中國醫藥學大學
醫務管理學研究所碩士論文 編號:IHAS-344
口腔癌患者之存活分析與其影響因素
- 以中部某醫學中心為例
Survival Analysis of Oral Cancer and its Affecting Factors in a Medical Center of Central Taiwan
指導教授:蔡 文 正 博士 研 究 生:劉 時 安 撰
中華民國九十四年七月
摘 要
目的:本研究之目的有三:統計中部某醫學中心口腔癌患者之存活狀態,並 分析死亡族群與存活族群間之差異,同時探討社會人口學因素與口腔癌患者 預後之關係。
方法:本研究以中部某醫學中心為對象,收集自民國八十四年三月至民國九十 一年十二月底,曾因口腔癌之診斷至個案醫院住院之病例,進行存活分析。研 究採病歷回溯性分析,統計則包括描述性統計、雙變項分析、Kaplan-Meier 之 存活分析、及 Cox proportional hazard model 來探討社會人口學因素與口腔癌患
者存活之關係。計有 1,612 位患者曾於該期間因口腔癌之診斷住院,排除紀錄
不完整、在外院接受第一次治療、未完成療程等病例,結果共有 1,118 位患者
進入本研究之分析。
結果:男性佔絕大多數(1,042 例, 93.2%),平均年齡為 51.9 歲(+11.81 歲)。
Kaplan-Meier 存活分析顯示整體五年存活率為 59.79%,第一、二、三、四期 之五年存活率分別為 79.84%、67.74%、54.69%、及 44.73%(Log Rank test=102.90, p <0.001)。Cox proportional hazard model 結果顯示,在控制其他變項後,
社會人口學因素當中,無宗教信仰者,較有宗教信仰個案之死亡相對危險性 為 2.169(95%信賴區間:1.734 – 2.713, p < 0.001),單身較結婚個案之死亡相 對危險性為 1.439(95%信賴區間:1.052 – 1.967, p = 0.023)。其他顯著相關因 素還包括:年齡大於 60 歲(死亡相對危險性:1.570,95%信賴區間:1.082–
2.279, p = 0.018)、腫瘤位於顎區(死亡相對危險性:2.673,95%信賴區間:
1.329 – 5.375, p = 0.006)、治療前身高體重指數小於 22.8 kg/M2(死亡相對危 險性:1.403,95%信賴區間:1.131 – 1.741, p = 0.002)、治療前血中白蛋白濃 度小於 4 g/dl(死亡相對危險性:1.284,95%信賴區間:1.027 – 1.605, p = 0.028)、腫瘤大於 3.5 公分(死亡相對危險性:1.607,95%信賴區間:1.288 – 2.005, p < 0.001)、腫瘤復發(死亡相對危險性:2.352,95%信賴區間:1.818 –
3.042, p < 0.001)、手術邊緣不乾淨(死亡相對危險性:1.762,95%信賴區間:
1.383 – 2.246, p = 0.024)、術後產生併發症(死亡相對危險性:1.351,95%信 賴區間:1.054 – 1.733, p = 0.018)、病理報告有肌肉侵犯(死亡相對危險性:
1.688,95%信賴區間:1.282 – 2.222, p < 0.001)、淋巴囊外擴散(死亡相對危 險性:4.812,95%信賴區間:3.155 – 5.542, p < 0.001)等為預後不良之相關 因子。
結論:本研究針對 1,118 例口腔癌患者進行回溯性、橫斷式之存活分析,發現
除了臨床特質對預後有影響外,社會人口學特質也存在顯著的相關,所以醫師 除了臨床照護之外,對於患者之心靈層面也宜多加留意。未來將以世代研究之 方式,更進一步釐清社會人口學特質與口腔癌患者之預後相關性,以作為臨床 醫師照護患者之參考,進而期望能提高口腔癌患者之存活機會。
關鍵字:口腔癌,存活分析,社會人口學因素
致謝
本來以為專科醫師執照是人生的最後一次試煉,怎麼也沒料到還有機會 拿到碩士學位,甚至進一步攻讀博士學位。總覺得人生是不斷的考驗,就看 您願不願意面對;想不想去挑戰自己。在研究所求學的過程當中,也曾反問 自己何苦如此?看人家日子過得輕鬆愜意,自己就像蠟燭兩頭燒,放棄休息 的時間,也犧牲與家人相聚的光陰,只是這些疑慮在此時已經化為烏有,我 也更進一步地肯定自己:“Yes, I can!”
要感謝的人很多,首先當然是指導教授蔡文正老師,雖然自己臨床上的 研究也進行多年,但是盲點還是不少,有賴蔡老師從旁一一予以指正及協助,
才得以完成這不可能的任務。另外也要感謝戴志展所長,他不但是耳鼻喉科 界的前輩,同時還是我的口試委員,給予學生諸多建議。還有健康管理學院 的龔佩珍老師,在口試的過程中,提供不少關於統計方面的獨到見解,也著 實讓學生得到不少啟示。而在資料整合的過程中,有賴怡如學姐和凱平學長 的協助建檔及統計分析,在此一併致謝。
同學間的鼓勵協助,也是助我渡過兩年的精神支柱,柏巖、昭佾、秀美、
文吉、瑋貞、麒丞、春米、蜀雯、味娟、美礽、瓊玉、曾醫師、白醫師、陸 醫師、秀花、美月、珮嘉、婷雯、盈偵、名毅、俊華、惠珊、瑛琳、惠娟、
雪萍、盟文、怡君,謝謝您們陪我走過這兩年。
最後要感謝上帝賜給我這麼一位任勞又任怨的老婆――筑清,將家中大 小雜事一肩扛起,全心全力照顧那三個有點煩又有點可愛的濰維、娣伊、娣 羽,讓我毫無後顧之憂,得以全力衝刺,達陣成功。
其實要感謝的人還有很多,不及一一詳述,在此向您們說謝謝,您們的 幫忙,我永遠銘記在心,謝謝。
時安 謹誌 2005.06
Abstract
Purpose: This study aims to determine the survival rate of oral cancer patients
treated in a medical center of central Taiwan. Furthermore, this study wants to discover the differences between the death group and the survival group. Finally, this study attempts to investigate if socio-demographic factors will influence the survival of oral cancer patients.
Methods: From March 1995 to December 2002, there were total 1,612 patients
admitted to cased hospital diagnosed as having oral cancer. Over 1,600 charts records were retrospectively reviewed. Statistical methods included descriptive statistics, bivariate analyses, Kaplan-Meier survival analyses and Cox proportional hazard models for investigating the relationship between socio-demographic factors and survival of oral cancer patients. After excluding those with inadequate chart records, those who had treatment in other hospitals or didn’t finish therapeutic protocol, there were 1,118 patients chosen for the final analyses.
