行政院國家科學委員會專題研究計畫 成果報告
子計畫(四):身心障礙者家庭自動化系統之臨床功能評估與 輔助裝具設計
計畫類別: 整合型計畫
計畫編號: NSC91-2614-E-006-002-
執行期間: 91 年 08 月 01 日至 92 年 07 月 31 日 執行單位: 國立成功大學職能治療學系
計畫主持人: 張哲豪
計畫參與人員: 共同主持人: 陳若佟 國立成大醫院復健科主治醫師
報告類型: 精簡報告
處理方式: 本計畫涉及專利或其他智慧財產權,1 年後可公開查詢
中 華 民 國 92 年 10 月 16 日
行政院國家科學委員會補助專題研究計畫成果報 告
※ ※※※※※※※※※※※※※※※※※※※※※
※※※ 身心障礙者家庭自動化系統的研製評估訓練---子計
畫 四 : ※ ※ 身 心 障 礙 者 家 庭 自 動 化 系 統 之
※ ※ 臨 床 功 能 評 估 與 輔 助 裝 具 設 計 (III)
※※ Clinical Evaluation and Orthosis Design of Assistive Home ※ ※ Automata System for Persons with Disabilities(III) ※※※※※※※※※※※※※※※
※※※※※※※※※※※
計畫類別:□個別型計畫 v 整合型計畫 計畫編號:NSC91-2614-E-006-002
執行期間:91 年 08 月 01 日至 92 年 07 月 31 日
計畫主持人:
張哲豪 國立成功大學職能治療系講 師
共同主持人:
陳若佟 國立成大醫院復健科主治醫
師
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:成功大學職能治療學系
中 華 民 國 92 年 10 月 15 日
行政院國家科學委員會專題研究計畫成果報告
身心障礙者家庭自動化系統的研製評估訓練---子計畫四:
身心障礙者家庭自動化之臨床功能評估與輔助裝具設計(III) Clinical Evaluation and Orthosis Design of Assistive
Home Automata System for Persons with Disabilities(III) 計畫編號:NSC 91-2614-E-006-002
執行期限:91 年 08 月 01 日至 92 年 07 月 31 日
主持人:張哲豪 國立成功大學職能治療系講師 E-mail: jerhao@mail.ncku.edu.tw
共同主持人:陳若佟 國立成大醫院復健科主治醫師
中文摘要
身心障礙者囿於先後天疾病或傷害導致部份肢體功能無法發揮,影響日常生 活甚鉅。藉由家庭自動化系統之開發與研製,配合電腦科技之應用即能協助身心 障礙者操作各項家電用品,進行種種日常生活活動。然而各種類身心障礙者的臨 床病理與功能障礙實有不同的特色及程度差異,故需要職能治療師與復健醫師的 臨床評估,以瞭解各個案的實際能力與可供訓練之方向與潛力,再配合選用適當 之家庭自動化系統。若個案的肢體另須穿戴特殊之輔助裝具(assistive orthosis),
亦可由職能治療師設計製造之,再配合使用操控家庭自動化系統。故本計畫旨在 搭配其它子計畫之家庭自動化系統,提供案主之生理職能評估與個別輔具設計,
以檢驗身心障礙者使用家庭自動化系統後所改善之日常生活功能與活動。
職能治療以協助各類身心障礙者發揮潛能達成日常生活之各種職能表現
(occupational performance)為目標,透過職能評估並尋求適當輔助裝具及訓練 與治療,讓身心障礙者發揮最大的生活功能。本計劃採用質性探究與量化評估的 方法為各類身心障礙者提供最適切的職能評估與分析,以作為設計相關輔具及檢 驗輔具效能之參考。
關鍵詞:身心障礙者、家庭自動化、輔助科技、職能評估、裝具設計
Abstract
People with disability are handicapped by their dysfunction in daily activities.
Nowadays, assistive home automata (AHA) are developed to help them control household appliances and regain independent life. To reach the maximal efficacy of AHA application depends on the need and the residual capability of the individual client. A precise clinical evaluation of rehabilitation can reveal the limitation, ability, as well as potentials of the disabled clients. The information can helpfully match the clients with the proper AHA to optimal operation efficiency. In addition, the design and fabrication of the necessary orthoses can also play a key role in bridging the gap between the clients and the automata. This study reports several case examples to demonstrate the application of assistive home automata by clinical evaluation and orthosis design.
