行政院國家科學委員會專題研究計畫 期中進度報告
砷甲基化能力、香菸及代謝酵素基因多形性、DNA 損傷及細 胞增生生物標記與泌尿上皮細胞癌之相關性研究(1/3)
計畫類別: 個別型計畫
計畫編號: NSC94-2314-B-038-023-
執行期間: 94 年 08 月 01 日至 95 年 07 月 31 日 執行單位: 臺北醫學大學公共衛生學科
計畫主持人: 薛玉梅
報告類型: 精簡報告
報告附件: 出席國際會議研究心得報告及發表論文 處理方式: 本計畫可公開查詢
中 華 民 國 95 年 7 月 10 日
行政院國家科學委員會補助專題研究計畫 □ 成 果 報 告
□期中進度報告
(計畫名稱)
砷甲基化能力、香菸及代謝酵素基因多形性、DNA 損傷及細胞增生生物標記與泌 尿上皮細胞癌之相關性研究
Arsenic methylation capability, cigarette smoking and metabolic enzymes polymorphism, DNA damage, cell proliferation biomarker and urothelial carcinoma
計畫類別:■ 個別型計畫 整合型計畫 計畫編號:NSC 94-2314-B-038-023 (1/3)
執行期間:94 年 8 月 1 日至 95 年 7 月 31 日
計畫主持人:薛玉梅 共同主持人:
計畫參與人員:
成果報告類型(依經費核定清單規定繳交):■精簡報告 □完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
■出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計
附件一
砷甲基化能力、香菸及代謝酵素基因多形性、DNA 損傷及細胞增生生物標記 與泌尿上皮細胞癌之相關性研究
前言
無機砷被認為是人類皮膚癌與肺癌之致癌物。最近研究發現長期經由食入與吸 入暴露無機砷會增加膀胱癌與腎臟癌的危險性,特別是移行細胞癌(Chiou et al.
2001)。無機砷甲基化過去被認為是去毒作用,但是,最近有研究指出無機砷甲基化 也許是致毒作用而非去毒作用。因為在代謝過程中產生的三價的甲基化代謝物如三 價的單甲基砷酸、三價的雙甲基砷酸和少量的三價的三甲基砷酸也許比無機砷毒性 更大(Lin et al. 1999;Petrick et al. 2000;Styblo et al. 1997)。臺灣烏腳病盛行地區居民尿 液無機砷百分比隨年齡增加而增加,而單甲基砷酸百分比、雙甲基砷酸百分比隨年 齡增加而減少。女性尿液無機砷與單甲基砷酸百分比比男性偏低而雙甲基砷酸百分 比比男性偏高,顯示女性代謝能力比男性好(Hsueh et al. 1998)。臺灣西南沿海烏腳 病盛行地區研究,亦發現累積砷暴露越高且尿液中單甲基砷酸百分比越高者,皮膚 癌危險性顯著偏高(Hsueh et al. 1997)。臺灣的醫院收集之膀胱癌病例對照研究中也 發現二級砷代謝指標(雙甲基砷酸百分比/單甲基砷酸百分比)較差且慢性砷暴露較
高者罹患膀胱癌之危險性較高(Chen et al. 2003)。
在人類細胞(Schwerdtle et al. 2003)與動物細胞(Kessel et al. 2002)體外試驗均可
觀察到砷誘發氧化性DNA 傷害。雖然許多機轉被提出,但砷如何誘發氧化性 DNA
傷害尚未清楚。氧化性DNA 傷害的代謝產物,8-hydroxydeoxyguanine (8-OHdG)在 尿液排出,不僅可作為DNA 修復而且亦可作為 DNA 氧化傷害的生物標記(Cooke et al. 2000;Helbock et al. 1999)。有研究利用 enzyme-linked immunosorbent (ELISA)測定 尿液8-OHdG 濃度,發現膀胱癌與胰臟癌病患尿液中 8-OHdG 濃度顯著高於健康對 照者(Chiou et al. 2003a)。最近也有研究利用 ELISA 測定尿液 8-OHdG 濃度(Saito et al.
2000),發現急性三價砷或慢性五價砷暴露者尿液中 8-OHdG 濃度增加(Yamauchi et al.
2004)。然而這些研究其樣本數較少且低砷暴露者是否也會增加 8-OHdG 濃度,而與 泌尿上皮細胞癌之危險性有關應深入探討。
很多的癌細胞是因為細胞生長調控失衡而使細胞不斷生長導致腫瘤增生,在調 控細胞生長過程中,cyclin 隨著 G1、S、G2 與 M 細胞週期而變動,是一個控制細
胞週期相當重要的蛋白。不同型態的cyclin 在不同的細胞週期出現,當任務完成時
cyclin 就會被分解或失去活性。細胞生長週期 G1 到 S 期生長調控相關基因若失去 平衡,細胞會不停增生,導致腫瘤發生(Obaya and Sedivy 2002)。調控細胞生長週期 G1 到 S 期相關的基因有 cyclin D1 (CCND1)、cyclin dependent kinase 4 (CDK4)、
cyclin-dependent kinase inhibitor 1a (CDKN2A, p21/p14)、retinoblastoma (RB)與 p53。
有報告指出致癌性金屬會影響細胞內訊息傳遞與細胞週期(Chen and Shi 2002)。
P53 Arg/Arg 基因型比 Pro/Pro 基因型更有效的誘發細胞凋亡且抑制細胞轉形 (Thomas et al. 1999),顯示 Pro/Pro 基因型較 Arg/Arg 基因型更具癌症易感性,其中
包括攝護腺癌。由於P53 在控制細胞週期扮演重要角色,它或許也參與泌尿上皮細
胞癌的癌化過程是應值得研究。P21(W/CIP1)是一個 cyclin-dependent kinase
inhibitor,是 P53 抑癌基因下游調控細胞週期的因子(Xiong et al. 1993)。P21 基因改 變也許能中斷P53 所調控之細胞週期停止而增加癌症的易感性。P21 在 codon 31 發
最近分子基因研究發現累積活化致癌基因與抑制抑癌基因會導致膀胱癌的發生與 惡化(Reznikoff et al. 2000b)。膀胱癌癌化過程的標的是在細胞週期的 G1-S 期進展失 調,而G1 至 S 期是由 cyclin、cyclin-dependent kinases 與其抑制劑調控(Reznikoff et al. 2000a)。Cyclin D1 是 G1/S 期很重要的調控者且與許多人類癌症有關(Hunter and Pines 1994)。Cyclin D1 基因位於染色體 11q13 上,在第 807 位置有 A/G 的基因多形 性,這個基因多形性會影響到基因的splicing(Betticher et al. 1995),膀胱癌經常偵測 到此染色體位置有增殖現象(Habuchi et al. 1994;Proctor et al. 1991)。在流行病學研究 中,兩股皆帶有G allele 的人比帶有 AG 或 AA 基因型的人直腸癌發生的年齡較低 且存活率較高(Kong et al. 2000)。而 AA 基因型的高加索人罹患直腸癌的危險性是帶 有GG 基因型的 2.68 倍(Kong et al. 2001)。在夏威夷研究中日本人、白人與夏威夷 人等不同種族間,CCND1 (A807G)帶 AG 或 AA 基因型者直腸癌的危險性比 GG 基 因型者較高,但僅發現在夏威夷族群(Le Marchand et al. 2003b)。CCND1 A allele 與 膀胱移形細胞癌的危險性增加有關,特別是發生在沒有抽菸的男性且其與疾病的嚴 重程度有關(Wang et al. 2002)。CCND1 A allele 是否與砷或抽菸造成之泌尿上皮細胞 癌有關是有趣的課題。
材料與方法
自民國九十一年五月到九十三年十二月間,至臺大醫院與台南縣奇美醫院泌尿 科門診就診或複診之泌尿上皮細胞癌患者共323 人(臺大醫院 201 人,奇美醫院 122 人)為病例組。由醫師轉介,訪員進行患者面訪,同時採取血液及尿液加以冷凍儲存。
所有研究對象皆有簽署同意書。預計從九十四年八月至九十七年七月繼續收案 200
位泌尿上皮細胞癌患者。
自臺大醫院與奇美醫院泌尿科門診就診無癌症之年齡與性別配對的對象經由 醫師轉介,此外並從台北醫學大學附設醫院與萬芳醫院健康住院檢查者之年齡與性 別配對之健康對照為對照組,由訪員面訪並收集其血液尿液。所有研究對象皆有簽 署同意書。九十一年五月到九十三年十二月間共收案 465 人,預計從九十四年八月
至九十七年七月繼續收案300 位健康對照。毎位研究對象由受過標準化訪視訓練的
訪員利用結構式問卷進行訪視。問卷內容包括社會人口學資料、職業史、居住史、
抽菸與喝酒等生活習慣、個人及家族疾病史等。
尿液經濾膜與C18前處理後,利用高效能液相層析儀分離尿液中三價砷酸、五
價砷酸、單甲基砷酸與雙甲基砷酸等砷物種,連結氫化器與原子吸收光譜儀進行各 砷物種濃度定量。
測定8-OHdG 的方法為高效能液相層析儀(Wood et al. 2000),而有另一種 enzyme-linked immunosorbent (ELISA)測定方法(Yin et al. 1995)。尿液檢體經 1500 rpm 離心十分鐘,上清液以備 8-OHdG 測定。離心後尿液上清液(1:5 in PBS) 50µl 放入 96 孔盤上,加 50µl 8-OHdG 抗體(1:150000 in PBS 含 1%BSA),室溫 下震盪一小時,利用緩衝液洗四次,毎個孔中加入50µenzyme-liked secondary 抗 體,室溫下培養一小時,清洗後毎個孔中加100µl 的 tetramethylbenzidine,加 入100µl 的 0.5 mol/1 H2SO4將反應停止五分鐘後,450 nm 波長測定吸光值 (Chiou et al. 2003b)。
分解,電泳圖出現113-bp 與 86-bp 片段者為 Arg allele,出現 199-bp 片段者為 Pro allele,出現 113-bp 、86-bp 與 199-bp 片段者為 Arg/Pro 基因型(Fan et al.
