Original Investigation Title:
Separate and joint effects of diabetes mellitus and chronic kidney disease on the risk of acute coronary syndrome – a population-based cohort study.
Authors:
Yu-Tzu Chang, MD, MSc1,2Chih-Ching Liu, MSc,3,4Liang-Miin Tsai, MD, 1Chung- Yi Li, PhD,4,5*Junne-Ming Sung, MD,1, 4,*
Institutions:
1Department of Internal Medicine, National Cheng Kung University Hospital, Tainan.
2Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
3Health Promotion Administration, Ministry of Health and Welfare, Taipei, Taiwan.
4Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
5Department of Public Health, College of Public Health, China Medical University, Taichung, Taiwan.
Running head (short title): Effects of CKD and DM on ACS
*Corresponding authors:
Junne-Ming Sung
Department of Internal Medicine and Department of Public Health, National Cheng Kung University and Hospital, 138 Sheng-Li Rd., Tainan 70428, Taiwan. Email:
[email protected] . Tel: +886-6-2353535 ext: 2591. Fax: +886-6-2766175.
or
Chung-Yi Li
Department of Public Health, National Cheng-Kung University, 138 Sheng-Li Rd., Tainan 70428, Taiwan. E-mail: [email protected]. Tel: +886-6-2353535 ext:
5862. Fax: +886-6-2359033.
1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
1 2
Abbreviations:
ACS Acute coronary syndrome AHR Adjusted hazard ratio CHD Coronary heart disease CKD Chronic kidney disease CV Cardiovascular
DM Diabetes mellitus
ESRD End-stage renal disease
ICD-9 International Statistical Classification of Diseases and Related Health Problems, 9th edition
ICD-9-CM International Statistical Classification of Diseases and Related Health Problems, 9th edition, Clinical Modification
IR Incidence rate
NHI National Health Insurance
NHIRD National Health Insurance Research Database 35
36 37 38 39 40 41 42 43 44 45 46 47 48 49
Abstract:
Patient with diabetes (DM) and chronic kidney disease (CKD) are at a higher risk of developing acute coronary syndrome (ACS). However, only a few studies have investigated the separate and joint effects of DM and CKD on the risk of ACS, especially population-based studies under age-, sex- and various cardiovascular risk factor-stratifications. By using a national diabetes cohort derived from the Taiwan National Health Insurance Research Database, we identified a total of 416,143 DM and 541,724 non-DM patients, including 51,208 DM/CKD and 8,894 non-DM/CKD patients, in 2000 who did not have a history of ACS (ICD-9: 410.x, 413.9, 411.1) before 2000. We then prospectively investigated the incidence of ACS by linking to inpatient claims data from 2000-2007. A Cox proportional hazard model was used to estimate the relative risk of ACS in individuals with DM and/or CKD under various
stratifications.
Age- and sex-specific incidence rates were similar between the non-DM/CKD and DM/non-CKD groups, except for female patients under 45 years, in whom DM was associated with a higher risk of ACS than CKD (8.21 vs. 3.82 per 1000 person-years).
In the group aged <45 years, the DM/non-CKD patients were associated with a higher relative hazard of ACS than those in the non-DM/CKD group when compared with the non-DM/non-CKD group (men: adjusted hazard ratios [AHR]:1.77; 95%
confidence interval [CI]:1.61-1.93 vs. 1.42 [95% CI:0.73-2.73]; women 1.97 [95%
3
50 51 52 53 54 55 56 57 58 59 60 61
62 63 64 65 66 67 68 69
7 8
CI:1.76-2.20] vs. 1.13 [95% CI:0.36-3.52]). This discrepancy in AHR was reduced with increasing age. The co-existence of DM and CKD further enhanced the AHR in a
multiplicative independent manner. A significant age-modification effect was noted in the DM individuals regardless of their CKD status, but not in the non-DM/CKD
group. In stratification by various cardiovascular risk factors, diabetes had a higher risk of ACS than CKD in patients with ≤ 2 selected risk factors, with the exception of the hyperlipidemia and hypertension subgroup. When all three selected risk factors were included, CKD was associated with a higher risk of ACS than DM
(AHR:1.43[1.27-1.60] vs. 1.25[1.22-1.29]). In conclusion, DM and CKD were associated with different levels of risk for ACS according to age, sex and certain
cardiovascular risk factors. Strategies aimed at preventing ACS should therefore be individualized according to the presence of DM, CKD and various cardiovascular risk factors.
70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86
Introduction:
Diabetes mellitus (DM) and chronic kidney diseases (CKD) are a growing threat to public health1-6. The number of patients with CKD and DM had risen abruptly in the past few decades worldwide, and management for the related complications characteristic of both illnesses has been associated with a heavy medical financial burden in many countries5,7-9. Cardiovascular diseases, including acute coronary syndrome (ACS), are among the major causes of morbidity and mortality in patients with CKD and DM, and the risk for cardiovascular events has been reported to exit even in the early stages of both illnesses2,3,7,10. Therefore, patients with CKD or DM are considered to be at a very high risk of developing coronary heart disease (CHD),
or even a CHD equivalent3,11-15.
