科技部補助專題研究計畫報告
Cilostazol對於血中PCSK9濃度之影響與改變血管內皮前驅細胞 數目和功能以及血管新生因子效應之關聯性(第2年)
報 告 類 別 : 成果報告 計 畫 類 別 : 個別型計畫
計 畫 編 號 : MOST 107-2314-B-006-076-MY2 執 行 期 間 : 108年08月01日至109年07月31日 執 行 單 位 : 國立成功大學醫學系內科學科
計 畫 主 持 人 : 趙庭興 共 同 主 持 人 : 李政翰
計畫參與人員: 學士級-專任助理:毛淑寰
博士後研究-博士後研究:曾詩雅
本研究具有政策應用參考價值:■否 □是,建議提供機關
(勾選「是」者,請列舉建議可提供施政參考之業務主管機關)
本研究具影響公共利益之重大發現:□否 □是
中 華 民 國 109 年 10 月 26 日
中 文 摘 要 : 背景及目標:周邊循環內皮前驅細胞(endothelial progenitor cells; EPCs),其數目及功能是心血管風險以及心血管疾病很重要 的生物標記。前蛋白轉化酶枯草溶菌素第九型(proprotein
convertase subtilisin/kexin type 9; PCSK9)血漿值與血脂濃度 及血糖指標有正向之關聯性,也跟冠心症之嚴重度相關;吾人發現 與週邊動脈硬化疾病之存在以及嚴重度相關外,也和周邊循環中 EPCs凋零數目及血管新生因子具有關聯性。吾人系列研究發現 cilostazol具血管新生效應,另外還可以在週邊血管病變患者上
,增加EPCs數目及功能。但目前為止並無cilostazol在冠心病患者 對於PCSK9濃度影響、EPCs數目及功能、血管新生因子等關聯性之探 討---這也是此次兩年的計劃的目標。
方法:吾人組成一個前瞻性雙盲隨機分組控制組之大型研究PEVA團 隊,納入穩定冠心症及高心血管風險患者,一組給予
cilostazol(100毫克每日兩次),一組給予贋品安慰劑(dummy placebo)。檢測受試者基礎點跟12週時血漿中PCSK9、完整血脂值
、EPCs數目及功能。主要療效終點(primary endpoint)為治療 12週EPCs數目、存活(viability)及PCSK9值之改變;另外尚有長 期追蹤之次要療效終點和其他療效終點。吾人假設cilostazol會影 響冠心症及心血管高風險者之PCSK9血漿濃度,而這個效應與 cilostazol改善血管內皮前驅細胞數目和功能相關。
結果:分析266位患者(134位使用cilostazol;132位使用安慰劑
)。吾人發現cilostazol治療會減少PCSK9及降低三酸甘油脂、增加 EPCs數目。PCSK9濃度改變與三酸甘油脂成正相關;總膽固醇以及低 密度膽固醇之濃度改變則和PCSK9濃度改變成負相關,但是和EPCs數 目的改變無關。在校正總膽固醇低密度膽固醇以及三酸甘油脂濃度 改變、EPCs數目改變以及糖尿病病史後,cilostazol治療仍與 PCSK9改變相關。追蹤臨床預後,吾人發現使用cilostazol治療組
,有較低之主要冠狀動脈事件發生率以及主要心血管以及腦血管事 件發生率,具統計顯著差異。
結論:本研究分析發現,在冠心症和心血管高風險患者上
,cilostazol治療與PCSK9濃度改變具統計相關意義,但跟是否已有 statin治療無關;cilostazol治療亦會改善某些代謝因子以及 EPCs的數目;此外cilostazol治療會顯著改善某些臨床預後。本研 究探討的主題是獨一無二的,對於學術及臨床實務將具重大衝擊影 響,引發更進一步之PCSK9研究,並造福廣大人類。
中 文 關 鍵 詞 : 前蛋白轉化酶枯草溶菌素第九型;cilostazol;冠心症;內皮前驅 細胞;血管新生
英 文 摘 要 : Background: Circulating endothelial progenitor cells (EPCs) have been considered as novel biomarkers of vascular
endothelial function on cardiovascular (CV) risks. Plasma proprotein convertase subtilisin/kexin type 9 (PCSK9)
levels are not only correlated with atherogenic lipoprotein levels but also with many other CV risk factors, and the presence and severity of coronary artery disease (CAD) and peripheral artery disease. We found that circulating EPC dysfunction and some vasculo-angiogenic biomarkers were
significantly correlated with PCSK9 levels. Recently, we and other researchers found that cilostazol has potential vasculoangiogenic effects and shows beneficial effects on human early EPCs in vitro and in vivo. However, there is no study aimed at the investigation of the effect of
cilostazol on plasma levels of PCSK9 and vasculo-angiogenic biomarkers and behavior of EPCs in patients with CAD.
Aims: This 2-year project is aimed at the investigation of the associations between the effect of cilostazol on the proprotein convertase subtilisin/kexin type 9
concentrations and the number and functions of circulating endothelial progenitor cells in patients with CAD or at a high risk of CV disease.
Methods: This was a prospective, randomized, double-blind, placebo-controlled trial, PEVA Study, which consecutively enrolled 266 eligible patients with stable CAD and at high risk of CV disease (ClinicalTrials.gov identifier:
NCT02174939). Serum or plasma levels of PCSK9 and complete lipid profiles, and the number and functions of EPCs were measured at baseline and 12 weeks. The influence of gender effect was also evaluated.
Results: Use of cilostazol (n = 134), but not placebo (n = 132), significantly reduced plasma PCSK9 concentrations and triglyceride levels, and increased the number of
circulating EPCs. Changes in PCSK9 levels were positively correlated with the changes in the triglyceride (TG) concentrations and were inversely correlated with changes in the total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels. After adjusting for changes in levels of TC, TG, LDL-C and the numbers of circulating EPCs and history of diabetes, use of cilostazol remained
independently associated with changes in plasma PCSK9 levels. Use of cilostazol, but not placebo, significantly reduced the risk of the major coronary event (MCE) and major adverse CV and cerebrovascular event (MACCE). After multi-variable adjustment, cilostazol treatment
independently predicted a lower risk of the MCE and MACCE.
Conclusion: This study showed that cilostazol treatment was significantly and independently associated with a decrease in plasma PCSK9 levels in patients with CAD or at a high risk of CV disease regardless of gender or background statin use and caused an improvement in some metabolic disorders and EPC numbers. Furthermore, cilostazol
treatment significantly reduced the risk of CV events in patients with CAD or at a high risk of CV disease. These results will be novel and clinically significant with translational therapy potential.