An intellectual wireless remote control system with Consumer Electronics Bus (CEBus) module was adopted to connect the household appliances as assistive the AHA system. A radio-frequency (RF) transmitter with large button panel and Morse code input system was manufactured as operation interface. The performance components of the disabled clients included neuromuscular function, integration of sensation and perception, cognitive function, activity of daily living, as well as psychosocial function and were concisely evaluated. Two clients with cerebral palsy (CP) had problems in touching the button of the remote control. One was evaluated to have fine control of his head and neck and thus a head stick was customized for him to press buttons. The other one with ataxic movement can not point by fingers and was taught to grasp a foam cone to perform button-pushing. One young adult with high level spinal cord injury was evaluated to have strong needs and potentials to operate AHA by Morse code input system. A customized mouth switch device was designed and fabricated for him to input Morse code to control the household appliances.
An infrared module was integrated into the AHA system to drive some household appliances with infrared frequency. The CP client using head stick to press the large buttons in control panel can immediately master the AHA system after several practices. He can easily operate the television, light, and fan in his room. The other CP client also can use the foam cone to control the AHA system very efficiently and even learned to type with better speed and accuracy by the device. The SCI client is ventilator- dependent and bed-ridden for over four years. He felt deeply sad to be non-functional till applying the AHA system. He becomes very active to use his mouth device and input Morse code to control television, air condition, and light twinkling to call his attendant. Moreover, he can use the input system to key in 43 alphabets per minute to computer. Now he can surf the website to explore the world
and design homepage to earn some stipend. He really regains his new life.
This study demonstrates the powerful evidence to integrate clinical evaluation and orthosis design for applying AHA to the optimal enhancement. The results are expected to be a model reference for the home automation system devices in the future design.
Keywords: disabilities, home automation, assistive technology, occupational evaluation, orthosis design
INTRODUCTION
Home electric equipment plays an important role in daily life to everyone while the advanced technology strides forward the 21st century. With the variety of electrical products, such as televisions, electric fans, electric lights, air conditionings, computers, etc, most people can enjoy the convenient and high quality modern life easily. People with disabilities are handicapped in their daily activities by the congenital or acquired dysfunction, especially when there has no proper interfaces for them to manipulate the home facilities. Nowadays, assistive technology (AT) has provided consumers to compensate their impairment and perform functional tasks based on their needs and desired roles. In this paper, three cases (two with cerebral palsy and one with spinal cord injury) demonstrated that customized environmental control system (ECS) developed by AT made their life more convenient and also enriched their spirit with more dignity.
The Human Activity Assistive Technology (HAAT) Model (Cook & Hussey, 1995), widely used by AT practioners, explains the interrelationship between human and non-human elements. In this model, human refers to an individual attempting to engage in activity. The AT portion includes four sections: the human-technology interface, processor, activity output, and environmental interface. The human-technology interface is the contact between the person and the technology device. The processor, the mechanical or electrical linkage, relays or interprets information from the interface. The activity output includes actions such as opening doors and printing a page of text. The environmental interface adjusts the output of the device in response to input from the environment. The HAAT Model shows that assistive technology can link the person and the activity and make the activity possible. Removing the assistive technology may restrict the person from performing the activity. The contribution made by a well-chosen and fully used AT device is remarkable.
As science and technology changed with each passing day, they made human life more convenient and comfortable. However, most disable people are unable to enjoy the advantages of technology and civilization adequately. Because the technological
products stress on capital benefit, they can’t actually conform to all needs for the disable individuals. Therefore, the disable might not deserve benefits and then depend on others’ assistance to live with dependency. We can infer that it would be a burden for social capital and human resources. In order to integrate modern technology with ideas of serving the disable, the research team particularly designs a set of domestic automation system which is also called environmental control system. It makes use of promoting living quality of disabilities and enhances the independent abilities of their daily lives. Meanwhile it also helps to reduce the burdens of the disable clients and their families through the concerns of technology and humanities.
Environmental control system
Environmental control systems are made up by environmental control units (ECUs). ECUs provide a way for persons with severe disabilities to participate in life activities that would otherwise not be possible, giving them greater independence and enhanced quality of life (Garrison, 1982; Vanderheiden, 1982). ECUs consist of a control interface or input device (e.g., keyboard, joystick, switch, voice activator) and a feedback display that reflects the action being controlled (Cook & Hussey, 1995).
The disable clients can use ECUs easily through controlling switches or computers and obtain their communicative function. Thus, they can interact with external environment well. The ECS emphasizes on the individual design and can facilitate the disable to get the maximal independence in their daily living. To customize ECS should consider the environmental conditions where the clients live in and all aspects of their physical and psychosocial status. The security of the systems is the most important point to respect.