2000)。
P21 codon 31 基因多形性測定方法,利用正向引子 5’-GTCAGAACCGGATGGGGATG-3’ 及反向引子
5’-CTCCTCCCAACTCATAAAGG-3’ 夾出所需基因片段,經由聚合酵素連鎖反 應增幅此一基因片段。增幅條件為one cycle 94℃,5 min; 35 cycles,94℃,40s,
60.3℃ 30s, 72℃,40s;及 one cycle 72℃,10 min。利用限制酵素 BlpI 分解,
電泳圖出現89-bp 與 183-bp 片段者為 Ser allele,出現 272-bp 片段者為 Arg allele,
89-bp、183-bp 與 272-bp 片段者為 Ser/Arg 基因型(Li et al. 1995)。
CCND1 基因多形性測定方法,基因多形性主要以 Le Marchand 等人的方法 為主再加以修飾,利用正向引子5’-AGTTCATTTCCAATCCGCCC-3’與反向引子 5’-TTTCCGTGGCACTAGGTGTC-3’夾出所需基因片段,經由聚合酵素連鎖增幅 此一基因片段。增幅條件為94 °C 起始 denature 5 分鐘,再以 94°C 30、60 °C 30 秒與72 °C30 秒循環 35 次,最後停留在 72 °C 10 分鐘。放大的基因再以限制 酵素 Moraxella species (MspI)作用之後以 3%凝膠電泳辨識 CCND1 基因多形性 (Le Marchand et al. 2003a)。
討論
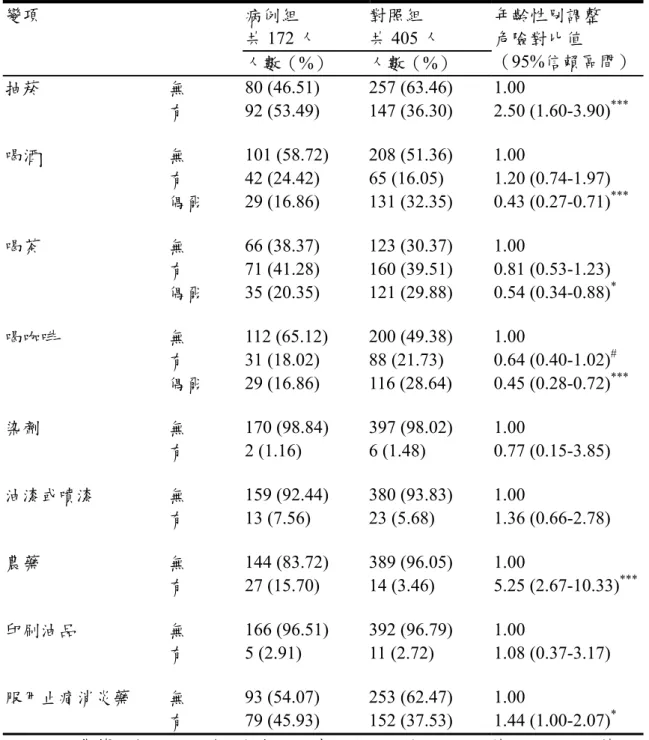
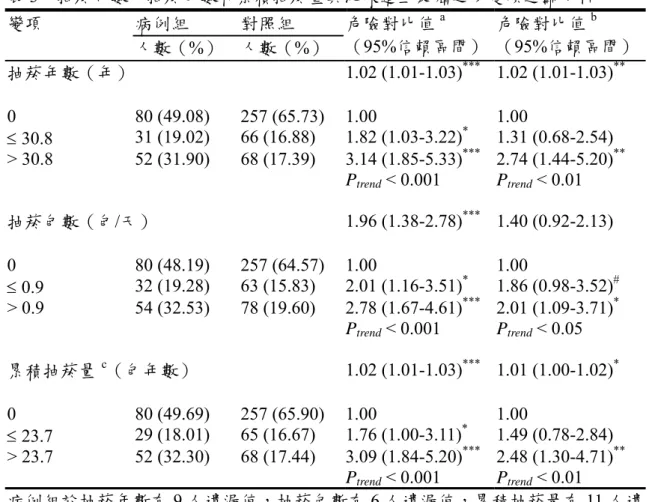
泌尿道上皮癌危險對比值與教育程度呈負相關,父母親氏族為外省人者危險性 比閩南人顯著偏低。抽菸者泌尿道上皮癌危險對比值顯著比非抽菸者偏高,農藥暴 露者泌尿道上皮癌危險對比值顯著比非暴露偏高,偶而喝酒者有較低的危險性。隨 著抽菸年樹、包數與年包數的增加泌尿道上皮癌危險對比值顯著增加。
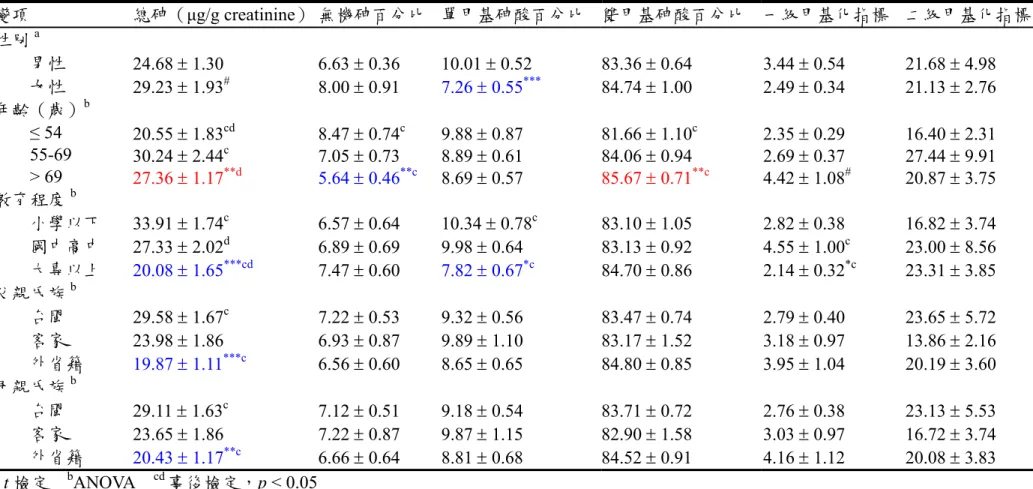
雖然本研究對象屬於ㄧ般飲用自來水之族群,而自來水中砷的含量在過去是 50 ppb,自 2000 年降為 10 ppb。雖然研究個案的總砷濃度比高砷暴露地區居民高,
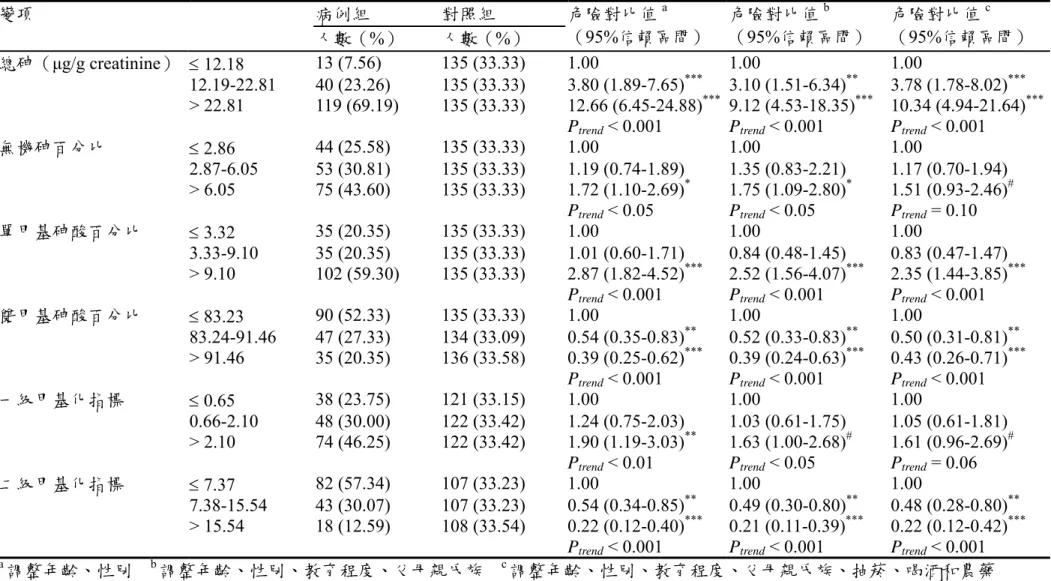
但是個體對於砷甲基化能力的差異仍會影響疾病的發展。單甲基砷酸百分比較高者 或雙甲基砷酸百分比較低者泌尿道上皮癌危險對比值顯著增加。抽菸與砷甲基化能
力對泌尿道上皮癌危險對比有交互作用。本研究中抽菸與尿液中8-OHdG 濃度無
關,抽菸並非增加尿液中8-OHdG 含量的重要來源。然而隨著總砷濃度增加,尿液
中8-OHdG 含量顯著增加。尿液中 8-OHdG 含量與泌尿道上皮癌危險對比值呈顯 著正相關。p21 codon 31 基因型與泌尿道上皮癌有關。隨著基因型異常個數增加泌 尿道上皮癌危險對比值增加。基因型與尿液砷物種之間對泌尿道上皮癌危險對比值 有交互作用,但統計上並無顯著性。
本研究是一個病例對照研究,而病患為盛行病例,尿液和血液檢體的取得是在 疾病診斷後,因此除了與生俱來的特性,如性別及遺傳基因等之外,在因果時序性
上較不易辨明。未來須待發生病例探討8-OHdG 和砷甲基化能力與泌尿道上皮癌的
相關性。總而言之,抽菸、砷甲基化能力差及DNA 氧化傷害較高是泌尿道上皮癌
的重要危險因子。飲用水中含砷量降為10ppb 之後,砷甲基化能力與泌尿道上皮癌
的相關有待釐清。減少外來環境暴露所造成的氧化壓力,應能有效降低疾病發生的 危險性。
結果
表1 泌尿道上皮癌病例組與對照組之社會人口學特性
病例組 共172 人
對照組 共405 人 變項
人數(%) 人數(%)
年齡性別調整 危險對比值
(95%信賴區間)
性別 女性 49 (28.49) 126 (31.11) 1.00
男性 123 (71.51) 279 (68.89) 1.12 (0.75-1.65)a 年齡(歲) 61.98 ± 1.08 61.52 ± 0.71 1.00 (0.99-1.02)b 血型 A 46 (26.74) 96 (23.70) 1.00
B 38 (22.09) 85 (20.99) 0.90 (0.54-1.53) O 62 (36.05) 180 (44.44) 0.71 (0.45-1.12) AB 12 (6.98) 22 (5.43) 1.13 (0.51-2.49) 婚姻狀況 未婚 12 (6.98) 22 (5.43) 1.00
已婚 136 (79.07) 322 (79.51) 0.73 (0.34-1.56) 離婚分居 6 (3.49) 21 (5.19) 0.52 (0.16-1.66) 鰥寡 18 (10.47) 39 (9.63) 0.80 (0.30-2.18) 教育程度 小學以下 66 (38.37) 74 (18.27) 1.00
國中高中 67 (38.95) 138 (34.07) 0.47 (0.30-0.75)**
大專以上 39 (22.67) 190 (46.91) 0.19 (0.11-0.31)***
父親氏族 台閩 125 (72.67) 219 (54.07) 1.00
客家 16 (9.30) 45 (11.11) 0.65 (0.35-1.19) 外省籍 31 (18.02) 138 (34.07) 0.36 (0.22-0.57)***
原住民 0 (0.00) 2 (0.49)
母親氏族 台閩 126 (73.26) 229 (56.54) 1.00
客家 16 (9.30) 45 (11.11) 0.67 (0.36-1.24) 外省籍 30 (17.44) 127 (31.36) 0.39 (0.24-0.62)***
原住民 0 (0.00) 3 (0.74)
病例組於血型變項有14 人遺漏值,而對照組於血型變項有 22 人、教育程度變項有
3 人及婚姻狀況和父母親氏族等變項皆各有 1 人遺漏值
a調整年齡 b調整性別
* p < 0.05, ** p < 0.01, *** p < 0.001
表2 泌尿道上皮癌病例組與對照組之生活型態和化學物質暴露分佈 病例組
共172 人
對照組 共405 人 變項
人數(%) 人數(%)
年齡性別調整 危險對比值
(95%信賴區間)
抽菸 無 80 (46.51) 257 (63.46) 1.00
有 92 (53.49) 147 (36.30) 2.50 (1.60-3.90)***
喝酒 無 101 (58.72) 208 (51.36) 1.00
有 42 (24.42) 65 (16.05) 1.20 (0.74-1.97) 偶爾 29 (16.86) 131 (32.35) 0.43 (0.27-0.71)***
喝茶 無 66 (38.37) 123 (30.37) 1.00
有 71 (41.28) 160 (39.51) 0.81 (0.53-1.23) 偶爾 35 (20.35) 121 (29.88) 0.54 (0.34-0.88)* 喝咖啡 無 112 (65.12) 200 (49.38) 1.00
有 31 (18.02) 88 (21.73) 0.64 (0.40-1.02)# 偶爾 29 (16.86) 116 (28.64) 0.45 (0.28-0.72)***
染劑 無 170 (98.84) 397 (98.02) 1.00
有 2 (1.16) 6 (1.48) 0.77 (0.15-3.85) 油漆或噴漆 無 159 (92.44) 380 (93.83) 1.00
有 13 (7.56) 23 (5.68) 1.36 (0.66-2.78) 農藥 無 144 (83.72) 389 (96.05) 1.00
有 27 (15.70) 14 (3.46) 5.25 (2.67-10.33)***
印刷油品 無 166 (96.51) 392 (96.79) 1.00
有 5 (2.91) 11 (2.72) 1.08 (0.37-3.17) 服用止痛消炎藥 無 93 (54.07) 253 (62.47) 1.00
有 79 (45.93) 152 (37.53) 1.44 (1.00-2.07)*
病例組於農藥和印刷油品變項各有1 人遺漏值,而對照組於抽菸、喝酒、喝茶及
喝咖啡等變項各有1 人遺漏值,染劑、油漆或噴漆、農藥和印刷油品等變項則各
有2 人遺漏值