Results: Males accounted for 93.2% (N=1042) of the oral cancer patients and the
average age was 51.9 years (+ 11.81 years). Using Kaplan-Meier survival analysis, the overall 5-year survival rate was 59.79%. The 5-year survival rates for stage I, II, III and IV diseases were 79.48%, 67.74%, 54.69% and 44.73%, respectively (Log Rank test=102.90, p <0.001). Cox proportional hazard model revealed that those without religious beliefs tended to have higher death probability than those who had religious beliefs after controlling other variables (Relative risk (RR): 2.169, 95% CI:
1.734-2.713, p < 0.001). In addition, those who were single, widow/widower or separated had a poorer prognosis than those who were married (RR: 1.439, 95% CI: 1.052-1.967, p
= 0.023). Further significant factors included: age more than 60 years old (RR: 1.570,
95% CI: 1.082-2.279, p = 0.018), a tumor located over palate (RR: 2.673,95% CI:
1.329-5.375, p = 0.006), pre-treatment body mass index less of than 22.8 kg/M2 (RR:
1.403, 95% CI: 1.131-1.741, p = 0.002), pre-treatment serum albumin level of less than 4 g/dl (RR: 1.284, 95% CI: 1.027 -1.605, p = 0.028), tumor size larger than 3.5 cm (RR:
1.607, 95% CI: 1.288-2.005, p < 0.001), tumor recurrence or distal metastasis (RR:
2.352, 95% CI: 1.818-3.042, p <0.001), inadequate surgical margin (RR: 1.762,95% CI:
1.383-2.246, p < 0.001), development of post-operative complications (RR: 1.351, 95%
CI: 1.054-1.733, p = 0.018), tumor invaded muscular layer (RR: 1.688, 95% CI:
1.282-2.222, p < 0.001), extra-capsular spread of lymph node (RR: 4.812, 95% CI:
3.155-5.542, p < 0.001).
Conclusion: This study retrospectively reviewed 1,118 oral cancer patients and found that
apart from clinical features, socio-demographic factors also significantly influenced the survival of oral cancer patients. Therefore care providers should take socio-psychological issues into consideration aside from ordinary clinical health care. Further investigation with a prospective cohort study is needed to further clarify the relationship between socio-demographic factors and the survival of oral cancer patients.
Key Words: Oral cancer, survival analysis, socio-demographic factor
Tables of Contents
Chapter 1 Introduction
Session 1 Background 1 Session 2 Statements of Problems 1 Session 3 Research Questions 2 Session 4 Research Objectives 3 Chapter 2 Literature Review 5 Chapter 3 Research Methods 21
Session 1 Research Structure 21 Session 2 Sample and Data Sources 21 Session 3 Measurement 23 Session 4 Analytical Methods 25
Chapter 4 Results 26
Chapter 5 Discussion 36
Chapter 6 Conclusion and Recommendations 40 Chapter 7 Research Limitations 41
References 75
List of Tables
2-1 Mortality rate of oral cavity cancer in males and betel nut
production in Taiwan 42
2-2 Accumulative data from several large-scale studies in the Taiwan area 43 2-3 Tumor Node Metastasis (TNM) staging group 44 3-1 Operational definitions of variables 23 4-1 Descriptive analyses of oral cancer patients 45 4-2 Descriptive analyses of oral cancer patients (Continuous variables) 49 4-3 Bivariate analyses of oral cancer patients 50 4-4 Comparison of continuous variables between death and survival group 54 4-5 Kaplan-Meier survival analyses 55 4-6 Cox proportional hazard model 59
List of Figures
2-1 Five-year, observed survival by “combined” AJCC stage for squamous cell carcinoma of the oral cavity, 1985-1991 61
3-1 Research structure 22
4-1 Overall survival curve of oral cancer patients in Taichung Veteran
General Hospital 62
4-2 Survival curve by tumor stage 63 4-3 Survival curve by marital status 64 4-4 Survival curve by religious belief 65 4-5 Survival curve by occupations 66 4-6 Survival curve by the presence of post-operative complication 67 4-7 Survival curve by the status of surgical margin 68 4-8 Survival curve by the status of bony invasion 69 4-9 Survival curve by the status of muscle invasion 70 4-10 Survival curve by histological grading 71 4-11 Survival curve by the presentation of neck metastasis 72 4-12 Survival curve by the presentation of extra-capsular spread in
those with neck metastasis 73 4-13 Survival curve by the presence of recurrence or distal metastasis 74
Chapter 1 Introduction
Session 1 Background
According to the statistical data from the Department of Health of the Executive Yuan of Republic of China, malignant tumors became the leading cause of death since 1982 (1). Among all the malignant tumors, oral cancer turned out to be in the top 10 forms of cancer in Taiwan area since 1991. In addition, over 90%
of those who died of oral cancer were male patients. In 2003, another report from Bureau of Health Promotion, Department of Health, revealed that the death rate of oral cancer (that is, ICD-9 of 140, 141, 143 to 146, 148, 149) ranked 7th in the top 10 types of cancer in Taiwan area. Furthermore, the crude death rate of oral cancer in male was 14.98 per 100,000 persons; ranked the 4th in the top 10 cancers in males (2). Also, the death rate of oral cancer was the most rapid growing one among other cancers (1). It increased up to 1.4 times when compared with 10 years ago. Thus, oral cancer became one of the focusing issues of public health in Taiwan.
Session 2 Statements of Problems
I. Oral Cancer
No amazing progress in the management of oral cancer can be noted in recent years. Simple surgical excision or radiotherapy is enough for oral cancer of early stages. In oral cancer of the late stage, a combination therapy such as, surgical excision with post-operative radiotherapy or induction chemotherapy with surgical excision, was suggested. Although better combinations of local-regional treatment modalities have improved the quality of life after diagnosis, the relative 5-year
survival rate of 30-50% has not changed much over the years (3). Some authors tried induction chemotherapy with 5-FU, cisplatin, followed by wide surgical excision and post-operative radiotherapy in order to improve the survival rate of the late stage oral cancer. Although the reported 5-year survival rate reached 80% (4), it still needs further comprehensive study to confirm the results.
II. The Prognosis of Oral Cancer Patients
In the assessment of the prognosis of oral cancer patients, the most popular one is the cancer staging system proposed by the American Joint Committee on Cancer (AJCC). Poor prognosis is anticipated when the stage is higher. Other prognostic factors have been proposed including: excessive tumor volume, histo-pathological feature, the presence of post-operative complications, involvement of bone cortex, number of cervical lymph nodes involved, albumin concentration in the serum, and special gene presentation. However, those were all judging from the clinical characteristic and few articles talk about the socio-demographic issues.
Session 3 Research Questions
There are some differences between Asian and Caucasian in oral cancers. First, betel nut chewing has a close relationship with oral cancer in Asians whereas sunshine, tobacco smoking and chewing are predisposing factors of oral cancer in Caucasians. Second, the most common sites of oral cancer in Asians are buccal mucosa and anterior tongue region because of betel nuts chewing. On the other hand, the most common sites of oral cancer in Caucasians are the lips and tongue region.
Since differences exist between Asians and Caucasians in racial, geographic,
traditional aspect, relevant predictive factors in Caucasians that were published in previous studies are not necessarily suitable for Asians. Furthermore, the definition of oral cavity cancer in the cancer registry of the Department of Health of the Executive Yuan of Republic of China includes oral cavity cancer, oropharyngeal caner, and hypopharyngeal cancer (ICD-9: 140, 141, 143, 144, 145, 146, 148, 149) whereas most studies include only oral cavity cancer (ICD-9: 140, 141, 143, 144, 145). So some head and neck surgeons (5) suggested oral cancer to represent oral cavity cancer together with oropharyngeal cancers because of their adjacent anatomical association.
To our knowledge, most studies about survival analysis of oral cancer focus on clinical issues, such as Tumor-Node-Metastasis (TNM) staging, the presence of cervical lymph node, impact of special genes in the prediction of survival rate etc.
However, fewer studies discuss socio-demographic issues such as, marital status, religion, occupation, and education level on the impact of oral cancer survival.
Session 4 Research Objectives
1. Analyze the survival condition of oral cancer patients in a medical center of central Taiwan.
Using the Kaplan-Meier method, this study wants to determine the 5-year survival rate of oral cancer patients who had completed the therapeutic protocols in cased hospital.