Aging and male gender are two known detrimental risk factors for coronary
events. DM and CKD have also been reported to increase the risk of developing coronary events, however little is known about the age-specific coronary effects that occur in association with DM and/or CKD. In addition, only a very few studies have simultaneously investigated both the separate and combined effects of DM and CKD on the risks of coronary events via head-to-head comparisons16-18. Moreover, DM and CKD usually co-exist with many common risk factors for coronary events, such as hyperlipidemia and hypertension. How the presence of DM and/or CKD per se,
5
87 88 89 90 91 92 93 94 95 96
97 98 99 100 101 102 103 104 105
13 14
independently of these coronary disease risk factors, further increase the risk of coronary events is still unclear. This study aimed to investigate the risks for first ever cases of ACS onset in relation to DM and CKD both separately and jointly across different spectra, including age, sex, and selected cardiovascular risk factors (i.e., hypertension, hyperlipidemia, and previous CHD history) in a nationally
representative diabetic cohort selected from the National Health Insurance Research Database (NHIRD).
106 107 108 109 110 111 112
113 114
Methods:
Data source
The Taiwan National Health Insurance (NHI) program was initiated in March 199519. Up to 99% of the 23 million residents of Taiwan currently receive medical care through the NHI program. In addition, over 96% of the hospitals (including over 100 regional and tertiary care hospitals) and clinics in Taiwan are contracted to provide health care services, which are reimbursed by the Bureau of NHI, and all data related to these services are collected and input into the NHIRD by the National Health Research Institutes (NHRI) to provide a comprehensive record of medical care19. The NHRI release these data for research purposes, and numerous high quality studies have been published based on data from the NHIRD20-24. The in-hospital health care database makes an epidemiological study of ACS in relation to DM and/or CKD possible, because nearly all patients with ACS are hospitalized in order to receive
optimal medical care.
Identification of diabetic, non-diabetic, CKD and dialysis groups
In this study, we used an established diabetes cohort, which included 615,532 diabetic and 614,871 age- and sex-matched control subjects selected from the NHIRD from 1997-2000 after ethical approval by the NHRI. Details of this diabetes cohort
have been described previously20. Briefly, a diabetes-related diagnosis was coded using the International Statistical Classification of Diseases and Related Health
7
115 116 117 118 119 120 121 122 123 124 125 126 127
128 129 130 131 132 133 134
19 20
Problems, 9th edition (ICD-9) code 250 or A181. All patients who had an initial diabetes-related diagnosis in the year 2000 and another diagnosis within the same year were classified into the diabetes group, with the interval between these two visits of more than 30 days. Individuals who had been admitted to hospitals for any kind of
malignancy (ICD-9:140-208) from 1997-1999 were then excluded. The index date in this group was defined as the date of their first visit for diabetes care in 2000. In the non-diabetes group, any subject diagnosed as having diabetes or malignancy during 1997-1999 was excluded. Using a sex- and age-matched technique, a total of 614,871 non-diabetic individuals were chosen. The index date in the non-diabetes group was defined as the date when each subject enrolled in the NHI program. If the first date of
enrollment was before January 1, 2000, the index date was set as January 1, 2000.
We defined the diagnosis of CKD as the following ICD-9-CM codes:016.0, 095.4, 189.0, 189.9, 223.0, 236.91, 250.4, 271.4, 274.1, 283.11, 403.×1, 404.×2, 404.×3, 440.1, 442.1, 447.3, 572.4, 580-588, 591, 642.1, 646.2, 753.12-753.17, 753.19, 753.2, and 794.4, in accordance with the recommendations from the United States Renal Data System report25. Patients who had made at least two visits (with the interval between the two visits being more than 30 days) for CKD care in an
outpatient clinic within one year or had been diagnosed with CKD from inpatient claims during 1997-1999 were defined as having CKD. Patients on dialysis were 135
136 137 138 139 140 141 142 143 144
145 146 147 148 149 150 151 152 153
identified from outpatient or inpatient claims using ICD-9 code: 585.6 combined with
copayment code “001”, which indicated the presence of a catastrophic illness. In addition, patients with a diagnosis of ACS and those receiving dialysis during 1997-
1999 were excluded.
The enrolled patients were further divided into the following groups: 1.non-
DM/non-CKD group; 2.non-DM/CKD group; 3.DM/non-CKD group; and 4.DM/CKD group. The follow-up period, from January 1, 2000 to December 31, 2007, was used to establish the onset of ACS. The incidence of CKD during the follow-up period for the DM/non-CKD group was three to four times higher than that of the non-DM/non-CKD group, and this may have caused significant statistical bias in the analyses. Therefore, the patients in these two groups with new physician- diagnosed CKD during the follow-up period were excluded. Since the incidence of new-onset diabetes did not increase in the CKD patients26, they were not excluded
(Figure 1).
Endpoint of the study
The endpoint of this study was the initial onset of ACS during the eight-year follow-up period. Since nearly all patients with ACS are hospitalized for optimal medical care, only inpatients with a discharge diagnosis of ICD-9-CM codes 410.X (acute myocardial infarction), 413.9 (unstable angina), and 411.1 (intermediate
9
154 155 156
157 158 159 160 161 162 163 164 165 166
167 168 169 170 171 172
25 26
syndrome) were defined as having reached the end point. The index date of the endpoint was defined as the first day of hospitalization. When patients died due to causes unrelated to ACS, or they required maintenance dialysis during the follow-up
period, the date of mortality or receiving dialysis was defined as the date of censoring.
Identification of clinical risk factors and other covariates
Certain clinical risk factors, including hypertension (ICD-9:401–402, 405, A260), hyperlipidemia (ICD-9: 272.0–272.4, A182), and CHD (ICD-9: 414.8 and 414.9) were identified for analysis and risk factor-stratification. The patients who had been diagnosed as having these risk factors before reaching the endpoint or prior to censoring were considered to have these co-morbidities. The age of each subject was calculated by the difference between the index date and the date of birth. Moreover, the geographic area of the patients was defined as the location of their NHI unit,
which was likely the area of their residence or workplace.