英 文 關 鍵 詞 : proprotein convertase subtilisin/kexin type 9; cilostazol;
coronary artery disease; endothelial progenitor cells;
angiogenesis
目錄
目錄………..….I 一、報告中英文摘要
(一) 中文摘要……….…………..…II (二) 英文摘要………...…III
二 報告內容: ... 1
(一) 前言 ... 1
(二) 研究目的 ... 2
(三) 文獻探討 ... 3
(四) 研究方法 ... 5
(五) 結果與討論(含結論與建議) ... 7
(六) 參考文獻 ... 8
(七) 表一 ... 11
(八) 表二 ... 12
(九) 表三 ... 133
(十) 表四 ... 144
(十一) 表五 ... 155
(十二) 表六 ... 166
(十三) 表七 ... 197
(十四) 表八及九... 11
(十五) 圖一 ... 129
一、報告中英文摘要:
(一) 報告中文摘要。
背景及目標:周邊循環內皮前驅細胞(endothelial progenitor cells; EPCs),其數目及功能是心血管風險 以 及 心 血 管 疾 病 很 重 要 的 生 物 標 記 。 前 蛋 白 轉 化 酶 枯 草 溶 菌 素 第 九 型 (proprotein convertase subtilisin/kexin type 9; PCSK9)血漿值與血脂濃度及血糖指標有正向之關聯性,也跟冠心症之嚴重度相
關;吾人發現與週邊動脈硬化疾病之存在以及嚴重度相關外,也和周邊循環中 EPCs 凋零數目及血管
新生因子具有關聯性。吾人系列研究發現cilostazol 具血管新生效應,另外還可以在週邊血管病變患者
上,增加 EPCs 數目及功能。但目前為止並無 cilostazol 在冠心病患者對於 PCSK9 濃度影響、EPCs
數目及功能、血管新生因子等關聯性之探討---這也是此次兩年的計劃的目標。
方法:吾人組成一個前瞻性雙盲隨機分組控制組之大型研究PEVA 團隊,納入穩定冠心症及高心血管
風險患者,一組給予 cilostazol(100 毫克每日兩次),一組給予贋品安慰劑(dummy placebo)。檢測
受試者基礎點跟12 週時血漿中 PCSK9、完整血脂值、EPCs 數目及功能。主要療效終點(primary endpoint)
為治療12 週 EPCs 數目、存活(viability)及 PCSK9 值之改變;另外尚有長期追蹤之次要療效終點
和其他療效終點。吾人假設cilostazol 會影響冠心症及心血管高風險者之 PCSK9 血漿濃度,而這個效
應與cilostazol 改善血管內皮前驅細胞數目和功能相關。
結果:分析 266 位患者(134 位使用 cilostazol;132 位使用安慰劑)。吾人發現 cilostazol 治療會 減少 PCSK9 及降低三酸甘油脂、增加 EPCs 數目。PCSK9 濃度改變與三酸甘油脂成正相關;總膽固醇以 及低密度膽固醇之濃度改變則和 PCSK9 濃度改變成負相關,但是和 EPCs 數目的改變無關。在校正總 膽固醇低密度膽固醇以及三酸甘油脂濃度改變、EPCs 數目改變以及糖尿病病史後,cilostazol 治療 仍與 PCSK9 改變相關。追蹤臨床預後,吾人發現使用 cilostazol 治療組,有較低之主要冠狀動脈事 件發生率以及主要心血管以及腦血管事件發生率,具統計顯著差異。
結論:本研究分析發現,在冠心症和心血管高風險患者上,cilostazol 治療與 PCSK9 濃度改變具統計 相關意義,但跟是否已有 statin 治療無關;cilostazol 治療亦會改善某些代謝因子以及 EPCs 的數 目;此外 cilostazol 治療會顯著改善某些臨床預後。本研究探討的主題是獨一無二的,對於學術及臨 床實務將具重大衝擊影響,引發更進一步之 PCSK9 研究,並造福廣大人類。
關鍵詞:前蛋白轉化酶枯草溶菌素第九型;cilostazol;冠心症;內皮前驅細胞;血管新生
[在此鍵入] III [在此鍵入]
(二) 報告英文摘要。
Background: Circulating endothelial progenitor cells (EPCs) have been considered as novel biomarkers of vascular endothelial function on cardiovascular (CV) risks. Plasma proprotein convertase subtilisin/kexin type 9 (PCSK9) levels are not only correlated with atherogenic lipoprotein levels but also with many other CV risk factors, and the presence and severity of coronary artery disease (CAD) and peripheral artery disease. We found that circulating EPC dysfunction and some vasculo-angiogenic biomarkers were significantly correlated with PCSK9 levels. Recently, we and other researchers found that cilostazol has potential vasculoangiogenic effects and shows beneficial effects on human early EPCs in vitro and in vivo. However, there is no study aimed at the investigation of the effect of cilostazol on plasma levels of PCSK9 and vasculo-angiogenic biomarkers and behavior of EPCs in patients with CAD.
Aims: This 2-year project is aimed at the investigation of the associations between the effect of cilostazol on the proprotein convertase subtilisin/kexin type 9 concentrations and the number and functions of circulating endothelial progenitor cells in patients with CAD or at a high risk of CV disease.
Methods: This was a prospective, randomized, double-blind, placebo-controlled trial, PEVA Study, which consecutively enrolled 266 eligible patients with stable CAD and at high risk of CV disease
(ClinicalTrials.gov identifier: NCT02174939). Serum or plasma levels of PCSK9 and complete lipid profiles, and the number and functions of EPCs were measured at baseline and 12 weeks. The influence of gender effect was also evaluated.
Results: Use of cilostazol (n = 134), but not placebo (n = 132), significantly reduced plasma PCSK9 concentrations and triglyceride levels, and increased the number of circulating EPCs. Changes in PCSK9 levels were positively correlated with the changes in the triglyceride (TG) concentrations and were inversely correlated with changes in the total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels.
After adjusting for changes in levels of TC, TG, LDL-C and the numbers of circulating EPCs and history of diabetes, use of cilostazol remained independently associated with changes in plasma PCSK9 levels. Use of cilostazol, but not placebo, significantly reduced the risk of the major coronary event (MCE) and major adverse CV and cerebrovascular event (MACCE). After multi-variable adjustment, cilostazol treatment independently predicted a lower risk of the MCE and MACCE.
Conclusion: This study showed that cilostazol treatment was significantly and independently associated with a decrease in plasma PCSK9 levels in patients with CAD or at a high risk of CV disease regardless of gender or background statin use and caused an improvement in some metabolic disorders and EPC numbers.
Furthermore, cilostazol treatment significantly reduced the risk of CV events in patients with CAD or at a high risk of CV disease. These results will be novel and clinically significant with translational therapy potential.
Keywords: proprotein convertase subtilisin/kexin type 9; cilostazol; coronary artery disease;
endothelial progenitor cells; angiogenesis
二 報告內容:
(一) 前言。
Proprotein convertase subtilisin/kexin type 9 (PCSK9), a newly recognized protein, plays a key role in cholesterol homeostasis by enhancing degradation of hepatic low-density lipoprotein receptor. Interestingly, PCSK9 is also involved in the inflammatory and oxidative process. Some studies have revealed that plasma PCSK9 levels could be affected with drugs such as statins. Statins significantly increase PCSK9
concentrations probably via upregulation of sterol regulatory element-binding protein-2 (SREBP-2).
Interestingly, the expression of PCSK9 can be regulated not only by SREBP-2 but also by peroxisome proliferator-activated receptor-γ (PPARγ) and adenosine monophosphate-activated protein kinase (AMPK) signaling pathways. Recently, we and other researchers found that this compound has potential
vasculoangiogenic effects and shows beneficial effects on human early EPCs in vitro and in vivo. However, there is no study aimed at the investigation of the effect of cilostazol on plasma levels of PCSK9 in patients with coronary artery disease (CAD). In light of stimulating effect of cilostazol on PPARγ and AMPK signaling pathways, the effect of this compound on PCSK9 concentrations could be anticipated.
We previously found that circulating endothelial progenitor cell (EPC) dysfunction and some vasculo- angiogenic and oxidative biomarkers were significantly correlated with PCSK9 levels. However, there is no study aimed at the investigation of the effect of cilostazol on the PCSK9 levels and the behaviors of EPCs in patients with CAD and at a high risk of cardiovascular (CV) disease (CVD).
2
(二) 研究目的。
This was a prospective, randomized, double-blind, placebo-controlled trial, PEVA Study, consecutively enrolled 266 eligible patients with stable CAD and at high risk of CV disease. We hypothesized that cilostazol treatment would result in a significant change in PCSK9 concentrations associated with the changes in the number and functions of EPCs in patients with CAD and at a high risk of CVD.
# Specific aims
1. To evaluate the effects of cilostazol on PCSK9 concentrations in patients with CAD and at a high risk of CVD.
2. To evaluate the effects of cilostazol on the number and functions of circulating EPCs in patients with CAD and at a high risk of CVD.
3. To evaluate the associations between the effects of cilostazol on PCSK9 concentrations and the number and functions of circulating EPCs.
4. To investigate the outcome effect of cilostazol in patients with CAD or at a high risk of CVD.
(三) 文獻探討。
# Background
1. PCSK9 plays an important role in lipid homeostasis and atherosclerosis
PCSK9, a newly recognized protein, plays an important role in cholesterol homeostasis and affects plasma lipoprotein levels by enhancing the degradation of hepatic low-density lipoprotein receptors and subsequently reducing expression of these receptors on hepatocytes, thereby leading to increased plasma levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) [1]. From a genetic point of view,
individuals with certain sequence variations in the PCSK9 gene have not only lower plasma LCL-C levels but also a lower incidence of CAD [2]. Plasma PCSK9 levels are not only correlated with atherogenic lipoprotein levels but also with many other cardiovascular risk factors, such as fasting plasma glucose, age, and blood pressure [3, 4]. In addition to traditional risk factors, PCSK9 is also associated with non-traditional risk factors involving inflammatory and oxidative processes [5-9]. Moreover, plasma PCSK9 levels have been reported to be associated with the severity of CAD [10], and the presence of peripheral artery disease, especially those with extensive, severe, and complicated peripheral artery disease [11]. We found that circulating EPC dysfunction, in particular, the number of apoptotic circulating endothelial cells, and some vasculo-angiogenic and oxidative biomarkers were significantly correlated with PCSK9 levels [11]. Taken together, PCSK9 protein is an important target for the prevention and treatment of atherosclerosis.