2. Examine the differences between the death group and the survival group.
Using biraviate analyses, this study aims to determine if there any difference existing between the death group and the survival group in socio-demographic factors, personal characteristics, related history, cancer
related features, or laboratory data.
3. Investigate if the socio-demographic factors would influence the survival status.
Apart from the Kaplan-Meier survival analyses, this study uses the Cox proportional hazard model to examine if socio-demographic factors such as marital status, religion, occupation, and education level will influence the survival status after adjusted for other variables.
Chapter 2 Literature Review
There are two components to be discussed in the literature review. First is the introduction of oral cancer. The other is the relevant factors in the prognosis of oral cancer patients.
Session 1 Introduction of Oral Cancer
1. Anatomical Structure of Oral Cavity
The oral cavity extends from the skin-vermilion junction of the lips to the junction of the hard and soft palate above and to the line of circumvallate papillae below and is divided into the lips, buccal mucosa, upper and lower alveolar ridges, retromolar trigone, floor of the mouth, hard palate and anterior two thirds of the tongue.
The lips begin at the junction of the vermilion border with the skin and form the anterior boundary of the oral vestibule. In addition, the lips include only the vermilion surface, or that portion of a lip that comes into contact with the opposing lip.
The buccal mucosa includes the entire membrane lining of the interior surface of the cheek and lips, from the opposing lip’s line of contact to the pterygomandibular raphe posteriorly and, to the line of attachment of the alveolar ridge mucosa above and below. Furthermore, the buccal mucosa forms the lateral wall of the oral cavity.
The alveolar ridges include the alveolar processes of the mandible and maxilla and their mucosal covering that, in the case of the lower alveolar ridge, extend from the line of attachment of mucosa in the buccal gutter to the line of free
mucosa in the floor of the mouth. Posteriorly, the lower alveolar ridge’s mucosa extends to the ascending ramus of the mandible. The upper alveolar ridge’s mucosa extends from the line of attachment of mucosa in the upper buccal gutter to the junction of the hard palate. Its posterior margin is the upper end of the pterygopalatine arch.
The retromolar trigone is the attached gingiva overlying the ascending ramus of the mandible. The distal surface of the last lower molar forms the base of this triangular area, and its apex terminates at the maxillary tuberosity. The upward extension of the oblique line of the mandible to the coronoid process forms the triangle’s lateral side, and a line connecting the distal lingual cusp of the last molar and the coronoid process forms the medial side. The triangle’s base is continuous laterally with the gingivobuccal sulcus and medially with the gingivolingual sulcus.
The triangle’s lateral side is continuous with the buccal mucosa, and the medial side blends into the anterior tonsillar pillars.
The hard palate is a semilunar area consisting of mucous membranes covering the horizontal laminae of the palatine bones. The upper alveolar ridge partly surrounds the hard palate, which extends from the inner surface of the superior alveolar ridge to the posterior edge of the palatine bone.
The floor of the mouth is a crescent-shaped region of mucosa overlying the mylohyoid and hyoglossus muscles, extending from the inner aspect of the lower alveolar ridge to the underside of the anterior two thirds of the tongue. Posteriorly, the floor of the mouth is continuous with the base of the anterior tonsillar pillar, and anteriorly the frenulum of the tongue divides it into two sides.
The anterior two thirds of the tongue, known as the oral tongue or mobile tongue, are considered part of the oral cavity. The oral tongue is the freely mobile portion of the tongue that extends anteriorly from the line of the circumvallate
papillae to the root. The oral tongue can further divide into four anatomic regions:
the tip, the lateral borders, the dorsum, and the undersurface (nonvillous surface).
Since the definition of oral cavity cancer in the cancer registry of the Department of Health of the Executive Yuan of the Republic of China includes oropharyngeal caner, this study also introduces the anatomy of oropharynx. The oropharynx is defined superiorly by the soft palate and inferiorly by the epiglottis;
it includes the tonsillar crypt and the palatine tonsil. It is limited anteriorly by the posterior third of the tongue and posteriorly by the midline wall of the pharyngeal constrictor muscles.
According to the International Classification of Disease, 9th Edition (ICD-9), relevant coding for oral cavity cancer will be listed as below. “140” stands for malignant neoplasm of lip. “141” represents malignant neoplasm of tongue. “143”
symbolizes malignant neoplasm of gum. “144” corresponds to malignant neoplasm of floor of mouth. “145” characterizes malignant neoplasm of other and unspecific parts of mouth such as, buccal, palate, retromolar trigone region, etc. “146” is the malignant neoplasm of oropharynx including the palatine tonsil, tongue base, posterior pharyngeal wall, etc. “149” refers to malignant neoplasm of other and ill-defined sites within the lip, oral cavity, and pharynx (6).
2. Epidemiology of Oral Cancer
The incidence of oral cancer varies widely throughout the world. In developed countries, the incidence is relatively small, comprising less than 5 % of all malignancies. In developing nations, oral cancer is reported to be the third most common malignancy after cancer of the cervix and stomach (7).
In Taiwan, oral cancer has become one of the top 10 causes of death from cancer since 1991. According to the statistical data from the Department of Health
of the Executive Yuan, the annual death toll for oral cancer in males was increasing surprisingly (8) (Table 2-1). In addition, a higher mortality rate was noted among central and southern Taiwan areas, probably due to more prevalent betel nut chewing habit in those regions.
According to the latest report from the Department of Health, the standardized incidence rate of oral cancer in Taiwan area was 15.07 per 100,000 people in 2001.
From 1996 to 2001, the standardized incidence rate of oral cancer increased 29.4%, the highest among all cancers in Taiwan (1). The average age of diagnosis was 52.0 and 53.4 year-old in male and female respectively.
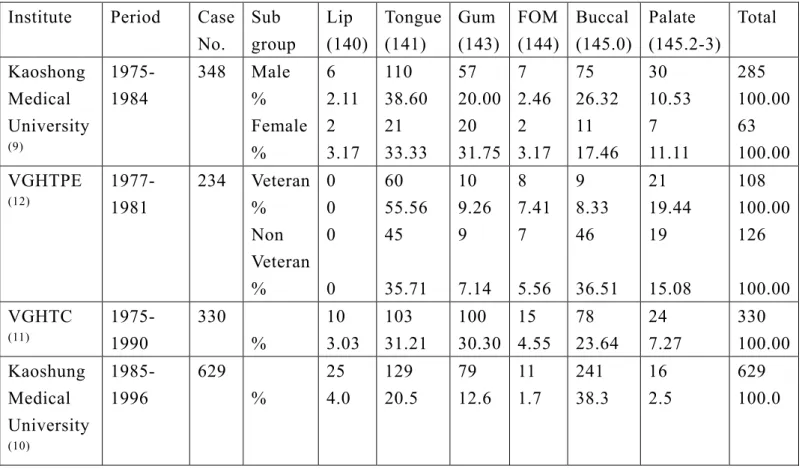
According to several large-scale studies in Taiwan (9, 10, 11, 12), the most prevalent site of oral cancer was buccal mucosa and followed by anterior tongue.
They account for over half of oral cancers (Table 2-2).
3. Etiology of Oral Cancer
The etiology of oral cancer is still unknown. However, oral cancer is strongly correlated with usage of tobacco products, alcohol, betel nut or exposure to ultraviolet light. Though poor oral and dental hygiene, certain dietary deficiency, virus infection, various chemical agents have been reported to be close related with oral cancer, no large scale study was confirmed a final conclusion (3).
