Introduction
Hypoalbuminemia can be attributed to condi- tions of ( 1) decreased synthesis such as poor protein intake or liver disease, or ( 2) excessive protein loss.
Excessive protein loss generally occurs because of
nephrotic syndrome or protein-losing enteropathies (PLE). There are numerous conditions associated with gastrointestinal loss of proteins, among which the most common are congestive heart failure, in- testinal lymphangiectasia, lymphoma, specific small- and large-bowel enteropathies, abdominal tuberculo-
Correspondence and requests for reprints : Dr. Li-Che Lu
Address : Division of Nephrology, Department of Internal Medicine, Shin-Kong Wu Ho-Su Memorial Hospital; 95, Wen-Chang Rd, Shih-Lin, Taipei 111, Taiwan.
Nephrotic Syndrome and Protein-Losing Enteropathy in A Patient with Suspected
Systemic Lupus Erythematosus A Case Report
Chung-Hsin Chang, Li-Che Lu, Shou-Shan Chiang, and An-Hang Yang
1Abstract
We report a 57-year-old female patient with suspected systemic lupus erythematosus presented with general anasarca, pleural effusions, hypercholesterolemia and severe hypoalbuminemia. First, nephrotic-range proteinuria was revealed and membranous glomerulonephritis was diagnosed and suc- cessfully treated. She developed diarrhea 2 years later with similar clinical presentations but this time no proteinuria was found. Primary protein-losing enteropthy, a rare complication of systemic lupus ery- thematosus, was diagnosed after other causes of gastrointestinal protein loss were excluded. Complete remission was achieved with steroid therapy. This case is unusual by the presentation of the same cli- nical pictures with different etiologies. Hypoalbuminemia and general anasarca need further investi- gation if renal protein loss was not found. ( J Intern Med Taiwan 2005; 16: 139-145 )
Key Words Systemic lupus erythematosus, Hypoalbuminemia, Hypercholesterolemia, Nephrotic syndrome, Protein-losing enteropthy
Division of Nephrology, Department of Internal Medicine, Shin-Kong Wu Ho-Su Memorial Hosipital
and
1Department of Pathology, Veterans General Hospital-Taipei, Taipei, Taiwan
sis and retroperitoneal tumors
1.
Gastrointestinal manifestations of systemic lu- pus erythematosus (SLE) are uncommon. Recently, it has been reported that SLE can be a cause of pro- tein-losing enteropthy
2-4. This association is rare with a total about 20 cases having been reported in the English literature. Here we report another case of PLE associated with SLE, besides, this case is unusual by the preceding similar clinical manifestation of hy- poalbuminemia due to class V lupus nephritis.
Case Report
A 57-year-old woman was first admitted to Shin Kong Wu Ho-Su Memorial Hospital in January 1997 because of generalized edema, exertional dyspnea and malaise for 1 week. Three months prior to ad- mission, the patient gradually experienced puffy eye- lids, abdominal fullness and general weakness. She had no history of fever, arthralgia or skin rashes. On admission, moderate bilateral pretibial edema and puffy eyelids were noted and her blood pressure was 130/70 mmHg, pulse rate 90/min with regular rhythm, and temperature 36.6 . Urinalysis showed 3+ protein with insignificant sediment. The 24-hour urine protein was 3870 mg. Hemoglobin was 12.1gm/dl, white blood cell count was 4500/mm
3with normal classification, platelet count was 297000/
mm
3and bleeding time (Duke) was 1 minute. Blood urea nitrogen (BUN) was 9 mg/dl, serum creatinine (Cr) was 1.0 mg/dl, serum albumin 1.6 gm/dl, glo- bulin 2.8 gm/dl, total cholesterol 267 mg/dl, trigly- ceride 281 mg/dl, AST 30 U/L and ALT 12 U/L.
Creatinine clearance was 77 ml/min. The serum com- plements were within normal range and the tests for antinuclear antibody (ANA), anti-DNA antibody, an- ti-HCV antibody and HBs antigen were negative. A chest X-ray showed pulmonary infiltration and mo- derate right pleural effusion, but the heart was nor- mal. Renal ultrasonagraphy showed normal renal size (right 10.6cm, left 12.2cm) with smooth surface and slightly hyperechoic cortex.
