I
MPACT
OF
N
ATIONAL
H
EALTH
I
NSURANCE
ON
THE
S
URVIVAL
R
ATE
OF
P
ATIENTS
WITH
O
STEOSARCOMA
IN
T
AIWAN
: R
EVIEW
OF
74 P
ATIENTS
Kein-Boon Poon, Song-Hsiung Chien, Gau-Tyan Lin, and Gwo-Jaw Wang Department of Orthopedic Surgery, Kaohsiung Medical University Chung-Ho
Memorial Hospital, Kaohsiung, Taiwan.
The 2-year survival rate for high-grade osteosarcoma was 46.9% before the introduction of National Health Insurance (NHI) in Taiwan on March 1, 1995, but increased to 73.8% after the implementation of NHI. The 5-year survival rate also increased, from 37.5% to 63.6%. Between May 1990 and May 2001, 74 patients with high-grade osteosarcoma were treated at our hospital. Median age was 17 years (range, 7–63 years). Inadequate surgical margins, poor histologic response to chemotherapy, advanced stage of disease, and incomplete treatment were strongly associated with poor prognosis. Before NHI, 10 patients had incomplete treatment, mainly because of unaffordable medical fees. After NHI, only three patients had incomplete treatment, due to personal reasons. Patient survival improved dramatically with advances in multiagent chemotherapy, but it was the NHI that enabled patients to complete expensive treatment courses, including preoperative neoadjuvant chemotherapy, limb-salvage surgery, and postoperative adjuvant chemotherapy. The NHI also improved the accessibility of medical care, with more patients presenting in the early stages of disease and, as a result, it not only improved survival rate but also increased the number of patients undergoing limb-salvage surgery. We concluded that the NHI significantly improved the survival rate for patients with osteosarcoma in Taiwan.
Key Words: National Health Insurance, osteosarcoma, survival rate, Taiwan
(Kaohsiung J Med Sci 2004;20:230–4)
Received: November 16, 2003 Accepted: March 30, 2004
Address correspondence and reprint requests to: Dr. Song-Hsiung Chien, Department of Orthopedic Surgery, Kaohsiung Medical University Chung-Ho Memorial Hospital, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
Osteosarcoma is the most common primary malignancy of bone, with an aggressive local pattern of growth and high metastatic potential [1]. Since the advent of multiagent adjuvant and neoadjuvant chemotherapy, patient survival has improved dramatically [2–4]. In our study, poor response to chemotherapy, inadequate surgical margin, advanced stage of disease, and incomplete treatment were all related to poor prognosis.
The government of Taiwan introduced the National Health Insurance (NHI), to cover all citizens, on March 1,
1995. Before the implementation of NHI, complete treat-ment for osteosarcoma was unaffordable for most patients. The average cost of complete neoadjuvant chemother-apy was NT$300,000 (US$8,571), for complete adjuvant chemotherapy was NT$700,000 (US$20,000), and for limb-salvage surgery was NT$300,000 (US$8,571). Amputations were more popular because they incurred less medical expense. The high cost of medical treatment might have hindered the accessibility of appropriate management for osteosarcoma in the early stages of the disease and, as a result, patients always presented to the hospital in the advanced stages of disease. After the implementation of NHI, these barriers were removed. Under the NHI system, all treatments are free of charge for patients with osteosar-coma. This study was conducted to analyze the influence of NHI on the survival rate for osteosarcoma.
M
ATERIALSANDM
ETHODSBetween May 1990 and May 2001, 74 patients with high-grade osteosarcoma of the extremities were treated at our hospital. The median age was 17 years (range, 7–63 years). The 44 males and 30 females were followed for 2 to 13 years after osteosarcoma treatment; 32 patients were treated before the implementation of NHI and 42 after the imple-mentation of NHI.
Lesions were located in the proximal humerus in four patients, in the proximal femur in five, in the distal femur in 40, in the proximal tibia in 17, in the distal tibia in two, in the proximal fibula in four, and in the distal fibula in two. The Enneking staging system was used throughout the study [5]. Nine patients presented with stage IIA lesions, 42 with stage IIB lesions, six with stage IIIA lesions, and 17 with stage IIIB lesions.
