Objective: Many studies have constructed predictive models for outcome after traumatic brain injury. Most of these attempts focused on dichotomous result, such as alive vs dead or good outcome vs poor outcome. If we want to predict more specific levels of outcome, we need more sophisticated models. We conducted this study to determine if artificial neural network modeling would predict outcome in five levels of Glasgow Outcome Scale (death, persistent vegetative state, severe disability, moderate disability, and good recovery) after moderate to severe head injury. Methods: The database was collected from a nation-wide epidemiological study of traumatic brain injury in Taiwan from July 1, 1995 to June 30, 1998. There were total 18583 records in this database and each record had thirty-two parameters. After pruning the records with minor cases (GCS13) and missing data in the 132 variables, the number of cases decreased from 18583 to 4460. A step-wise logistic regression was applied to the remaining data set and 10 variables were selected as being statically significant in predicting outcome. These 10 variables were used as the input neurons for constructing neural network. Results: Overall, 75.8% of predictions of this model were correct, 14.6% were pessimistic, and 9.6% optimistic. This neural network model demonstrated a significant difference of performance between different levels of Glasgow Outcome Scale. The prediction performance of dead or good recovery is best and the prediction of vegetative state is worst. Conclusion: An artificial neural network may provide a useful“second opinion” to assist neurosurgeon to predict out-come after traumatic brain injury.
Key words: head injury, artificial neural network, outcome prediction
Taipei City Med J 2005; 2 (3):272-277
Outcome Prediction in Moderate or Severe Head Injury
Using an Artificial Neural Network
Min-Huei Hsu, M.D., MSc.
1,3, Yu-Chuan Li, M.D., Ph.D.
4, Wen-Ta Chiu, M.D., Ph.D.
5,
Ju-Chuan Yen, M.D.
21Department of Neurosurgery and2Ophthalmology, Zhongxiao Branch, Taipei City Hospital;3Graduate Institute of Medical Sciences, 4Graduate Institute of Medical Informatics, Taipei Medical University;5Taipei Municipal Wanfang Hospital.
Received: 6 December 2004; Accepted: 2 March 2005.
Correspondence to: Dr. Ju-Chuan Yen, Department of Ophthalmology, Zhongxiao Branch, Taipei City Hospital, No. 87, Tongde Road, Nangang District, Taipei 115, Taiwan.
Introduction
Considerable effort has been devoted to improv-ing our ability to predict outcome after traumatic brain
injury (TBI). More reliable prediction of outcome would be helpful for clinicians as an important aid to decision making about management and for commu-nication with relatives and other healthcare
professionals.
Mathematical and statistical methods have been used to develop models for outcome prediction. The most commonly used methods include Bayes’ theo-rem[1], logistic regression and neural networks.[2]
An artificial neural network is a computerized construct consisting of input neurons (which pro-cess input data) connected to hidden neurons (to mathematically manipulate values they receive from all the input neurons) connected to output neurons (to output a prediction). Artificial neural networks have been successfully used for pattern recognition and outcome prediction in several clinical settings. The advantage of a neural network is the ability of the model to capture nonlinearities and complex in-teractions between factors related to the outcome of interest. Neural networks differ from other decision support systems in that the learning occurs by ex-ample through training and not by programming or pre-defined rules.
We conducted this study to determine if artifi-cial neural network modeling would predict outcome using five levels of Glasgow Outcome Scale[3](death,
persistent vegetative state, severe disability, moder-ate disability, and good recovery) after modermoder-ate and severe head injury ( initial Glasgow Coma Scale-Score
of 3-12 )
Materials and Methods
This study was conducted using data collected from a nation-wide epidemiological study of trau-matic brain injury in Taiwan from July 1, 1995 to June 30, 1998. One hundred and sixteen large to medium-sized teaching hospitals with qualified neu-rosurgeon participated in this study. There were to-tal 18583 records in this database. The causes of head trauma were traffic crashes (14354 cases, of whom more than 65% were motorcycle crash victims), falls (2534 cases), and others (1695 cases). The mean age of the victims was 36.5 +/- 15.3 (SD), range 1 to 85 years old. In 7.8% of the cases, the victims were older than 60. The male to female ratio was about 3:1.
One hundred and thirty-two parameters includ-ing age, gender, causes of head trauma, GCS scores at the emergency department, CT findings and cran-iotomy for intracranial hematoma were recorded for each patient. The outcome was estimated by the Glasgow Outcome Scale (GOS), and was assessed as longer as 12 months after injury if possible.
After pruning the records with mild cases (GCS ≧ 13) and missing data in the 132 variables , the number of cases decreased from 18583 to 4460. In the second step, a step-wise logistic regression was applied to the remaining data set and 10 variables (Table 1) were selected as being statically signifi-cant (p<0.05) in predicting of the dependent vari-able (Glasgow Outcome Scale).
