Risk of pneumonia among patients with chronic kidney disease in outpatient and inpatient: a nationwide population-based study
Che-Yi Chou
1,2, Shu-Ming Wang
1,2, Chih-Chia Liang
1,2, Chiz-Tzung Chang
1,2, Jiung- Hsiun Liu
1,2, I-Kuan Wang
1,2, Lien-Cheng Hsiao
2,3, Chih-Hsin Muo
4,5, Chiu-Ching
Huang
1,2, Chi-Jung Chung
6,71
Division of Nephrology and Kidney Institute, Department of Internal Medicine,
China Medical University Hospital, Taichung 40447, Taiwan
2
College of Medicine, China Medical University, Taichung 40402, Taiwan
3
Division of Cardiology, Department of Internal Medicine, China Medical University
Hospital, Taichung, Taiwan
4
Department of Public Health, China Medical University and Hospital, 91 Hsueh-Shih
Road, Taichung 404, Taiwan
5
Management Office for Health Data, China Medical University and Hospital, 91
Hsueh-Shih Road, Taichung 404, Taiwan
6
Department of Health Risk Management, College of Public Health, China Medical
University, Taichung, Taiwan
7
Department of Medical Research, China Medical University Hospital, Taichung, Taiwan
Address correspondence to Chi-Jung Chung, PhD,
Department of Health Risk Management, College of Public Health, China Medical
University, No. 91 Hsueh Shih Road, Taichung City 404, Taiwan
E-mail: [email protected] Tel: 886-4-22053366-6505
Fax: 886-4-2207-0429
Abstract
Chronic kidney disease (CKD) patients are more at risk for pneumonia than the general population. Patients with pneumonia were usually treated in outpatients, but previous studies were conducted based on inpatient pneumonia. This may under- estimate the risk of pneumonia in patients with CKD. We investigated the pneumonia
risk in both outpatient and inpatient settings in CKD patients.
Method
A total of 15562 CKD patients and 62109 non-CKD individuals (matched for age and gender) in the Longitudinal Health Insurance Database of Taiwan National Insurance from 1996 to 2010 were analyzed. Incidence density rates of inpatient and outpatient pneumonia were calculated. Risk factors associated with pneumonia were analyzed
using Cox proportional hazards models with adjustments for confounders.
Results
The incidence density rate of pneumonia was 65.6 per 1000 person-years in CKD
patients and 28.4 per 1000 person-year in non-CKD individuals. The incidence
density rate of inpatient pneumonia was 43.3 per 1000 person-years in CKD patients
and 16.6 in non-CKD individuals. CKD was associated with increased risk for
pneumonia [adjusted hazard ratio (aHR): 1.97, 95% CI (confidence interval): 1.89-
2.05, p<0.001], outpatient pneumonia (aHR: 1.40, 95 % CI: 1.31-1.49), and inpatient
pneumonia (aHR: 2.17, 95% CI: 2.07-2.29, p<0.001). Patients’ comorbidity including
diabetes, cardiovascular disease, asthma, and chronic obstructive pulmonary disease
were independently associated with increased risk of pneumonia.
Conclusion
Chronic kidney disease is associated with increased risk of both outpatient and
inpatient pneumonia. This association is independent of comorbid diabetes,
cardiovascular disease, asthma and chronic obstructive pulmonary disease.
Introduction
Pneumonia is one of the most common infectious morbidity in chronic kidney disease (CKD) patients. Pneumonia in CKD patients is associated with increased hospitalization, cardiovascular event and mortality . Pneumonia related mortality rate of CKD patients is 14 to 16 fold higher than that of general population
4. The risk of inpatient pneumonia and mortality within 30 days is increased with the decline of renal function in CKD patients
5. However, all the previous studies were based on the incidence of inpatient pneumonia. This may underestimate the risk of pneumonia because most treatment for pneumonia was provided in outpatient settings. The aim of the study is to determine the incidence of both inpatient and outpatient pneumonia in
CKD patients using the National Health Insurance (NHI) data from Taiwan.