CASE ONE
Clinical evaluation
The client with cerebral palsy (CP) and his family were invited to participate in our study. The client usually stays in prone position in bed as his most comfortable posture and moderately depends on his family in the daily life. Though he may sometimes sit in a wheel chair, his abnormal muscle tone would increase and he may slide down easily with poor trunk control. He never went to school, but he could use his chin to operate the computer system with an enlarged track ball at home. All the knowledge about operate the computer was taught by his family, including using internet that making fun in his life. Expect to visit the website, client showed great interests in watching television and listening to the radio but he had trouble to use these equipments by his own.
To improve the client functional performance, occupational therapists firstly
evaluated his motor ability and maximize the residual capability to meet his needs.
His muscle tone evaluation was described as table 1.
Table 1. Muscle tone of Case 1
Muscle Tone Muscle Tone
Head & Neck Slight spasticity Right Hand Moderate flexor spasticity Trunk Extensor spasticity Left Leg Moderate flexor spasticity Left Arm Moderate flexor spasticity
and shoulder retraction
Right Leg Moderate flexor spasticity Right Arm Moderate flexor spasticity
and shoulder retraction
Left Foot Severe flexor spasticity Left Hand Moderate flexor spasticity Right Foot Severe flexor spasticity Approach and orthosis design
As the client could use the computer system with his chin, we designed a chin touch bottom (Figure 1.) connected with ECS and Morse code control system to let him input signals. The system also helps him possible to control the fans, television, and light by himself. Besides, we also designed an assistive wedge to provide him a proper positioning in prone.
Figure 1. The chin touch bottom
Results
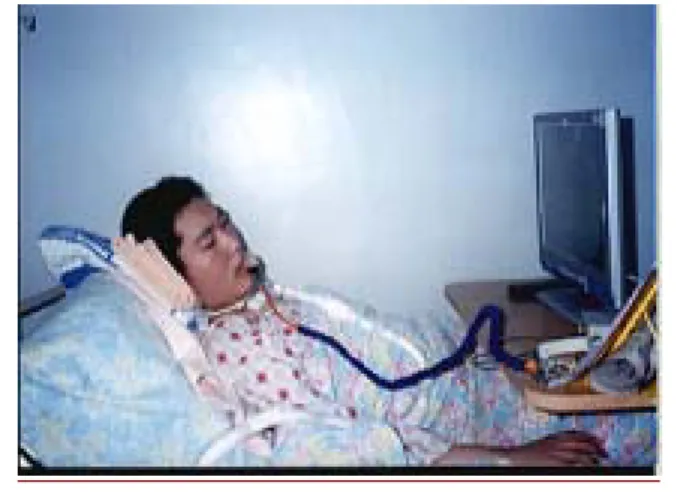
After several practice, he now can easily operate the television, fans, and light in his own room. He can also learn to type with better speed and accuracy by the device (Figure 2).
Figure 2. Case 1 used the chin touch bottom to operate his computer.
CASE TWO
Clinical evaluation
This client with CP and ataxic movement lives with his family and totally depended on them. To interact with the environment and other people, he could only show his agreement or disagreement to his family with laughing or making sounds to let them know his needs. Most of his usual time, he stayed in front of the television and watched the program his family set for him.
His muscle tone status is listed as the following table (Table 2). The low postural tone and flexor spasticity of his limbs limited his function in daily living though he has little cognitive ability. Besides, the client could make hands grasp and release but have no individual finger movement to point.
Table 2. Muscle tone of Case 2 Muscle Tone Muscle Tone
Head &
Neck
Hypotonia Right Hand
Flexor spasticity Trunk Low postural
tone
Left Leg
Moderate extensor spasticity Left
Arm
Mild spasticity
Right Leg
Moderate extensor spasticity Right
Arm
Mild spasticity
Left Foot
Moderate spasticity Left
Hand
Flexor spasticity
Right Foot
Moderate spasticity Approach and orthosis design
According to his interest and needs, his family wished he could turn on/off the television and choose the channel by himself and even control the fans and light without anyone’s assistance. Therefore, we considerate two factors that might affect
his functional performance. One was his residual strength, the right hand; the other was the size of bottom which he may hit with his fist. When the ordinary size bottom was not suitable for him, we designed a remote control panel with large bottoms (5-cm diameter) of necessary functions (Figure 3).
Figure 3. A remote control panel with large bottoms
Results
After practice, he can operate the system efficiently to control the television, fans, and the light in his own chair (Figure 4).