Statistical methods
The age- and sex-specific incidence rates (IRs) expressed as person-years were calculated using the Poisson assumption. Cox proportional hazard regression models were conducted to analyze the overall, sex- and age-specific effects of diabetes and CKD, both separately and jointly, on the risk of ACS. The Cox model was further used to assess the risk of ACS in the patients with diabetes or CKD and various cardiovascular risk factors. Aside from the common ACS risk factors, including age, 173
174 175
176 177 178 179 180 181 182 183 184
185 186 187 188 189 190 191 192
sex, hypertension, hyperlipidemia and previous CHD history15,27-30, we adjusted for insurance premium as a surrogate marker of socioeconomic status31, which was an independent risk factor for ACS, in the Cox model. Since an urban-rural difference has been reported to affect the accessibility and utilization of medical care in Taiwan32, geographic area was also adjusted for in the Cox model. The potential
effect-modification by sex (or age) for the relationships between DM/CKD and ACS was assessed according to the statistical significance of the interaction term of DM/CKD and sex (or age). All statistical analyses were performed with SAS version 9.2 (SAS Institute, Cary, NC.) A p value < 0.05 was considered statistically
significant.
11
193 194 195 196 197 198 199 200 201 202
31 32
Results:
The baseline characteristics of the study population
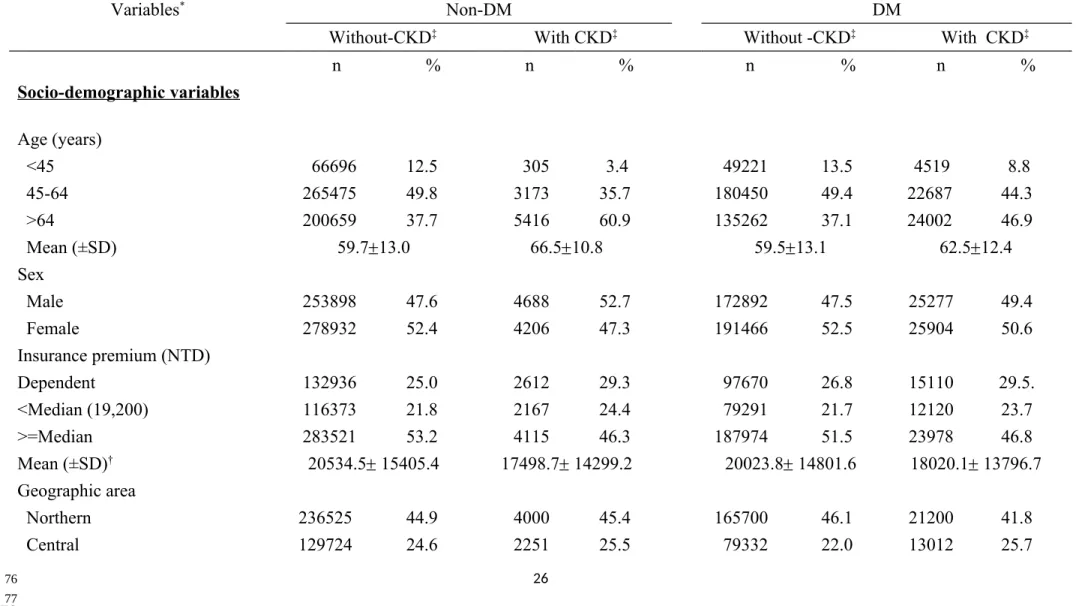
In total, 416,143 diabetic (51,208 with CKD) and 541,724 non-diabetic (8,894 with CKD) patients were included in the study (Figure 1). The patients in the non-
DM/CKD group were the oldest (66.510.8 years), followed by those in the DM/CKD group (62.512.4 years). The mean age of the patients in the non-DM/non-CKD and
DM/non-CKD groups was similar (59.713.0 and 59.513.1 years, respectively).
With the exception of the non-DM/CKD patients, the patients in the other three groups were mostly female. In addition, the distributions of insurance premium, geographic area, and urbanization were similar in the study groups. The patients in the DM/CKD group had the highest proportions of the selected co-morbidities, while the lowest proportion was seen in the non-DM/non-CKD group (Table 1). The median follow up period were 6.6, 7.7, 8.0 and 8.0 years in the DM/CKD, DM/non-CKD,
non-DM/CKD and non-DM/non-CKD groups, respectively.