# 0.05 < p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001
表3 抽菸年數、抽菸包數和累積抽菸量與泌尿道上皮癌之多變項迴歸分析
病例組 對照組
變項
人數(%) 人數(%)
危險對比值a
(95%信賴區間)
危險對比值b
(95%信賴區間)
抽菸年數(年) 1.02 (1.01-1.03)*** 1.02 (1.01-1.03)**
0 80 (49.08) 257 (65.73) 1.00 1.00
≤ 30.8 31 (19.02) 66 (16.88) 1.82 (1.03-3.22)* 1.31 (0.68-2.54)
> 30.8 52 (31.90) 68 (17.39) 3.14 (1.85-5.33)*** 2.74 (1.44-5.20)**
Ptrend < 0.001 Ptrend < 0.01 抽菸包數(包/天) 1.96 (1.38-2.78)*** 1.40 (0.92-2.13) 0 80 (48.19) 257 (64.57) 1.00 1.00
≤ 0.9 32 (19.28) 63 (15.83) 2.01 (1.16-3.51)* 1.86 (0.98-3.52)#
> 0.9 54 (32.53) 78 (19.60) 2.78 (1.67-4.61)*** 2.01 (1.09-3.71)* Ptrend < 0.001 Ptrend < 0.05 累積抽菸量c(包年數) 1.02 (1.01-1.03)*** 1.01 (1.00-1.02)* 0 80 (49.69) 257 (65.90) 1.00 1.00
≤ 23.7 29 (18.01) 65 (16.67) 1.76 (1.00-3.11)* 1.49 (0.78-2.84)
> 23.7 52 (32.30) 68 (17.44) 3.09 (1.84-5.20)*** 2.48 (1.30-4.71)**
Ptrend < 0.001 Ptrend < 0.01
病例組於抽菸年數有9 人遺漏值,抽菸包數有 6 人遺漏值,累積抽菸量有 11 人遺
漏值;對照組於抽菸年數有14 人遺漏值,抽菸包數有 7 人遺漏值,累積抽菸量則
有15 人遺漏值
a調整年齡、性別
b調整年齡、性別、教育程度、父母親氏族、喝酒、農藥和總砷濃度
c累積抽菸量=(抽菸包數/天)× 抽菸年數
# 0.05 < p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001
表4 尿液總砷濃度及砷甲基化能力指標與社會人口學特性之比較
變項 總砷(µg/g creatinine) 無機砷百分比 單甲基砷酸百分比 雙甲基砷酸百分比 一級甲基化指標 二級甲基化指標
性別a
男性 24.68 ± 1.30 6.63 ± 0.36 10.01 ± 0.52 83.36 ± 0.64 3.44 ± 0.54 21.68 ± 4.98 女性 29.23 ± 1.93# 8.00 ± 0.91 7.26 ± 0.55*** 84.74 ± 1.00 2.49 ± 0.34 21.13 ± 2.76 年齡(歲)b
≤ 54 20.55 ± 1.83cd 8.47 ± 0.74c 9.88 ± 0.87 81.66 ± 1.10c 2.35 ± 0.29 16.40 ± 2.31 55-69 30.24 ± 2.44c 7.05 ± 0.73 8.89 ± 0.61 84.06 ± 0.94 2.69 ± 0.37 27.44 ± 9.91 > 69 27.36 ± 1.17**d 5.64 ± 0.46**c 8.69 ± 0.57 85.67 ± 0.71**c 4.42 ± 1.08# 20.87 ± 3.75 教育程度b
小學以下 33.91 ± 1.74c 6.57 ± 0.64 10.34 ± 0.78c 83.10 ± 1.05 2.82 ± 0.38 16.82 ± 3.74 國中高中 27.33 ± 2.02d 6.89 ± 0.69 9.98 ± 0.64 83.13 ± 0.92 4.55 ± 1.00c 23.00 ± 8.56 大專以上 20.08 ± 1.65***cd 7.47 ± 0.60 7.82 ± 0.67*c 84.70 ± 0.86 2.14 ± 0.32*c 23.31 ± 3.85 父親氏族b
台閩 29.58 ± 1.67c 7.22 ± 0.53 9.32 ± 0.56 83.47 ± 0.74 2.79 ± 0.40 23.65 ± 5.72 客家 23.98 ± 1.86 6.93 ± 0.87 9.89 ± 1.10 83.17 ± 1.52 3.18 ± 0.97 13.86 ± 2.16 外省籍 19.87 ± 1.11***c 6.56 ± 0.60 8.65 ± 0.65 84.80 ± 0.85 3.95 ± 1.04 20.19 ± 3.60 母親氏族b
台閩 29.11 ± 1.63c 7.12 ± 0.51 9.18 ± 0.54 83.71 ± 0.72 2.76 ± 0.38 23.13 ± 5.53 客家 23.65 ± 1.86 7.22 ± 0.87 9.87 ± 1.15 82.90 ± 1.58 3.03 ± 0.97 16.72 ± 3.74 外省籍 20.43 ± 1.17**c 6.66 ± 0.64 8.81 ± 0.68 84.52 ± 0.91 4.16 ± 1.12 20.08 ± 3.83
a t 檢定 bANOVA cd事後檢定,p < 0.05
表5 尿液總砷濃度及砷甲基化能力指標與泌尿道上皮癌之相關性
病例組 對照組
變項
人數(%) 人數(%)
危險對比值a
(95%信賴區間)
危險對比值b
(95%信賴區間)
危險對比值c
(95%信賴區間)
≤ 12.18 13 (7.56) 135 (33.33) 1.00 1.00 1.00
總砷(µg/g creatinine)
12.19-22.81 40 (23.26) 135 (33.33) 3.80 (1.89-7.65)*** 3.10 (1.51-6.34)** 3.78 (1.78-8.02)***
> 22.81 119 (69.19) 135 (33.33) 12.66 (6.45-24.88)*** 9.12 (4.53-18.35)*** 10.34 (4.94-21.64)***
Ptrend < 0.001 Ptrend < 0.001 Ptrend < 0.001
≤ 2.86 44 (25.58) 135 (33.33) 1.00 1.00 1.00
無機砷百分比
2.87-6.05 53 (30.81) 135 (33.33) 1.19 (0.74-1.89) 1.35 (0.83-2.21) 1.17 (0.70-1.94)
> 6.05 75 (43.60) 135 (33.33) 1.72 (1.10-2.69)* 1.75 (1.09-2.80)* 1.51 (0.93-2.46)# Ptrend < 0.05 Ptrend < 0.05 Ptrend = 0.10
≤ 3.32 35 (20.35) 135 (33.33) 1.00 1.00 1.00
單甲基砷酸百分比
3.33-9.10 35 (20.35) 135 (33.33) 1.01 (0.60-1.71) 0.84 (0.48-1.45) 0.83 (0.47-1.47)
> 9.10 102 (59.30) 135 (33.33) 2.87 (1.82-4.52)*** 2.52 (1.56-4.07)*** 2.35 (1.44-3.85)***
Ptrend < 0.001 Ptrend < 0.001 Ptrend < 0.001
≤ 83.23 90 (52.33) 135 (33.33) 1.00 1.00 1.00 雙甲基砷酸百分比
83.24-91.46 47 (27.33) 134 (33.09) 0.54 (0.35-0.83)** 0.52 (0.33-0.83)** 0.50 (0.31-0.81)**
> 91.46 35 (20.35) 136 (33.58) 0.39 (0.25-0.62)*** 0.39 (0.24-0.63)*** 0.43 (0.26-0.71)***
Ptrend < 0.001 Ptrend < 0.001 Ptrend < 0.001
≤ 0.65 38 (23.75) 121 (33.15) 1.00 1.00 1.00
一級甲基化指標