2. The potential mechanisms responsible for statins- or others-induced changes in PCSK9 levels
Some studies have revealed that plasma PCSK9 levels were affected by some drugs, such as an increase in PCSK9 levels with the use of statins [12], ezetimibe [13], and fibrates [14], and a decrease with nicotinic acid treatment [15]. The mechanisms underlying the effect of the above compounds on PCSK9 concentrations is poorly understood and could only be speculated. Statins [12] and fibrates [14] significantly increase PCSK9 concentrations probably via upregulation of SREBP-2. In contrast, the mechanisms for ezetimibe and niacin are not well known [13, 15]. Recently, some studies have indicated a relationship between PCSK9 and the metabolism of high-density lipoprotein cholesterol (HDL-C) [16] and triglyceride [17]. Interestingly, the expression of PCSK9 can be regulated not only by SREBP-2 but also by PPARγ [18, 19]. Furthermore, activation of the adiponectin receptor can also regulate PCSK9 expression through activation of PPARγ and the AMPK signaling pathway [19].
3. The vasculo-angiogenesis effects of cilostazol in vitro and in vivo
Cilostazol, a phosphodiesterase 3 inhibitor, is licensed for treatment of patients with peripheral artery disease and intermittent claudication owing to its antiplatelet and vasodilatory effects [20-22]. Recently, we
4
and other researchers found that this compound has beneficial effects on metabolic parameters, angiogenesis, numbers and functions of circulating human early EPCs in vitro [20, 23-26], in vivo [20, 23-26], and in clinical settings [21, 22]. In particular, cilostazol treatment is beneficial for a reduction in triglyceride levels and an increase in HDL-C levels in patients with peripheral artery disease [21, 27] or at high risk of CVD [22]. However, no study has investigated the effect of cilostazol on plasma PCSK9 levels.
4. The speculated effects and mechanisms of cilostazol on PCSK9 concentrations and the potential
associations between the effect of cilostazol on the PCSK9 concentrations and the number and functions of circulating EPCs and vasculo-angiogenesis factors
Our previous experimental studies revealed that cilostazol could serve as an activator of AMPK signaling molecules [23] and adiponectin receptors (unpublished data), by which cilostazol can provide vasculo-
angiogenesis effects in EPCs and vascular endothelial cells. According to our previous clinical trial, we found that cilostazol treatment could also increase adiponectin concentrations in patients with peripheral artery disease. In addition, Sanada et al. found that induction of angiogenesis by cilostazol was through activation of PPARγ [28]. Taken together, we hypothesized that cilostazol treatment would result in a significant change in PCSK9 concentrations associated with the changes in the number and functions of EPCs in patients with CAD and at a high risk of CVD.
(四) 研究方法。
MATERIALS AND METHODS 1. Study design
The current study was originally designed as a prospective, single-center, double-blind, double-dummy, superior, randomized placebo-controlled trial. This study protocol (version 4.0; October 21, 2015) has been approved by the Institutional Review Board (IRB) of National Cheng Kung University Hospital (identifier:
A-BR-102-076) as well as registered in ClinicalTrials.gov (identifier: NCT 02174939).
2. Participants and eligibility Inclusion criteria
This study consecutively enrolled 266 patients with stable CAD (age > 20 years), including old myocardial infarction (MI) (>6 months), and high risk for CVD. The definitions of CAD and high risk for CVD were described in the approved protocol.
Exclusion criteria
Subjects were excluded if they had at least one of the following situations before screening: 1) had unstable CAD ; 2) had plan to do revascularization within recent 3 months; 3) had severe liver dysfunction;
4) had left ventricular dysfunction; 5) documented active malignancy; 6) had chronic inflammatory disease;
7) current use of cilostazol or any other cAMP-elevator; 8) had known drug allergy history for cilostazol;
and 9) premenopausal women. All study participants gave informed consent and this study followed the regulation of the ethics committee of the National Cheng Kung University Hospital.
3. Blinding and randomization
Participants, participants’ relatives, care providers and those assessing biomarkers, EPCs and clinical endpoints were all blinded and the statistical analyses were also conducted blinded with intervention.
4. Allocation and interventions: study drugs
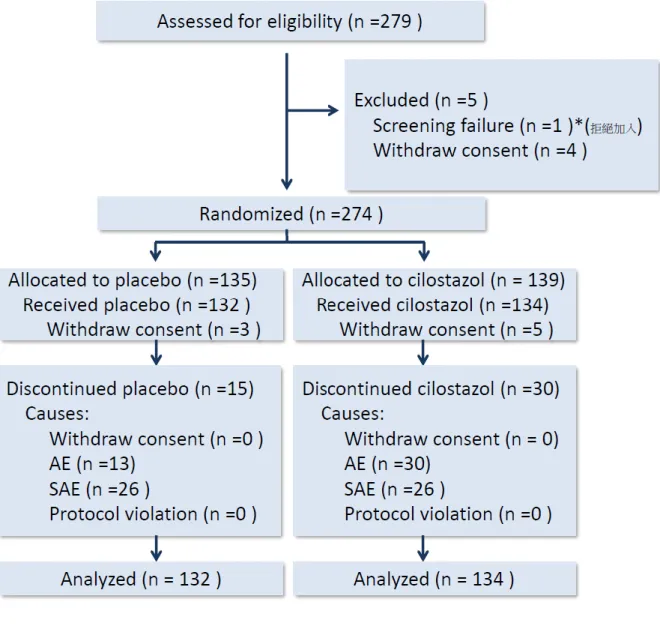
Patients were randomly assigned to receive cilostazol (100 mg twice daily) or matching dummy placebo twice daily. The participant flow scheme is shown in Figure 1.
5. Blood sampling and measurement of serum or plasma biomarkers
The baseline blood samples were obtained from the peripheral veins in all participants before treatment and the final samples were obtained using the same procedure one day immediately after 12-week treatment.
The blood samples were sent for isolation, cell culture, and assay of human EPCs, and prepared and stored for use in an enzyme-linked immunosorbent assay, as described previously [11, 21, 22].Plasma or serum concentrations of biomarkers were measured using commercial kits (R&D Systems Inc., Minneapolis, MN, USA; and Mercodia AB, Uppsala, Sweden).
6. Isolation and culture of EPCs, and determination of numbers of circulating EPCs and apoptotic endothelial cells
Isolation of early EPCs was performed by Ficoll density gradient centrifugation according to standard protocols, and colony formation by EPCs was identified and quantified, as described previously [11, 21- 23]. EPCs were defined as CD45-CD34+ kinase insert domain receptor (KDR)+ cells, and circulating
6
endothelial cells were defined as CD45-CD146+ annexin V+ cells [11, 22]. All fluorescence-labeled antibodies were purchased from Becton Dickinson (Arlington, VA, USA).
7. Measurement of EPC functions in vitro
As previously described [11, 21-23], EPC migration was measured using modified Boyden chambers, proliferation and viability were assessed by bromodeoxyuridine (BrdU) and 2,3-bis-(2-methoxy-4-nitro-5- sulfophenyl)-2H-tetrazolium-5-carboxanilide (XTT) assays, and EPC apoptosis was determined using a terminal 2′-deoxyuridine 5′-triphosphate nick end labeling assay kit (Roche, Basel, Switzerland).
8. Data collection and outcome measurement
Clinical outcomes were obtained by chart review and followed up by clinic visit, telephone call or direct contact with participants or subjects’ family at 3 months after starting treatment and every 6 months thereafter. The primary endpoint of the current study was the number of circulating EPCs and plasma PCSK9 levels after 12-week treatment, and the secondary outcome measures included viability (proliferation) of EPCs after 12-week treatment, long-term composite major adverse cardiac event (MACE) (CV death, nonfatal MI, nonfatal stroke, congestive heart failure, or unplanned coronary revascularization), major coronary event (MCE) (MI, angina pectoris, or unplanned coronary revascularization) and major adverse cardiovascular and cerebrovascular events (MACCE) (CV death, nonfatal MI, nonfatal stroke, CHF, major amputation, minor amputation, or unplanned coronary revascularization).