Age- and sex-specific incidence rates and adjusted hazard ratios of acute coronary
syndrome in the four study groups
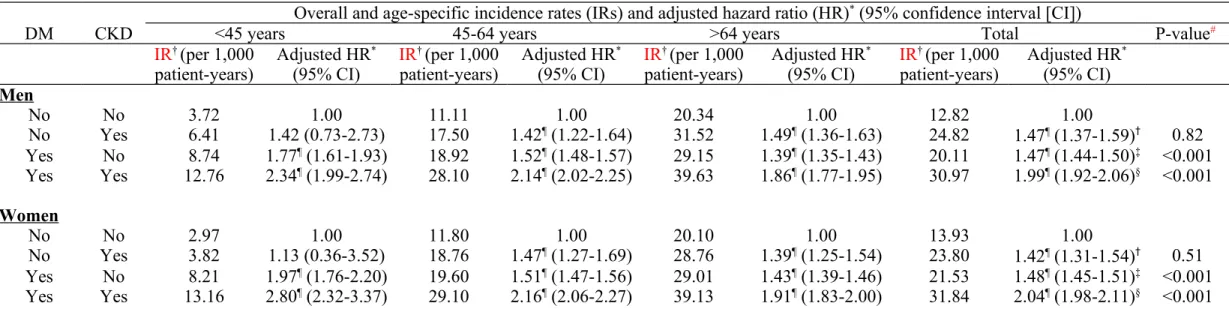
Table 2 and Supplementary Table 1 show the overall, age- and sex-specific IRs and adjusted hazard ratios (AHRs) of ACS. The IRs for ACS increased with
increasing age in all study groups. The non-DM/non-CKD group had the lowest ACS event rates for men (12.82 per 1000 patient-years) and women (13.93 per 1000 203
204 205 206 207 208 209 210 211 212 213 214 215
216 217
218 219 220 221 222
patient-years) in the whole age-groups, whether the DM/CKD group had the highest
overall ACS event rates of 30.97 and 31.84 per 1000 patient-years in men and
women, respectively. In addition, the overall sex-specific IR was slightly higher in the non-DM/CKD group compared to the DM/non-CKD group (24.82 vs. 20.11 per 1000 patient-years in men; 23.80 vs. 21.53 per 1000 patient-years in women). Similar IRs were found in both the non-DM/CKD and DM/non-CKD groups across all age stratifications, except in females aged < 45 years, in which the DM/non-CKD group
had a higher IR than the non-DM/CKD group (8.21 vs. 3.82 per 1000 person-years).
In male subjects, diabetes alone conferred a similar risks for ACS as CKD alone, with an AHR of 1.47 [95% CI:1.37-1.59], when compared to the non-DM/non-CKD group (Table 2). The AHR increased to 1.99 [95% CI:1.92-2.06] in male patients with DM/CKD. Similar magnitudes and patterns of AHRs were observed in the female subjects. Age-specific analysis showed that the increased risks of ACS in the non- DM/CKD patients were similar across all age stratifications in both men and women, whereas age showed a significant modification effect on the risk of ACS in both
DM/non-CKD and DM/CKD groups. The AHR associated with DM/non-CKD patients decreased gradually from 1.77, 1.52, to 1.39 for male subjects aged <45, 45- 64, and >64 years, respectively (p < 0.001). The corresponding AHRs for male patients with DM/CKD also diminished from 2.34, 2.14 to 1.86 (p < 0.001). In
13
223 224 225 226 227 228 229
230 231 232 233 234 235 236 237 238 239 240 241
37 38
contrast, the AHRs remained constant in the male subjects in the non-DM/CKD group aged < 45 years, 45-64 years, and > 64 years (1.42, 1.42 and 1.49, respectively; p = 0.82). Similar results were noted for the female subjects. Moreover, the magnitude of the increase in hazard ratios for ACS among the patients in the DM/CKD group was nearly equal to the direct multiplication product of the AHRs of DM and CKD, which indicated the multiplicatively independent effect of DM and CKD on the risk for ACS. For example, in the male subjects aged 45-64 year, the AHR of the DM/CKD group (2.14) was nearly the same as the direct product of AHRs of the non-DM/CKD
and DM/non-CKD groups (2.16).
Adjusted hazard ratios for ACS in relation to diabetes and CKD alone with other
selected risk factors
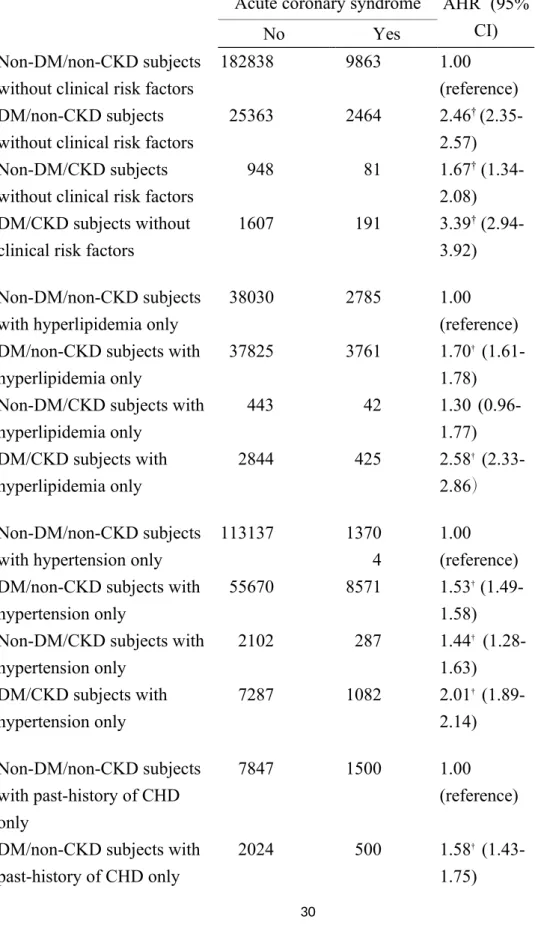
Table 3 shows the relative hazards of ACS in relation to diabetes and CKD
according to the presence of various cardiovascular (CV) risk profiles. After adjusting for baseline characteristics, the DM/CKD group still had the highest risk of ACS across various risk factors stratifications. In subjects without any selected risk factor, diabetes increased the risk of ACS by a magnitude of 146% (AHR: 2.46 [95%
CI:2.35-2.57]), while CKD only conferred an increased risk of 67% (AHR:1.67 [95%
CI:1.34-2.08]). In contrast, in subjects with all three selected risk factors, CKD conferred a higher risk of ACS than diabetes (AHR:1.43 [95% CI:1.27-1.60] vs. 1.25 242
243 244 245 246 247 248 249
250 251
252 253 254 255 256 257 258 259 260
[95% CI:1.22-1.29], respectively). The effect of diabetes on the risk of ACS was higher than CKD in the subjects with ≤ 2 selected CV risk factors, except in the hyperlipidemia+hypertension subgroup. Therefore, there was a tendency for the discrepancy in AHR between the DM/non-CKD and non-DM/CKD groups to be diminished as the number of risk factors increased. Furthermore, the multiplicative independent effect of diabetes and CKD on the risk for ACS was also observed in different risk factor-stratification subgroups.