Various studies have shown that 90% of patients with oral cancer use tobacco, and the relative risk of developing such cancers raised with the amount of smoking and the period of the habit. The incidence of oral cancer in smokers is around six times that of nonsmokers. Exposure to tobacco causes progressive sequential morphologic changes in the oral mucosa extending over a long period, with eventual neoplastic transformation. To support the theory of sustained mucosal injury, approximately 40% of patients who continued smoking after proper
treatment of their oral cancer developed second cancers of the upper aerodigestive tract, compared to 6% of those who ceased smoking.
Numerous studies have investigated the relationship between the oral cancer and alcohol consumption. Around 75% to 80% of cases having oral cancer consume alcohol. Also, oral cancer is observed six times more often in drinkers than nondrinkers. Alcohol probably acts in various ways to induce neoplastic changes in the mucosa, including acting as a direct irritant and causing underlying nutritional deficiencies.
Alcohol and tobacco are synergistic rather than just additive in their effect of causing dysplastic changes in the mucous membranes. Ko et al in their study has shown that relative risk of developing oral cancer in patients who have the habit of smoking, alcoholic consumption and betel nut chewing were 123 times higher than those who did not (13).
More than one third of patients with carcinoma of the lip have outdoor occupations. Prolong exposure to sunlight has been suggested as a major contributing factor to the development of carcinoma of the lip.
4. Staging of Oral Cancer
The most common staging system is TNM staging system established by American Joint Committee on Cancer (AJCC) since 1977 (14). The TNM system is an expression of the anatomic extent of disease and is based on the assessment of three components. First, “T” is the extent of the primary tumor. Second, “N”
represents the absence or presence and extent of regional lymph node metastasis.
Last, “M” stands for the absence or presence of distal metastasis. For oral cavity and oropharynx cancer, the definition of TNM is as follows:
Primary tumor (T)
TX Primary tumor cannot be assessed T0 No evidence of primary tumor Tis Carcinoma in situ
T1 Tumor 2 cm or less in greatest dimension
T2 Tumor more than 2 cm but not more than 4 cm in greatest dimension
T3 Tumor more than 4 cm in greatest dimension
T4 (lip) Tumor invades through cortical bone, inferior alveolar nerve, floor of mouth, of skin of face, i.e., chin or nose T4a (oral cavity) Tumor invades adjacent structures (e.g.,
through cortical bone, into deep [extrinsic] muscle of tongue [genioglossus, hyoglossus, palatoglossus, and styloglossus], maxillary sinus, skin of face)
(oropharynx). Tumor invades the larynx, deep/extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible T4b Tumor invades masticator space, pterygoid plates, or skull
base and/or encases internal carotid artery
(oropharynx) Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base or encases carotid artery
Regional Lymph Nodes (N)
NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node, is 3 cm or less
in greatest dimension
N2 Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension; or in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension; or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N2a Metastasis in single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
Distant Metastasis (M)
MX Distant metastasis cannot be assessed M0 No distant metastasis
M1 Distant metastasis
All cancers are further divided into 4 stages according to the “T”, “N”, and
“M” categories. This study summarized the staging group in Table 2-3. Generally speaking, poorer prognosis or survival interval is expected when higher stage is noted.
5. Treatment Protocol of Oral Cancer Nowadays
When facing the oral cancer, every physician must keeps in mind that the initial therapy of any cancer offers the best chance for cure (3). Frequently,
“recurrent tumor” is a synonym of “poor prognosis”.
Therapeutic modalities in common use for treating oral cavity and oropharynx cancers include surgery, radiotherapy, chemotherapy or a combination of these modalities (3, 15). In treatment planning, the pros and cons of each modality must be thoroughly evaluated (3). Generally, stage I and II tumors can be controlled equally well with surgery or radiotherapy as single modalities. Determinant survivals for this magnitude of disease are favorable because of the small size of the primary tumor and the lack of metastatic spread. The decision for surgery or radiotherapy is influenced by a variety of tumor and patient factors. For example, radiotherapy might be the best choice for a small lesion anatomically related to any neurovascular bundle, which has a pathway to the base of skull (e.g., small palate cancer adjacent to greater palatine neurovascular bundle) because the entire course of the nerve could be encompassed in the radiotherapy port. Another advantage of radiotherapy is the avoidance of surgery, anesthesia, and their associated risks. On the other hand, all other thing being equal, a gainfully employed patient might prefer an operation with a short convalescent period rather than appearing for daily treatments for 7 weeks.
The ability to control local-regional disease or to cure the patient decreases as the primary tumor increase in size (T3 or T4) and with the addition of positive cervical adenopathy. A planned combination of surgery and radiotherapy is generally considered necessary for the physician to have any chance to control stage III and IV disease. The frequent inadequacy of this combination has led in recent years to the addition of chemotherapy in an attempt to control advanced
disease.
Immunotherapy, gene therapy, and other biological agent are all under investigation now. So, they are not recommended in the treatment of oral cavity or oropharynx cancer (2).
Session 2 Relevant Factors in the Prognosis of Oral Cancer
1. Cancer Staging System
According to the AJCC cancer staging system, a higher stage indicates larger primary tumor, presence of cervical lymph node, or existence of distal metastases.
That is, a higher stage will have a poorer prognosis or survival interval. For example, a 5-year observed survival by “combined” AJCC stage for squamous cell carcinoma of the oral cavity from 1985-1991 was 59.8% for stage I, 46.3% for stage II, 36.3% for stage III, and 23.3% for stage IV (14). (Detail in Figure 2-1)
2. Tumor Volume in the Prognosis of Oral Cancer
In Spain, a hospital-based population of 94 oral cancer patients’ survival was analyzed by Kaplan-Meier curves (a log rank test for comparison among curves) and single and multivariate Cox regression model (16). The results disclosed that tumor size and age have significant prognostic values in oral cancer patients. That is, age and tumor size should be considered as the most relevant clinical variables for predicting survival of oral cancer at the time of diagnosis. However, a small population limited the interpretation of the results.
Kuriakose et al. used computed tomography (CT) to measure tumor volume and found that the disease-specific survival rate was 100% for patients with low-volume tumors (<13 cc) compared with 79% for those with stage T1 and T2
tumors (17).
3. Tumor Thickness on the Impact of Prognosis
In most studies, attention is also being directed to the measured depth of the tumor as a significant prognosticator for squamous cell carcinoma of the head and neck (3). Sheahan et al. in their clinical observation also disclosed that tumor thickness and size were both significantly predictive of an outcome in stage I and II oral cancer patients (18). However, they only evaluated early oral cancer instead of all stages of oral cancer.
4. Histology on the Impact of Prognosis
Of all prognostic parameters, the histologic grade of the primary tumor is considered to be the least informative for head and neck squamous cell carcinoma.
Poorly differentiated tumors generally tend to have a faster growth rate and a greater tendency to metastasize early and more frequently than well- or moderately-differentiated tumors.
Clinicians generally accept that endophytic invasive tumors are less favorable than exophytic superficial lesions. Deep tumors presumably gain access to blood and lymph vessels favoring the diffusion of loco-regional and distal spread and are also more resistant to radiotherapy because of the anoxic environment (3).
Woolgar et al. in their survival analysis study of oral cancer illustrated that some pathological features (e.g. histological pattern of invasion, status of resection margins and, for patients with metastasis, the number and anatomical level of positive nodes and the presence and extent of extra-capsular spread) are important indicators of tumor behavior and should be incorporated into protocols for assessment of prognosis (19). Another study also showed that the most predictive factor for survival of oral cancer was extra-capsular spread followed by the status
of resection margins (16).