9. Statistical analysis
Each analysis was performed in a per-protocol manner. Distributions of numerical variables in both groups were expressed as mean standard deviation, and skewed data were reported as median (interquartile range). Chi-square or Fisher’s exact test were performed for comparing categorical variables between groups, whereas the Mann-Whitney U test or unpaired Student’s t-test were performed for comparing numerical variables, as appropriate. Differences between baseline and post-treatment values were analyzed by the Wilcoxon signed-rank test or paired Student’s t-test, as appropriate. The Pearson correlation or Spearman's rank correlation coefficient (Spearman's rho) was used to assess the relationship between the changes in metabolic factor levels in the plasma or serum, EPC parameters, and changes in plasma PCSK9 levels after treatment over the entire cohort. The independent correlation of cilostazol use with the changes in plasma PCSK9 levels was adjusted for all uni-variables (a P value < 0.1) with a multivariable linear regression model by a stepwise regression method. Each analysis was performed by
“intention-to-treat”. Kaplan-Meier analysis was used to study patient survival and event-free status, using the log-rank test (Cox-Mantel) to ascertain differences between groups. A P 0.05 (2-sided) was considered to indicate statistical significance. All statistical analyses were performed using SPSS for Windows (Version 13.0, SPSS Inc., Chicago, IL, USA).
(五) 結果與討論(含結論與建議)。 RESULTS
266 cases (n = 134 with 200 mg/d cilostazol treatment; n = 132 with dummy placebo) were analyzed. The results of the current study were shown below.
1. The baseline characteristics of 266 participants were demonstrated in Table 1. Participants assigned to cilostazol treatment were younger and had higher prevalence of peripheral artery disease and the experience of aspirin use and coronary artery bypass surgery.
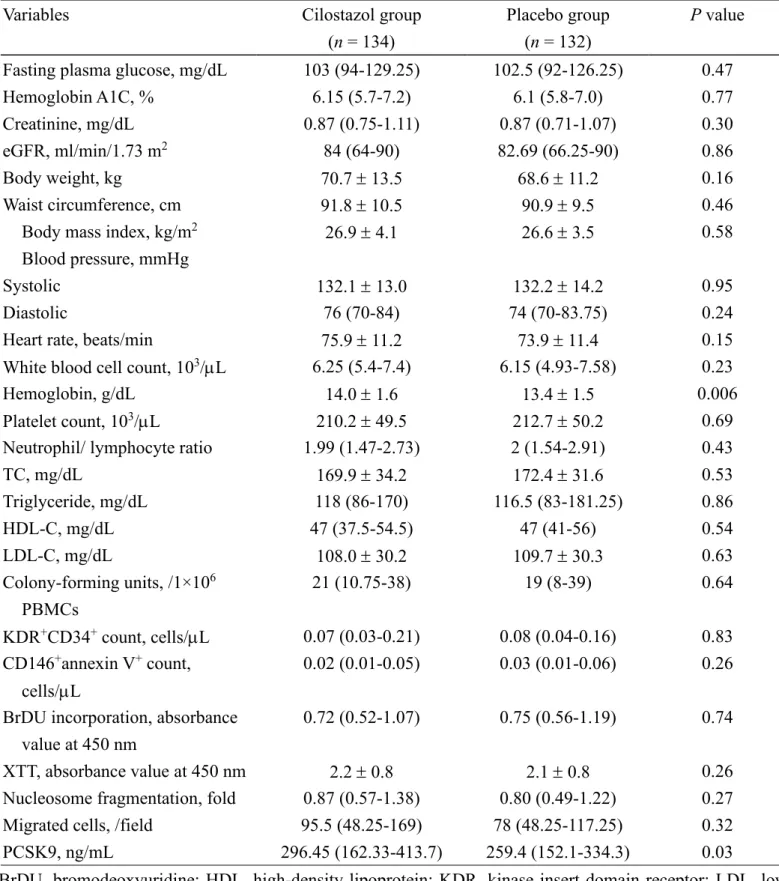
2. The baseline laboratory data were compared between both groups (Table 2). Those were almost well matched except for the hemoglobin and PCSK9 levels.
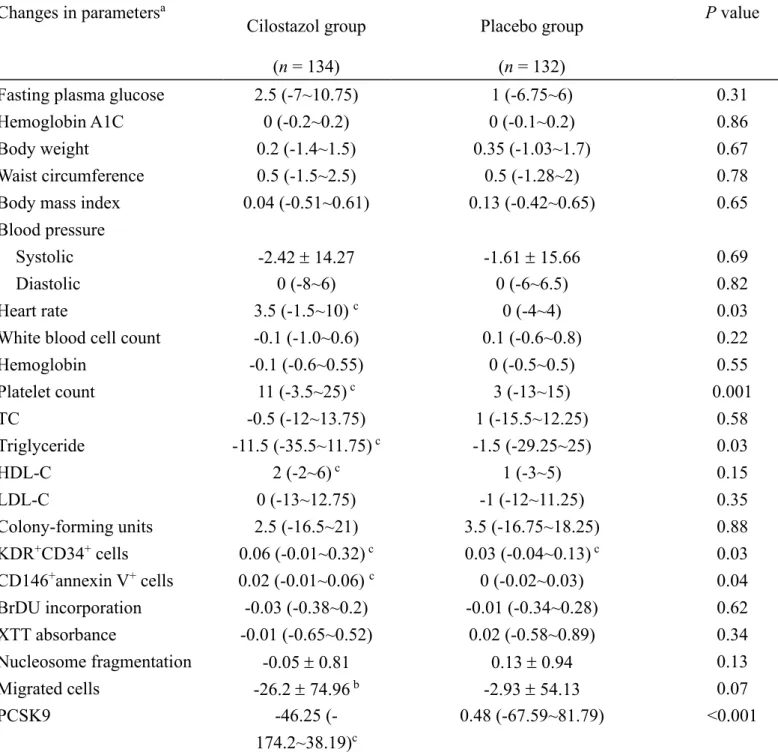
3. Comparisons of changes in the background parameters, number of circulating EPCs and apoptotic
endothelial cells, in vitro EPC functions, and serum/plasma biomarker levels, after treatment between the groups are demonstrated in Table 3. Cilostazol treatment significantly decreased plasma PCSK9 levels and improved triglyceride levels despite no statistically significant changes in the TC and LDL-C levels
between the groups. Use of cilostazol, but not placebo, significantly increased the circulating EPC count and the apoptotic endothelial cell count with a trend toward to reduce migration capacity of EPCs, without any effects on or other EPC functions.
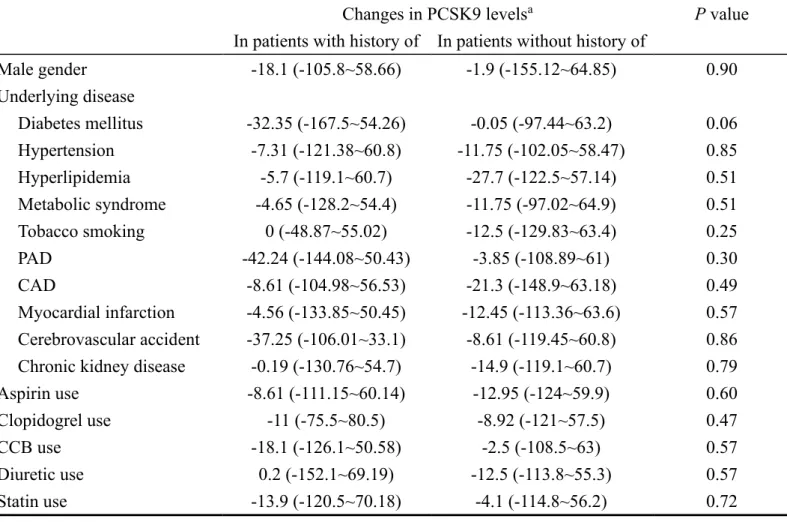
4. Table 4 demonstrated that changes in PCSK9 plasma levels were similar with respect to the background characteristics or medications despite a trend toward more reduction in PCSK9 levels in patients with diabetes mellitus. Of note, changes in PCSK9 levels was similar in patients regardless of gender or statin use during the 3-month study period.