15
261 262 263 264 265 266 267
43 44
Discussion:
In this population-based cohort study, diabetes and CKD were both found to be associated with a higher risk of ACS. However, the magnitude of association varied across different age-, sex- and risk factor-stratifications. In general, diabetes had a greater negative effects than CKD in the younger patients (< 45 years) and in the patients without or with a small number of CV risk factors. On the other hand, CKD conferred a similar risk of ACS to that of diabetes in the older patients, especially in
those aged > 64 years of age, or with more selected CV risk factors. Moreover, we also noted that diabetes and CKD multiplicatively contributed to the risk of ACS regardless of age, gender, and cardiovascular risk factors, which is similar to findings
reported in patients with diabetes and end-stage renal disease (ESRD)28. Our results revealed that age may modify the risk of ACS in diabetic patients regardless of CKD status, which is consistent with previous studies29,33. Younger diabetic patients have been reported found to be at a higher risk of CV diseases than
older diabetic patients, mainly due to poor glycemic control, adverse health-related behaviors, and irregular assessment of diabetes-related complications in younger diabetic patients33. On the other hand, our study showed no significant modification effect by age for the relationship between CKD and ACS (p=0.820 and 0.511, in men and women, respectively). Since we adjusted for several major traditional CV risk 268
269 270 271 272 273 274 275 276 277
278 279 280 281 282 283 284 285 286
factors, a possible explanation is that non-traditional CV risk factors, such as mineral metabolism dysregulation and inflammation, can enhance vascular calcification and arterial stiffness, which therefore accelerates the process of vascular aging in patients with CKD34. Premature arterial aging can further contribute to the excess burden of ischemic heart disease in CKD patients, in concert with numerous other risk factors, including endothelial dysfunction, oxidative stress, accelerated thrombosis and malnutrition34. In addition, even intensive modification of both traditional and non- traditional CV risk factors has been reported to be unable to reduce the incidence of ACS in CKD patients35. Thus, the presence of CKD may superpose a constant excess hazard with regard to the risk of ACS beyond an age effect, which might partly explain the mechanism related to the constant effect of CKD in the different age groups (Table 2). Evidence supporting the concept of acceleration of premature
vascular aging in CKD patients was also revealed in the current study. The incidence rates of ACS in the CKD patients aged between 45-64 years were similar to those of the non-CKD patients older than 64 years in both the diabetes and non-diabetes
groups (Table 2), and this phenomenon was more prominent in the patients with diabetes. Large prospective clinical trials are needed to explore strategies to lower the risk of ACS in CKD patients.
Compared with the patients without DM and CKD, both diabetes and CKD were
17
287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303
304 305
49 50
found to enhance the risk of ACS. However, different weights of the relative hazard of diabetes and CKD were found in various CV risk factor stratifications. Diabetes conferred a higher risk of ACS than CKD in the patients without any selected risk
factors. As the number of risk factors increased, the effect of CKD approached that of diabetes and was even higher if all selected risk factors were present. The CKD patients were prone to have more selected risk factors if they were in the advanced stages of CKD, and it is biologically plausible that more non-traditional risk factors emerge as CKD stages progresses. This suggested an enhanced effect of non-
traditional risk factors on the future risk of ACS in patients with advanced stage CKD.
Previous studies have suggested that estimating the risk of future CV events using traditional CV risk factors only (via Framingham risk equation) is inadequate for patients with diabetes and CKD population36,37. Therefore, the different relative hazards related to diabetes and CKD in the various selected risk factor stratifications may highlight the distinct effect of non-traditional risk factors for ACS in these two
populations. Preventing and controlling both traditional and non-traditional CV risk factors simultaneously may be essential to control the heavy burden of CV events
burden in patients with diabetes and CKD populations.
Only a few studies revealed the effect of CKD on the risk of ACS in patients under the age of 45. The findings of this study suggest that younger (< 45 years) 306
307 308 309 310 311 312 313 314 315 316 317 318 319 320 321
322 323 324
female patients with CKD tended to have the lowest risk of ACS (AHR:1.13 [95%
CI:0.36-3.52]). The biological mechanism may be a result of the fact that estrogen can ameliorate the negative impact induced by CKD. In one study comparing the effect of
estrogen use and its relationship to renal function38, the use of estrogen was found to better preserve renal function than in those not receiving estrogen in cross-sectional analysis, however these results were not found in prospective analysis. The interaction between estrogen and various CV risk factors in patients with CKD population still
needs to be clarified in further studies.