From the 4460 cases, 75% were randomly se-lected as the training group (n=3345) in the develop-ment of the neural network models. The validation group (n=1115) was used to test the performance of this model. Generalized regression neural network software was used (NeuralShell Classifier Version 2; Ward Systems Group; Frederick, MD).
Age
Number of nonreactive pupils Score of motor resonse Score of verbal response Score of eye opening
Use of helmet in motorcycle crash Intracerebral hematoma on CT Subdural hematoma on CT
Craniotomy for intracranial hematoma Alcohol-related traffic accident
Table 1. Variables as input neurons in the ANN
The accuracy, sensitivity and specificity are used to describe the performance of the predictive model.
Results
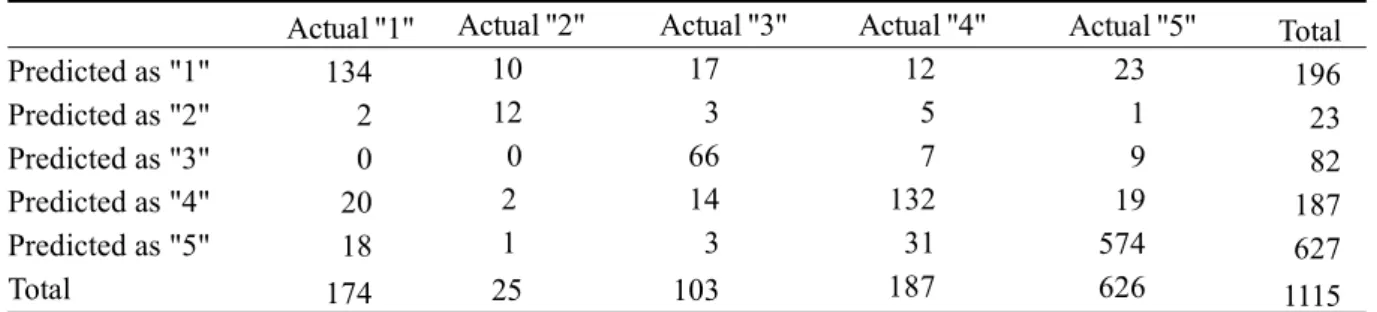
The prediction results from the artificial neural etwork are shown in Table 2. As can be seen from he diagonal cells in the contingency table, Overall, 5.8% of predictions were correct, 14.6% were pes-simistic (outcome better than predicted), and 9.6% optimistic (outcome worse than predicted). For pa-tients with good recovery, 91.6 % of predictions ere correct. For patients with moderate disability, 70.5% of predictions were correct. For patients with severe disability, 64.0% of predictions were correct. For death, 77.0% of prediction were correct but for vegetative state only 48.0% of prediction were correct. The sensitivity and specificity for each level are shown in Table 3.
Discussion
Approaches to developing prognostic models vary from using traditional probabilistic techniques, originating from the field of statistics, to more quali-tative and model-based techniques, originating from the field of artificial intelligence (AI).
Until recently, attempts to predict outcome have focused on dichotomous result, such as alive vs dead or good outcome vs poor function.[4]The use of single
variables, such as GCS[5], image finding[6],
intracra-ial pressure[7]or cerebral blood flow[8], has allowed
for a reasonable degree of accuracy in predicting those outcomes. With increased interest in predict-ing more specific levels of function, however, more sophisticated models are required. Such models re-quire inclusion of multiple variables and better algorithm.
The neural network model developed in this study provided acceptable performance of overall outcome prediction. However it demonstrated a sig-nificant difference of performance between differ-ent levels of prediction. The prediction performance of dead or good recovery is best and the prediction
Predicted as "1" Predicted as "2" Predicted as "3" Predicted as "4" Predicted as "5" Total Actual "1" 134 2 0 20 18 174 Actual "2" 10 12 0 2 1 25 Actual "3" 17 3 66 14 3 103 Actual "4" 12 5 7 132 31 187 Actual "5" 23 1 9 19 574 626 Total 196 23 82 187 627 1115
Table 2. Actual and predicted outcome for 1115 patients.
1=death, 2=vegetative, 3= severe disability, 4= moderate disability, 5=good recovery.
Sensitivity Specificity 1 77.01% 93.41% 2 48.00% 98.99% 3 64.08% 98.42% 4 70.59% 94.07% 5 91.69% 89.16%
Table 3. The sensitivity and specificity of prediction.
of vegetative state is worst. This may be due to the small case number of the vegetative group in this study.
In most outcome prediction studies of TBI patients, death and vegetative state are combined as a single level (poor outcome). However, these two states have significant difference for clinicians and patient’s relatives. Some people even think survival in a persistent vegetative state is worse than death. Any model could predict persistent vegetative state in early stage would be very helpful for clinicians in assisting treatment limiting decisions. But the pre-dictive power of our model is still not good enough for that purpose.
