行政院國家科學委員會專題研究計畫 成果報告
皮質類固醇影響上皮細胞癌生長及化學藥物敏感性機轉之
研究並探討與癌細胞反應模式相關之分子分類(3/3)
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-002-006- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 國立臺灣大學醫學院內科 計畫主持人: 鄭安理 計畫參與人員: 鄭安理 盧彥伸 郭明良 葉坤輝 陳健尉 報告類型: 完整報告 報告附件: 出席國際會議研究心得報告及發表論文 處理方式: 本計畫可公開查詢中 華 民 國 94 年 10 月 31 日
行政院國家科學委員會補助專題研究計畫
■ 成 果 報 告
□期中進度報告
皮質類固醇影響上皮細胞癌生長及化學藥物敏感性機轉之研
究並探討與癌細胞反應模式相關之分子分類
計畫類別:■ 個別型計畫 □ 整合型計畫
計畫編號:NSC 91-2314-B-002-166
執行期間: 91 年 8 月 1 日至 94 年 7 月 31 日
計畫主持人:鄭安理
共同主持人:盧彥伸 郭明良 葉坤輝 陳健尉
計畫參與人員:
成果報告類型(依經費核定清單規定繳交):□精簡報告 ■完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
■出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:國立台灣大學醫學院 內科
中 華 民 國 94 年 10 月 31 日
一、中文摘要 皮質類固醇除本身對於某些血液腫瘤具細胞毒性之外,也常與抗癌化學藥物併用以治 療因化學藥物引起之噁心、嘔吐及過敏反應等副作用。雖然類固醇己被証實可以影響多種 細胞之重要訊息傳遞徑路,其中有些與癌細胞抗藥性有關。然而我們對類固醇類藥物對於 與一般癌細胞生長以及化學藥物感受性可能產生之影響仍所知極少。釐清這個問題對臨床 腫瘤治療將會有重要影響。 我們隨機選擇了十四株癌細胞株有系統地進行研究以解答這個問題。Dexamethasone (DEX)被選為皮質類固醇代表藥物。我們發現: 1. DEX 確實對癌細胞株(十四株之中的七株)的生長以及化學藥物感受性有影響。DEX 對 癌細胞的影響呈現異質性而且似乎是彼此互斥的。DEX(0.01~1.0uM)抑制四株細胞的 生長(MCF-7,MCF/MXR1,MCF/TPT300及 HeLa 細胞),提高了一株細胞對 cisplatin 的化
學藥物感受性(SiHa),並降低兩株細胞對 cisplatin, doxorubicin, 5FU,及 taxol 的 化學藥物感受性(H460 及 Hep3B)。 2. 此影響是皮質類固醇受體—依賴性的。因為 DEX 只有在含有高濃度皮質類固醇受體(≧ 2.1x104 /細胞)的七株細胞才有影響。在其他七株不受 DEX 影響的細胞中,有五株細胞 皮質類固醇受體濃度範圍僅在 2.0~5.7x103 /細胞之間。而另二株含有高濃度皮質類固醇 受體但不受 DEX 影響的細胞中(TW01, TW04),我們發現其皮質類固醇受體不具有功能。 3. DEX 在 SiHa 細胞所造成的化學藥物致敏感效應與其對 NF-kB 的調控有著高度相關。透
過轉殖含有 dominant negative IkB 的 plasmid 進入 SIHa cells 中以抑制 NFkB 活性, 我們發現原先 DEX 提高 SiHa 細胞對 cisplatin 的化學藥物感受性的現象消失。而在我 們進一步的研究發現在 SiHa 細胞中皮質類固醇受體確實會與 NFkB 有直接作用(dirrect protein-protein interaction)。 4. 我們另外發現 DEX 會直接作用於 MCF7 細胞的 p21 promoter 上造成 p21 的向上調控, 表現量增加進而造成細胞週期 G1 arrest, 抑制癌細胞的生長。 5. 為了尋找可能造成 DEX 對癌細胞株的生長以及化學藥物感受性異質性影響的機轉或決 定性因子(determinant factor),我們研究皮質類固醇受體共同協調因子(steroid receptor co-regulator)在這些細胞的表現。我們發現這些對 DEX 有著不同反應的癌細 胞中皮質類固醇受體共同協調因子(steroid receptor co-regulator)的表現各有不 同。而且其中有許多共同協調因子之表現量本身亦受到皮質類固醇受體所影響。 6. 利用即時定量 RT-PCR 測定,以及利用免疫組織化學染色檢驗一百多位病患的(肺癌、乳 癌、子宮頸癌)癌細胞檢體我們發現在不同病人的癌細胞中的皮質類固醇受體含量有高 有低。我們推測臨床上有一定比例之癌細胞含有高濃度皮質類固醇受體,並可能對 DEX 有感受性。 利用免疫組織染色測定癌病患癌細胞檢體,我們發現: 1. 在不同病人的癌細胞中的皮質類固醇受體含量有高有低。我們推測臨床上有一定比例 之癌細胞含有高濃度皮質類固醇受體,並可能對 DEX 有感受性。 2. 在非小細胞肺癌的患者中,癌細胞中的皮質類固醇受體含量較高者其臨床預後較佳。 關鍵詞:皮質類固醇、癌細胞、化學藥物感受性
I
Abstract
Objectives: Glucocorticoids (GCs) are commonly co-administered with anti-cancer drugs such as cisplatin to prevent drug-induced allergic reaction, nausea, and vomiting. But little is known regarding the effects of GCs on the growth and chemosensitivity of common carcinomas cells. Methods: Fourteen carcinoma cell lines representing breast (MCF-7, MCF-7/MXR1,
MCF-7/TPT300), gastric (AGS, N87,SNU1), lung (H460), cervical (SiHa, HeLa, Caski), liver (Hep3B, Hut7), and nasopharyngeal (NPC-TW01, NPC-TW04) cancer were selected to assess the effects of dexamethasone (DEX) on the cell growth and cisplatin chemosensitivity of
common human cancers. Immunohistochemical stain of tissues and cells were done by PA1-511A, an anti-GR monoclonal antibody.
