patients was 51.6 12.9 years (n = 251), and that of the female patients was 43.2 13.1 years (n = 63). Following radiotherapy, all patients reached complete remission, except 23 patients who had disease advanced and 30 patients who had only partial remission. The two-year local relapse rate was 20.3%. The five-year survival rate decreased with advancement of the disease (stage I, 100%; stage II, 71.2%; stage III, 42.0%;
and stage IV, 29.5%), and with the increased
number of lymph nodes involved (N0, 68.1%;
N1, 50.7%; N2, 43.8%; and N3, 31.2%). We used six EBV-encoded proteins that were expressed at different phases of virus infection to appraise serum IgA level in these NPC patients. Consistent with our previous results [1], the elevated serum IgA to EA-D and EBNA- 1 was found in 97.5% of patients by ELISA.
When the survival rates of patients were stratified with the initial IgA titer to the respective EBV antigen, no significant correlation was detected (data not shown).
There was no correlation found between the initial IgA titer to a single EBV antigen and the complete remission rate either.
After treatment, eight patients whose results were negative for serum IgA/EBV at diagnosis remained negative. The combination of EBNA-1 and EA-D was further used to monitor patients with positive serum IgA/EBV during the follow-up. The results are shown in Table 2. Among the 306 patients with positive results of serum IgA/EBV, serum level of IgA in 169 patients (55.2%) stayed above the cut-off value [1]. In 100 patients, the serum IgA level decreased gradually, and in 37 patients, the serum IgA level increased aberrantly. Mostly, the increases of IgA titers were associated with a high risk of disease recurrence, early
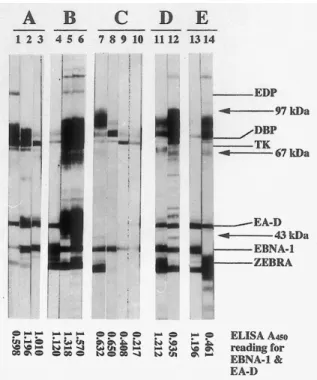
distant metastasis, and early death. However, IgA titer change may not procure the same result in every patient. During the first year, five patients (15.6%) died who indeed had substantially decreased serum IgA levels to EBNA-1 and EA-D. A spectrum of six EBV antigens was then used in western blot analysis to monitor the disease. We emphasized on the 32 patients who died in the first year and ten patients who had obviously increased IgA levels but lived for more than five years after cessation of therapy. Representative examples from five patients are shown in Fig. 1. Lanes 1 3 indicate an increase in ELISA reading, however, IgA levels measured using immunoblotting decreased. The virus replication-associated proteins, such as EDP, DBP, TK and ZEBRA, had decreased markedly. Patient B had obviously increased IgA levels according to both ELISA and immunoblotting as shown in lanes 4 6. The increases were mainly the virus replication-associated proteins (lanes 5 and 6). The extraneous bands detected between the virus proteins could be a minor bacterial proteins left during the extensive purification. IgA levels that were not changed on ELISA readings, but decreased on
T N Stage *
35 (11.1) 84 (26.8) 73 (23.2) 122 (38.8) T1
T2 T3 T4
84 (26.8) 25 (8.0) 78 (24.8) 127 (40.4) N0
N1 N2 N3
23 (7.3) 40 (2.7) 63 (20.1) 188 (58.9) I
II III IV T
Ta ab blle e 11.. IIn niittiia all cclliin niicca all cch ha arra acctte erriissttiiccss o off 33114 4 p pa attiie en nttss w wiitth h n na asso op ph ha arry ya ag ge ea all cca arrcciin no om ma a
* Lymph node involvement 73.2% (230); number in parenthess represents the percentage.
Survival time Serum IgA level to EBNA-1 and EA-D after therapy*
T
Ta ab blle e 22.. C Ch ha an ng ge ess o off sse erru um m IIg gA A lle ev ve ellss tto o E EB BN NA A--11 a an nd d E EA A--D D d du urriin ng g ffo ollllo ow w--u up p a an nd d cco orrrre ella attiio on n o off IIg gA A lle ev ve ell cch ha an ng ge ess w wiitth h tth he e ssu urrv viiv va all ttiim me e iin n 330 06 6 p pa attiie en nttss w wiitth h n na asso op ph ha arry yn ng ge ea all cca arrcciin no om ma a
No change Decreased
≤ 1 year (n = 30)
1 year 5 years (n = 103)
> 5 years (n = 173)
5 (16.7) 32 (31.1) 63 (36.4)
15 (50.0) 54 (52.4) 100 (57.8)
10 (33.3) 17 (16.5) 10 (5.8)
* Significant difference was noted patients with different survival time (p < 0.005); number in the parenthesis represents the percentage.