Figure 4. Case 2 operates his ECS
CASE THREE
Clinical evaluation
The client has strong needs for using automatic control systems at home. Four years ago, he dived into the swimming pool and suffered from an athletic accident.
His head hit on the ground directly and sustained a C4 to C6 spinal cord injury. The client was bedridden due to his quadriplegia and then induced the spinal nerves to atrophy. All of his C1 to C6 spinal cord were influenced. The client has clear consciousness and intact cognitive function, but he is respiratory-dependent.
We evaluated this client’s sensorimotor status by sensation test and manual
muscle testing and described the result as the following table (Table 3).
Table 3. Sensation and Motor Status of Case 3 Test of Sensation Motor Evaluation
Light Touch Left Right Manual Muscle Test Left Right C1 Intact Intact Muscles of the face N N C2 Impaired Impaired Muscles of mouth/lips N N C3 Impaired Impaired Muscles of the TM joint P T
C4 Impaired Impaired Capital flexors N N
C5 Absent Absent Cervical flexors P T
C6 Absent Absent Cervical extensors Z Z
N:normal P:poor T:Trace Z:Zero
Approach and orthosis design
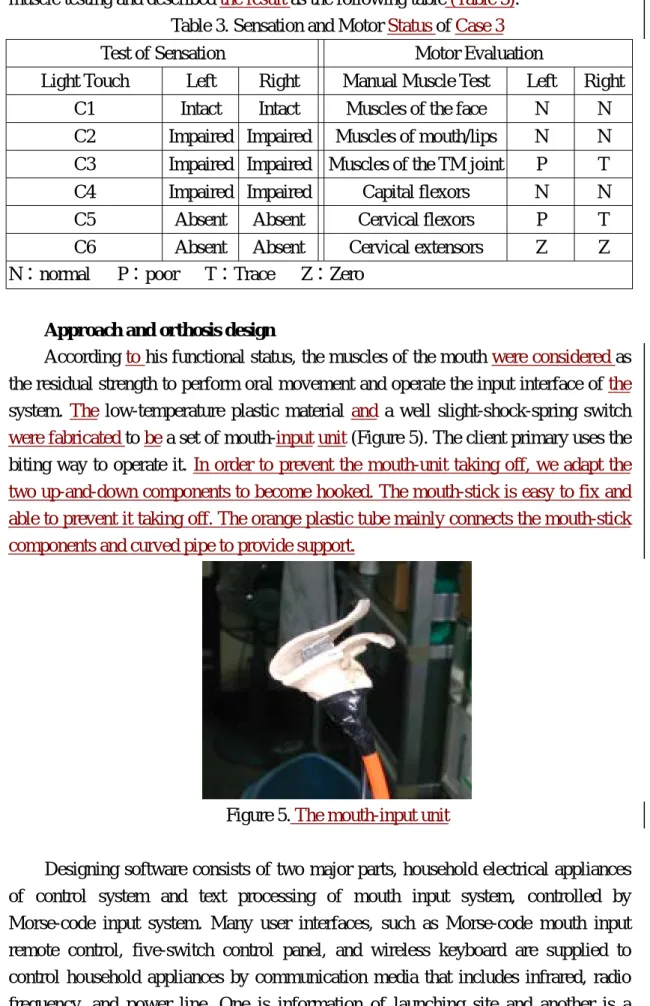
According to his functional status, the muscles of the mouth were considered as the residual strength to perform oral movement and operate the input interface of the system. The low-temperature plastic material and a well slight-shock-spring switch were fabricated to be a set of mouth-input unit (Figure 5). The client primary uses the biting way to operate it. In order to prevent the mouth-unit taking off, we adapt the two up-and-down components to become hooked. The mouth-stick is easy to fix and able to prevent it taking off. The orange plastic tube mainly connects the mouth-stick components and curved pipe to provide support.
Figure 5. The mouth-input unit
Designing software consists of two major parts, household electrical appliances of control system and text processing of mouth input system, controlled by Morse-code input system. Many user interfaces, such as Morse-code mouth input remote control, five-switch control panel, and wireless keyboard are supplied to control household appliances by communication media that includes infrared, radio frequency, and power line. One is information of launching site and another is a
wireless information receiver. The information of launching site uses the wires to connect the oral input system and wireless electronic information of launching site.
The wireless information receiver connects with the household electrical appliances and is able to receive the information from launching site. Thus, operating in the Morse codes and oral input system, the client can operate the electrical appliances easily.