Results: DEX had mutually exclusive effects on either growth or cisplatin sensitivity in 7 of the 14 cell lines. DEX inhibited cell growth of 4 (MCF-7, MCF-7/MXR1, MCF-7/TPT300, and HeLa), increased cisplatin cytotoxicity of one (SiHa), and decreased cisplatin cytotoxicity of 2 (H460 and Hep3B) cells lines. Although the effect of DEX on these carcinoma cells was
unexpectedly diverse, it remained GC receptor (GCR) dependent. The GCR contents of the 7 cell lines affected by DEX were significantly higher than those of the other 7 cell lines unaffected by DEX (5.2±2.5×104 vs 1.3±1.4×104, P=0.005).Only two DEX-unresponsive cell lines
(NPC-TW01 and NPC-TW04) had GCR contents at the high range as those of the 7
DEX-responsive cell lines. On further examination, the function of the endogenous GCR of these two cell lines was found to be impaired. Further, transfection and expression of a vector encoding GCR to AGS, a GCR low-expressing and GC non-responsive cell line, increased its susceptibility to DEX manifested as an increased resistance toward cisplatin. The cytotoxicity-enhancing effect of GC in SiHa cells correlated well with its effect on abrogating the cisplatin-induced activation of NF-κB. Expression of a dominant-negative truncated IκBα gene in SiHa cells completely abolished the cytotoxicity-enhancing effect of DEX. Conclusions: GCs may affect growth or chemosensitivity of carcinoma cells containing high concentration of functional GCR. Although the effects are heterogeneous and currently unpredictable , our data underscore the importance of clarifying the impact on tumor control by the co-administed GCs to carcinoma patients
receiving chemotherapy. The expressions of the steroid receptor co-regulators of these cells are examined. Correlation with the difference between expression of the coregulators and DEX responsiveness were also examined. Furthermore, the expressions of some of the co-regulators were influenced by the GCR. In human cancer samples, we demonstrated that some of the breast, lung and uterine cervical cancer do express high level of GCR. In MCF7 cells, we found DEX induced p21 up-regulation and caused G1 phase arrest of MCF-7. Addition of excess amounts of a structure homologue of DEX, RU486, completely abolished the growth suppression effect of DEX, suggesting that DEX act via GCR-related signal transduction pathways. Furthers, DEX has no effect on the growth of MCF-7/GCR(-), an MCF-7 subclone contains vary low levels of GCR (<1x103/cell). Compared with MCF-7, MCF-7/GCR(-) contains no detectable level of CBP300, HDAC1, and significantly lower levels of NCOR1, TIF2, GCN5L2, and ARA70. Transfection of GCR RNAi to MCF-7 cells also resulted in no detectable level of CBP300, HDAC1, and
significantly lowers levels of NCOR1, TIF2, GCN5L2, and ARA70. Transfection of human GCR
to MCF-7/GCR(-) restored the expression of GCR and all these co-regulators and sensitivity to DEX in MCF-7/GCR(-) cells. Chromosome IP with anti-GCR antibody and PCR study showed positive result with TIF-2, imply the possibility of direct regulation of TIF-2 expression by GCR.