5. Changes in PCSK9 levels were positively correlated with the changes in the triglyceride concentrations and were inversely correlated with changes in the TC and LDL-C levels (Table 5).
6. By using multi-variable analysis, we could not identify any factor which was independently associated with changes in the plasma PCSK9 levels (Table 6).
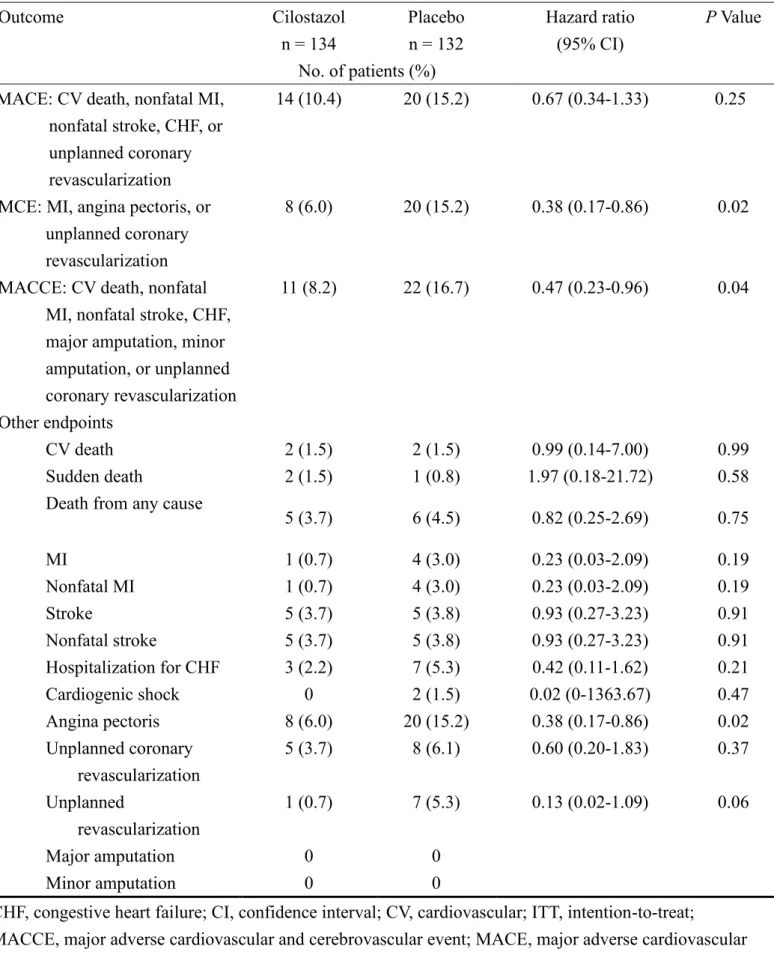
7. During clinical follow-up, our data showed that use of cilostazol, but not placebo, significantly reduced the risk of the MCE and MACCE, whereas cilostazol treatment had only a borderline effect on risk reduction in the MACE (Table 7).
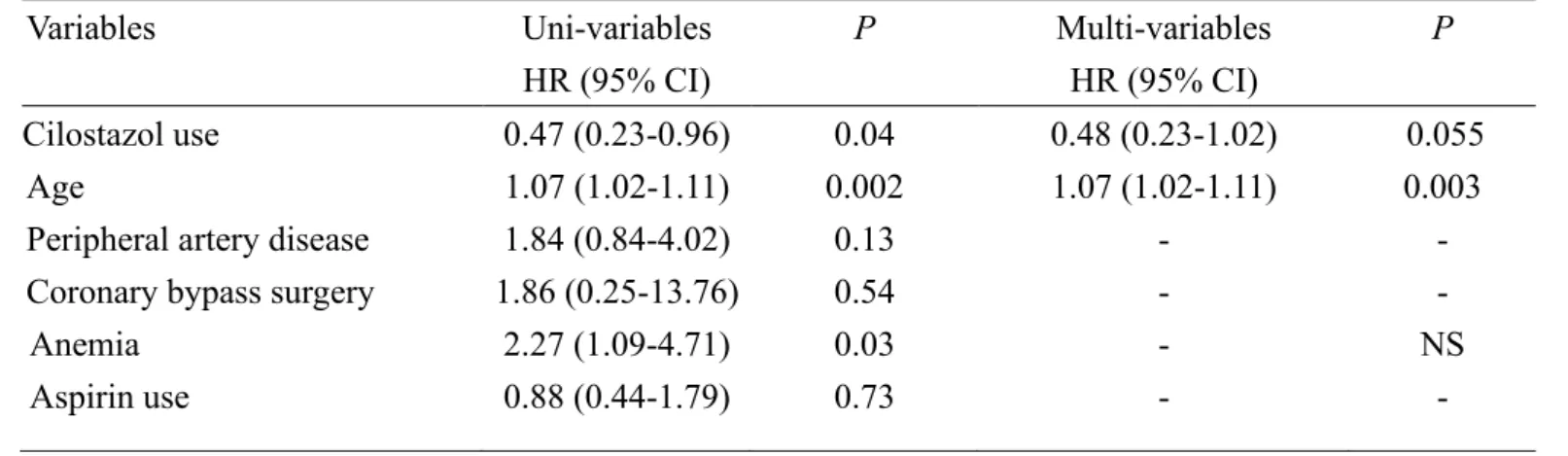
8. After multi-variable adjustment, cilostazol treatment independently predicted a lower risk of the MCE and MACCE (Table 8 and 9).
CONCLUSIONS AND SUGGESTIONS
1. This study revealed that cilostazol treatment was significantly and independently associated with a decrease in plasma PCSK9 levels in patients with CAD or at a high risk of CV disease regardless of gender or background statin use and caused an improvement in some metabolic disorders and EPC numbers. These results will be novel and clinically significant with translational therapy potential.
2. Therefore, cilostazol use might have a prognostic impact in patients with CAD or at a high risk of CVD.
8
(六) 參考文獻
1. Li S, Li JJ. PCSK9: A key factor modulating atherosclerosis. J Atheroscler Thromb. 2015; 22: 221-230.
2. Cohen JC, Boerwinkle E, Mosley Jr TH, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006; 354: 1264-1272.
3. Baass A, Dubuc G, Tremblay M, Delvin EE, O’Loughlin J, Levy E, Davignon J, Lambert M. Plasma PCSK9 is associated with age, sex, and multiple metabolic markers in a population-based sample of children and adolescents. Clin Chem. 2009; 55: 1637-1645.
4. Cui Q, Ju X, Yang T, Zhang M, Tang W, Chen Q, Hu Y, Haas JV, Troutt JS, Pickard RT, Darling R, Konrad RJ, Zhou H, et al. Serum PCSK9 is associated with multiple metabolic factors in a large Han Chinese population. Atherosclerosis. 2010; 213: 632-636.
5. Feingold KR, Moser AH, Shigenaga JK, Patzek SM, Grunfeld C. Inflammation stimulates the expression of PCSK9. Biochem Biophys Res Commun. 2008; 374: 341-344.
6. Urban D, Pöss J, Böhm M, Laufs U. Targeting the proprotein convertase subtilisin/kexin type 9 for the treatment of dyslipidemia and atherosclerosis. J Am Coll Cardiol. 2013; 62: 1401-1408.
7. Zhang Y, Zhu CG, Xu RX, Li S, Guo YL, Sun J, Li JJ. Relation of circulating PCSK9 concentration to fibrinogen in patients with stable coronary artery disease. J Clin Lipidol. 2014; 8: 494-500.
8. Li S, Guo YL, Xu RX, Zhang Y, Zhu CG, Sun J, Qing P, Wu NQ, Jiang LX, Li JJ. Association of plasma PCSK9 levels with white blood cell count and its subsets in patients with stable coronary artery disease.
Atherosclerosis. 2014; 234: 441-445.
9. Ding Z, Liu S, Wang X, Deng X, Fan Y, Shahanawaz J, Shmookler Reis RJ, Varughese KI, Sawamura T, Mehta JL. Cross-talk between LOX-1 and PCSK9 in vascular tissues. Cardiovasc Res. 2015; 107:
556-567.