0.66-2.10 48 (30.00) 122 (33.42) 1.24 (0.75-2.03) 1.03 (0.61-1.75) 1.05 (0.61-1.81)
> 2.10 74 (46.25) 122 (33.42) 1.90 (1.19-3.03)** 1.63 (1.00-2.68)# 1.61 (0.96-2.69)# Ptrend < 0.01 Ptrend < 0.05 Ptrend = 0.06
≤ 7.37 82 (57.34) 107 (33.23) 1.00 1.00 1.00
二級甲基化指標
7.38-15.54 43 (30.07) 107 (33.23) 0.54 (0.34-0.85)** 0.49 (0.30-0.80)** 0.48 (0.28-0.80)**
> 15.54 18 (12.59) 108 (33.54) 0.22 (0.12-0.40)*** 0.21 (0.11-0.39)*** 0.22 (0.12-0.42)***
P < 0.001 P < 0.001 P < 0.001
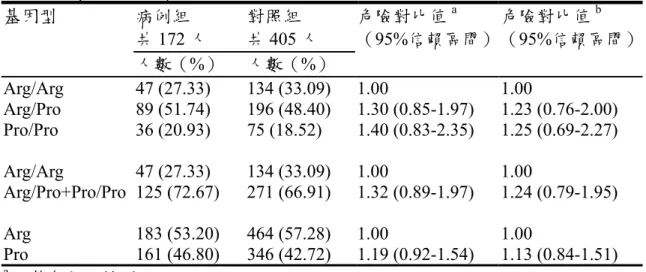
表6 泌尿道上皮癌病例組與對照組之 p53 codon 72 基因型分佈 病例組
共172 人
對照組 共405 人
危險對比值a
(95%信賴區間)
基因型
人數(%) 人數(%)
危險對比值b
(95%信賴區間)
Arg/Arg 47 (27.33) 134 (33.09) 1.00 1.00
Arg/Pro 89 (51.74) 196 (48.40) 1.30 (0.85-1.97) 1.23 (0.76-2.00) Pro/Pro 36 (20.93) 75 (18.52) 1.40 (0.83-2.35) 1.25 (0.69-2.27) Arg/Arg 47 (27.33) 134 (33.09) 1.00 1.00
Arg/Pro+Pro/Pro 125 (72.67) 271 (66.91) 1.32 (0.89-1.97) 1.24 (0.79-1.95) Arg 183 (53.20) 464 (57.28) 1.00 1.00
Pro 161 (46.80) 346 (42.72) 1.19 (0.92-1.54) 1.13 (0.84-1.51)
a調整年齡、性別
b調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒、農藥和總砷濃度
表7 泌尿道上皮癌病例組與對照組之 p21 codon 31 基因型分佈 病例組†
共171 人
對照組 共405 人
危險對比值a
(95%信賴區間)
基因型
人數(%) 人數(%)
危險對比值b
(95%信賴區間)
Ser/Ser 44 (25.73) 98 (24.20) 1.00 1.00
Ser/Arg 75 (43.86) 216 (53.33) 0.76 (0.48-1.18) 0.69 (0.42-1.15) Arg/Arg 52 (30.41) 91 (22.47) 1.26 (0.77-2.07) 1.25 (0.71-2.21) Ser/Ser+Ser/Arg 119 (69.59) 314 (77.53) 1.00 1.00
Arg/Arg 52 (30.41) 91 (22.47) 1.52 (1.02-2.28)* 1.59 (1.00-2.53)# Ser 163 (47.66) 412 (50.86) 1.00 1.00
Arg 179 (52.34) 398 (49.14) 1.13 (0.88-1.46) 1.13 (0.84-1.51)
†病例組1 人之 PCR 反應不成功
a調整年齡、性別
b調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒、農藥和總砷濃度
# 0.05 < p < 0.1, * p < 0.05
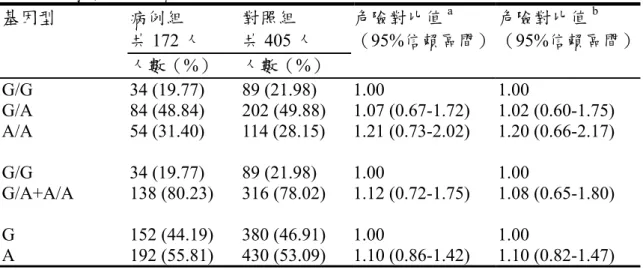
表8 泌尿道上皮癌病例組與對照組之 CCND1 G870A 基因型分佈 病例組
共172 人
對照組 共405 人
危險對比值a
(95%信賴區間)
基因型
人數(%) 人數(%)
危險對比值b
(95%信賴區間)
G/G 34 (19.77) 89 (21.98) 1.00 1.00
G/A 84 (48.84) 202 (49.88) 1.07 (0.67-1.72) 1.02 (0.60-1.75) A/A 54 (31.40) 114 (28.15) 1.21 (0.73-2.02) 1.20 (0.66-2.17) G/G 34 (19.77) 89 (21.98) 1.00 1.00
G/A+A/A 138 (80.23) 316 (78.02) 1.12 (0.72-1.75) 1.08 (0.65-1.80) G 152 (44.19) 380 (46.91) 1.00 1.00
A 192 (55.81) 430 (53.09) 1.10 (0.86-1.42) 1.10 (0.82-1.47)
a調整年齡、性別
b調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒、農藥和總砷濃度
表9 危險基因型個數與泌尿道上皮癌之相關性
變項 病例組
/對照組
危險對比值a
(95%信賴區間)
危險對比值b
(95%信賴區間)
基因型 危險基因型個數c
p53 codon 72 0 c 9/22 1.00 1.00
p21 codon 31 1 40/131 0.76 (0.32-1.78) 0.68 (0.24-1.91) CCND1 G870A 2 93/209 1.08 (0.48-2.45) 0.92 (0.34-2.48) 3 29/43 1.66 (0.67-4.12) 1.56 (0.52-4.65)
Ptrend < 0.05 Ptrend = 0.06
a調整年齡、性別
b調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒、農藥和總砷濃度
c p53 codon 72 基因型為 Arg/Pro+Pro/Pro、p21 codon 31 基因型為 Arg/Arg 及 CCND1 G870A 基因型為 G/A+A/A
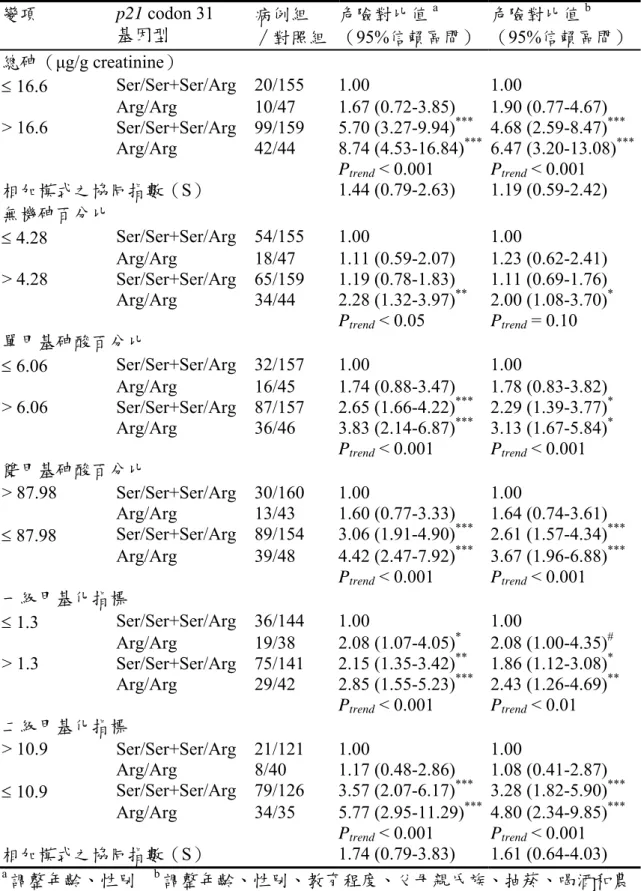
表10 砷甲基化能力指標和 p21 codon 31 基因型與泌尿道上皮癌之交互作用 變項 p21 codon 31
基因型
病例組
/對照組
危險對比值a
(95%信賴區間)
危險對比值b
(95%信賴區間)
總砷(µg/g creatinine)
≤ 16.6 Ser/Ser+Ser/Arg 20/155 1.00 1.00
Arg/Arg 10/47 1.67 (0.72-3.85) 1.90 (0.77-4.67)
> 16.6 Ser/Ser+Ser/Arg 99/159 5.70 (3.27-9.94)*** 4.68 (2.59-8.47)***
Arg/Arg 42/44 8.74 (4.53-16.84)*** 6.47 (3.20-13.08)***
Ptrend < 0.001 Ptrend < 0.001 相加模式之協同指數(S) 1.44 (0.79-2.63) 1.19 (0.59-2.42) 無機砷百分比
≤ 4.28 Ser/Ser+Ser/Arg 54/155 1.00 1.00
Arg/Arg 18/47 1.11 (0.59-2.07) 1.23 (0.62-2.41)
> 4.28 Ser/Ser+Ser/Arg 65/159 1.19 (0.78-1.83) 1.11 (0.69-1.76) Arg/Arg 34/44 2.28 (1.32-3.97)** 2.00 (1.08-3.70)*
Ptrend < 0.05 Ptrend = 0.10 單甲基砷酸百分比
≤ 6.06 Ser/Ser+Ser/Arg 32/157 1.00 1.00
Arg/Arg 16/45 1.74 (0.88-3.47) 1.78 (0.83-3.82)
> 6.06 Ser/Ser+Ser/Arg 87/157 2.65 (1.66-4.22)*** 2.29 (1.39-3.77)* Arg/Arg 36/46 3.83 (2.14-6.87)*** 3.13 (1.67-5.84)*
Ptrend < 0.001 Ptrend < 0.001 雙甲基砷酸百分比
> 87.98 Ser/Ser+Ser/Arg 30/160 1.00 1.00