In our previous study, diabetes and ESRD were demonstrated to contribute to the risk of acute myocardial infarction in a nearly multiplicative effect28. We speculated that different penetrations of disease-specific CV risk factors among diabetes and ESRD patients might explain this phenomenon. Similar findings related to the effect of diabetes and non-dialysis CKD on the risk of ACS in this study further extended our previous hypothesis to non-dialysis CKD patients. The magnitude of the increased risk for ACS in the patients with both diabetes and CKD also nearly reached the value
of the direct multiplicative product of those with either diabetes or CKD alone.
Because patients with ESRD were excluded before enrollment and the CKD patients were censored when they developed ESRD, the effect of CKD on ACS could not be explained by the presence of ESRD.
19
325 326 327 328 329 330 331
332 333 334 335 336 337 338 339 340 341 342 343
55 56
Several previous studies compared the effect of CKD and diabetes on the risk of CV events, and concluded that CKD conferred a similar CV risk as diabetes in different
study populations14,15,17,18. However, our study results showed that this effect was not constant across various age-, sex- and risk factor-stratifications. Thus, it may not be appropriate to treat CKD in the same manner as diabetes in all patients. The graded differences in the risk of ACS in the DM and CKD patients with different ages and CV risk factors suggest that individualized management of ACS is warranted in different target populations in order to optimize the utilization of medical resources and avoid possible treatment-related side effects. For example, women with CKD who are less than 45 years old or CKD patients without any selected CV risk factors may not need as intensive management as diabetic patients. Different therapeutic goals, such as the control of hypertension or lipid profiles and the use of antiplatelet agents for primary prevention, should be considered according to the presence of diabetes, CKD, CV risk factors and age. Intensive screening strategies and therapies may therefore be reserved for patients who value the potential benefits of the management
to a greater extent than the potential harm, especially in CKD patients at a low risk of ACS because clinical evidence involving the effects of these treatments is still
limited39,40.
This study has several strengths. First, the NHIRD covers most of the residents in 344
345 346 347 348 349 350 351 352 353 354 355 356 357 358 359 360 361 362
Taiwan and contains data on most of the medical services that beneficiaries receive.
Such a sizable study population in a real-world setting can avoid most of the selection and recall bias or missing information related to medical conditions which can arise in referral subjects, volunteers or clinical trial populations. Thus, the results of our study are probably more generalizable. Second, this large and diverse database provides sufficient power by which to investigate the effects of DM and CKD on the incidence of ACS, especially with regards to age, sex and various CV risk factors. This allowed us to clarify the separate and joint effects of DM and CKD according to various
clinical conditions.
There are several limitations to this study. First, the exclusive reliance on the
claims data may have resulted in disease misclassification. However, we used at least two visits for diabetes or CKD-related diagnoses that were >30 days apart to reduce the likelihood of misclassification20,29. In our non-DM population, 1.64% of the patients were found to have CKD after excluding subjects with cancer and ACS
before the start of follow-up. This is generally consistent with the proportion of patients having CKD (2.1%), including patients with cancer identified from a non-
diabetic Medicare population using a method similar to that reported by Foley et al41. Second, some individuals in the non-DM/CKD and non-DM/non-CKD groups may have developed diabetes during the follow-up period. However, the overall 5-year
21
363 364 365 366 367 368 369 370
371 372 373 374 375 376 377 378 379 380 381
61 62
incidence of diabetes is 197.0 per 100,000 population in Taiwan42. The contribution of newly diagnosed diabetes to the non-DM/CKD group were therefore to be considered low. In addition, the misclassification in the non-DM/non-CKD (control) group is likely to be non-differential, which would tend to underestimate the true relative hazard. Third, due to limited information available from the claims data, not all traditional and non-traditional CV risk factors or confounders were adjusted for, such as smoking, body mass index, proteinuria amount and the concurrent use of
medications. Furthermore, a lack of the records for the estimated glomerular filtration rate made it impossible to provide detailed CKD stage information in our study population. Since the prevalence of hypertension is around 56.6~77.6% in CKD stage III-V patients in Taiwan1, which is consistent with the results found in our non-
DM/CKD group, we speculate that most of our CKD patients were likely to have CKD stage III-V. Fourth, since dialysis per se has different impacts on ACS, we did not extend the follow-up period after the initiation of dialysis in our CKD patients.
However, this is likely to have underestimated the risk of ACS in our non-dialysis- dependent CKD population because dialysis patients have a higher risk of ACS than
non-dialysis-dependent CKD patients.
In summary, we found that diabetes conferred a higher risk of ACS than CKD in younger patients (< 45 years) and in those with fewer CV risk factors, and that the 382
383 384 385 386 387 388 389 390 391 392 393 394 395 396 397
398 399 400
difference in the risk was minimized in older patients ( ≥ 45 years) and in those with more CV risk factors. In addition, age was found to modify the risk of ACS in patients with diabetes, but not in those with CKD alone. Furthermore, the presence of both diabetes and CKD further enhance the risk of ACS in a multiplicatively independent effect. Management for the primary prevention of ACS in patients with diabetes/CKD should be individualized by taking into account age, sex and CV risk factors.
23
401 402 403 404 405 406 407
67 68
Acknowledgments:
The authors would like to extend grateful thanks to the National Health Research Institutes for kindly providing the data for analysis. The interpretation and conclusions in the current study do not represent those of the National Health Research Institutes.
Conflicts of interest: The authors have no conflicts of interest to disclose.
Funding/Support:
Our research was partly supported by grants NCKUH-10105009 and NCKUH- 10205003 from National Cheng-Kung University Hospital, Tainan, Taiwan, ROC.
None of the funding sources had any role in the study design, analysis and interpretation of the data, the preparation, review, or approval of the manuscript.