10. Li S, Guo YL, Xu RX, Zhang Y, Zhu CG, Sun J, Qing P, Wu NQ, Li JJ. Plasma PCSK9 levels are associated with the severity of coronary stenosis in patients with atherosclerosis. Int J Cardiol. 2014;
174: 863-864.
11. Chao TH, Chen IC, Li YH, Lee PT, Tseng SY. Plasma Levels of proprotein convertase subtilisin/kexin type 9 are elevated in patients with peripheral artery disease and associated with metabolic disorders and dysfunction in circulating progenitor cells. J Am Heart Assoc. 2016; 5: e003497.
12. Sahebkar A, Simental-Mendía LE, Guerrero-Romero F, Golledge J, Watts GF. Effect of statin therapy on plasma proprotein convertase subtilisin kexin 9 (PCSK9) concentrations: a systematic review and meta-analysis of clinical trials. Diabetes Obes Metab. 2015; 17: 1042-1055.
13. Davignon J, Dubuc G. Statins and ezetimibe modulate plasma proprotein convertase subtilisin kexin- 9 (PCSK9) levels. Trans Am Clin Climatol Assoc. 2009; 120: 163-173.
14. Sahebkar A. Circulating levels of proprotein convertase subtilisin kexin type 9 are elevated by fibrate therapy: a systematic review and meta-analysis of clinical trials. Cardiol Rev. 2014; 22: 306-312.
15. Croyal M, Ouguerram K, Passard M, Ferchaud-Roucher V, Chétiveaux M, Billon-Crossouard S, de Gouville AC, Lambert G, Krempf M, Nobécourt E. Effects of extended-release nicotinic acid on apolipoprotein (a) kinetics in hypertriglyceridemic patients. Arterioscler Thromb Vasc Biol. 2015; 35:
2042-2047.
16. Choi S, Korstanje R. Proprotein convertases in high-density lipoprotein metabolism. Biomark Res.
2013; 1: 27.
17. Druce I, Abujrad H, Ooi TC. PCSK9 and triglyceride-rich lipoprotein metabolism. J Biomed Res. 2015;
29: 429-436.
18. Duan Y, Chen Y, Hu W, Li X, Yang X, Zhou X, Yin Z, Kong D, Yao Z, Hajjar DP, Liu L, Liu Q, Han J. Peroxisome proliferator-activated receptor γ activation by ligands and dephosphorylation induces proprotein convertase subtilisin kexin type 9 and low density lipoprotein receptor expression. J Biol Chem. 2012; 287: 23667-23677.
19. Sun L, Yang X, Li Q, Zeng P, Liu Y, Liu L, Chen Y, Yu M, Ma C, Li X, Li Y, Zhang R, Zhu Y, et al.
Activation of adiponectin receptor regulates proprotein convertase subtilisin/kexin type 9 expression and inhibits lesions in ApoE-deficient mice. Arterioscler Thromb Vasc Biol. 2017; 37: 1290-1300.
20. Chao TH, Tseng SY, Li YH, Liu PY, Cho CL, Shi GY, Wu HL, Chen JH. A novel vasculo-angiogenic effect of cilostazol mediated by cross-talk between multiple signalling pathways including the ERK/p38 MAPK signaling transduction cascade. Clin Sci. (Lond) 2012; 123: 147-159.
21. Chao TH, Tseng SY, Chen IC, Tsai YS, Huang YY, Liu PY, Ou HY, Li YH, Wu HL, Cho CL, Tsai LM, Chen JH. Cilostazol enhances mobilization and proliferation of endothelial progenitor cells and collateral formation by modifying vasculo-angiogenic biomarkers in peripheral arterial disease. Int J Cardiol. 2014; 172: e371-374.
22. Chao TH, Chen IC, Lee CH, Chen JY, Tsai WC, Li YH, Tseng SY, Tsai LM, Tseng WK. Cilostazol enhances mobilization of circulating endothelial progenitor cells and improves endothelium-dependent function in patients at high risk of cardiovascular disease. Angiology. 2016; 67: 638-646.
23. Tseng SY, Chao TH, Li YH, Liu PY, Lee CH, Cho CL, Wu HL, Chen JH. Cilostazol improves high glucose-induced impaired angiogenesis in human endothelial progenitor cells and vascular endothelial cells as well as enhances vasculoangiogenesis in hyperglycemic mice mediated by the adenosine monophosphate-activated protein kinase pathway. J Vasc Surg. 2016; 63: 1051-1062.e3.
24. Tseng SY, Chao TH, Li YH, Cho CL. Cilostazol improves proangiogenesis functions in human early endothelial progenitor cells through the stromal cell-derived factor system and hybrid therapy provides a synergistic effect in vivo. Biomed Res Int. 2016; 2016: 3639868.
25. Biscetti F, Pecorini G, Straface G, Arena V, Stigliano E, Rutella S, Locatelli F, Angelini F, Ghirlanda G, Flex A. Cilostazol promotes angiogenesis after peripheral ischemia through a VEGF-dependent mechanism. Int J Cardiol. 2013; 167: 910-916.
26. Kawabe-Yako R, Ii M, Masuo O, Asahara T, Itakura T. Cilostazol activates function of bone marrow-
10
derived endothelial progenitor cell for re-endothelialization in a carotid balloon injury model. PLoS One. 2011; 6: e24646.
27. O'Donnell ME, Badger SA, Sharif MA, Young IS, Lee B, Soong CV. The vascular and biochemical effects of cilostazol in patients with peripheral arterial disease. J Vasc Surg. 2009; 49: 1226-1234.
28. Sanada F, Kanbara Y, Taniyama Y, Otsu R, Carracedo M, Ikeda-Iwabu Y, Muratsu J, Sugimoto K, Yamamoto K, Rakugi H, Morishita R. Induction of angiogenesis by a type III phosphodiesterase inhibitor, cilostazol, through activation of peroxisome proliferator-activated receptor-γ and cAMP pathways in vascular cells. Arterioscler Thromb Vasc Biol. 2016; 36: 545-552.
(七) 表一
Table 1. Comparisons of baseline characteristics between participants assigned to cilostazol or placebo treatment
Cilostazol n = 134
Placebo n = 132
P Value
Age, years 64.5 9.6 67.2 9.9 0.03
Male gender 104 (77.6) 91 (68.9) 0.11
Underlying disease
PAD 27 (20.1) 14 (10.6) 0.03
CAD 103 (76.9) 97 (73.5) 0.52
Old myocardial infarction 38 (28.4) 29 (22.0) 0.23
Old cerebrovascular accident 8 (6.0) 5 (3.8) 0.41
Diabetes mellitus 54 (40.3) 51 (38.6) 0.78
Hypertension 101 (75.4) 106 (80.3) 0.33
Hyperlipidemia 108 (80.6) 102 (77.3) 0.51
Metabolic syndrome 77 (57.5) 79 (59.8) 0.69
Tobacco smoking 30 (22.4) 27 (20.5) 0.70
Peptic ulcer disease 28 (20.9) 43 (32.6) 0.03
Chronic kidney disease 13 (9.7) 14 (10.6) 0.81
Percutaneous coronary intervention 67 (50.0) 65 (49.2) 0.90
Coronary artery bypass surgery 6 (4.5) 0 0.03
Anemia 24 (18.2) 41 (31.1) 0.015
Aspirin use 94 (70.1) 77 (58.3) 0.04
Clopidogrel use 12 (9.0) 19 (14.4) 0.17
Ticagrelor use 1 (0.7) 2 (1.5) 0.62
ACEI use 37 (27.6) 31 (23.5) 0.44
ARB use 47 (35.1) 51 (38.6) 0.55
CCB use 68 (50.7) 56 (42.4) 0.17
Diuretic use 31 (23.1) 35 (26.5) 0.52
Statin use 76 (56.7) 66 (50.0) 0.27
Fibrate use 1 (0.7) 3 (2.3) 0.37
Thiazolidinedione use 4 (3.0) 5 (3.8) 0.75
DPP4 inhibitor use 7 (5.2) 8 (6.1) 0.77
GLP-1 antagonist use 0 0
Data are expressed as mean SD or n (%), as appropriate. P values compared between both groups were obtained using an unpaired Student’s t test or 2 test. ACEI indicates angiotensin-converting enzyme inhibitor;
ARB, angiotensin receptor blocker; CCB, calcium channel blocker; DPP4, dipeptidyl peptidase-4; GLP-1, glucagon -like peptide-1.
