Gas-Forming Pyogenic Liver Abscess
Developed after Drug-Eluting Bead Transarterial Chemoembolization Therapy for A Large
Hepatocellular Carcinoma: A Case Report and Review of Literature
Poh-Poo Lim, Lok-Beng Koay , Ching-Yih Lin, Ming-Jen Sheu, Hsing-Tao Kuo, Chi-Shu Sun, I-Che Feng, Yu-Min Lin, and Ping-Hsin Hsieh
Department of Internal Medicine, Division of Hepato-Gastroenterology, Chi Mei Medical Center
Abstract
Liver abscess after hepatic artery embolization is a rare but serious complication associated with significant morbidity and mortality. Here we report a 52-year-old case of chronic hepatitis B, liver cirrhosis and diabetes mellitus (DM) type 2 with a large gas forming liver abscess (11.4 cm) developed after transarterial chemoembolization (TACE) treatment for a large hepatocellular carcinoma (HCC). The condition responded well to four weeks of antibiotics treatment plus percutaneous drainage with continuous abscess regression after treatment. Infection of the necrotic tumor seems to be the cause of abscess formation in this case. We suggest that for patient with large tumor size, multiple risk factors such as DM, liver cirrhosis, associated biliary disease and old age; post TACE abscess formation should be highly aware of, investigated early and treated promptly. Prophylaxis antibiotics may also be considered. (J Intern Med Taiwan 2015; 26: 115-119) Key Words: Hepatocellular carcinoma, Drug-eluting bead transarterial chemoembolization, Liver abscess
Background
Transarterial chemoembolization (TACE) has become a useful treatment modality for manage- ment of unresectable hepatocellular carcinoma (HCC). It is an important palliative treatment for unresectable HCC and a bridge therapy before liver transplantation1. It has been proven to be a safe and effective procedure for treatment of primary liver cancer including HCC, neuroendocrine tumor, ocular
melanoma, cholangiocarcinoma and sarcoma2. Although rarely encountered, severe complications can develop, especially in patients with severe cir- rhosis and poor liver function reserve.
The most common adverse event is post-embo- lization syndrome3,4, presented as fever, nausea, vomiting and abdominal pain lasting for a few hours to a few days. Other severe and rare complications include hepatic artery occlusion, spontaneous tumor rupture, liver abscess, pulmonary embolism and
Reprint requests and correspondence:Dr. Lok-Beng Koay
Address: Department of Internal Medicine, Division of Hepato-Gastroenterology, Chi Mei Medical Center, No.901, Zhonghua Rd., Yongkang Dist., Tainan City 710, Taiwan
perforation of duodenum5,6. Of these rare compli- cations, hepatic abscess is rarely encountered and fatal, the incidence was 0-3.3%3,5,7. We herein pre- sented a case with huge hepatoma complicated with liver abscess formation after TACE. Literatures of the mechanisms, the risk factors and the manage- ment of TACE induced liver abscess were reviewed.
Case report
A 52 year-old man with history of chronic hep- atitis B, liver cirrhosis (Child-Pugh score 5, classifi- cation A) and diabetes mellitus type 2, was admitted to our hospital due to gallbladder stone and a large HCC. Four phase dynamic abdominal computed tomography (CT) shows a lobulated hypodense lesion (about 9.3 x 7.2 x 7.9 cm in size) with early arterial enhancement and late venous phase wash out in segment 5 and 6 of right liver lobe (Figure 1), with marked elevated alpha-fetoprotein level (681.1 ng/mL) confirmed as HCC. The stage was Barce- lona clinical liver cancer (BCLC) stage B. Patient refused surgical treatment that he received a drug eluting bead TACE treatment.