5. The Present of Cervical Lymph Node in the Prognosis of Oral Cancer
The most significant prognosticator for head and neck squamous cell carcinoma is the presence or absence of cervical lymph node metastases. A widely accepted adage is that the cure rate for squamous cell carcinoma of the head and neck decreases by at least 50% when cervical metastases are present (3).
In a hospital-based study by Leite et al. in Brazil found that the most common prognostic variables were lymph node involvement (N) and distant metastasis (M) for oral cancer. As lymph node involvement or distant metastasis stage increased, a proportional decrease in survival was observed (20). Furthermore, Woolgar et al. in their survival analysis of 200 oral cancer patients showed that the 5-year actuarial survival rate for patients with metastasis confined to the lymph node(s) was less than that of patients without metastasis (21) and the most dramatic fall in the 5-year survival rate was seen in patients with metastasis and extra-capsular spread (ECS).
6. Genetic Influence in the Prognosis of Oral Cancer
Many genetic over-expressions had been proposed to be the prognosticators for oral cancers. Ralhan et al. in their study showed the median disease-free survival time was significantly shorter in patients with oral squamous cell carcinomas showing co-expression of MDM2 and p53 proteins compared with tumors that did not show concomitant over expression of these proteins (p = 0.02)
(22).
Chen et al. found that on multivariate analysis in their 59-paired patients, EGFR over-expression (p = 0.041) and N stage (p = 0.024) were the only
independent factors for overall survival (23). However, large-scale studies are still needed for clarifying the correlation between genetic over-expressions and survival of oral cancers.
7. Complications on the Impact of Prognosis
Post-operative complication was suggested to be a prognostic factor for oral cancer (24). The occurrence of systemic complications, advanced extended clinical severity stage, and staying in an ICU adversely affect the prognosis. Gallo et al.
found that in a Cox multivariate analysis of 327 laryngeal cancer patients, tumor size, histologic grading and post-operative complications had a significant impact on disease-free survival (25). However, they included laryngeal cancers instead of oral cancer patients.
8. Secondary Primary Tumor in the Prognosis of Oral Cancer In patients both with localized and advanced index tumors, 5-year survival rates were lower in those with secondary primary tumors and the difference was statistically significant for the 2-year survivors who were most likely to overcome the first diseases (26).
9. Marital Statuses and the Prognosis of Oral Cancer Elwood et al. in their case-control study showed that unmarried subjects have a higher relative risk for head and neck cancer than married subjects (27). For men, the crude relative risks compared to married men were 2.0 for widowed, 2.4 for single, and 4.8 for divorced or separated men. For women, the relationships were less strong but still significant with relative risks of 2.5 for the widowed, 1.4 for the single, and 2.0 for the divorced and separated. Simplification of this variable to
a comparison of non-married to married yields an unconfounded relative risk of 2.8 (95% CI 1.7-4.5) for both sexes combined, based on a multivariate analysis including alcohol consumption, smoking, socio-economic status, dental care and a history of tuberculosis. However, they didn’t discuss the prognosis of oral cancers.
Furthermore, their study was not population-based.
Another study by Krongrad et al. using the Surveillance, Epidemiology and End Results (SEER) program as a data base demonstrated that married patients had significantly longer median survival period than those who were divorced, single, separated or widowed. Controlling for age, stage, race and treatment, married patients still had a significantly lower risk of mortality than those who were divorced, single, separated, or widowed (28). Nevertheless, no previous study had addressed the difference of mortality rate between married and non-married oral cancer patients.
10. Relation between Religion and Survival
Yeole et al. in their population-based study in India showed that survival differences reached statistical significance for age, sex, religion, marital status, site and clinical stage (29). However, they used univariate analysis instead of controlling other relevant factors. Furthermore, they included cancers of head and neck rather than oral cancers.
Kark JD et al. in their study in secular versus religious kibbutzim showed that mortality was considerably higher in secular kibbutzim. Cox proportional hazards analysis was used to adjust for age and the matched design. Kaplan-Meier survival analysis of birth cohorts confirmed the association. The lower mortality in religious kibbutzim was consistent for all major causes of death (30). However, some traditional risk factors such as diet, smoking, obesity, alcohol intake, exercise, and
exposure to accidents were not available at the onset of this historical prospective study and limited the interpretation of the results. The authors speculated that such differences could be explained by the fact that a religious environment induces less stress, enhances host resistance, and promotes overall well being and a positive health status.
11. Education Level and the Prognosis of Oral Cancer
Ferraroni M et al. in their case-control study revealed that cancer of the mouth or pharynx were inversely and strongly related to education, cigarette, and alcohol consumption (31). Relative risks (RR) together with 95% approximate confidence intervals (CI) were derived from data stratified for sex, age, education, marital status, smoking, coffee, and alcohol consumption by multiple logistic regression models. However, there were only fifty cases included in this study. In addition, they only addressed the occurrence of neoplasm instead of prognosis of oral cancer.
Mariotto A et al. projected cancer survival for the entire US as well as states from survival data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program. The results illustrated that education was the best indicator of longer cancer survival (32). However, they only included breast, prostate and colorectal cancer patients. Besides, they measured the percentage of the population who graduated from high school instead of individual educational level.
12. Laboratory Data on the Impact of Prognosis
Bryne M et al. in their clinical observation illustrated that patients with Rhesus (Rh) (D)-negative blood group had significantly poorer prognosis (Mean 5-year survival, 8%) than patients with Rh (D)-positive blood group (5-year
survival, 30%) (p = 0.04). Since the Rh gene locus is located on the short arm of chromosome 1 which reportedly has shown rearrangements in some head and neck squamous cell carcinoma and other human neoplasms, they speculated that the Rh gene locus might be linked with chromosome 1 changes of importance for the progression of oral squamous cell carcinoma (33). However, they only discussed Rh group instead of ABO group on the impact of oral cancer prognosis.
Pre-operative serum albumin level had been proposed to be a prognostic factor for head and neck squamous cell carcinoma. Medos MA et al. showed that those with a serum albumin concentration of 3.85 g/dl had a longer median survival interval than those with a serum albumin concentration less than 3.85 g/dl (34).
13. Delay in the Diagnosis and Survival of Oral Cancer
A hospital-based study by Pitiphat W et al. in Greece showed that former smokers had a 4.3 times greater risk of delayed diagnosis in oral cavity cancer compared with current smokers (95% CI: 1.1-17.1). The length of delay was greater among single patients, non-smokers, or those with stage IV tumors (35). However, they didn’t research the relationship between delay in the diagnosis and prognosis of oral cancers.
14. Human Papilloma Virus (HPV) Infection and Survival of Oral Cancer
Abundant evidence in recent years has implicated human papilloma viruses (HPV) in the genesis of squamous cell carcinomas in the anogenital region as well as in carcinomas within the upper aero-digestive tract, including oral cancer (36). HPV 16 and 18 seem to be the most important viruses responsible for tumourigenesis and can be found in premalignant and malignant lesions of the oral
cavity in up to 80%. However, there is less evidence that an infection with HPV has prognostic relevance for patients’ outcome.