Arg/Arg 13/43 1.60 (0.77-3.33) 1.64 (0.74-3.61)
≤ 87.98 Ser/Ser+Ser/Arg 89/154 3.06 (1.91-4.90)*** 2.61 (1.57-4.34)***
Arg/Arg 39/48 4.42 (2.47-7.92)*** 3.67 (1.96-6.88)***
Ptrend < 0.001 Ptrend < 0.001 一級甲基化指標
≤ 1.3 Ser/Ser+Ser/Arg 36/144 1.00 1.00
Arg/Arg 19/38 2.08 (1.07-4.05)* 2.08 (1.00-4.35)#
> 1.3 Ser/Ser+Ser/Arg 75/141 2.15 (1.35-3.42)** 1.86 (1.12-3.08)* Arg/Arg 29/42 2.85 (1.55-5.23)*** 2.43 (1.26-4.69)**
Ptrend < 0.001 Ptrend < 0.01 二級甲基化指標
> 10.9 Ser/Ser+Ser/Arg 21/121 1.00 1.00
Arg/Arg 8/40 1.17 (0.48-2.86) 1.08 (0.41-2.87)
≤ 10.9 Ser/Ser+Ser/Arg 79/126 3.57 (2.07-6.17)*** 3.28 (1.82-5.90)***
Arg/Arg 34/35 5.77 (2.95-11.29)*** 4.80 (2.34-9.85)***
Ptrend < 0.001 Ptrend < 0.001 相加模式之協同指數(S) 1.74 (0.79-3.83) 1.61 (0.64-4.03)
a調整年齡、性別 b調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒和農
藥 # 0.05 < p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001
表11 泌尿道上皮癌病例組與對照組尿液中氧化傷害指標之比較
病例組 對照組
變項
人數 平均值±標準誤 人數 平均值±標準誤
t 檢定† p 值 170 7.48 ± 0.97 402 5.95 ± 0.21 0.03 8-OHdG 濃度
(ng/mg creatinine)
病例組2 人和對照組 3 人之尿液遺漏
† 8-OHdG 濃度以 Log10轉換
表12 尿液中氧化傷害指標與泌尿道上皮癌之相關性
變項 危險對比值a
(95%信賴區間)
危險對比值b
(95%信賴區間)
危險對比值c
(95%信賴區間)
Log10 8-OHdG 濃度
(ng/mg creatinine)
2.19 (1.16-4.13)* 2.09 (1.10-3.99)* 1.50 (0.77-2.95)
變項 危險對比值d
(95%信賴區間)
危險對比值e
(95%信賴區間)
危險對比值f
(95%信賴區間)
Log10 8-OHdG 濃度
(ng/mg creatinine)
2.01 (1.01-4.00)* 1.99 (1.00-3.97)# 1.41 (0.69-2.91) 病例組2 人和對照組 3 人之尿液遺漏
a調整年齡、性別 b調整年齡、性別、抽菸 c調整年齡、性別、總砷濃度 d調整
年齡、性別、教育程度、父母親氏族、喝酒和農藥 e調整年齡、性別、教育程度、
父母親氏族、抽菸、喝酒、農藥 f調整年齡、性別、教育程度、父母親氏族、抽
菸、喝酒、農藥和總砷濃度
# 0.05 < p < 0.1, * p < 0.05
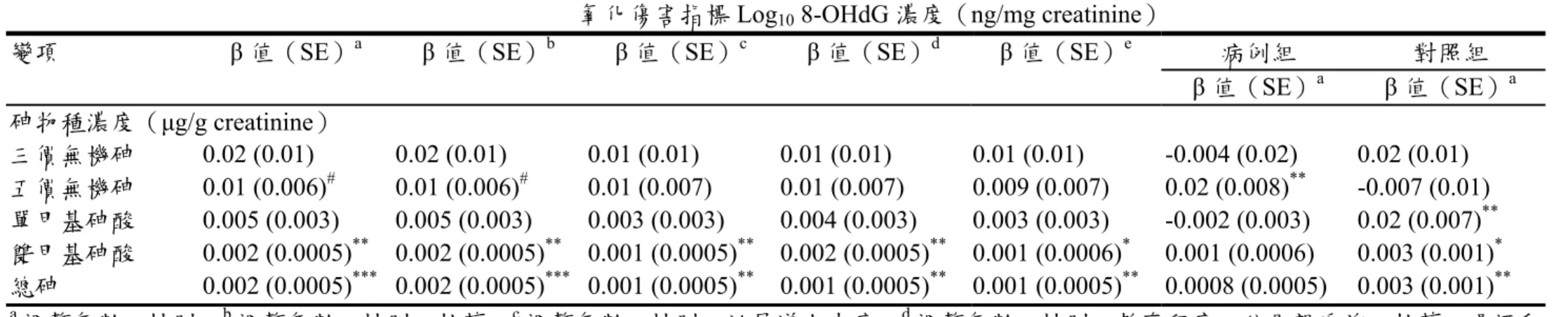
表13 尿液砷物種濃度與尿液中氧化傷害指標之多變項迴歸分析
氧化傷害指標Log10 8-OHdG 濃度(ng/mg creatinine)
病例組 對照組
變項 β 值(SE)a β 值(SE)b β 值(SE)c β 值(SE)d β 值(SE)e
β 值(SE)a β 值(SE)a 砷物種濃度(µg/g creatinine)
三價無機砷 0.02 (0.01) 0.02 (0.01) 0.01 (0.01) 0.01 (0.01) 0.01 (0.01) -0.004 (0.02) 0.02 (0.01) 五價無機砷 0.01 (0.006)# 0.01 (0.006)# 0.01 (0.007) 0.01 (0.007) 0.009 (0.007) 0.02 (0.008)** -0.007 (0.01) 單甲基砷酸 0.005 (0.003) 0.005 (0.003) 0.003 (0.003) 0.004 (0.003) 0.003 (0.003) -0.002 (0.003) 0.02 (0.007)**
雙甲基砷酸 0.002 (0.0005)** 0.002 (0.0005)** 0.001 (0.0005)** 0.002 (0.0005)** 0.001 (0.0006)* 0.001 (0.0006) 0.003 (0.001)* 總砷 0.002 (0.0005)*** 0.002 (0.0005)*** 0.001 (0.0005)** 0.001 (0.0005)** 0.001 (0.0005)** 0.0008 (0.0005) 0.003 (0.001)**
a調整年齡、性別 b調整年齡、性別、抽菸 c調整年齡、性別、泌尿道上皮癌 d調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒和
農藥 e調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒、農藥和泌尿道上皮癌
# 0.05 < p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001
表14 抽菸年數、抽菸包數和累積抽菸量與尿液中氧化傷害指標之多變項迴歸分析
氧化傷害指標Log10 8-OHdG 濃度(ng/mg creatinine)
病例組 對照組
變項 β 值(SE)a β 值(SE)b β 值(SE)c β 值(SE)d β 值(SE)e
β 值(SE)a β 值(SE)a 抽菸年數(年) -0.0002 (0.0007) -0.0003 (0.0007) -0.0005 (0.0008) -0.0008 (0.0008) -0.0009 (0.0008) 0.001 (0.001) -0.001 (0.0009) 抽菸包數(包/天) 0.006 (0.02) -0.003 (0.02) -0.004 (0.02) -0.02 (0.03) -0.02 (0.03) 0.07 (0.04)# -0.03 (0.03) 累積抽菸量f(包年數) -0.0004 (0.0006) -0.0006 (0.0006) -0.0007 (0.0006) -0.001 (0.0007) -0.001 (0.0007) 0.001 (0.001) -0.002 (0.0009)*
a b c d
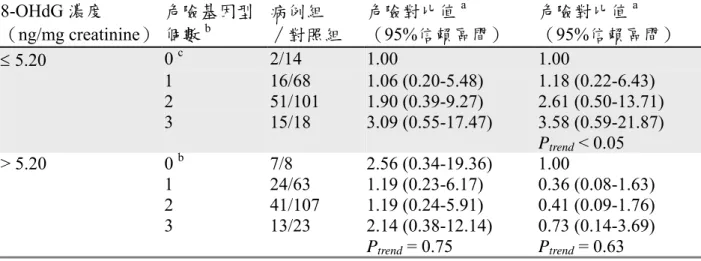
表15 尿液中氧化傷害指標和危險基因型個數與泌尿道上皮癌之交互作用 8-OHdG 濃度
(ng/mg creatinine)
危險基因型 個數b
病例組
/對照組
危險對比值a
(95%信賴區間)
危險對比值a
(95%信賴區間)
≤ 5.20 0 c 2/14 1.00 1.00
1 16/68 1.06 (0.20-5.48) 1.18 (0.22-6.43) 2 51/101 1.90 (0.39-9.27) 2.61 (0.50-13.71) 3 15/18 3.09 (0.55-17.47) 3.58 (0.59-21.87)
Ptrend < 0.05
> 5.20 0 b 7/8 2.56 (0.34-19.36) 1.00 1 24/63 1.19 (0.23-6.17) 0.36 (0.08-1.63) 2 41/107 1.19 (0.24-5.91) 0.41 (0.09-1.76) 3 13/23 2.14 (0.38-12.14) 0.73 (0.14-3.69)
Ptrend = 0.75 Ptrend = 0.63
a調整年齡、性別、教育程度、父母親氏族、抽菸、喝酒、農藥和總砷濃度
b p53 codon 72 基因型為 Arg/Pro+Pro/Pro、p21 codon 31 基因型為 Arg/Arg 及 CCND1 G870A 基因型為G/A+A/A