12
(八) 表二
Table 2. Baseline laboratory data between patients in the cilostazol treatment and placebo groups
Variables Cilostazol group
(n = 134)
Placebo group (n = 132)
P value
Fasting plasma glucose, mg/dL 103 (94-129.25) 102.5 (92-126.25) 0.47
Hemoglobin A1C, % 6.15 (5.7-7.2) 6.1 (5.8-7.0) 0.77
Creatinine, mg/dL 0.87 (0.75-1.11) 0.87 (0.71-1.07) 0.30 eGFR, ml/min/1.73 m2 84 (64-90) 82.69 (66.25-90) 0.86
Body weight, kg 70.7 13.5 68.6 11.2 0.16
Waist circumference, cm 91.8 10.5 90.9 9.5 0.46
Body mass index, kg/m2 26.9 4.1 26.6 3.5 0.58
Blood pressure, mmHg
Systolic 132.1 13.0 132.2 14.2 0.95
Diastolic 76 (70-84) 74 (70-83.75) 0.24
Heart rate, beats/min 75.9 11.2 73.9 11.4 0.15
White blood cell count, 103/L 6.25 (5.4-7.4) 6.15 (4.93-7.58) 0.23
Hemoglobin, g/dL 14.0 1.6 13.4 1.5 0.006
Platelet count, 103/L 210.2 49.5 212.7 50.2 0.69 Neutrophil/ lymphocyte ratio 1.99 (1.47-2.73) 2 (1.54-2.91) 0.43
TC, mg/dL 169.9 34.2 172.4 31.6 0.53
Triglyceride, mg/dL 118 (86-170) 116.5 (83-181.25) 0.86
HDL-C, mg/dL 47 (37.5-54.5) 47 (41-56) 0.54
LDL-C, mg/dL 108.0 30.2 109.7 30.3 0.63
Colony-forming units, /1×106 PBMCs
21 (10.75-38) 19 (8-39) 0.64
KDR+CD34+ count, cells/L 0.07 (0.03-0.21) 0.08 (0.04-0.16) 0.83 CD146+annexin V+ count,
cells/L
0.02 (0.01-0.05) 0.03 (0.01-0.06) 0.26 BrDU incorporation, absorbance
value at 450 nm
0.72 (0.52-1.07) 0.75 (0.56-1.19) 0.74 XTT, absorbance value at 450 nm 2.2 0.8 2.1 0.8 0.26 Nucleosome fragmentation, fold 0.87 (0.57-1.38) 0.80 (0.49-1.22) 0.27 Migrated cells, /field 95.5 (48.25-169) 78 (48.25-117.25) 0.32 PCSK9, ng/mL 296.45 (162.33-413.7) 259.4 (152.1-334.3) 0.03
BrDU, bromodeoxyuridine; HDL, high-density lipoprotein; KDR, kinase insert domain receptor; LDL, low- density lipoprotein; PBMC, peripheral blood mononuclear cell; PCSK9, protein complex proprotein convertase subtilisin/kexin type 9.
Numerical values are expressed as mean standard deviation or median (interquartile range), as appropriate.
(九) 表三
Table 3. Changes in parameters between patients in the cilostazol treatment and placebo groups Changes in parametersa
Cilostazol group (n = 134)
Placebo group (n = 132)
P value
Fasting plasma glucose 2.5 (-7~10.75) 1 (-6.75~6) 0.31
Hemoglobin A1C 0 (-0.2~0.2) 0 (-0.1~0.2) 0.86
Body weight 0.2 (-1.4~1.5) 0.35 (-1.03~1.7) 0.67
Waist circumference 0.5 (-1.5~2.5) 0.5 (-1.28~2) 0.78
Body mass index 0.04 (-0.51~0.61) 0.13 (-0.42~0.65) 0.65 Blood pressure
Systolic -2.42 14.27 -1.61 15.66 0.69
Diastolic 0 (-8~6) 0 (-6~6.5) 0.82
Heart rate 3.5 (-1.5~10) c 0 (-4~4) 0.03
White blood cell count -0.1 (-1.0~0.6) 0.1 (-0.6~0.8) 0.22
Hemoglobin -0.1 (-0.6~0.55) 0 (-0.5~0.5) 0.55
Platelet count 11 (-3.5~25) c 3 (-13~15) 0.001
TC -0.5 (-12~13.75) 1 (-15.5~12.25) 0.58
Triglyceride -11.5 (-35.5~11.75) c -1.5 (-29.25~25) 0.03
HDL-C 2 (-2~6) c 1 (-3~5) 0.15
LDL-C 0 (-13~12.75) -1 (-12~11.25) 0.35
Colony-forming units 2.5 (-16.5~21) 3.5 (-16.75~18.25) 0.88 KDR+CD34+ cells 0.06 (-0.01~0.32) c 0.03 (-0.04~0.13) c 0.03 CD146+annexin V+ cells 0.02 (-0.01~0.06) c 0 (-0.02~0.03) 0.04 BrDU incorporation -0.03 (-0.38~0.2) -0.01 (-0.34~0.28) 0.62 XTT absorbance -0.01 (-0.65~0.52) 0.02 (-0.58~0.89) 0.34
Nucleosome fragmentation -0.05 0.81 0.13 0.94 0.13
Migrated cells -26.2 74.96 b -2.93 54.13 0.07
PCSK9 -46.25 (-
174.2~38.19)c
0.48 (-67.59~81.79) <0.001 Abbreviations as shown in Table 2.
aChanges in parameters = (post-treatment value – baseline value) / baseline value × 100%. Values are expressed as mean standard deviation, number (%), or median (interquartile range), as appropriate.
bP < 0.05 vs. baseline. cP < 0.01 vs. baseline.
14
(十) 表四
Table 4. The association of baseline characteristics and changes in plasma levels of PCSK9 in the entire cohort
Changes in PCSK9 levelsa P value In patients with history of In patients without history of
Male gender -18.1 (-105.8~58.66) -1.9 (-155.12~64.85) 0.90 Underlying disease
Diabetes mellitus -32.35 (-167.5~54.26) -0.05 (-97.44~63.2) 0.06 Hypertension -7.31 (-121.38~60.8) -11.75 (-102.05~58.47) 0.85 Hyperlipidemia -5.7 (-119.1~60.7) -27.7 (-122.5~57.14) 0.51 Metabolic syndrome -4.65 (-128.2~54.4) -11.75 (-97.02~64.9) 0.51 Tobacco smoking 0 (-48.87~55.02) -12.5 (-129.83~63.4) 0.25
PAD -42.24 (-144.08~50.43) -3.85 (-108.89~61) 0.30
CAD -8.61 (-104.98~56.53) -21.3 (-148.9~63.18) 0.49
Myocardial infarction -4.56 (-133.85~50.45) -12.45 (-113.36~63.6) 0.57 Cerebrovascular accident -37.25 (-106.01~33.1) -8.61 (-119.45~60.8) 0.86 Chronic kidney disease -0.19 (-130.76~54.7) -14.9 (-119.1~60.7) 0.79 Aspirin use -8.61 (-111.15~60.14) -12.95 (-124~59.9) 0.60 Clopidogrel use -11 (-75.5~80.5) -8.92 (-121~57.5) 0.47
CCB use -18.1 (-126.1~50.58) -2.5 (-108.5~63) 0.57
Diuretic use 0.2 (-152.1~69.19) -12.5 (-113.8~55.3) 0.57 Statin use -13.9 (-120.5~70.18) -4.1 (-114.8~56.2) 0.72 Abbreviations as shown in Table 1.
aChanges in parameters = (post-treatment value – baseline value) / baseline value × 100%. Values are expressed as mean standard deviation.
(十一) 表五
Table 5. Correlation between changes in PCSK9 levels and significant changes of parameters in the entire cohort
Changes in PCSK9 levels
r* P value
Changes in TC -0.15 0.02
Changes in TG 0.14 0.03
Changes in LDL -0.21 0.002
Abbreviations as shown in Table 2. *r values are expressed as the Spearman's rank correlation coefficient (Spearman's rho).