Chapter 3 Research Methods
Session 1 Research Structure
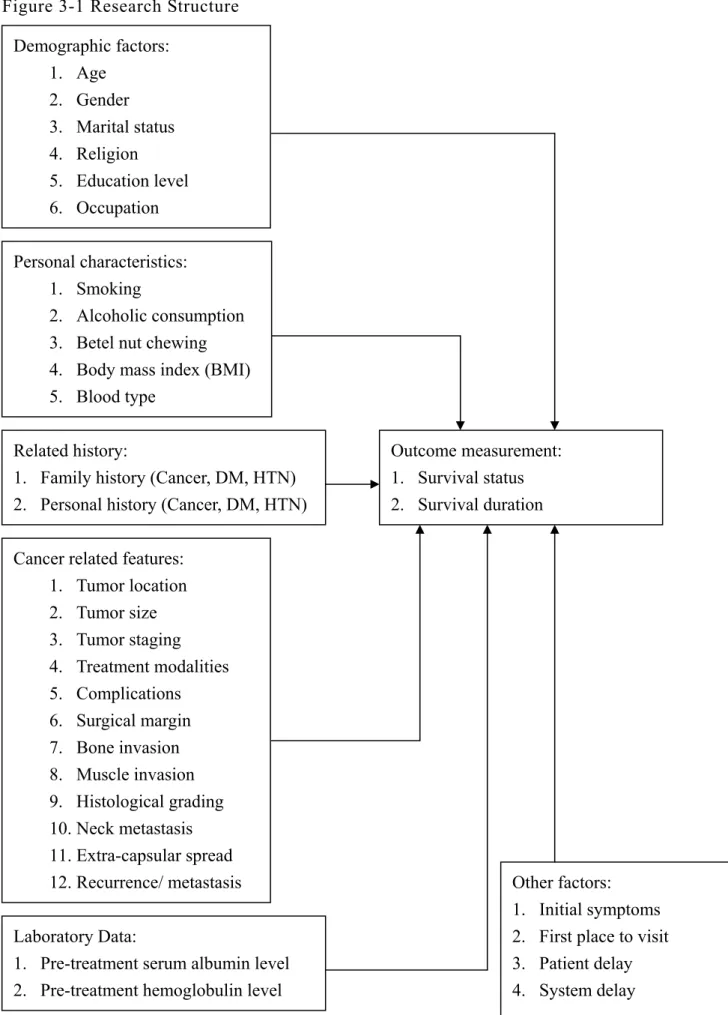
The structure of this study was summarized in Figure 3-1. This study aims to investigate if relevant factors such as, demographic factors, personal characteristics, related history, cancer related features, laboratory data, and other factors would influence the survival of oral cancer patients.
Session 2 Sample and Data Sources
This is a hospital-based study. All patients who were admitted under the diagnosis of oral cancer in cased hospital from March 1995 to December 2002 were included and the observation end point was set on 31 Dec. 2004. This study retrospectively reviewed the chart records of over 1600 patients. Exclusive criteria were as below:
1. Those who had no pathological report.
2. Those who had been treated at other institutes.
3. Those who didn’t complete therapeutic protocol in our hospital.
4. Those with inadequate chart records.
After these exclusions, there were 1,118 cases which fulfilled the requirements and were included for further analyses.
Figure 3-1 Research Structure Demographic factors:
1. Age 2. Gender 3. Marital status 4. Religion 5. Education level 6. Occupation
Personal characteristics:
1. Smoking
2. Alcoholic consumption 3. Betel nut chewing 4. Body mass index (BMI) 5. Blood type
Cancer related features:
1. Tumor location 2. Tumor size 3. Tumor staging 4. Treatment modalities 5. Complications 6. Surgical margin 7. Bone invasion 8. Muscle invasion 9. Histological grading 10. Neck metastasis 11. Extra-capsular spread 12. Recurrence/ metastasis
Outcome measurement:
1. Survival status 2. Survival duration Related history:
1. Family history (Cancer, DM, HTN) 2. Personal history (Cancer, DM, HTN)
Laboratory Data:
1. Pre-treatment serum albumin level 2. Pre-treatment hemoglobulin level
Other factors:
1. Initial symptoms 2. First place to visit 3. Patient delay 4. System delay
Session 3 Measurement
The operational definitions of variables in this study were listed in Table 3-1.
Table 3-1 Operational definitions of variables
Variable Operation definition Attribute
Age of onset <40 yrs, 40-49 yrs, 50-59 yrs, >60 yrs Ordinal
Gender Male, female Nominal
Marital status Married, Single, Widow/widower, Divorced/separated
Nominal
Religion Buddhist, Christian, Catholic, Muslim, Dao, None Nominal Education level Nil, <6 yrs, 6-12 yrs, >12 yrs Ordinal Occupation Non-skilled, Professional/managerial, None Nominal
Smoking No, Yes Nominal
Alcoholic No, Yes Nominal
Betel nut No, Yes Nominal
Blood type A, B, O, AB Nominal
Tumor location Lip, Gingiva, Mouth floor, Anterior tongue, Buccal, Palate, Retromolar trigone, Palatine tonsil, Tongue base, Posterior pharyngeal wall
Nominal
Treatment modality
Radiation alone, Chemotherapy alone, Surgery, Concurrent chemoradiotherapy, Surgery alone, Surgery plus radiotherapy, Surgery plus
chemotherapy, Surgery plus chemoradiotherapy
Nominal
Post-operative complications
No, Yes Nominal
Complication type
Wound infection, pneumonia, hemorrhage, Others Nominal
Post-operative reconstruction
No, Yes Nominal
Table 3-1 Operational definitions of variables (cont’)
Variable Operation definition Attribute
Reconstruction type Free flap, Pectoris major myo-cutaneous flap (PMMCF), Tongue flap, Others
Nominal
Pathological margin Free, Not free Nominal
Bony invasion No, Yes Nominal
Histological grading
Well-differentiated,
moderately-differentiated, Poorly- or Un-differentiated, Others
Nominal
Neck dissection No, Unilateral, Bilateral Nominal
Neck metastases No, Yes Nominal
Extra-capsular spread
No, Yes Nominal
Muscle invasion No, Yes Nominal
Family history No, Yes Nominal
Family history of cancer
No, Yes Nominal
Family history of diabetes mellitus
No, Yes Nominal
Family history of hypertension
No, Yes Nominal
Personal history No, Yes Nominal
Personal history of cancer
No, Yes Nominal
Personal history of diabetes mellitus
No, Yes Nominal
Personal history of hypertension
No, Yes Nominal
Initial Symptom Oral mass, Oral ulcer, Neck mass, Odynophagia, Others
Nominal
First place to visit Medical centers, Loco-regional hospitals, General practitioners
Nominal
Stage Stage I, Stage II, Stage III, Stage IV Ordinal
Table 3-1 Operational definitions of variables (cont’)
Variable Operation definition Attribute
Recurrence or metastases
No, Yes Nominal
Survival status Death, Alive Nominal Tumor size (cm) The length of the longest axis (cm) Ratio Body mass index
(kg/M2)
Body weight (kg) divided by square of height (M)
Ratio
Albumin (g/dl) Pre-treatment serum albumin level Ratio Hemoglobulin
(g/dl)
Pre-treatment hemoglobulin level Ratio
Patient delay (day)
From the present of initial symptom to the day of looking for help
Ratio
System delay (day)
From the day of first visit to the day of confirmed diagnosis
Ratio
Survival interval (month)
From the time of treatment finished to the time of death or last follow-up date
Ratio
Session 4 Analytical Methods
This study used descriptive statistics for general data presentation.