Material and Methods
This is as a retrospective cohort study using an encrypted database from the Bureau of
National Health Insurance (BNHI). The Institutional Review Board of China Medical
waved the need for informed consent. The Longitudinal Health Insurance Database
(LHID) of the Taiwan National Health Research Institute (NHRI) was released by the
BNHI. The LHID included all medical records from 1996 to 2010, from which one
million people were randomly selected. There were no significant differences in the
sex and age distributions between LHID and all individuals in the NHRI. The
International Classification of Disease Revision 9th Clinical Modification (ICD-9- CM) was used for the diagnosis codes. A 1:4 study design was used as the increase of
controls did not increase statistical efficiency
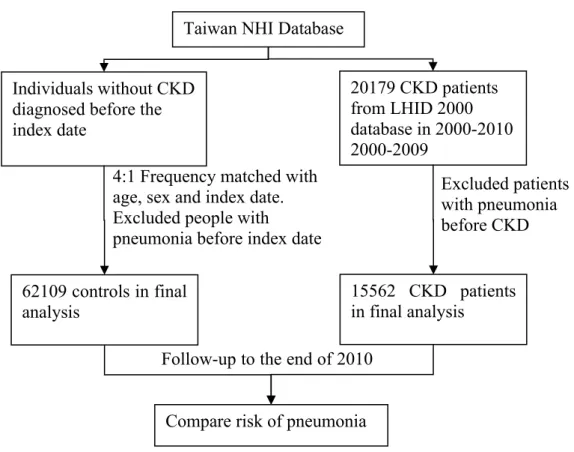
6. Study sample
CKD patients was defined as patients with a ICD-9-CM codes 585 from LHID who is not in catastrophic illness patients database that include patients with CKD stage 3 to 5 without renal replacement therapy (Figure 1)
7. A total of 15562 CKD patients and 62109 non-CKD patients (matched for age and sex) were included. Pneumonia was identified using ICD-9-CM codes 481, 482, 485 and 486 and pneumonia related hospitalization was also recorded. For patients who developed more than one episode of pneumonia, the first episode of pneumonia was recorded. As we focused on primary pneumonia risk, patients with pneumonia before the diagnosis of CKD were excluded. Time was calculated from the index date of CKD to the date of pneumonia.
Co-morbidities including diabetes (ICD-9-CM codes 250), hypertension (401-405), cardiovascular disease (CVD) (410-414), asthma (493) and chronic obstructive pulmonary disease (COPD) (491, 492, 494, 496) are defined as more than three
medical visits.
Statistical analysis
Distribution of sex, age, and co-morbidities for CKD patients and control individuals
were analyzed using chi-square test for categorical variables or t-test for continuous
variables. The incidence density was defined as the number of pneumonia cases divided by the total follow-up person-years (expressed as per 1000 person-years). The adjusted hazard ratio (aHR) and the 95 % confidence intervals (CIs) of pneumonia risk factors were analyzed using Cox proportional-hazards regression with adjustment for sex, age, hypertension, diabetes, cardiovascular disease (CVD), asthma, and COPD. The statistical significance level was set at a two-tailed probability value of <
0.05. All analyses was performed using the SAS software version 9.1 (SAS Institute,
Cary, NC, USA).
Results
The incidence density rate of pneumonia was 65.6 in CKD patients and 28.4 per 1000
person-years in non-CKD patients (Table 1). The incidence density rate was used
because the follow-up of non-CKD patients was longer. The incidence density rate of
inpatient pneumonia was 43.3 per 1000 person-years in CKD patients and 16.6 per
1000 person-years in non-CKD patients. CKD patients had a higher rate of diabetes
(p<0.001), hypertension (p<0.001), CVD (p<0.001), asthma (p<0.001) and COPD
(p<0.001) than non-CKD patients did. Compared to patients without pneumonia,
patients who developed pneumonia were older and they were more likely to have
CKD, diabetes, hypertension, and CVD, asthma and COPD (Table 2). Of 5536
patients with outpatient pneumonia, 1375 (24.8%) of them had CKD. Of 7240
patients with inpatient pneumonia, 2661 (36.8%) of them had CKD. The patients with inpatients pneumonia were older than the patients with outpatient pneumonia.
Compared to patients with outpatient pneumonia, patients with inpatients pneumonia were more likely to have diabetes, hypertension and CVD. The percentage of patients with asthma was lower in inpatients patients compared to the patients with outpatient pneumonia. The prevalence of patients with COPD was not different between the
patients with inpatient pneumonia and those with outpatient pneumonia.
CKD, patients’ age, male gender, hypertension, diabetes, CVD, asthma, and COPD were associated with increased risk of pneumonia (Table 3). The aHR of CKD for any type of pneumonia was 1.97 (95% CI: 1.89-2.05, p < 0.001), 1.40 (95% CI: 1.31-1.49) for outpatient pneumonia, and 2.17 (95% CI: 2.07-2.29) for inpatient pneumonia.