We excluded the mild cases in our study, be-cause most these patients will have a good recovery. Including mild cases could let prediction models have better performance without clinical significance.
Many other authors have shown age[9,10], GCS
score, pupillary responsiveness[11,12]and findings of
computed tomography (CT) to be significant pre-dictors of outcome after traumatic brain injury. In our study, use of helmet in motorcycle crash was a significant outcome predictor. Before implementa-tion of the motorcycle helmet use law, motorcycle collisions accounted for 74% of the traffic accidents in Taiwan, and most of the motorcycle riders were not helmet users. The motorcycle-related deaths have reached 48 percent of all motor vehicle-related deaths.[13]After implementation the helmet law in
Taiwan on June 1, 1997, the mortality and morbidity from motorcycle-related head injuries decreased ef-fectively in Taiwan.[14]
Although the ANN is a valuable method for out-come prediction, some of its nature should be noted before it can be widely applied. One is the‘black box’ nature of the ANN, which means that the logi-cal procedure of how networks determine a predic-tion cannot be observed. Hart and Wyatt believe that this“black box” aspect is a major obstacle to the
acceptance of neural nets as part of medical deci-sion support systems.[15]
Accurate prediction of outcome in the individual patient remains difficult to achieve for both clini-cians and computer program. Our research indicates that an artificial neural network may provide a use-ful“second opinion” to assist neurosurgeon to pre-dict outcome after traumatic brain injury.
References
1. Barlow P, Teasdale GM, Jennett B, et al: Com-puter assisted prediction of outcome of severely head-injured patients. J Microcomputer Appl 1984; 7:271-7.
2. Lang EW, Pitts LH, Damron SL, Rutledge R: Outcome after severe head injury: an analysis of prediction based upon comparison of neu-ral network versus logistic regression analysis. Neurol Res 1997; 19(3):274-80.
3. Jennett B, Bond M: Assessment of outcome after severe brain damage. A practical scale. Lancet 1975; 1:480.
4. Benzer A, Mitterschiffthaler G, Marosi M, et al: Prediction of non-survival after trauma. Lancet 1991; 338:977-8.
5. J e n n e tt B , Te a s d a le G , B r a a kma n R , Minderhoud J, Knill-Jones R: Predicting out-come in individual patients after severe head injury. Lancet 1976; 1(7968):1031-4.
6. van Dongen KJ, Braakman R, Gelpke GJ: The prognostic value of computerized tomography in comatose head-injured patients. J Neurosurg 1983; 59:951.
7. Czosnyka M, Guazzo E, Whitehouse M, et al: Significance of intracranial pressure waveform analysis after head injury. Acta Neurochir 1996; 138(5):531-41.
8. Kelly DF, Martin NA, Kordestani R, et al: Ce-rebral blood flow as a predictor of outcome
following traumatic brain injury. J Neurosurg 1997; 86(4):633-41.
9. Luerssen TG, Klauber MR, Marshall LF: Age and outcome from head injury: A longitudinal prospective study of adult and pediatric head injury. J Neurosurg 1988; 68:409.
10. Vollmer DG, Torner JC, Jane JA, et al: Age and outcome following traumatic coma: Why do older patients fare worse? J Neurosurg 1991; 75:S37.
11. Price DJ, Knill-Jones R: The prediction of out-come of patients admitted following head in-jury in coma with bilateral fixed pupils. Acta Neurochir 1979; Suppl 28:179.
12. Jennett B, Teasdale G, Braakman R, et al: Pre-dicting outcome in individual patients after se-vere head injury. Lancet 1976; 1:1031. 13. Chiu WT: The motorcycle helmet law in
Taiwan. JAMA 1995; 274(12):941-2.
14. Chiu WT, Kuo CY, Hung CC, Chen M: The effect of the Taiwan motorcycle helmet use law on head injuries. Am J Public Health 2000; 90(5):793-6.
15. Hart A, Wyatt J: Evaluating black-boxes as medical decision aids: issues arising from a study of neural networks. Med Inform 1990; 15: 229-36.
目的:目前已知之頭部外傷預後預測模式大多為兩 極性結果之選擇,如存活相對於死亡;良好的預後相對 於不良之預後。如欲預測更詳細的預後等級則需建構更 複雜的預測模式。方法:在本實驗中我們嘗試以類神經 元網路預測中重度頭部外傷病患在格拉斯哥預後量表中 五個等級(死亡、植物人狀態、嚴重殘障、中度殘障、恢 復良好)之落點。分析資料來源為臺灣頭部外傷資料庫 1995 年 6 月 1 日至 1998 年 5 月 30 日收錄之個案。資料庫 中共有18583筆資料,每筆資料有132個變數。在剔除輕 關鍵詞:頭部外傷,類神經元網路,預後預測。 北市醫學雜誌 2005; 2 (3):272-277