Results
Through several practice, he can control electric equipments (electric fan and desk lamp) by himself at will. He also retained the ability to use computer and was able to deal with text processing (Figure 6). He input 26 English letters A to Z and only spent 55 seconds; when he typed English short essay, he could type about 4.7 words per minute (about 24 letters); when he typed Chinese short essay, he could type about 5 words per minute in the training period. Besides, he could surf the website to explore the world and communicate with people. Now he can write or answer e-mail to anyone at anytime easily and design homepage to earn some stipend. The ECUs not only increases the living independence but also promotes the living quality. This client really retains his competence and confidence, and restarts the new life.
Figure 6. Case 3 use mouth-unit to operate computer
CONCLUSION
In this study, clinical evaluation and AT devices provided clients to maximize the capability using ECUs to make their life better. Occupational therapists will always pay attention for the current technology which brings more convenient for human being. Though the main role of the occupational therapist is to treat people as they are, there should be widely noticed that what makes people live easier also helps the disabled people enjoy their life while the scientific view grows up. Treatment planning required the involvement of clients’ residual strength and the psychosocial factors including their interests and favorite life styles. This study provided powerful
evidence to integrate the ECUs and proper clinical approach into their life and satisfied these clients with more dignity and convenience. Besides, the burden of their family was also decreased while the clients showed great improvement in controlling their own living place. The results are expected to be taken a broad look at the using of ECUs and to be a model reference for the design in the future.
REFERENCES
1. Angelo, J., & Buning, M. E. (2002). High-Technology Adapations to Compensate for Disability Catherine A. Trombly, Mary Vining Radomski. (Eds.) Occupational Therapy for Physical Dysfunction (pp.389-417) Baltimore:Lippincott Williams & Wilkins.
2. Bain, B.K. (1998). Assistive technology in occupational therapy. In M.E.
Neistadt(Eds), Willard & Spackman’s occupational therapy (9th ed.), pp.498-317.
New York: Lippincott.
3. Barnes, M. P. (1994). Switching devices and independence of disable people.
BMJ, 309:1181-1182
4. Christiansen, C., & Baum, C. (1997). Occupational therapy: Enableing function and well being. (2nd ed.). Thorofare, NJ: Slack.
5. Cook, A. M., Hussey, S. M. (1995). Assistive technology: Principles and practice. Baltimore: Mosby.
6. Cook, A. M., Hussey, S. M. (1996). Electonic assistive technology in occupational therapy practice. In L. M. Pedretti (Ed.), Occupational therapy: Practice skills for physical dysfunction. Baltimore: Mosby.
7. Holm, M. B., Rogers, J. C., & Stone, R. G. (1998). Person-Task-Environmrnt interventions: A decision-making-guide. In M.E. Neistadt(Eds), Willard &
Spackman’s occupational therapy (9th ed.), pp.498-317. New York: Lippincott.
8. Lamport, N. K., Coffey, M. S., & Hersch, G. I. (1993). Activity analysis handbook (2nd ed.). Thorofare, NJ: Slack.
9. Lienden, C. A., & Trombly, C. A. (1995). Orthoses: Kinds and purposes. In C.
C. Trombly (Eds.), Occupational therapy for physical dysfunction (4th ed.), pp.
551-581. Baltimore: Williams & Wilkins.
10. Mann, W. C., & Lane, J. P. (1995). Assistive technology for persons with disabilities (2nd ed.). Bethesda, Md : The American Occupational Therapy Association.
11. Wellings, D. J., & Unsworth, J. (1997). Environmental control systems for people with a disability: an update. BMJ, 315:409-412.
SELF COMMENTS
This study played an important role in the whole package project by providing clinical evaluation and assistive orthosis for the subjects in other subprojects. This subproject had reached the aims to support the whole package project and also examine the efficacy of the home automation system devices developed by other subprojects through our trans-disciplines team work and regular meetings.
The components of occupational performance for the people with disabilities were well evaluated. Those components included: neuromuscular function, integration of sensation and perception, cognitive function, activity of daily living, and psychosocial function. This project used not only qualitative method but also quantitative data to evaluate and analyze the occupational performance of the disable subjects. The study applied the assistive home automata to the matched subjects based on the evaluation results. Besides, the researchers customized the orthoses to fit the whole system and the subjects to their best function and kept following-up for their improving performance. Although there were not so many subject-candidates as our previous expectation, these outstanding achievements of our subjects with the assistive systems still could be a model in the application of assistive technology.
These case reports were presented in “World Congress on Medical Physics and Biomedical Engineering” at Sydney on 28 August 2003 and will be prepared to summit for publication.