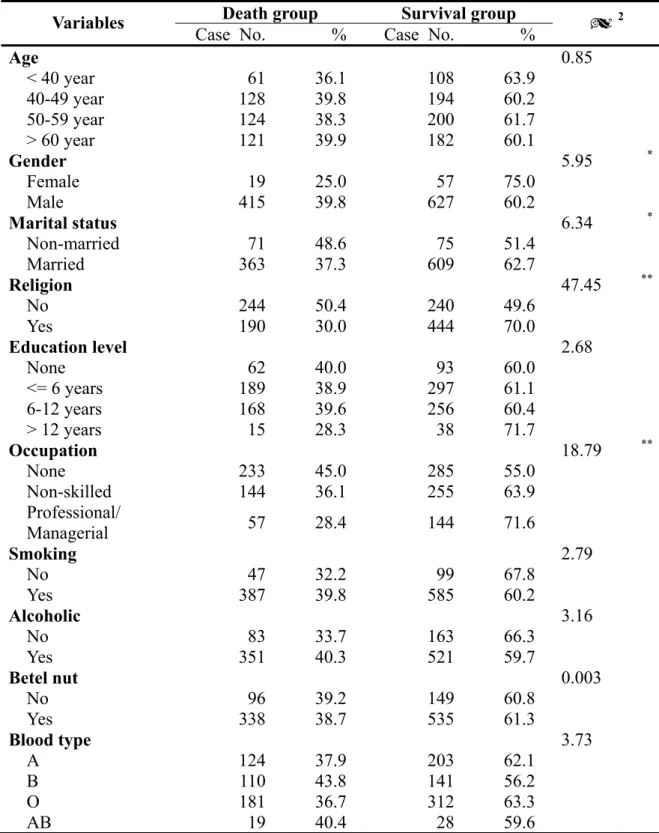
Comparison of nominal or ordinal variables between survival group and death group were analyzed by the Chi-square test while continuous variables were analyzed with the student’s t-test. Survival analysis was investigated by the Kaplan-Meier method. The differences between subgroups were examined by the log-rank test. Furthermore, relevant factors influencing the survival period were examined by the Cox proportional hazard model. We used backward regression method to exclude those variables with p-value of more than 0.1. Finally, age and gender were added into model for controlling.
Chapter 4 Results
Session 1 Descriptive analyses
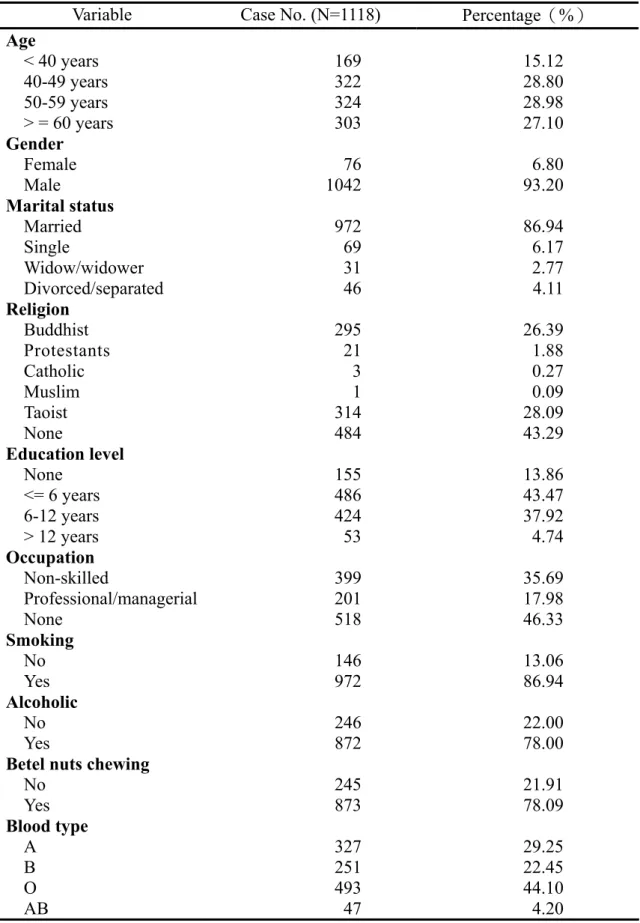
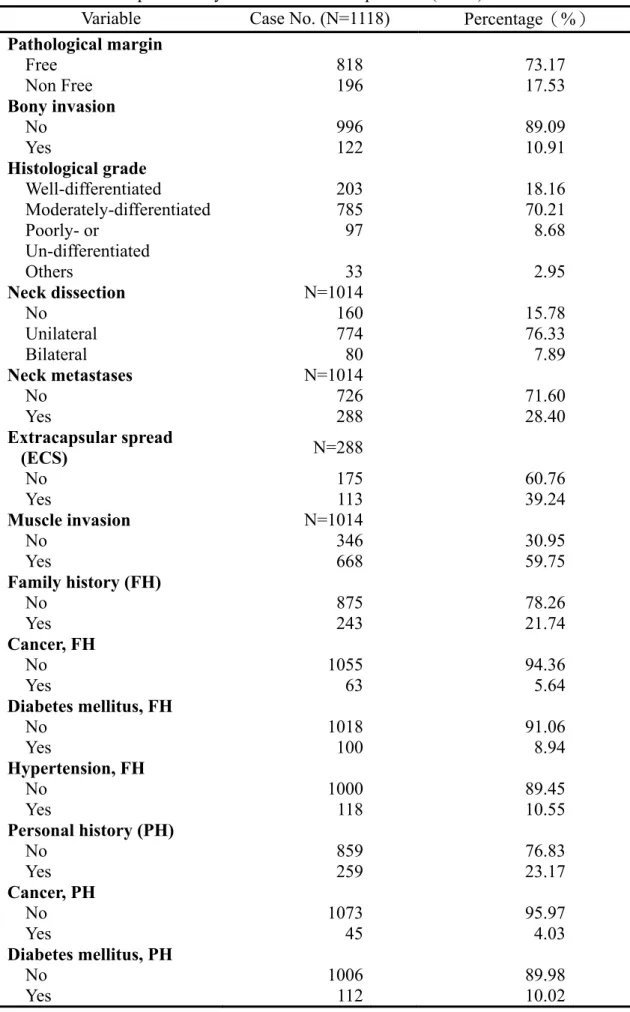
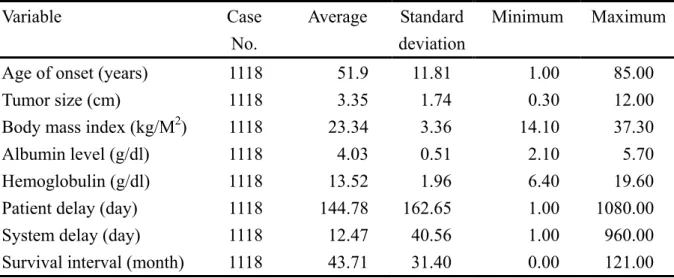
There were total 1,612 patients admitted to cased hospital under the diagnosis of oral cancer from March 1995 to December 2002. Adequate data were obtained from chart records of 1,118 patients. The average age of onset was 51.90 years old. One hundred and sixty nine patients aged less than 40 years old (15.1%) and other patients were almost equally distributed among 40-49, 50-59, and more than 60-year-old groups. Males accounted for 93.2% (N=1042) of all patients. In personal habits, 86.9% patients (N=972) were habitual smokers, 78% patients (N=872) had an alcoholic consumption lifestyle, and 78.9% patients (N=873) used to chew betel nuts before (Table 4-1).