表16 危險因子個數與泌尿道上皮癌之相關性
變項
危險因子 個數
病例組
/對照組
危險對比值a
(95%信賴區間)
危險對比值b
(95%信賴區間)
抽菸狀態 0 10/52 1.00 1.00
無機砷百分比 1 48/140 1.71 (0.81-3.65) 1.64 (0.74-3.63) p21 codon 31 基因型 2 48/89 2.80 (1.29-6.05)** 2.32 (1.02-5.31)* 8-OHdG 濃度 3 30/54 2.85 (1.25-6.51)* 2.38 (0.96-5.90)# 4 12/11 5.56 (1.89-16.34)** 3.75 (1.17-12.07)*
Ptrend < 0.001 Ptrend < 0.05
抽菸狀態 0 3/48 1.00 1.00
單甲基砷酸百分比 1 41/156 4.13 (1.22-13.94)* 3.48 (1.01-12.04)* p21 codon 31 基因型 2 51/76 10.61 (3.09-36.43)*** 9.65 (2.71-34.34)***
8-OHdG 濃度 3 37/63 9.53 (2.73-33.22)*** 6.94 (1.92-25.12)**
4 10/11 14.74 (3.41-63.72)*** 9.73 (2.12-44.59)**
Ptrend < 0.001 Ptrend < 0.001
抽菸狀態 0 3/44 1.00 1.00
二級甲基化指標 1 33/127 3.66 (1.07-12.56)* 3.34 (0.95-11.71)# p21 codon 31 基因型 2 51/85 8.37 (2.44-28.71)*** 7.33 (2.06-26.09)**
8-OHdG 濃度 3 40/69 8.16 (2.34-28.42)** 6.88 (1.89-25.00)**
4 14/10 19.48 (4.60-82.54)*** 12.44 (2.78-55.76)**
Ptrend < 0.001 Ptrend < 0.001
危險因子包括抽菸、無機砷百分比> 4.28、單甲基砷酸百分比> 6.06、二級甲基化指標≤ 10.9、
p21 codon 31 基因型為 Arg/Arg 及氧化傷害指標 8-OHdG 濃度> 5.20(ng/mg creatinine)
a調整年齡、性別
b調整年齡、性別、教育程度、父母親氏族、喝酒、農藥
Reference List
Betticher DC, Thatcher N, Altermatt HJ, Hoban P, Ryder WD, Heighway J. 1995. Alternate splicing produces a novel cyclin D1 transcript. Oncogene 11: 1005-1011.
Chen F, Shi X. 2002. Intracellular signal transduction of cells in response to carcinogenic metals.
Crit Rev Oncol Hematol 42: 105-121.
Chen YC, Su HJ, Guo YL, Hsueh YM, Smith TJ, Ryan LM, et al. 2003. Arsenic methylation and bladder cancer risk in Taiwan. Cancer Causes Control 14: 303-310.
Chiou CC, Chang PY, Chan EC, Wu TL, Tsao KC, Wu JT. 2003a. Urinary
8-hydroxydeoxyguanosine and its analogs as DNA marker of oxidative stress: development of an ELISA and measurement in both bladder and prostate cancers. Clin Chim Acta 334: 87-94.
---. 2003b. Urinary 8-hydroxydeoxyguanosine and its analogs as DNA marker of oxidative stress: development of an ELISA and measurement in both bladder and prostate cancers. Clin Chim Acta 334: 87-94.
Chiou HY, Chiou ST, Hsu YH, Chou YL, Tseng CH, Wei ML, et al. 2001. Incidence of
transitional cell carcinoma and arsenic in drinking water: a follow-up study of 8,102 residents in an arseniasis-endemic area in northeastern Taiwan. Am J Epidemiol 153: 411-418.
Cooke MS, Evans MD, Herbert KE, Lunec J. 2000. Urinary 8-oxo-2'-deoxyguanosine--source, significance and supplements. Free Radic Res 32: 381-397.
Fan R, Wu MT, Miller D, Wain JC, Kelsey KT, Wiencke JK, et al. 2000. The p53 codon 72 polymorphism and lung cancer risk. Cancer Epidemiol Biomarkers Prev 9: 1037-1042.
Habuchi T, Kinoshita H, Yamada H, Kakehi Y, Ogawa O, Wu WJ, et al. 1994. Oncogene amplification in urothelial cancers with p53 gene mutation or MDM2 amplification. J Natl Cancer Inst 86: 1331-1335.
Helbock HJ, Beckman KB, Ames BN. 1999. 8-Hydroxydeoxyguanosine and 8-hydroxyguanine as biomarkers of oxidative DNA damage. Methods Enzymol 300: 156-166.
Hsueh YM, Chiou HY, Huang YL, Wu WL, Huang CC, Yang MH, et al. 1997. Serum beta-carotene level, arsenic methylation capability, and incidence of skin cancer. Cancer
Huang SP, Wu WJ, Chang WS, Wu MT, Chen YY, Chen YJ, et al. 2004. p53 Codon 72 and p21 Codon 31 Polymorphisms in Prostate Cancer. Cancer Epidemiol Biomarkers Prev 13: 2217-2224.
Hunter T, Pines J. 1994. Cyclins and cancer. II: Cyclin D and CDK inhibitors come of age. Cell 79: 573-582.
Kessel M, Liu SX, Xu A, Santella R, Hei TK. 2002. Arsenic induces oxidative DNA damage in mammalian cells. Mol Cell Biochem 234-235: 301-308.
Kong S, Amos CI, Luthra R, Lynch PM, Levin B, Frazier ML. 2000. Effects of cyclin D1 polymorphism on age of onset of hereditary nonpolyposis colorectal cancer. Cancer Res 60:
249-252.