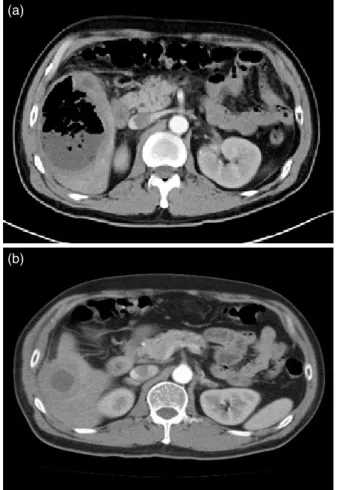
Superselective chemoembolization was per- formed using epirubicin 75 mg and drug-eluting bead (DC bead, 300 -500 μm) embolization. Fever developed on post procedure day 1, post emboliza- tion syndrome was impressed initially. However, due to high fever and chills persisted, blood culture was performed and empiric antibiotic was pre- scribed on post procedure day 3. We had consult infection doctor since fever was not subsided on post procedure day 7, and antibiotic was shifted to ciprofloxacin according to the culture result and drug susceptibility test. Abdominal CT (at day 14) revealed a lobulated lesion with gas and fluid density in segment 5 and 6 treatment site (Figure 2a), gas forming liver abscess developed after TACE was impressed.
A 10-French percutaneous pigtail drain was placed and cultures from the abscess grew
Figure 1. Four phase dynamic abdominal CT shows a lobulated hypodense lesion about 9.3 x 7.2 x 7.9 cm in size with early arterial enhancement and late venous phase wash out in segment 5 and 6 of right liver lobe, diagnosed as HCC.
Figure 2. (a) Abdominal CT performed 14 days after TACE showed a large gas forming abscess;
(b) three months after treatment showed regression of abscess and hepatoma in right liver lobe.
(a)
(b)
Enterobacter clocae, consistent with blood culture result. The abdominal pain and anorexia of this patient improved and fever subsided three days after treatment. Follow up abdominal ultrasonography showed regression of abscess size (from 9.8 cm to 4.3 cm, Figure 3a&b) after three weeks of combined antibiotics treatment with drainage.
Serial ultrasonography follow up after dis- charge showed continued regression of abscess and the latest abdominal CT (3 months post-TACE) reported interval regressed of hepatic abscess and tumor (Figure 2b).
Discussion
Liver abscess following hepatic artery embo- lization is a rare but serious complication associ- ated with significant morbidity and mortality. The incidence of abscess formation after TACE ranged
from 0 to 3.3%3,5,7. Common symptoms of TACE induced liver abscess included pain, high-grade fever, nausea, and vomiting 2-4 weeks after treat- ment8. These symptoms should be differentiated from post embolization syndrome, which usually occurs within the first 72 hours, with less severity.
It should be noted that if fever, chills and abdominal pain persists for more than 7 days after TACE, liver abscess should be suspected7,8.
Further image studies, such as gas collection at right upper abdomen on plain abdomen radiog- raphy should raise the suspicious of abscess forma- tion; and single or multiple hypodense lesions on abdominal CT can be evidence of liver abscess for- mation after TACE7. Sometimes, gas forming in the necrotic tissue or air trapped in embolic agent can confound gas forming in an abscess, which occurs in 20-29% of all pyogenic liver abscess7. Diagnostic aspiration is the mainstay for definite diagnose in this situation. We were hesitated for performing this procedure due to the concern of tumor seeding, reported to be occurred in 0% to 11%9. In this case, owing to persistent high fever despite antibiotics treatment, we performed CT examination on day 14 after TACE, was a little bit late for diagnosis of abscess formation. It would be better if CT was arranged immediately after positive blood culture for earlier detection of abscess formation.
Ischemic destruction of the intrahepatic ducts, secondary occlusion of the peribiliary arterial plexus by lipiodol and toxic effects of anticancer drugs on vascular endothelial cells are important mechanism of post TACE liver abscess formation10,11. Other causes included bacterial infection superimposed after liver embolization, procedure related infection and immunosuppressant effect of chemotherapeutic agents5.
The most common predisposing risk factors were history of bilioenteric anastomosis or incompe- tent sphincter of Oddi from stenting or prior sphinc- terotomy12,13, up to 7.4% abscess rate reported13. Figure 3. Serial abdominal ultrasonography follows up
showed continual abscess regress. (a) Post TACE day 11 and (b) 30 days after treat- ment.