Male gender (aHR 1.13, 95% CI: 1.07-1.19), comorbid diabetes (aHR 1.12, 95 % CI:
1.05-1.19), comorbid CVA (aHR 1.11, 95% CI: 1.04-1.20), comorbid asthma (aHR 1.66, 95% CI: 1.56-1.79), and comorbid COPD (aHR 1.89, 95% CI: 1.77-2.02) was independently associated with increased outpatients pneumonia risk. The comorbid hypertension was not associated with increased outpatients pneumonia risk, but was
associated with increased inpatient pneumonia risk (aHR 1.10, 95 % CI: 1.04-1.16).
Discussions
Chronic kidney disease is associated with increased both outpatient and inpatient
pneumonia. Compared to non-CKD patients, the risk of all pneumonia in CKD patients was 1.97-fold higher, 1.4 fold higher for outpatient pneumonia, and 2.17 fold higher for inpatient pneumonia. CKD patients not only had increased risk of pneumonia but also increased severity of pneumonia (indicated by hospitalization) than non-CKD patients. The incidence of pneumonia in this study was higher than the incidence of pneumonia reported in the previous studies because outpatient pneumonia was taken into consideration in this study. The increased infection risk in CKD patients can be explained by uremia related impairment in monocyte
12, neutrophil phagocytosis
13, T-lymphocytes
14, B-lymphocytes
15and increased cytokines
16. The increased risk of inpatient pneumonia in CKD patients may be related to the comorbidity of patients with CKD because comorbidities were
associated with severity of pneumonia .
The percentage of inpatient pneumonia was 58.6% in non-CKD patients who developed pneumonia and 65.9% in CKD patients who developed pneumonia. The high hospitalization rate of pneumonia can be explained by two reasons. First, the hospitalization costs in Taiwan are low. Second, most of the hospitalization cost was covered by the health insurance and the patients only need to pay 10% of the cost.
The high rate of diabetes, hypertension, CVD , asthma and COPD in CKD patients
was consistent to the findings of the previous studies .
There were some limitations of this study. First, the ICD-9-CM code 585.1-585.5 for CKD 1-5 was not used and the incidence of CKD can be under-estimated using ICD- 9-CM code 585 (patients with CKD 1 and patients with CKD 2 were not included).
Second, variables of pneumonia severity index such as mental status, vital signs and laboratory data were not available in the LHID. Third, the pneumonia pathogen that was associated with the severity of pneumonia
23was not recorded in the LHID. We were not able to determine if any specific pathogen was related to the pneumonia in
CKD patients.
In conclusion, chronic kidney disease patients have increased risk for inpatient and outpatient pneumonia, especially pneumonia that required hospitalization. The
increased risk of pneumonia in CKD patients is independent of their comorbidity.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Guo H, Liu J, Collins AJ, Foley RN: Pneumonia in incident dialysis patients--the United States Renal Data System. Nephrol Dial Transplant, 23: 680-686, 2008
2. Viasus D, Garcia-Vidal C, Cruzado JM, Adamuz J, Verdaguer R, Manresa F, Dorca J, Gudiol F, Carratala J: Epidemiology, clinical features and outcomes of pneumonia in patients with chronic kidney disease. Nephrol Dial Transplant, 26: 2899-2906, 2011
3. Collins AJ, Foley RN, Gilbertson DT, Chen SC: The state of chronic kidney disease, ESRD, and morbidity and mortality in the first year of dialysis. Clin J Am Soc Nephrol, 4 Suppl 1: S5-11, 2009
4. Sarnak MJ, Jaber BL: Pulmonary infectious mortality among patients with end- stage renal disease. Chest, 120: 1883-1887, 2001
5. James MT, Quan H, Tonelli M, Manns BJ, Faris P, Laupland KB, Hemmelgarn BR: CKD and risk of hospitalization and death with pneumonia. Am J Kidney Dis, 54: 24-32, 2009