Treatment included limb-salvage surgery, amputation, and incomplete treatment (Table 1). Rotationplasties were regarded as amputations [6,7]. Incomplete treatment was defined as biopsy without further management, incomplete neoadjuvant chemotherapy after biopsy, or refusal of sur-gery after completing neoadjuvant chemotherapy. Fifty-one patients completed neoadjuvant and adjuvant chemo-therapy, and their histologic response to chemotherapy was classified as “good” (≥ 90% tumor necrosis) or “poor” (< 90% tumor necrosis) [8]. Before 1995, methotrexate was used for preoperative and postoperative chemotherapy,
but it was changed to doxorubicin and cisplatin postopera-tively because of poor histologic response with methotrex-ate. After 1995, we used high-dose methotrexate, cisplatin or carboplatin, and doxorubicin for neoadjuvant chemo-therapy, and we added ifosfamide postoperatively for patients with poor histologic response. The 2- and 5-year overall survival rates were calculated without considering the influence of NHI. The 2- and 5-year survival rates before and after the implementation of NHI were analyzed using the Kaplan-Meier method.
R
ESULTSOf the 51 patients who received neoadjuvant chemother-apy, 31 had good histologic response (60.8%) and 20 had poor histologic response (39.2%). The 2-year survival rates for patients with good and poor histologic response to chemotherapy were 100% and 40% (8/20), respectively. Nine patients had inadequate surgical margins. Six pa-tients developed local recurrence and their 2-year survival rate was 16.7% (1/6).
Before the implementation of NHI, four patients pre-sented with stage IIIA and 11 with stage IIIB lesions. Af-ter NHI implementation, there were two stage IIIA and six stage IIIB lesions. The overall 2-year survival rate for stage IIA disease was 100%, for stage IIB was 81%, for stage IIIA was 50%, and for stage IIIB was 0%.
Ten patients had incomplete treatment before the im-plementation of NHI, which decreased to three patients after NHI implementation. For patients with incomplete treatment, the 2-year survival rate was 15.4% (2/13).
The 2- and 5-year overall survival rates without con-sidering the influence of NHI were 62.2% (46/74) and 48.1% (26/54), respectively. The 2-year survival rates before and after implementation of NHI were 46.9% (15/32) and 73.8% (31/42), respectively (Figure 1). The 5-year survival rates before and after implementation of NHI were 37.5% (12/32) and 63.6% (14/22), respectively (Figure 2).
D
ISCUSSIONThis retrospective study analyzed the influence of NHI on the survival rate of patients with osteosarcoma. The 2- and 5-year overall survival rates were 62.2% and 48.1%, re-spectively. These are lower than the rates in other reports [6,9–11]. We identified several factors that could influence the survival rate of our patients. Patients with inadequate
Table 1. Type of treatment for patients with osteosarcoma at Kaohsiung Medical University Hospital
Limb-salvage surgery (n = 33)
Custom-made knee prosthesis 21
Custom-made hip prosthesis 3
Shoulder prosthesis 1
Wide excision with allograft 6
Wide excision with autoclave autograft 1
Wide excision with limb lengthening 1
Amputation (n = 28) Below-the-knee amputation 1 Above-the-knee amputation 10 Hip disarticulation 14 Segmental amputation 1 Rotationplasty 2 Incomplete treatment (n = 13) Biopsy 5
Biopsy and incomplete neoadjuvant chemotherapy 6
surgical margins had a higher rate of local recurrence and their 2-year survival rate was very low. Patients with poor histologic response to chemotherapy also had lower survi-val rates compared to those with good histologic response. Bacci et al suggested immediate amputation for patients with inadequate surgical margins and poor histologic re-sponse to preoperative chemotherapy [6,12]. Advanced stage of disease and incomplete treatment were strongly associated with poor prognosis.