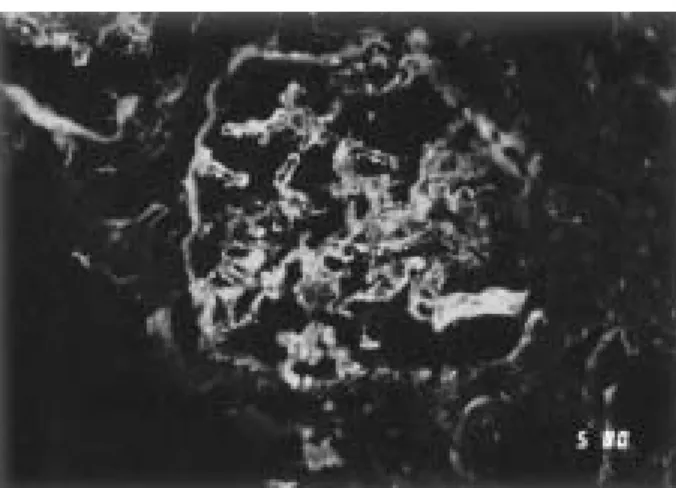
Renal biopsy was performed on the fifth day of admission. Light microscopy revealed membranous glomerulonephritis. Immunofluorescent examina- tion revealed diffuse global granular IgG deposition in capillary wall and mesangium ( Fig.1 ) and trace focal segmental granular deposition of IgM, IgA, C1q, C3, C4 in mesangium. Electron microscopy showed global effacement of foot process, scattered Fig. 1. Renal biopsy. Immunofluorescence microscopy revealed IgG deposits along the glomerular capil- lary walls, mainly subepithelial, and in the mesangium (x 250).
Fig. 2. Renal biopsy. Electron microscopy showed global
effacement of foot process, scattered deposition of
electron-dense materials in subepithelial regions
( x 15000).
deposition of electron-dense materials in subepithe- lial and mesangial regions ( Fig. 2 ). Under the diag- nosis of membranous glomerulonephritis, stage 1, with nephrotic syndrome, the patient was treated with albumin, furosemide and prednisolone 60mg per day.
Her condition improved and discharged on the eighth day of admission.
After discharge, she was regularly followed in our out patient clinic. The edema waxed and waned.
A test for ANA 6 months later showed 1: 640x, speck- led type positive, but the C3 and C4 level was still within the normal range. Lupus nephritis, class V, was suspected, however, she was lost in the next 2 years.
This patient visited us again in June 2000 with the complaints of diarrhea, abdominal fullness and legs edema. Hypoalbuminemia, hyperchlosterolemia were found, ANA showed 1:1280x but the symptoms were resistant to diuretics, so she was admitted again on August 2000.
During admission, her blood pressure was 130/60 mmHg, pulse rate was 82/min with regular rhythm, and temperature was 36.5 . Hemoglobin was 12.2gm/dl; white blood cell count was 4800/mm
3with normal classification; platelet count was 258000/ mm
3. BUN was 8 mg/dl, Cr was 0.9 mg/dl, serum albumin 1.0 gm/dl, globulin 2.4 gm/dl, total cholesterol 317 mg/dl, triglyceride 226 mg/dl, AST 16 U/L and ALT 8 U/L. However, urinalysis showed no proteinuria and 24-hour urine protein was 54 mg.
Renal ultrasonagraphy showed normal renal size (right 9.8cm, left 11.3cm) with smooth surface and good cortex. The serum C3 was 64.1 mg/dl (normal 69-137), C4 was 20.7 mg/dl (normal 9-33), but anti- DNA was negative. Because the diarrhea and hy- poalbuminemia persisted in spite of aggressive the- rapy, protein-losing enteropathy was suspected. A pro- tein losing study with Tc-99m human serum albumin was performed and showed increased radioactivity in ileum at 6.5 hour and colon at 24 hour ( Fig. 3 ). Under the impression of systemic lupus erythematosus with protein-losing enteropathy, pulse methylpredniso-
lone 1gm daily was given for 3 days followed by prednisolone 50 mg per day. Her diarrhea improved dramatically and the edema disappeared, so she was discharged with stable condition. Her serum albumin was 4.2 gm/dl, globulin 3.0 gm/dl, total cholesterol 181 mg/dl, triglyceride 149 mg/dl, BUN 8 mg/dl and Cr 0.9 mg/dl four months after discharge.