6. Chung CJ, Huang CY, Tsai HB, Muo CH, Chung MC, Chang CH, Huang CC: Sex Differences in the Development of Malignancies among End-Stage Renal Disease Patients: A Nationwide Population-Based Follow-Up Study in Taiwan. PLoS One, 7: e44675, 2012
7. Liu JH, Lin SY, Hsu CY, Lin HH, Liang CC, Sung FC, Huang CC: The risk for chronic kidney disease in patients with heart diseases: a 7-year follow-up in a cohort study in Taiwan. BMC Nephrol, 13: 77, 2012
8. Agarwal R, Bunaye Z, Bekele DM, Light RP: Competing risk factor analysis of end-stage renal disease and mortality in chronic kidney disease. Am J Nephrol, 28: 569-575, 2008
9. Hwang SJ, Lin MY, Chen HC, Hwang SC, Yang WC, Hsu CC, Chiu HC, Mau LW: Increased risk of mortality in the elderly population with late-stage chronic kidney disease: a cohort study in Taiwan. Nephrol Dial Transplant, 23: 3192-3198, 2008
10. Menendez R, Torres A, Zalacain R, Aspa J, Martin Villasclaras JJ, Borderias L, Benitez Moya JM, Ruiz-Manzano J, Rodriguez de Castro F, Blanquer J, Perez D, Puzo C, Sanchez Gascon F, Gallardo J, Alvarez C, Molinos L: Risk factors of treatment failure in community acquired pneumonia: implications for disease outcome. Thorax, 59: 960-965, 2004
11. Slinin Y, Foley RN, Collins AJ: Clinical epidemiology of pneumonia in
hemodialysis patients: the USRDS waves 1, 3, and 4 study. Kidney Int, 70:
1135-1141, 2006
12. Lim WH, Kireta S, Leedham E, Russ GR, Coates PT: Uremia impairs monocyte and monocyte-derived dendritic cell function in hemodialysis patients. Kidney Int, 72: 1138-1148, 2007
13. Anding K, Gross P, Rost JM, Allgaier D, Jacobs E: The influence of uraemia and haemodialysis on neutrophil phagocytosis and antimicrobial killing. Nephrol Dial Transplant, 18: 2067-2073, 2003
14. Sester U, Sester M, Hauk M, Kaul H, Kohler H, Girndt M: T-cell activation follows Th1 rather than Th2 pattern in haemodialysis patients. Nephrol Dial Transplant, 15: 1217-1223, 2000
15. Fernandez-Fresnedo G, Ramos MA, Gonzalez-Pardo MC, de Francisco AL, Lopez-Hoyos M, Arias M: B lymphopenia in uremia is related to an accelerated in vitro apoptosis and dysregulation of Bcl-2. Nephrol Dial Transplant, 15: 502-510, 2000
16. Kimmel PL, Phillips TM, Simmens SJ, Peterson RA, Weihs KL, Alleyne S, Cruz I, Yanovski JA, Veis JH: Immunologic function and survival in hemodialysis patients. Kidney Int, 54: 236-244, 1998
17. Arnold FW, Ramirez JA, McDonald LC, Xia EL: Hospitalization for community- acquired pneumonia: the pneumonia severity index vs clinical judgment.
Chest, 124: 121-124, 2003
18. Ewig S, Ruiz M, Mensa J, Marcos MA, Martinez JA, Arancibia F, Niederman MS, Torres A: Severe community-acquired pneumonia. Assessment of severity criteria. Am J Respir Crit Care Med, 158: 1102-1108, 1998
19. Di Angelantonio E, Chowdhury R, Sarwar N, Aspelund T, Danesh J, Gudnason V: Chronic kidney disease and risk of major cardiovascular disease and non- vascular mortality: prospective population based cohort study. BMJ, 341:
c4986, 2010
20. Palmer SC, Hayen A, Macaskill P, Pellegrini F, Craig JC, Elder GJ, Strippoli GF:
Serum levels of phosphorus, parathyroid hormone, and calcium and risks of death and cardiovascular disease in individuals with chronic kidney disease: a systematic review and meta-analysis. JAMA, 305: 1119-1127, 2011
21. Kent BD, Eltayeb EE, Woodman A, Mutwali A, Nguyen HT, Stack AG: The Impact of Chronic Obstructive Pulmonary Disease and Smoking on Mortality and Kidney Transplantation in End-Stage Kidney Disease. Am J Nephrol, 36:
287-295, 2012
22. van Gestel YR, Chonchol M, Hoeks SE, Welten GM, Stam H, Mertens FW, van
Domburg RT, Poldermans D: Association between chronic obstructive
pulmonary disease and chronic kidney disease in vascular surgery patients.