(a)
(b)
Other risk factors included portal vein thrombosis, biliary disease, large tumor size and gastrointes- tinal malignancy14. It is reasonable to use prophy- lactic antibiotics with coverage of skin and gram negative enteric organisms in patient with these risk factors12,15,16. In our case, large tumor size and asso- ciated biliary disease (liver cirrhosis and gallbladder stones) seemed to be the predisposing risk factors.
There is not yet a conclusion of higher abscess rate in drug-eluting bead TACE than conventional TACE despite that higher abscess rate of drug-eluting bead TACE had been reported by Malagari et al.17
Once liver abscess is diagnosed, early percu- taneous drainage and broad-spectrum intravenous antibiotics are the first line treatment. Systemic antibiotic treatment alone is probably adequate for small abscesses less than 5 cm in diameter18; while abscesses larger than 5 cm diameter might need pigtail or surgical drainage combined with antibi- otics. The most commonly used antibiotics were second and third-generation cephalosporins (74%) follow by metronidazole (31%) and the penicillin group of antibiotics (19%)18.
However, the outcome of pyogenic liver abscess after TACE was not favorable. Age and abscess size are unfavorable predictors of disease outcome.
Larger abscesses are more destructive to the liver, have higher risk of sepsis and hepatic failure, and are especially harmful for patients with underlying hepatitis or cirrhosis14. The poorer immunity and comorbidities of older patients also result in higher mortality. In our case, poor prognostic factors included large abscess size (11.4 cm) and multiple comorbidities (liver cirrhosis and diabetes mellitus type 2). Poor prognosis was initially expected but fortunately, after vigorous treatment with percuta- neous drainage and broad-spectrum antibiotics, the patient survived and recovered.
Conclusion
TACE induced liver abscess is rare but fatal and
associate with significant morbidity and mortality.
Having a high clinical suspicion of this complica- tion is important in recognizing this severe compli- cation. Patient with old age, multiple comorbidities and larger tumor size should be aware due to their higher mortality. Prophylaxis antibiotics may also be considered in patients with predisposing factors.
References
1. Rammohan A, Sathyanesan J, Ramaswami S, et al. Emboliza- tion of liver tumors: Past, present and future. World J Radiol 2012; 4: 405-12.
2. Brown DB, Geschwind JF, Soulen MC, et al. Society of Inter- ventional Radiology position statement on chemoemboliza- tion of hepatic malignancies. J Vasc Interv Radiol 2006; 17:
217-23.
3. Poggi G, Pozzi E, Riccardi A, et al. Complications of image- guided transcatheter hepatic chemoembolization of primary and secondary tumours of the liver. Anticancer Res 2010; 30:
5159-64.
4. Tasneem AA, Abbas Z, Luck NH, et al. Adverse events following transarterial chemoembolization for hepatocellu- lar carcinoma and factors predicting such events. J Pak Med Assoc 2013; 63: 239-44.
5. Xia J, Ren Z, Ye S, et al. Study of severe and rare compli- cations of transarterial chemoembolization (TACE) for liver cancer. Eur J Radiol 2006; 59: 407-12.
6. Sakamoto I, Aso N, Nagaoki K, et al. Complications asso- ciated with transcatheter arterial embolization for hepatic tumors. Radiographics 1998; 18: 605-19.
7. Chen C, Chen PJ, Yang PM, et al. Clinical and microbiologi- cal features of liver abscess after transarterial embolization for hepatocellular carcinoma. Am J Gastroenterol 1997; 92:
2257-9.
8. Vanderwalde AM, Marx H, Leong L. Liver abscess as a complication of hepatic transarterial chemoembolization: a case report, literature review, and clinical recommendations.
Gastrointest Cancer Res 2009; 3: 247-51.