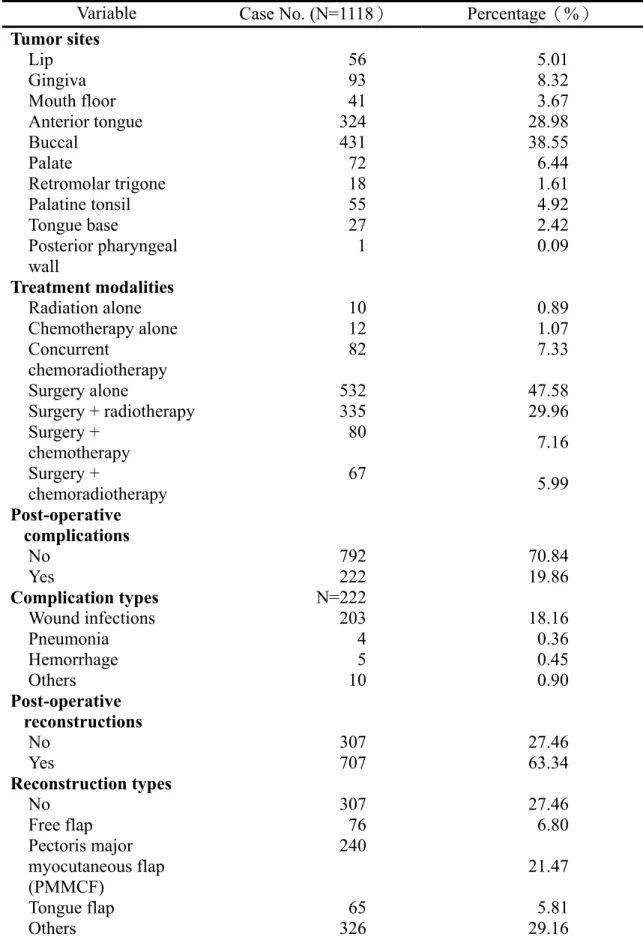
Buccal mucosa was the most common site (N=431, 38.6%) followed by the anterior tongue (N=324, 30.0%), gingival (N=93, 8.3%), palate (N=72, 6.4%), lip (N=56, 5.0%), palatine tonsil (N=55, 4.9%), floor of mouth (N=41, 3.7%), tongue base (N=27, 2.4%), retromolar trigone (N=18, 1.6%), and posterior pharyngeal wall. (N=1, 0.1%)
In therapeutic protocols, 104 patients (9.3%) chose non-surgical modalities including chemotherapy, radiotherapy, or concomitant chemo-radiotherapy. One thousand and fourteen patients (90.7%) received surgical resection with or without neck dissection. In those who had surgery, no further treatment was given in 532 patients (52.5%), 335 patients (33.0%) received post-operative radiotherapy, 80 patients (7.9%) had either pre-operative induction chemotherapy or post-operative adjuvant chemotherapy, and 67 patients (6.6%) had combined chemotherapy with radiotherapy.
Squamous cell carcinoma was the most common pathological diagnosis (N=1085, 97.0%). Two hundred and three patients (18.2%) were well-differentiated squamous cell carcinoma, 785 patients (70.2%) were moderately differentiated, and 97 patients (8.68) were poorly or un-differentiated.
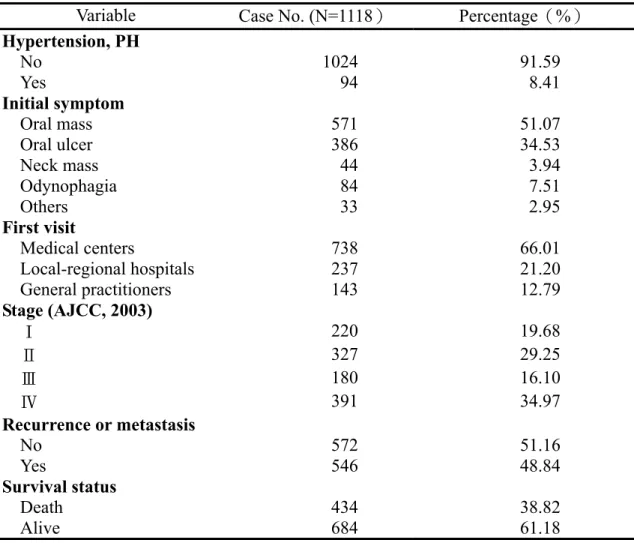
Oral mass is the major complaint when oral cancer patient first visited (N=571, 51.7%), followed by oral ulcer (N=386, 34.5%), oral pain (N=84, 7.5%), neck mass (N=44, 3.9%), and others (N=33, 3.0%). In addition, most patients (N=738, 66.0%) came to medical centers as their first visit while 380 patients (34.0%) were referred from loco-regional hospitals or general practitioners.
Two hundred and twenty patients (19.68%) were stage I diseases when they looked for medical treatment while stage II, stage III, and stage IV diseases were found in 327 (29.25%), 180 (16.10%), and 391 (34.97%) patients, respectively.
Recurrence or distal metastases were found in 546 patients (48.8%) and 434 patients (38.8%) already died during follow up periods.
In those received surgical procedures, 818 patients (80.7%) had a clear margin during pathological examination while 196 patients (9.3%) had a residual tumor after operation. One hundred and sixty patients (15.8%) received primary tumor excision only while 854 patients (84.2%) simultaneously had neck dissection. In those who had neck dissection, 80 patients (9.4%) received bilateral neck dissection whereas 774 patients (90.6%) received unilateral neck dissection only. Post-operative complications were found in 222 patients (21.9%) and wound infections were the most common complications (N=203, 91.4%), followed by hemorrhages (N=5, 2.3%), and pneumonias (N=4, 1.8%). No post-operative reconstruction was arranged in 307 patients (30.3%) whereas 707 patients (69.7%) received variable degrees of post-operative reconstruction. In those reconstructed patients, 310 patients (43.8%) had split thickness skin graft reconstruction while
240 patients (33.9%) received pectoris major myocuaneous flap, 76 patients (10.7%) had micro-vascular free flap, 65 patients (9.2%) received tongue flap, 16 patients (2.3%) had other types of reconstructions.
Two hundred and eighty eight patients (28.40%) had cervical metastasis confirmed by pathological examination. In addition, extra-capsular spread (ECS) was found in 113 out of 288 patients (39.24%).
One hundred and twenty two patients (10.9%) had bone invasion confirmed either by image study or by pathological examination while 996 patients (89.1%) had not.
Eight hundred and fifty nine patients (76.8%) had no obvious past history while 259 patients (23.2%) had related or unrelated past history including cancer of other sites in 45 patients, diabetes mellitus in 112 patients, and hypertension in 94 patients. Eight hundred and seventy five patients (78.3%) had no noticeable family history whereas 243 patients (21.7%) had a family history including cancers in 63 patients, diabetes mellitus in 100 patients, and hypertension in 118 patients.
In marital status, 972 patients were married (86.9%), 69 patients were single (6.17%), 31 were widows/widowers (2.77%), and 46 were divorced or separated.
(4.11%) When it comes to religion, 634 patients (56.7%) claimed to have religious affiliations while 484 patients (43.3%) did not. Most of them were Taoists (N=314, 28.09%), followed by Buddhists (N=295, 26.39%), Protestants (N=21, 3.3%), Catholics (N=3, 0.5%), and Moslem (N=1, 0.2%).
In educational status, 155 patients (13.9%) didn’t go to school at all while 486 patients (43.5%) graduated from elementary schools, 424 patients (37.9%) graduated from junior or senior high schools and 53 patients (4.7%) graduated from colleges or universities. As for occupation, 518 patients (46.3%) declared