Discussion
The patient first presented as nephrotic syn-
drome due to a membranous glomerulonephirtis
(class V of WHO morphologic classification of lupus
nephritis
5). It is known that patients with the mem-
branous form of lupus nephritis often have low or un-
detectable ANA titers
6. Moreover, antibody to native
DNA is markedly reduced in SLE patients with mem-
branous compared to proliferative glomerulonephir-
tis, and is almost exclusively non-precipitating
7. This
phenomenon is compatible with our patient's mani-
festation, because her ANA was not detected until 6
months after the diagnosis of nephrotic syndrome and
her anti-DNA was persistently negative. In SLE, low
levels of non- precipitating antinuclear antibody fa-
vor the presence of circulating unbound antigen; the
latter is known to be capable of binding non-im-
Fig.3. Tc-99m labeled human serum albumin scintig-
raphy showed increased radioactivity in ileum at
6.5 hour and entire colon at 24 hour.
munologically to glomerular basement membrane and promoting in situ subepithelial immune deposits formation
8.
There are numerous conditions associated with gastrointestinal loss of protein. The most frequently cause is congestive heart failure due to constrictive pericarditis, and forms of lymphatic obstruction, such as intestinal lymphangiectasia, lymphoma, Whipple's disease, abdominal tuberculosis and regional enteri-
tis
1,2,9,10. Intestinal lymphatic obstruction occurs either
directly (eg, intestinal lymphangiectasia) or indirect- ly through high venous pressure on lymphatic flow (eg, constrictive pericarditis) in these conditions.
Leakage from dilated lymphatics resulted in the di- rect loss of proteins, lipids, and lymphocytes
1,9,10. The resultant clinical findings are characteristic.
Hypoalbuminemia, hypoglobulinemia, and lympho- cytopenia with low or normal serum cholesterol oc- cur, frequently with steatorrhea. Other causes of PLE are generally the direct result of intestinal mucosal disruption such as tropical sprue and regional enteri- tis.
The association of SLE and PLE was first re- ported by Waldmann et al
9. in 1969. There are now 22 reported cases of PLE associated with SLE in English literature. Four cases were associated with other commonly recognized causes of PLE, ie, peri- cardial effusion and intestinal lymphangiectasia
4,9-11. The remaining 18 cases
2,3,12-26and our case appeared to be primary protein-losing enteropathies associat- ed with SLE. Young females are predominant in these patients. Diarrhea is present about 50% of the cases.
In the recent survey of the 14 patients with SLE who presented only with PLE
2, all of whom were diag- nosed as having SLE on the basis of a positive ANA.
None of these patients, including the one in our re- port, presented with any of the typical symptoms of SLE, such as malar rash, renal failure, pericarditis, pleural effusions, or vasculitis
2,3. It is of interest that SLE had not been previously diagnosed in one half patients, although some symptoms suggestive of the
disease were frequently present months or years be- fore diagnosis. Thus, severe hypoalbuminemia due to PLE may be the first manifestation of SLE.
The clinical presentation of PLE due to SLE differs markedly from that due to lymphatic obstruc- tion, suggesting a completely separate pathophysio- logy
2. Steatorrhea was absent in all eight cases in which fecal fat was measured, and serum cholesterol levels were abnormally high in 70% of the reported cases. Lymphocytopenia is associated with SLE pro- tein-losing enteropathy in only 10% of cases. In 8 of 8 cases, total serum globulin levels were normal. This pattern is consistent with a selective loss of low- molecular-weight proteins. These findings all suggest a mechanism independent of lymphatic leakage, and are consistent with the inability to demonstrate in- testinal lymphangiectasia in small- and large-bowel biopsy specimens.