Increased
immunoblotting are shown in lanes 7 10 (patient C). However, decreases were observed in the virus replication-associated proteins. In patient D, the IgA levels were not changed on ELISA reading, but were increased on immunoblot-ting (lanes 11 and 12). Lanes 13 and 14 demonstrated that patient E had a decrease on the ELISA reading, but an increase of IgA levels on immunoblotting. These results showed that western blot analysis resolved the immunoreactivity of serum IgA to the respective EBV antigens, and showed the fluctuation pattern of IgA levels at the same time. Persistent high IgA levels and the aberrant increases of IgA titers to EBV were associated with a high risk of disease recurrence and early distant metastasis. Local recurrence was confirmed using nasopharyn- goscopy, biopsies and identification of EBER
expression. Distant metastasis to the lung or liver was validated using sonography and X- ray radiography. Distant metastasis to bone marrow was proven with biopsy and ISH of EBERs [12].
D
DIIS SC CU US SS SIIO ON N
The results from the serological studies of the NPC patients have provoked a question about the persistently high titers of IgA to EBV [1-4,7-11]. High levels of IgA to EBV- specific antigens implicate continuous stimulation of the host immune system with these EBV-specific antigens from certain mucosa origins [1]. In addition, antibodies to the early and late gene products of EBV, such as viral capsid antigen (VCA), have suggested the recent encounter with these proteins and, probably, the mature virus particles.
The extensive search using electron microscopy, however, did not identify virus particles in the NPC cells [13]. Interestingly, following passages in a nude mouse, the NPC cells released EBV to infect marmoset lymphocytes [14]. Freshly cultured NPC cells that were activated by bromodeoxyuridine also released EBV particles [15]. These data suggest that pathological microenvironments in patients with NPC might modulate the gene expression of EBV in the tumor cells, which in turn were reflected in the pattern of IgA expression. The results also indicated that the unusual immunological response in NPC patients to EBV were a result of the aberrant viral gene expression [8,10,11], the reactivation of virus infection, or a mixture of both [1,9,16].
Therefore, using a single EBV antigen expressed during a certain phase of viral infection to study the disease and to predict the outcome of treatment might have intrinsic limitations.
Based on this concept, we used six EBV- specific antigens that were expressed during the latent and replication phases, to determine the concurrent presentation of serum IgA to these antigens [17]. Our results support the previous findings that EBV infections in NPC
Fig. 1 Representative examples of immunoblot analysis using six recombinant EBV antigens to determine the serum IgA levels in five NPC patients. Each nitrocellulose membrane strip contained six purified recombinant proteins: EDP, 0.25 g; DBP, 0.25 g; TK, 0.25 g; EA-D, 0.25 g;
EBNA-1, 0.1 g; and ZEBRA, 0.25 g. The relative position of each EBV protein (labeled on the right-hand side). Arrow:
position of protein molecular weight standard. A450
readings for the respective lanes are listed at the bottom.
patients are not latent alone [8,10,11]. Although the immunosensitivity and the immunospeci- ficity among the various proteins indicate the different antigenicities of recombinant proteins, the differences also suggest that the different duration and the quantities of these antigens are presented to the patient's immune system during disease progression. Detection of serum IgA to EBV gene products in the various phases of viral infection could then reflect, at least in part, the immunological reaction to the active processes of the virus in each patient. Other explanations are also possible. However, our results are consistent with the facts that EBNA-1 is essential for maintaining the episomal EBV while virus reactivation could take place by a yet-to- determine pathological mechanism in the patient [1,17,18]. Our previous results showed that complementation of EBNA-1 with that of lytic cycle-related EBV antigens provided a better predictive index than a single EBV antigen for the early detection of NPC [1].
Determination of serum IgA levels using a panel of EBV antigens from both latent and active phases in an immunoblot provided a better option for predicting treatment response of NPC and early detection of disease relapse. Furthermore, our current data are consistent with those found in other reports [1-4,8-11], and suggest that the viral gene expression in the tumor cells might be affected by the pathological microen- vironment. Details of the mechanism, how- ever, need further investigation.