Nephrol Dial Transplant, 24: 2763-2767, 2009
23. Ruiz M, Ewig S, Marcos MA, Martinez JA, Arancibia F, Mensa J, Torres A:
Etiology of community-acquired pneumonia: impact of age, comorbidity, and severity. Am J Respir Crit Care Med, 160: 397-405, 1999
Acknowledgements
We thank the National Health Research Institute in Taiwan for providing the
insurance claims data. This study was supported in part by the Executive Yuan
National Science Council (grant number NSC 98-2621-M-039 -001), Clinical Trial
and Research Center of Excellence of the Department of Health (grant number
DOH101-TD-B-111-004), Taiwan Department of Health Cancer Research Center of
Excellence (grant number DOH101-TD-C-111-005) and the China Medical
University Hospital (grant number 1MS1).
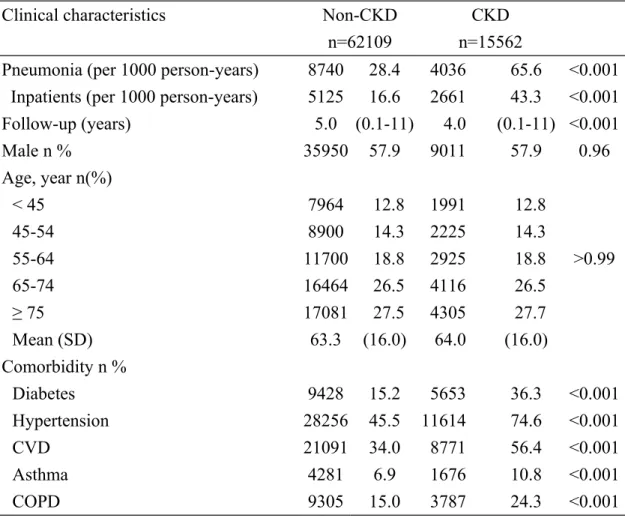
Table 1. Demographic data of patients with and without chronic kidney disease
(CKD)
Clinical characteristics Non-CKD
n=62109
CKD n=15562
Pneumonia (per 1000 person-years) 8740 28.4 4036 65.6 <0.001 Inpatients (per 1000 person-years) 5125 16.6 2661 43.3 <0.001
Follow-up (years) 5.0 (0.1-11) 4.0 (0.1-11) <0.001
Male n % 35950 57.9 9011 57.9 0.96
Age, year n(%)
< 45 7964 12.8 1991 12.8
>0.99
45-54 8900 14.3 2225 14.3
55-64 11700 18.8 2925 18.8
65-74 16464 26.5 4116 26.5
≥ 75 17081 27.5 4305 27.7
Mean (SD) 63.3 (16.0) 64.0 (16.0)
Comorbidity n %
Diabetes 9428 15.2 5653 36.3 <0.001
Hypertension 28256 45.5 11614 74.6 <0.001
CVD 21091 34.0 8771 56.4 <0.001
Asthma 4281 6.9 1676 10.8 <0.001
COPD 9305 15.0 3787 24.3 <0.001
*Pneumonia that required hospitalization, CVD: cardiovascular disease, COPD:
chronic obstructive pulmonary disease
Table 2. Characteristics of patients with and without pneumonia Clinical
characteristics
Pneumonia (-) n=64895
Pneumonia (outpatient)
n=5536
Pneumonia (inpatient)
n=7240
CKD n % 11526 17.8 1375 24.8
a2661 36.8
a,bMale n % 37126 57.2 3299 59.6
a4536 62.7
a,bAge n %
< 45 9311 14.4 453 8.2
a191 2.6
a,b45-54 10261 15.8 508 9.2
a356 4.9
a,b55-64 12952 20.0 880 15.9
a793 11.0
a,b65-74 16839 26.0 1671 30.2
a2070 28.6
a,b≥ 75 15532 23.9 2024 36.7
a3830 52.9
a,bComorbidity n %
Diabetes 11560 17.8 1260 22.8
a2261 31.2
a,bHypertension 31142 48.0 3414 61.7
a5314 73.4
a,bCVD 22692 35.0 2800 50.6
a4370 60.4
a,bAsthma 4097 6.3 886 16.0
a974 13.5
a,bCOPD 8900 13.7 1800 32.5
a2392 33.0
aCKD: chronic kidney disease, CVD: cardiovascular disease, COPD: chronic obstructive pulmonary disease
a
p < 0.05 in Chi-square test compared to patients without pneumonia
b