The actual pathophysiologic mechanism under-
lying lupus-associated PLE is unknown. Theories in-
clude intestinal lymphangiectasia and direct disrup-
tion of intestinal mucosa
4,9-11, but these causes are un-
likely due to the majority of cases in which lym-
phangiectasia and ulcer is absent. The important cha-
racteristic of this disease is that increased capillary
permeability will permit the loss of protein-rich flu-
id from the microvascular bed to intestinal intersti-
tial tissue, and leakage of colloid into the intestinal
lumen
15,18,23. The resulting hyperlipidemia resembles
the clinical presentation of nephrotic syndrome, in
which loss of proteins or lipid-clearing macro-
molecules stimulates hepatic lipoprotein synthesis
and inhibits lipoprotein catabolism
24. Although in-
testinal vasculitis is the most likely cause of lupus-
associated PLE, confirmation of its causative role is
still lacking. Intestinal venulitis has been described
in one patient by Weiser et al., when a full thickness
of jejunal biopsy was obtained
15. However in all oth-
er patients where small intestinal biopsy has been per-
formed, vasculitis has not been demonstrated
2-4,10,12,16- 23. There is currently few information as to why only
a small patients group develop PLE, especially when the majority of those who are affected lack obvious vasculitic changes or immune deposits on intestinal biopsy.
Lupus-associated PLE should be considered in any young female presenting with hypoalbuminemia and edema, with or without a diagnosis of SLE. If the 24-hour urine protein did not reach the nephrotic range, a protein-losing enteropathy should be con- sidered. Intravenous administered chromium 51- tagged albumin is the gold standard test to assess gas- trointestinal protein excretion
9. Technetium 99m-la- beled albumin and indium 111-labeled plasma trans- ferrin have also been used successfully and are more widely available
27,28, as in our case. Although 24-hour stool
1-antitrypsin clerarance has recently been de- scribed as a convenient nonisotopic diagnostic test, its reliability remains in doubt
23. Once excessive fe- cal protein excretion is found, steatorrhea, lym- phopenia, and hypoglobulinemia suggest the pre- sence of direct or indirect lymphatic obstruction.
Intestinal biopsy will demonstrate the presence of di- lated lymphatics and provide a definite diagnosis when mucosal abnormalities are present. If steator- rhea, lymphopenia, and hypoglobulinemia are not present, a positive antinuclear antibody and hyper- cholesterolemia strongly suggest the diagnosis of pri- mary SLE-associated PLE.
The treatment of choice to primary SLE-associ- ated PLE is steroids. The response of PLE to steroids is nearly uniform. Among 19 treated patients, only 2 cases
4,10were steroid resistant. Cyclophosphamide was successful if the steroids failed. The longest fol- low-up reported in the literature has been 4 years
16, with an average follow-up of 20 months. Relapse oc- curred in at least 30% of patients when the medica- tion was tapered or withdrawn. Nevertheless, steroid tapering is usually successful and one patient was able to discontinue treatment completely.
In summary, we report here a case of suspected SLE with both nephrotic syndrome and protein-los-
ing enteropathy. These two conditions share the com- mon clinical features: hypoalbuminemia, hyper- cholesterolemia and general anarsarca, but with dif- ferent sites of protein loss. The association of PLE should be considered in all patients with SLE having edema and hypoalbuminemia without renal protein loss, as the condition is readily treated with steroids and the overall prognosis is good.
References
1.Waldman TA. Protein-losing enteropathy. Gastroenterology 1966; 50; 422-43.
2.Perednia D, Curosh N. Lupus-associated protein-losing en- teropathy. Arch Intern Med 1990; 150: 1806-10.
3.Sunheimer RL, Finck C, Mortazavi S, Pincus MR. Primary lu- pus-associated protein-losing enteropathy. Ann Clin Lab Sci 1994; 24: 239-42.
4.Meulders Q, Michel C, Marteau P, et al. Association of chronic interstitial cystitis, protein-losing enteropathy and paralytic ileus with seronegative systemic lupus erythematosus: case report and review of the literature. Clin Nephrol 1992; 37: 239-44.
5.McCluskey RT. Lupus nephritis. In: Sommers SC, ed. Kidney Pathology. New York: Appleton-Century Crofts; 1975; 435.
6.Appeal GB, Silva PG, Pirani CL. Renal involvement in systemic lupus erythematosus. In-Medicine, Baltimore 1978; 57: 271.
7.Friend PS, Michael AF. Hypothesis: immunologic rationale for the therapy of membranous nephropathy. Clin Immunol Immunopathol 1978; 10: 35-40.