A
AC CK KN NO OW WL LE ED DG GE EM ME EN NT T
This study was supported by China Medical College Hospital (DMR-88-038).
R
RE EF FE ER RE EN NC CE ES S
1. Chow KC, Ma J, Lin LS, et al. Serum responses to the combination of Epstein-Barr virus antigens from both latent and acute phases in nasopharyngeal carcinoma: complementary test of EBNA-1 with EA- D. Cancer Epidemiol Biomarkers Prev 1997;6:363-8.
2. Zeng Y, Zhang LG, Wu YC, et al. Prospective studies on nasopharyngeal carcinoma in Epstein-Barr virus
IgA/VCA antibody-positive persons in Wuzhou City, China. Int J Cancer 1985;36:545-7.
3. Ho HC, Ng MH, Kwan HC. Factors affecting serum IgA antibody to Epstein-Barr viral capsid antigens in nasopharyngeal carcinoma. Br J Cancer 1978;
37:356-62.
4. Zeng Y, Zhong JM, Li LY, et al. Follow-up studies on Epstein-Barr virus IgA/VCA antibody-positive persons in Zangwu County, China. Intervirology 1983;20:190-4.
5. Muir C, Waterhouse J, Mack T, et al. Cancer incidence in five continents. IARC Sci Publ 1987;5:840-1.
6. Zheng X, Yan L, Nilsson B, et al. Epstein-Barr virus infection, salted fish and nasopharyngeal carcinoma.
A case-control study in southern China. Acta Oncol 1994;33:867-72.
7. Chan SH, Day NE, Kunaratham N, et al. HLA and nasopharyngeal carcinoma in Chinese - a further study. Int J Cancer 1983;32:171-6.
8. Feinmesser R, Miyazaki I, Cheung R, et al. Diagnosis of nasopharyngeal carcinoma by DNA amplification of tissue obtained by fine-needle aspiration. N Engl J Med 1992;326:17-21.
9. Wu TC, Mann RB, Epstein JI, et al. Abundant expression of EBER1 small nuclear RNA in nasopharyngeal carcinoma. A morphologically distinctive target for detection of Epstein-Barr virus in formalin-fixed paraffin-embedded carcinoma specimens. Am J Pathol 1991;138:1461-9.
10. Henle W, Ho HC, Henle G, et al. Antibodies to Epstein-Barr virus-related antigens in nasoph- aryngeal carcinoma. Comparison of active cases with long term survivors. J Natl Cancer Inst 1973;
51:361-9.
11. de-Vathaire F, Sancho-Garnier H, de-The H, et al.
Prognostic value of EBV markers in the clinical management of nasopharyngeal carcinoma (NPC):
a multicenter follow-up study. Int J Cancer 1988;42:176-81.
12. Chao TY, Chow KC, Chang JY, et al. Expression of Epstein-Barr virus-encoded RNAs as a marker for metastatic undifferentiated nasopharyngeal carcinoma. Cancer 1996;78:24-9.
13. Ga z z o l o L , d e - T h e G , Vu i l l a u m e M , e t a l . Nasopharyngeal carcinoma. II. Ultrastructure of normal mucosa, tumor biopsies, and subsequent epithelial growth in vitro. J Natl Cancer Inst 1972;48:73-86.
14. Trumper PA, Epstein MA, Giovanella BC, et al.
Isolation of infectious EB virus from the epithelial tumor cells of nasopharyngeal carcinoma. Int J Cancer 1977;20:655-62.
15. Trumper PA, Epstein MA, Giovanella BC. Activation in vitro by BUdR of a productive EB virus infection in the epithelial cells of nasopharyngeal carcinoma.
Int J Cancer 1976;17:578-87.
16. Lo YM, Chan LY, Lo KW, et al. Quantitative analysis
of cell-free Epstein-Barr virus DNA in plasma of patients with nasopharyngeal carcinoma. Cancer Res 1999;59:1188-91.
17. Martel-Renoir D, Grunewald V, Touitou R, et al.
Quantitative analysis of the expression of Epstein-
Barr virus lytic genes in nasopharyngeal carcinoma biopsies. J Gen Virol 1995;76:1401-8.
18. Liebowitz D, Kieff E. Epstein-Barr virus. In: Roizman
B, Whitley RJ, Lopez C, eds. The Human
Herpesviruses. New York: Raven Press, 1993:107-72.
EB
1 2
1 2