Kong S, Wei Q, Amos CI, Lynch PM, Levin B, Zong J, et al. 2001. Cyclin D1 polymorphism and increased risk of colorectal cancer at young age. J Natl Cancer Inst 93: 1106-1108.
Le Marchand L, Seifried A, Lum-Jones A, Donlon T, Wilkens LR. 2003a. Association of the cyclin D1 A870G polymorphism with advanced colorectal cancer. JAMA 290: 2843-2848.
---. 2003b. Association of the cyclin D1 A870G polymorphism with advanced colorectal cancer.
JAMA 290: 2843-2848.
Li YJ, Laurent-Puig P, Salmon RJ, Thomas G, Hamelin R. 1995. Polymorphisms and probable lack of mutation in the WAF1-CIP1 gene in colorectal cancer. Oncogene 10: 599-601.
Lin S, Cullen WR, Thomas DJ. 1999. Methylarsenicals and arsinothiols are potent inhibitors of mouse liver thioredoxin reductase. Chemical Research in Toxicology 12: 924-930.
Mousses S, Ozcelik H, Lee PD, Malkin D, Bull SB, Andrulis IL. 1995. Two variants of the CIP1/WAF1 gene occur together and are associated with human cancer. Hum Mol Genet 4:
1089-1092.
Obaya AJ, Sedivy JM. 2002. Regulation of cyclin-Cdk activity in mammalian cells. Cell Mol Life Sci 59: 126-142.
Petrick JS, Ayala-Fierro F, Cullen WR, Carter DE, Vasken AH. 2000. Monomethylarsonous acid (MMA(III)) is more toxic than arsenite in Chang human hepatocytes. Toxicology & Applied Pharmacology 163: 203-207.
Proctor AJ, Coombs LM, Cairns JP, Knowles MA. 1991. Amplification at chromosome 11q13 in transitional cell tumours of the bladder. Oncogene 6: 789-795.
---. 2000b. Genetic alterations and biological pathways in human bladder cancer pathogenesis.
Urol Oncol 5: 191-203.
Saito S, Yamauchi H, Hasui Y, Kurashige J, Ochi H, Yoshida K. 2000. Quantitative determination of urinary 8-hydroxydeoxyguanosine (8-OH-dg) by using ELISA. Res Commun Mol Pathol Pharmacol 107: 39-44.
Schwerdtle T, Walter I, Mackiw I, Hartwig A. 2003. Induction of oxidative DNA damage by arsenite and its trivalent and pentavalent methylated metabolites in cultured human cells and isolated DNA. Carcinogenesis 24: 967-974.
Styblo M, Serves SV, Cullen WR, Thomas DJ. 1997. Comparative inhibition of yeast glutathione reductase by arsenicals and arsenothiols. Chem Res Toxicol 10: 27-33.
Thomas M, Kalita A, Labrecque S, Pim D, Banks L, Matlashewski G. 1999. Two polymorphic variants of wild-type p53 differ biochemically and biologically. Mol Cell Biol 19: 1092-1100.
Wang L, Habuchi T, Takahashi T, Mitsumori K, Kamoto T, Kakehi Y, et al. 2002. Cyclin D1 gene polymorphism is associated with an increased risk of urinary bladder cancer. Carcinogenesis 23:
257-264.
Wood SG, Gedik CM, Collins AR. 2000. Controlled oxidation of calf thymus DNA to produce standard samples for 8-oxodeoxyguanosine analysis; effects of freeze-drying, storage and hydrolysis conditions. Free Radic Res 32: 327-332.
Xiong Y, Hannon GJ, Zhang H, Casso D, Kobayashi R, Beach D. 1993. p21 is a universal inhibitor of cyclin kinases. Nature 366: 701-704.
Yamauchi H, Aminaka Y, Yoshida K, Sun G, Pi J, Waalkes MP. 2004. Evaluation of DNA damage in patients with arsenic poisoning: urinary 8-hydroxydeoxyguanine. Toxicol Appl Pharmacol 198:
291-296.
Yin B, Whyatt RM, Perera FP, Randall MC, Cooper TB, Santella RM. 1995. Determination of 8-hydroxydeoxyguanosine by an immunoaffinity chromatography-monoclonal antibody-based ELISA. Free Radic Biol Med 18: 1023-1032.
行政院國家科學委員會補助國內專家學者出席國際學術會議報告
95 年 4 月 30 日
報告人姓名
薛玉梅
服務機構及職稱
臺北醫學大學
醫學系公共衛生學科 會議
時間 地點
2006.4.1-4.6.
Washington Convention Center, Washington, DC, USA
本會核定 補助文號
NSC-94-2314-B038-023 會議
名稱
(中文)第九十七屆美國癌症研究學會年會
(英文) American Association for Cancer Research 97th Annual Meeting 發表
論文 題目
(中文) 血清微量營養元素及砷甲基代謝能力與泌尿道上皮細胞癌之相關性研 究
(英文) The Relationship among Plasma Micronutrients, Antioxidant Enzyme Genetic Polymorphism, Arsenic Methylation Capability and Urothelial Carcinoma
報告內容應包括下列各項:
一、 參加會議經過
「第九十七屆美國癌症研究學會年會」於民國九十五年四月一日至四月五 日在美國 Washington Convention Center, Washington, DC 舉行。此會議由美國 癌症研究學會主辦。參加會議人士來自世界各地醫師、專家、學者,共計約 10000 人與會。
本人與公衛所博士班學生鍾季容與公衛系主任邱弘毅教授及中研院生醫所 李德章教授一行十四人於三月三十一日早上間八時二十分搭乘西北班機,三 月三十一日晚間約十二點,抵達華盛頓,住進 Golden Tulip Bethesda Court Hotel。四月一日至會場報到,領了會議議程日程表與會議摘要論文集。本次 會議內容針對細胞與分子生物學(cellular and molecular biology)、腫瘤生物學 (tumor biology)、致癌過程(carcinogenesis)、化學(chemistry)、臨床試驗(clinical research)、內分泌學(endocrinology)、流行病學(epidemiology)、實驗與分子治 療(experimental and molecular therapeutics)、免疫學(immunology)、預防研究 (prevention research)等領域分別進行討論。
本人於四月四日上午八點以海報發表論文,題目為” The Relationship among Plasma Micronutrients, Antioxidant Enzyme Genetic Polymorphism, Arsenic
Methylation Capability and Urothelial Carcinoma” 論文。發表時,與會多位學者 極表興趣,並與本人進行廣泛討論與交換意見。美國學者看到本人論文中在非
附件三
美國環境保護署目前也在內蒙古砷暴露地區,進行調查飲用地下含砷水所引起 的人體健康危害,故本研究發表時被詢問臺灣砷研究經驗獲極高的肯定。與會 中並與長期合作夥伴哈佛大學 David Christiani 教授針對砷代謝能力指標測定 問題交換意見。此外,此會議更邀請許多儀器廠商與書商展示最新儀器與新 書,讓與會者獲得各領域新知。一行人於四月六日中午十二時二十分搭乘西北 航空公司班機經底特律、大阪返回台灣,於四月七凌晨二點三十分左右安全返 抵國門。
二、 與會心得
參加本次國際會議,使筆者有機會與世界各國從事流行病學研究的知 名學者專家交換意見,對未來泌尿細胞癌研究工作有極大的助益。在流行 病學領域研討會中,得知目前生物標記在探討疾病病因上有很大助益。大 部分研究都在探討基 DNA 修復基因多形性、環境暴露與癌症之關係。此 外,並探討不同突變點的 SNP 之 haplotype 與癌症之關係; 強調基因與基因 之交互作用與基因與環境暴露之交互作用。此外並討論如何利用生物資訊 探討大量基因體與蛋白質體學資料與癌症之關係。此次會議中感觸最深為 國外研究都是團體戰(team work),利用多中心(multicenter)收集研究對象,
所以癌症病人動輒上千或甚至上萬人,國內應有類似的合作群體能共同收 集癌症病患,以大樣本探討基因與環境因子之機制,才能與國外競爭,並 能在國際盛名之期刊雜誌投稿順利。
三、 考察參觀活動(無是項活動者省略)
在每天五點起床,搭乘地鐵約四十分鐘,七時趕至會場聽 sunrise section 至 晚間六點半,辛苦的參與三天之研討會,獲新知洗禮後,與博士生至 National mold、國會、華盛頓紀念碑、傑佛遜紀念堂,放鬆心情旅遊並欣賞盛開的櫻花 及瞭解美國的風土人情。
四、 建議
過去數十年台灣烏腳病盛行地區無機砷健康危害研究,有關癌症危害結果備
受國際重視,美國環境保護局並以台灣的研究結果訂定水質標準。目前全世界
尚有許多國家如美國、中國大陸、日本、德國、阿根廷、墨西哥、印度、孟加
拉、智利等均有相同之砷暴露問題。希望政府能大力支持無機砷致病機制的研
究,並鼓勵整合大型研究,收集大樣本並將分子生物醫學之技術應用在台灣地
區研究,以便能傳承過去癌症流行病學研究之光榮歷史領先其他國家。並以臺
灣經驗分享於世界其他國家,進而對世界各地日益增多地下水砷污染及砷誘發
之健康危害事件有實質的幫助。
“The Relationship among Plasma Micronutrients, Antioxidant Enzyme Genetic Polymorphism, Arsenic Methylation Capability and Urothelial
Carcinoma”
Y Y.M. Hsueh1, Y.T. Chen2, H.J. Tsai1, C.J. Chung3, Y.K. Huang2, Y.S. Pu4, C.J. Chen5.