408 409 410 411 412 413 414 415
416 417 418 419 420
References:
25
421 422 423
73 74
Table 1. The baseline clinical characteristics of the study subjects
Variables* Non-DM DM
Without-CKD‡ With CKD‡ Without -CKD‡ With CKD‡
n % n % n % n %
Socio-demographic variables Age (years)
<45 66696 12.5 305 3.4 49221 13.5 4519 8.8
45-64 265475 49.8 3173 35.7 180450 49.4 22687 44.3
>64 200659 37.7 5416 60.9 135262 37.1 24002 46.9
Mean (±SD) 59.713.0 66.510.8 59.513.1 62.512.4
Sex
Male 253898 47.6 4688 52.7 172892 47.5 25277 49.4
Female 278932 52.4 4206 47.3 191466 52.5 25904 50.6
Insurance premium (NTD)
Dependent 132936 25.0 2612 29.3 97670 26.8 15110 29.5.
<Median (19,200) 116373 21.8 2167 24.4 79291 21.7 12120 23.7
>=Median 283521 53.2 4115 46.3 187974 51.5 23978 46.8
Mean (±SD)† 20534.5 15405.4 17498.7 14299.2 20023.8 14801.6 18020.1 13796.7
Geographic area
Northern 236525 44.9 4000 45.4 165700 46.1 21200 41.8
Central 129724 24.6 2251 25.5 79332 22.0 13012 25.7
424
Southern 144719 27.5 2348 26.7 103769 28.8 15065 29.7
Eastern 15720 3.0 211 2.4 11238 3.1 1402 2.8
Urbanization status
Metropolis 212652 40.3 3546 40.2 152391 42.2 21591 42.6
Satellite city/town 141783 26.8 2356 26.7 95388 26.4 12807 25.2
Rural area 173901 32.9 2924 33.1 113087 31.3 16339 32.2
Comorbidities§ Hypertension
No 248255 46.6 1739 19.5 77731 21.3 5909 11.5
Yes 284575 53.4 7155 80.5 287204 78.7 45299 88.5
Hyperlipidemia
No 364265 68.4 4528 50.9 116596 32.0 14076 27.5
Yes 168565 31.6 4366 49.1 248339 68.0 37132 72.5
Coronary heart diseases
No 445966 83.7 6301 70.8 274002 75.1 34381 67.1
Yes 86864 16.3 2593 29.2 90933 24.9 16827 32.9
Total 532830 100.0 8894 100.0 364935 100.0 51208 100.0
Abbreviations: CKD = chronic kidney disease; DM = diabetes mellitus; NTD = New Taiwan dollars; SD = standard deviation.
* Inconsistency between the total population and the population summed for individual variable was due to missing information.
27
425 426
79 80
†Dependent insurers were not included.
‡ CKD ICD-9-CM codes: 016.0, 095.4, 189.0, 189.9, 223.0, 236.91, 250.4, 271.4, 274.1, 283.11, 403.×1, 404.×2, 404.×3, 440.1, 442.1, 447.3, 572.4, 580-588, 591, 642.1, 646.2, 753.12-753.17, 753.19, 753.2, and 794.4.
§Hypertension (ICD-9:401–402, 405, A260), Hyperlipidemia (ICD-9: 272.0–272.4, A182), Coronary heart diseases (ICD-9: 414.8 and 414.9).
427 428 429 430 431 432
Table 2. Overall and age- and sex-specific incidence rates (IRs) and relative hazards of acute coronary syndrome in relation to diabetes and CKD
Overall and age-specific incidence rates (IRs) and adjusted hazard ratio (HR)* (95% confidence interval [CI])
DM CKD <45 years 45-64 years >64 years Total P-value#
IR† (per 1,000
patient-years) Adjusted HR*
(95% CI) IR† (per 1,000
patient-years) Adjusted HR*
(95% CI) IR† (per 1,000
patient-years) Adjusted HR*
(95% CI) IR† (per 1,000
patient-years) Adjusted HR* (95% CI) Men
No No 3.72 1.00 11.11 1.00 20.34 1.00 12.82 1.00
No Yes 6.41 1.42 (0.73-2.73) 17.50 1.42¶ (1.22-1.64) 31.52 1.49¶ (1.36-1.63) 24.82 1.47¶ (1.37-1.59)† 0.82 Yes No 8.74 1.77¶ (1.61-1.93) 18.92 1.52¶ (1.48-1.57) 29.15 1.39¶ (1.35-1.43) 20.11 1.47¶ (1.44-1.50)‡ <0.001 Yes Yes 12.76 2.34¶ (1.99-2.74) 28.10 2.14¶ (2.02-2.25) 39.63 1.86¶ (1.77-1.95) 30.97 1.99¶ (1.92-2.06)§ <0.001 Women
No No 2.97 1.00 11.80 1.00 20.10 1.00 13.93 1.00
No Yes 3.82 1.13 (0.36-3.52) 18.76 1.47¶ (1.27-1.69) 28.76 1.39¶ (1.25-1.54) 23.80 1.42¶ (1.31-1.54)† 0.51 Yes No 8.21 1.97¶ (1.76-2.20) 19.60 1.51¶ (1.47-1.56) 29.01 1.43¶ (1.39-1.46) 21.53 1.48¶ (1.45-1.51)‡ <0.001 Yes Yes 13.16 2.80¶ (2.32-3.37) 29.10 2.16¶ (2.06-2.27) 39.13 1.91¶ (1.83-2.00) 31.84 2.04¶ (1.98-2.11)§ <0.001
Abbreviations: CKD = chronic kidney disease; CI = confidence interval; DM = diabetes mellitus; HR = hazard ratio; IR = incidence rate.