On March 1, 1995, the government of Taiwan introduced NHI to cover all citizens. This NHI program was proposed to ensure that patients have access to health care at a rea-sonable cost [13]. We noted a significant difference in sur-vival rates before and after the implementation of NHI. Be-fore NHI implementation, the 2- and 5-year survival rates
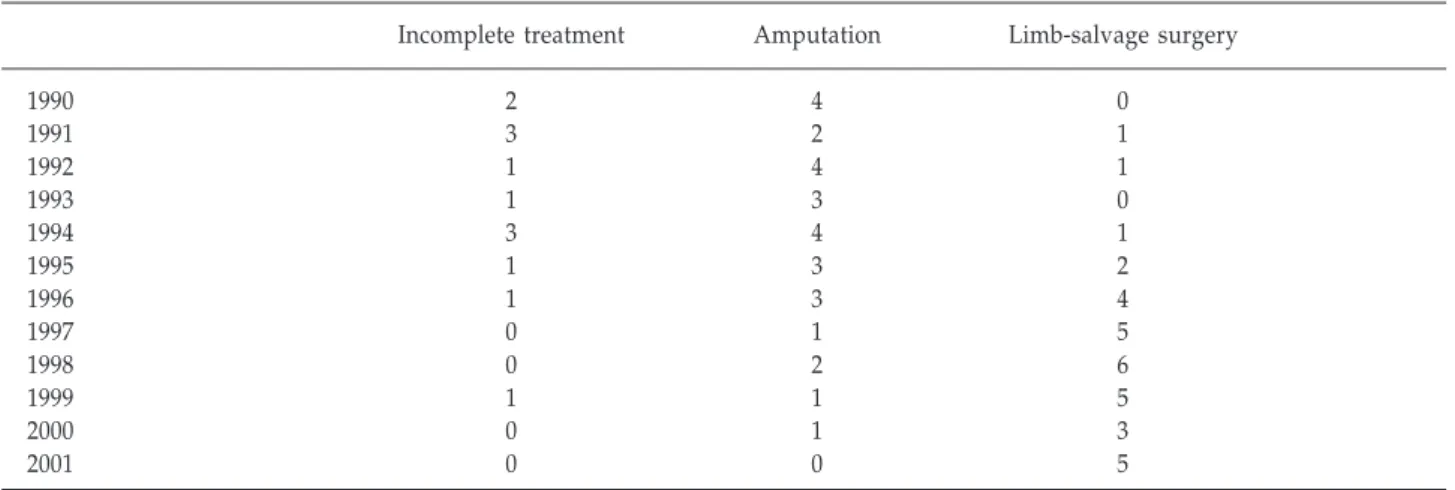
were 46.9% and 37.5%, respectively. After implementa-tion, these rates increased to 73.8% and 63.6%, respectively. Under the NHI system, all treatments for osteosarcoma are free of charge. NHI makes complete treatment accessible to patients. Before NHI implementation, only a few patients could afford to pay the expensive medical fees. More ampu-tations were performed before NHI implementation be-cause of the lower medical expenses and bebe-cause patients presented with advanced disease that was untreatable with limb-salvage surgery. Use of the limb-salvage procedure increased significantly after NHI implementation (Table 2). We attributed this to coverage of medical expenses by the NHI, more patients presenting in the early stages of disease, improvement in the efficacy of chemotherapy, improved operative techniques, and advances in prosthetic design.
Proportion surviving 1.2 1.0 0.8 0.6 0.4 0.2 0.0 0 10 20 30 Time (mo) After NHI, n = 42 Before NHI, n = 32 Proportion surviving 1.2 1.0 0.8 0.6 0.4 0.2 0.0 0 10 20 30 40 50 60 70 Time (mo) After NHI, n = 22 Before NHI, n = 32
Figure 2. Kaplan-Meier analysis of 5-year survival of patients with osteosarcoma treated before and after the implementation of National Health Insurance.
Figure 1. Kaplan-Meier analysis of 2-year survival of patients with osteosarcoma treated before and after the implementation of National Health Insurance.