1Department of Public Health, School of Medicine, Taipei Medical University, Taipei, Taiwan,
2Graduate Institute of Medical Sciences, Taipei Medical University, Taipei, Taiwan, 3School of Public Health, Taipei Medical University, Taipei, Taiwan, 4Department of Internal Medicine, National Taiwan University, Taipei, Taiwan, and College of Medicine and 5Graduate Institute of Epeidemiology, College of Public Health, National Taiwan University, Taipei, Taiwan.
Abstract
This study is to examine the potential role and interaction among the antioxidant enzyme polymorphism, plasma micronutrient, arsenic methylation capability, cigarette smoking, oxidative damage 8-OHdG levels and urothelial carcinoma (UC). There were 152 patients with
pathologically proven UC were recruited from the Department of Urology, National Taiwan University Hospital (NTUH) between September 2002 and May 2005. Age and gender matched 158 study subjects without UC were collected from adult health examination at Taipei Municipal WanFang Hospital. Well-trained interviewers did the standardized personal interviews for study subjects who gave their consent based on structural questionnaire and recruited their blood and urine samples. Obtained information including the demographic characteristics, cigarette smoking and alcohol drinking habits, occupational exposure history, and personal and family disease history. DNA was extracted from buffy coat to analyze the manganese superoxide dismutase (MnSOD) and catalase polymorphism utilizing polymerase chain reaction (PCR) and the restriction fragment length polymorphism (RFLP). The urinary concentration of 8-OHdG was assayed by enzyme-linked immunosorbent assays (ELISA). Urine samples were examined by high-performance liquid chromatography (HPLC) to separate arsenite (AsIII), arsenate (AsV), monomethylarsonic acid (MMA), and dimethyarsinic acid (DMA) and then quantified by hydride generator combined with atomic absorption spectrometry. Plasma samples were examined by HPLC to analyze micronutrients (retinol, α-tocopherol, β-carotene and lycopene). We found that arsenic methylation capability in case group was significantly worse than control group. We also found the α-tocopherol concentration was inversely related to UC risk. The lower α-tocopherol and the lower secondary methylation capability was the high UC risk. Cigarette smoker with
CI 4.78-58.21). The relationship among MnSOD and catalase genetic polymorphisms and 8-OHdG and UC will be presented in the conference.
Introduction
In Taiwan, urothelial carcinoma (UC) was ranked as the 7th and 10th most common cancer for males and for both sexes, respectively in 2000. The incidence rates of UC have been
progressively increased in the past decades in Taiwan; with the age-specific rates for males and females in 2000 were 10.2 and 4.4 per 105, respectively. It was found a clear dose-response relationship between arsenic water levels and UC mortality and incidence in an arseniasis
endemic area in Taiwan. The capability to metabolize inorganic arsenic differs among individuals.
Whether individual capability of arsenic methylation affects risks of UC among subjects exposed to a previously accepted safe level (50 µg/L) of arsenic is an important issue. Endogenous
defense against ROS includes catalase, and superoxide dismutase (SOD). Micronutrients are antioxidant against ROS. To examine the potential role and interaction among the antioxidant enzymes genetic polymorphisms, plasma micronutrients, arsenic methylation capability, cigarette smoking, oxidative damage 8-OHdG levels and urothelial carcinoma (UC).
Material and Methods
Study Subjects and questionnaire interview
One hundred and forty-three patients with pathologically proven UC (age 24 to 93 years) were recruited from the Department of Urology, National Taiwan University Hospital (NTUH) between September 2002 and May 2004. Age and gender matched 143 control subjects without UC were collected from a hospital-based pool including those with benign diseases (benign prostatic hyperplasia, urolithiasis, urinary tract infection, voiding dysfunctions, etc) from the Department of Urology, NTUH, those receiving senior citizen health examination at Taipei Medical University Hospital and those receiving adult health examination at Taipei Municipal WanFang Hospital.
Well-trained personnel carried out the standardized personal interview that was based on a structured questionnaire. Information obtained included demographic and socioeconomic characteristics, consumption of alcohol, cigarette smoking, occupational and environmental exposure to possible carcinogens, chronic medication history, and personal and familial history of urological diseases. Study subjects who gave their informed consent were subjected to
Frozen urine samples were thawed at room temperature, dispersed by ultrasonic wave, filtered through Sep-Pak C18 column. An aliquot of 200 µL urine was used for separation of arsenic species by high performance liquid chromatography and was quantified by hydride generator-atomic absorption spectrometer (HG-AAS). Arsenic methylation capability was assessed by the percentages of various arsenic species, the primary methylation index (PMI) defined as the ratio between MMA and inorganic arsenic (AsIII + AsV) levels, and the secondary methylation index (SMI) defined as the ratio between DMA and MMA.
Determination of serum antioxidant micronutrient level
Levels of α-carotene, β-carotene, lycopene, α-tocopherol and retinol of serum samples will be measured by high performance liquid chromatography (HPLC) according to the procedure described previously (63). Analysis will be carried out by using reversed-phase HPLC (Hitachi), mobile phase will be methanol: acetonitrite: chloroform = 47: 48 :5, and multiwavelength monitoring. Retinol will be detected at 325 nm, α-tocopherol at 280 nm, and lycopene, α- and β-carotene at 466 nm. Serum samples for each case-control set will be thawed from -70℃
refrigerator in the dim light at room temperature and assayed on the same day to ensure that temporal variability in the laboratory assays would equally affect cases and controls. All laboratory personnel will be unaware of disease status of subjects whose serum samples were tested. In order to obtain reliable analytical result, strict quality control procedures, such as blank analysis, duplicate test, spiked analysis will be carried out.
MnSOD gene polymorphism assay
Genotyping of MnSOD polymophism (a T to C substitution in the mitochondria targeting sequence) was performed by PCR amplification procedure using the primer set of
5’-GCACCAGCAGGCAGCTGGCGCCGG-3’ and 5’-TGCGCGTTGATGTGAGGTTCCAG-3’.
The amplified products were digested with TurboTM NaeⅠ(Progema) and analyzed by
electrophoresis on a 10% polyacrylamide gel. The wild-type allele had no NaeⅠ site and was characterized by a 112 base pair(bp) fragment on gel. 90 and 22 bp fragments on gel
characterized the mutant allele. The heterozygous genotype had both alleles and was characterized by 112, 90 and 22 bp fragments.
Genotyping of catalase polymorphism (a C-to-T substitution of the C262T polymorphic site located on chromosome 11 p 13) was performed by PCR amplification following digestion with Sma I, and analyzed by 4% agarose gel electrophoresis as previously described (Forsberg et al., 2001). Two fragments of 155 and 30 bp were characterized as the wild-type allele and a 185-bp fragment as the mutant allele.
Data analyses and statistical methods
Student’s t test was used to compare the differences in urinary arsenic profile between cases and controls. Univariate logistic regression was performed to compare the distributions of gender, age, cigarette smoking history, the frequencies of alleles and genotypes between cases and
controls. Multivariate logistic regression analysis to adjust for age and cigarette smoking history was performed to calculate odds ratio (OR), and 95% confident interval (CI). SAS Version 8.2 was used for all statistical analyses.
Conclusion
Our study is shown that higher total arsenicals, inorganic arsenics and MMA% in cases than those in controls and the α-tocopherol concentration was inversely related to UC risk. After adjusting for other risk factors, study subjects who are cigarette smoker or have poor arsenic methylation capability with lower VitE or lycopene concentration had significantly higher UC risk. We did not find a relationship among MnSOD and catalase gene polymorphisms, 8-OHdG and UC risk.
Table 1. Sociodemographic characteristics, the MnSOD and catalase genotype distribution in UC cases and healthy controls
UC Cases
(n=152)
Control (n=158)
Adjusted OR a (95%CI) Age (Mean±SE) 63.6 ± 1.08 61.3 ± 1.11 1.01 (0.99-1.03) Sex (%)
Female 28.9 29.1 1.03 (0.63-1.68)
Educational level (%)
Elementary school and below 36.8 22.8 1.00
High school 40.2 39.3 0.62 (0.32-1.21) University and above 23.0 37.9 0.38 (0.20-0.72) Smoking (%)
Never 47.4 59.5 1.00
Former 37.5 26.6 2.12 (1.16-3.88)
Current 15.1 13.9 1.68 (0.81-3.48)
Alcohol (%)
Table 2. Distribution of urinary arsenic index, 8-OHdG and micronutrients concentrations in UC patients and health controls
No. UC Cases Control P value Arsenic species
(μg/g creatinine)
Total 152/158 38.31 ± 3.29 26.01 ± 1.33 < 0.01 As3+ 152/158 0.86 ± 0.10 0.64 ± 0.09 0.11 As5+ 152/158 1.27 ± 0.16 0.60 ± 0.10 < 0.01 MMA% 152/158 13.03 ± 1.05 9.72 ± 0.65 < 0.01 DMA% 152/158 80.27 ± 1.17 85.26 ± 0.82 < 0.01 8-OHdG
(ng/mg Creatinine) 81/81 6.52± 0.51 5.99 ± 0.42 0.42 Micronutrients (μg/dL)
VitA 152/158 106.8 ± 4.2 92.0 ± 2.0 < 0.01 VitE 152/158 1061.8 ± 54.2 1174.4 ± 38.1 0.09 Lycopene 152/158 9.3 ± 0.9 12.8 ± 1.0 0.01 β-carotene 152/158 26.0 ± 2.4 26.5 ± 2.1 0.87