* Based on Cox proportional hazard regression with adjustment for age, sex, insurance premium, geographic area, urbanization status, hypertension, hyperlipidemia, and coronary heart diseases
†P-value for effect-modification by sex=0.47.
‡P-value for effect-modification by sex=0.93.
§P-value for effect-modification by sex=0.65.
¶ P<0.05.
# P-value for effect-modification by age.
29
433
434 435 436 437 438 439 440 441
85 86
Table 3. Selected clinical risk factor(s)-specific relative hazards of acute coronary syndrome in relation to diabetes (DM) and chronic kidney disease (CKD)
Acute coronary syndrome AHR* (95%
No Yes CI)
Non-DM/non-CKD subjects without clinical risk factors
182838 9863 1.00
(reference) DM/non-CKD subjects
without clinical risk factors
25363 2464 2.46†(2.35-
2.57) Non-DM/CKD subjects
without clinical risk factors
948 81 1.67† (1.34-
2.08) DM/CKD subjects without
clinical risk factors
1607 191 3.39† (2.94-
3.92) Non-DM/non-CKD subjects
with hyperlipidemia only
38030 2785 1.00
(reference) DM/non-CKD subjects with
hyperlipidemia only
37825 3761 1.70† (1.61- 1.78) Non-DM/CKD subjects with
hyperlipidemia only
443 42 1.30 (0.96-
1.77) DM/CKD subjects with
hyperlipidemia only
2844 425 2.58† (2.33- 2.86)
Non-DM/non-CKD subjects with hypertension only
113137 1370
4
1.00 (reference) DM/non-CKD subjects with
hypertension only
55670 8571 1.53† (1.49-
1.58) Non-DM/CKD subjects with
hypertension only
2102 287 1.44† (1.28-
1.63) DM/CKD subjects with
hypertension only
7287 1082 2.01† (1.89- 2.14) Non-DM/non-CKD subjects
with past-history of CHD only
7847 1500 1.00
(reference) DM/non-CKD subjects with
past-history of CHD only
2024 500 1.58† (1.43- 1.75) 442
443 444 445
Non-DM/CKD subjects with past-history of CHD only
105 23 1.39 (0.91-
2.12) DM/CKD subjects with past-
history of CHD only
201 42 1.61† (1.19-
2.19) Non-DM/non-CKD subjects
with
hyperlipidemia+hypertension
76537 9072 1.00
(reference) DM/non-CKD subjects with
hyperlipidemia+hypertension
123600 1674
8
1.31† (1.28- 1.35) Non-DM/CKD subjects with
hyperlipidemia+hypertension
2087 311 1.34† (1.20- 1.51) DM/CKD subjects with
hyperlipidemia+hypertension
17788 3157 1.99† (1.91- 2.07) Non-DM/non-CKD subjects
with past-history CHD+hyperlipidemia
4547 845 1.00
(reference) DM/non-CKD subjects with
past-history
CHD+hyperlipidemia
4716 1078 1.42† (1.30- 1.56) Non-DM/CKD subjects with
past-history
CHD+hyperlipidemia
79 18 1.22 (0.76-
1.94) DM/CKD subjects with past-
history CHD+hyperlipidemia
484 115 1.53† (1.25-
1.86) Non-DM/non-CKD subjects
with past-history CHD+hypertension
28696 6680 1.00
(reference) DM/non-CKD subjects with
past-history
CHD+hypertension
17426 4578 1.32† (1.27- 1.37) Non-DM/CKD subjects with
past-history
CHD+hypertension
785 197 1.31† (1.14-
1.51) DM/CKD subjects with past-
history CHD+hypertension
2889 777 1.76† (1.63- 1.90)
31
91 92
Non-DM/non-CKD subjects with past-history of CHD, hyperlipidemia and hypertension
30406 6343 1.00
(reference)
DM/non-CKD subjects with past-history of CHD,
hyperlipidemia and hypertension
49044 1156
7
1.25† (1.22- 1.29)
Non-DM/CKD subjects with past-history of CHD,
hyperlipidemia and hypertension
1079 307 1.43† (1.27- 1.60)
DM/CKD subjects with past- history of CHD,
hyperlipidemia and hypertension
9553 2766 1.76† (1.69- 1.85)
Abbreviations: AHR = adjusted hazard ratio; CHD = coronary heart disease; CKD = chronic kidney disease; DM = diabetes mellitus.
* Based on Cox proportional hazard regression with adjustment for age, sex, insurance premium, geographic area, and urbanization status.
† P<0.05 446
447 448 449 450
Supplementary Table 1. Numbers of overall age- and sex-specific events of acute coronary syndrome* in the four study groups
Variabl es
Non-DM DM
Non-CKD CKD Non-CKD CKD
Number of events
Number of events
Number of events
Number of events Men
<45 years
1078 9 1773 212
45-64 years
10329 184 10790 1730
>64 years
11450 483 9627 2193
Total 22857 676 22190 4135
Women <45 years
641 3 1249 168
45-64 years
12348 194 12985 1975
>64 years
14946 393 12830 2275
Total 27935 590 27064 4418
Overall 50792 1266 49267 8555
Abbreviations: CKD = chronic kidney disease; DM = diabetes mellitus.
*Including acute myocardial infarction (410.x), unstable angina (413.9), and intermediate syndrome (411.1).
33
451 452 453
454 455 456
97 98
457