8.Couser WJ, Salant DJ. In situ immune complex formation and glomerular injury. Kidney Int 1980; 17: 1-13.
9.Waldman TA, Wochner RD, Strober W. The role of gastroin- testinal tract in plasma protein metabolism. Am J Med 1969; 46:
275-85.
10.Chase GJ, O'Shea PA, Collins E, Brem AS. Protein-losing en- teropathy in systemic lupus erythematosus. Hum Pathol 1982;
13: 1053-5.
11.Pereira AS, Peraira-Ficho RA, Trevisan MAS, Magalhaes AFN.
Intestinal lymphangiectasia in systemic lupus erythematosus.
Arg Gastroenterol 1980; 17: 210-2.
12.Pachas WN, Linscheer WG, Pinals RS. Protein-losing en- teropathy in systemic lupus erythematosus. Am J Gastroenterol 1971; 55: 162-7.
13.Trentham DE, Masi AT. Systemic lupus erythematosus with a protein-losing enteropathy. JAMA 1976; 236: 287-8.
14.Tsukahara M, Matsuo K, Kojima H. Protein-losing enteropathy in a boy with systemic lupus erythematosus. J Pediatr 1980; 97:
778-80.
15.Weiser MM, Andres GA, Brentjens JR, Evans JT, Reichlin M.
Systemic lupus erythematosus and intestinal venulitis.
Gastroenterology 1981; 81: 570-9.
16.Takagi S, Oshimi K, Sumiya M, Gonda N, Kana S, Takku F.
Protein-losing enteropathy in systemic lupus erythematosus.
Am J Gastroenterol 1983; 78: 152-4.
17.Wood ML, Foulds IS, French MA. Protein-losing enteropathy due to systemic lupus erythematosus. Gut 1984; 25: 1013-5.
18.Monballyu J, Hauglustaine D, Grebos K, Desmet V, Michielsen P. Protein-losing enteropathy in systemic lupus erythematosus.
Digestion 1985; 31: 243-6.
19.Casteneda S, Moldenhauser F, Herrero-Beaumont G, Yanez R.
Protein-losing enteropathy as the initial manifestation of sys- temic lupus erythematosus. J Rheumatol 1985; 12: 1210-2.
20.Heck LW, Alcaron GS, Ball GV, et al. Pure red cell aplasia and protein-losing enteropathy in a patient with systemic lupus ery- thematosus. Arthritis Rheum 1985; 28: 1059-61.
21.Azais-Noblinski B, Liscia G, Tubiana JM, Marsot-Dupuch K.
Lupus erythemateaux aigu dissemine associe a une enteropathie exsudative. Ann Radiol 1988; 31: 183-7.
22.Edmunds SEJ, Ganju V, Reveridge BR, French MA, Quinlan MF. Protein-losing enteropathy in systemic lupus erythemato- sus. Aust N Z J Med 1988; 18: 868-71.
23.Benner KG, Montanaro A. Protein-losing enteropathy in sys- temic lupus erythematosus: diagnosis and monitoring immuno- suppressive therapy by alpha-1-antitrypsin clearance in stool.
Dig Dis Sci 1989; 34: 132-5.
24.Kobayashi K, Asakura H, Shinozawa T, et al. Protein-losing en- teropathy in systemic lupus erythematosus. Observation by mag- nifying endoscopy. Dig Dis Sci 1989; 34: 1924-8.
25.Chung U, Oka M, Nakagawa Y, et al. A patient with protein-los- ing enteropathy associated with systemic lupus erythematosus.
Intern Med 1992; 31: 521-4.
26.Nakajima A, Ohnishi S, Mimura T, Kubo K, Yazaki Y, Matsuhashi N. Protein-losing enteropathy associated with hypocomplementemia and anti-nuclear antibodies. J Gastroenterol 2000; 35; 627-30.
27.Divgi CR, Lisann NM, Yeh SDJ, Benua RS. Technetium 99m- labeled albumin scintigraphy in the diagnosis of protein-losing enteropathy. J Nucl Med 1986; 27: 1710-2.
28.Saverymuttu SH, Peters AM, Lavender JP, Hidgson HJF.
Detection of protein-losing enteropathy by
111In-transferrin
scanning. Eur J Nucl Med 1983; 8: 40-1.
1
1