Table 2. Number of patients who received incomplete treatment, amputation and limb-salvage surgery between 1990 and 2001
Incomplete treatment Amputation Limb-salvage surgery
1990 2 4 0 1991 3 2 1 1992 1 4 1 1993 1 3 0 1994 3 4 1 1995 1 3 2 1996 1 3 4 1997 0 1 5 1998 0 2 6 1999 1 1 5 2000 0 1 3 2001 0 0 5
Limb-salvage surgery became the main surgical procedure instead of amputation for treatment of osteosarcoma of the extremity in our hospital as well as many other medical centers [4,14,15].
Advances in adjuvant and neoadjuvant chemotherapy improved the survival rate dramatically for patients with osteosarcoma [2–4]. Chemotherapy remains the chief factor in curing patients with osteosarcoma and every attempt should be made to increase its efficacy [7]. However, it was the NHI that enabled patients to complete the expensive treatment courses. The implementation of NHI improved the accessibility of medical care among the general popula-tion, with more patients presenting at the early stage of disease. Therefore, a better survival rate was expected after NHI implementation. Without the NHI, despite the advances in chemotherapy and surgical technique, most patients with osteosarcoma would not receive adequate treatment, due to socioeconomic factors. We therefore conclude that the NHI had a great impact and improved the survival rate of patients with osteosarcoma in Taiwan.
R
EFERENCES1. Papagelopoulos PJ, Galanis EC, Vlastou C, et al. Current con-cepts in the evaluation and treatment of osteosarcoma.
Orthopedics 2000;23:858–67.
2. Picci P, Sangiorgi L, Bahamonde L, et al. Risk factors for local recurrences after limb-salvage surgery for high-grade osteo-sarcoma of the extremities. Ann Oncol 1997;8:899–903. 3. Provisor J, Ettinger LJ, Nachman JB, et al. Treatment of
non-metastatic osteosarcoma of the extremity with preoperative and postoperative chemotherapy: a report from the children’s cancer group. J Clin Oncol 1997;15:76–84.
4. Sluga M, Windhager R, Lang S, et al. Local and systemic
control after ablative and limb sparing surgery in patients with osteosarcoma. Clin Orthop 1999;358:120–7.
5. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980; 153:106–20.
6. Bacci G, Ferrari S, Lari S, et al. Osteosarcoma of the limb: amputation or limb salvage in patients treated by neoadjuvant chemotherapy. J Bone Joint Surg Br 2002;84:88–92.
7. Grimer RJ, Taminiau AM, Cannon SR. Surgical outcomes in osteosarcoma. J Bone Joint Surg Br 2002;84:395–400.
8. Picci P, Bacci G, Campanacci M, et al. Histologic evaluation of necrosis in osteosarcoma induced by chemotherapy. Re-gional mapping of viable and nonviable tumor. Cancer 1985; 56:1515–21.
9. Glasser DB, Lane JM, Huvos AG, et al. Survival, prognosis, and therapeutic response in osteogenic sarcoma: the Memorial Hospital experience. Cancer 1992;69:698–708.
10. Souhami RL, Craft AW, Van der Eijken JW, et al. Randomised trial of two regimens of chemotherapy in operable osteo-sarcoma: a study of the European Osteosarcoma Intergroup.
Lancet 1997;350:911–7.
11. Pochanugool L, Subhadharaphandou T, Dhanachai M, et al. Prognostic factors among 130 patients with osteosarcoma.
Clin Orthop 1997;345:206–14.
12. Bacci G, Ferrari S, Mercuri M, et al. Predictive factors for local recurrence in osteosarcoma: 540 patients with extremity tumors followed for minimum 2.5 years after neoadjuvant chemo-therapy. Acta Orthop Scand 1998;69:230–6.
13. Cheng SH, Chiang TL. The effect of universal health insurance on health care utilization in Taiwan: results from a natural experiment. JAMA 1997;278:89–93.
14. Bacci G, Ferrari S, Bertoni F, et al. Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Istituto Ortopedico Rizzoli according to the Istituto Ortopedico Rizzoli/Osteosarcoma-2 protocol: an updated report. J Clin Oncol 2000;18:4016–27.
15. Rougraff BT, Simon MA, Kneisl JS, et al. Limb salvage com-pared with amputation for osteosarcoma of the distal end of the femur. J Bone Joint Surg Am 1994;76:649–56.