9. Stigliano R, Marelli L, Yu D, et al. Seeding following percuta- neous diagnostic and therapeutic approaches for hepatocellu- lar carcinoma. What is the risk and the outcome? Seeding risk for percutaneous approach of HCC. Cancer Treat Rev 2007;
33: 437-47.
10. Sun Z, Li G, Ai X, et al. Hepatic and biliary damage after tran- sarterial chemoembolization for malignant hepatic tumors:
incidence, diagnosis, treatment, outcome and mechanism.
Crit Rev Oncol Hematol 2011; 79: 164-74.
11. Kim MH, Choi MS, Choi YS, et al. Clinical features of liver abscess developed after radiofrequency ablation and tran- sarterial chemoembolization for hepatocellular carcinoma.
Korean J Hepatol 2006; 12: 55-64.
12. Mezhir JJ, Fong Y, Fleischer D, et al. Pyogenic abscess after hepatic artery embolization: a rare but potentially lethal complication. J Vasc Interv Radiol 2011; 22: 177-82.
13. Song SY, Chung JW, Han JK, et al. Liver Abscess after Tran- scatheter Oily Chemoembolization for Hepatic Tumors: Inci- dence, Predisposing Factors, and Clinical Outcome. J Vasc Interv Radiol 2001; 12: 313-20.
14. Ong GY, Changchien CS, Lee CM, et al. Liver abscess compli- cating transcatheter arterial embolization. Eur J Gastroenterol Hepatol 2004; 16: 737-42.
15. Geschwind JF, Kaushik S, Ramsey DE, et al. Influence of a New Prophylactic Antibiotic Therapy on the Incidence of Liver Abscesses after Chemoembolization Treatment of Liver Tumors. J Vasc Interv Radiol 2002; 13: 1163-6.
16. Venkatesan AM, Kundu S, Sacks D, et al. Practice guidelines for adult antibiotic prophylaxis during vascular and inter- ventional radiology procedures. Written by the Standards of
Practice Committee for the Society of Interventional Radi- ology and Endorsed by the Cardiovascular Interventional Radiological Society of Europe and Canadian Interven- tional Radiology Association. J Vasc Interv Radiol 2010; 21:
1611-30.
17. Malagari K, Chatzimichael K, Alexopoulou E, et al. Tran- sarterial chemoembolization of unresectable hepatocellular carcinoma with drug eluting beads: results of an open-label study of 62 patients. Cardiovasc Intervent Radiol 2008; 31:
269-80.
18. Wong WM, Wong BC, Hui CK, et al. Pyogenic liver abscess:
retrospective analysis of 80 cases over a 10-year period. J Gastroenterol Hepatol 2002; 17: 1001-7.
巨大肝細胞癌經載藥微球肝動脈化療栓塞術後 併發化膿性肝膿瘍:病例報告以及文獻回顧
林寶寶 郭樂明 林勤益 許銘仁 郭行道 孫啟書 馮意哲 林育民 謝秉欣
奇美醫學中心 內科部胃腸肝膽科
摘 要
經肝動脈栓塞術後併發肝膿瘍是一種罕見但嚴重的併發症,並且伴隨著顯著的死亡率。
我們報告一名52歲慢性 B 肝肝硬化以及第二型糖尿病的病患,住院診斷為巨大肝癌後進行載
藥微球肝動脈化療栓塞術。然而術後持續地發燒長達一個星期,因此安排腹部電腦斷層檢查
顯示腫瘤嚴重壞死合併肝膿瘍達11.4厘米。隨後我們使用了經皮引流管放置以及強效抗生素
治療。經過三週的治療,追蹤腹部超音波顯示膿瘍逐漸縮小,臨床症狀也有顯著的改善。患 者出院後在門診持續地追蹤,每三個月的腹部超音波顯示膿瘍以及腫瘤持續消退中。對於高 齡、多種合併症以及較大的腫瘤患者,我們應該意識到其在經肝動脈栓塞後的併發症會有高 危險性,因此須提高警覺提早診斷及積極治療。