16
(十二) 表六
Table 6. Independent predictors of changes in plasma levels of PCSK9 by multivariable linear regression analysis in the entire cohort
Changes in PCSK9 levels
Beta (95% CI) P value
Cilostazol use -56.97 (-99.50, -14.44) 0.009
Changes in TC -1.09 (-1.82, -0.36) 0.004
Changes in triglyceride 0.61 (0.39, 0.84) <0.001
CI, confidence interval. Other abbreviations as shown in Table 2.
(十三) 表七
Table 7. Clinical outcome endpoints (intention-to-treat analysis)
Outcome Cilostazol
n = 134
Placebo n = 132
Hazard ratio (95% CI)
P Value
No. of patients (%) MACE: CV death, nonfatal MI,
nonfatal stroke, CHF, or unplanned coronary revascularization
14 (10.4) 20 (15.2) 0.67 (0.34-1.33) 0.25
MCE: MI, angina pectoris, or unplanned coronary revascularization
8 (6.0) 20 (15.2) 0.38 (0.17-0.86) 0.02
MACCE: CV death, nonfatal MI, nonfatal stroke, CHF, major amputation, minor amputation, or unplanned coronary revascularization
11 (8.2) 22 (16.7) 0.47 (0.23-0.96) 0.04
Other endpoints
CV death 2 (1.5) 2 (1.5) 0.99 (0.14-7.00) 0.99
Sudden death
Death from any cause
2 (1.5) 1 (0.8) 1.97 (0.18-21.72) 0.58 5 (3.7) 6 (4.5) 0.82 (0.25-2.69) 0.75
MI 1 (0.7) 4 (3.0) 0.23 (0.03-2.09) 0.19
Nonfatal MI 1 (0.7) 4 (3.0) 0.23 (0.03-2.09) 0.19
Stroke 5 (3.7) 5 (3.8) 0.93 (0.27-3.23) 0.91
Nonfatal stroke 5 (3.7) 5 (3.8) 0.93 (0.27-3.23) 0.91 Hospitalization for CHF 3 (2.2) 7 (5.3) 0.42 (0.11-1.62) 0.21 Cardiogenic shock 0 2 (1.5) 0.02 (0-1363.67) 0.47 Angina pectoris 8 (6.0) 20 (15.2) 0.38 (0.17-0.86) 0.02 Unplanned coronary
revascularization
5 (3.7) 8 (6.1) 0.60 (0.20-1.83) 0.37 Unplanned
revascularization
1 (0.7) 7 (5.3) 0.13 (0.02-1.09) 0.06
Major amputation 0 0
Minor amputation 0 0
CHF, congestive heart failure; CI, confidence interval; CV, cardiovascular; ITT, intention-to-treat;
MACCE, major adverse cardiovascular and cerebrovascular event; MACE, major adverse cardiovascular event; MCE, major coronary event; MI, myocardial infarction.
18
(十四) 表八及表九
Table 8. Uni- and multi-variables independently predicting major coronary events
Variables Uni-variables
HR (95% CI)
P Multi-variables HR (95% CI)
P
Cilostazol use 0.38 (0.17-0.86) 0.02 0.34 (0.15-0.78) 0.01
Age 1.01 (0.97-1.05) 0.56 - -
Peripheral artery disease 0.89 (0.32-2.48) 0.82 - -
Coronary bypass surgery 0.05 (0-10296.19) 0.63 - -
Anemia 0.93 (0.37-2.31) 0.88 - -
Aspirin use 2.52 (0.96-6.63) 0.06 2.88 (1.09-7.61) 0.03
Table 9. Uni- and multi-variables independently predicting major adverse cardiovascular and cerebrovascular events
Variables Uni-variables
HR (95% CI)
P Multi-variables HR (95% CI)
P
Cilostazol use 0.47 (0.23-0.96) 0.04 0.48 (0.23-1.02) 0.055
Age 1.07 (1.02-1.11) 0.002 1.07 (1.02-1.11) 0.003
Peripheral artery disease 1.84 (0.84-4.02) 0.13 - -
Coronary bypass surgery 1.86 (0.25-13.76) 0.54 - -
Anemia 2.27 (1.09-4.71) 0.03 - NS
Aspirin use 0.88 (0.44-1.79) 0.73 - -
(十五) 圖一
Figure 1. The schematic participants flow and allocation for assignment
107年度專題研究計畫成果彙整表
計畫主持人:趙庭興 計畫編號:107-2314-B-006-076-MY2
計畫名稱:Cilostazol對於血中PCSK9濃度之影響與改變血管內皮前驅細胞數目和功能以及血管新生 因子效應之關聯性
成果項目 量化 單位
質化
(說明:各成果項目請附佐證資料或細 項說明,如期刊名稱、年份、卷期、起 訖頁數、證號...等)
國
內 學術性論文 期刊論文 7 篇
1. Li YH, Chao TH, Liu PY, Ueng KC, Yeh HI. Lipid Lowering Therapy for Acute Coronary Syndrome and
Coronary Artery Disease: Highlights of the 2017 Taiwan Lipid Guidelines for High Risk Patients. Acta
Cardiol Sin 2018;34:371-378. (SCI) 2. *Chao TH, Hsiao PJ, Liu ME, Wu CJ, Chiang FT, Chen ZC, Chen CP, Yeh HI, Lee TH, Chiang CE. A sub- analysis of Taiwanese patients from ODYSSEY South Korea and Taiwan study (ODYSSEY KT) evaluating the efficacy and safety of alirocumab in high cardiovascular risk
patients with hypercholesterolemia.
J Chin Med Assoc 2019
Apr;82(4):265-271. (*corresponding author) (SCI)
3. HH, Wang PC, Yeh EH, Lin CJ,
*Chao TH. Impact of disease- specific care certification on clinical outcome and healthcare performance of myocardial
infarction in Taiwan. J Chin Med Assoc 2020 Feb;83(2):156-163.
(*corresponding author) (SCI) 4. Wang PY, Liu PY, Hsu CH, *Chao TH. Implementation of clinical decision support system to promote prescription of guideline-directed medical treatment drugs for
congestive heart failure.
Healthcare Qual 2020
(*corresponding author) (in press).
5. Su CY, *Chao TH. The anti- hypertensive effect of sodium- glucose cotransporter 2 inhibitors.
J Intern Med ROC 2020
(*corresponding author) (in press).
6. Chiang CE, Ueng KC, Chao TH, et al. 2020 Consensus of Taiwan
Society of Cardiology on the
pharmacological management of patients with type 2 diabetes and cardiovascular diseases. J Chin Med Assoc 2020 Jul;83(7):587-621. (SCI) 7. Cheng CY, *Chao TH. The lower the better for low-density
lipoprotein cholesterol lowering. J Intern Med ROC 2020 (*corresponding author) (submitted)
研討會論文 0
專書 0 本
專書論文 0 章
技術報告 0 篇
其他 0 篇
國
外 學術性論文
期刊論文 3
篇
1. Wang KC, Chen PS, Chao TH, Luo CY, Chung HC, Tseng SY, Huang TY, Lin YL, Shi GY, Wu HL, Li YH. The role of vascular smooth muscle cell membrane-bound thrombomodulin in neointima formation.
Atherosclerosis 2019 Aug;287:54-63.
(SCI)
2. Tseng SY, Chang HY, Li YH, *Chao TH. Cilostazol improves
hyperglycemia-induced impaired vasculo-angiogenesis through
stimulating adiponectin/adiponectin receptor 1/sirtuin 1 signaling pathway. Clin Sci (*corresponding author) (submitted) (SCI)
3. *Chao TH, Tseng SY, Liu PY, Li YH. A randomized controlled trial evaluating outcome impact of cilostazol in patients with coronary artery disease and at a high risk of cardiovascular disease. J Am Heart Assoc
(*corresponding author) (submitted) (SCI)
研討會論文 7
1. Chao TH, Li YH, Tseng SY, Liu PY. The associations between the effect of cilostazol on the proprotein convertase
subtilisin/kexin type 9
concentrations and circulating endothelial progenitor cells and vasculo-angiogenesis factors. Eur Heart J 2018;39(suppl):523.
2. Chao TH, Lee CH, Huang YL, Liu