Immunohistochemical studies of human cancer tissues showed that 5 of the 45 (11.1%) breast cancer and 43 of the 85 (50.6%) non-small cell lung cancer had high GR contents at the ranges of the glucocorticoid-responsive carcinoma cell lines. High GR expression was detected in 51% of the tumor specimens. The difference in tumor GR expression was not associated with cell type, gender, age, or stage. The outcome was significantly superior for patients whose tumor showed high GR expression compared to those with either low expression or non-expression. The median progression-free survival was 8.0 vs. 5.6 months (p=0.039) and overall survival was 18.1 vs. 10.2 months, (p=0.003), respectively. Almost all these patients have received GC as
antiemetics or allergic preventive treatment during chemotherapy courses, therefore, the effect of GC on the chemosensitivity in vivo was not evaluable.
Conclusions: GCs may affect growth or chemosensitivity of carcinoma cells containing high
concentration of functional GCR. Although the effects are heterogeneous and currently
unpredictable, our data underscore the importance of clarifying the impact on tumor control by the co-administed GCs to carcinoma patients receiving chemotherapy. It is mandatory to identify the molecular and cellular markers that help predict the diverse effect of GCs on carcinoma cells.
Keywords: Glucocorticoids, Glucocorticoid receptor, Carcinoma. Cell growth, Chemosensitivity, Drug resistance.
目錄 前言 page 1 研究目的 page 1 文獻探討 page 1-2 研究方法 page 2-6 結果 page 6-9 討論 page 9-11 圖表 page 12-17 參考文獻 page 18-20
IV
一、前言
Although glucocorticoids (GCs) are effective in inducing apoptosis via yet uncharacterized pathways in many hematological malignancies, they are considered not affecting the grwoth of most non-hematological solid tumors, such as carcinomas. However, in such tumors,
co-administration of GC with anti-cancer drugs; such as taxanes and platinums, is a common clinical practice to prevent or treat drug-induced allergic reaction or nausea/vomiting. GC is also commonly used in cancer patient for palliating the symptoms such as tumor compression of central nervous system, tumor bone metastases-related hypercalcemia, and tumor pain.
Therefore, the potential effect of GCs on the pharmacodynamic of anti-cancer drugs is clinically important.
二、研究目的
We have recently demonstrated that GC has important effect on the growth and chemosensitivity of carcinoma cells. However, the mechanisms of these effects and the determinants for the mode of effect (increase or decrease chemosensitivity, or growth inhibition) of GC on carcinoma cells remain elusive. In this study, we explored the possible upstream and downstream mechanisms which lead to the diverse effect of GC on carcinoma cells. And, further, we try to identify possible molecular classification which may help predict the modes of response to GC of carcinoma cells. We also try to establish the standard method of GR quantitative measurement in tumor tissue paraffin block samples, and to determine the GR expression in different human carcinoma tissue. The correlation of GR expression and prognosis, and correlation of GC treatment and outcome were also studied.
三、文獻探討
Although GC receptor (GCR) is ubiquitous in cancer cells and GC receptor has been linked to signal transduction pathways pertinent to cell growth, defense, and apoptosis, little is known regarding the effects of GC on the growth and chemosensitivity of common human carcinomas. There were only sporadic studies showing rather diverse effect of GC on the chemosensitivity in non-hematological neoplastic cells. Wolff et al. reported that dexamethasone (DEX) induced drug resistance toward cisplatin in C6 glioma cells. Weller et al. also reported a DEX-mediated cytoprotection in glioma cell lines. On the other hand, Benckhuijsen et al. reported an
enhancement of melphalan cytotoxicity by DEX in melanoma cells. However, the majority of carcinomas have not been studied, and the downstream mechanism by which DEX affect the chemosensitivity remain elusive.
GC has diverse biological functions, including effects on metabolism, immune system, and the central nervous system. GC exerts its biologic effects via GCR, an intracytoplasmic
glucocorticoid receptor. Upon binding with its ligands, the cytoplasmic GCR enters the nucleus, dimerize, and bind to specific DNA sequences, the glucocorticoid response elements (GREs), and activates the transcription of target genes harboring GRE. However, many effects of GC, such as anti-inflammation and immunosuppression are achieved by inhibition rather than activation of the expression of target genes. Many negatively regulated genes involved in the inflammatory
response do not contain GREs in their promoters and therefore must be regulated by a different mechanism. Recently, the transcriptional interference between GCR and other transcription factors, such as AP-1 and nuclear factor NF-κB, have been demonstrated. GCR has been shown to physically interact with Rel A, the subunit of NF-κB, and thereby suppressed the activation of NF-κB. Another mechanism by which GC suppresses NF-κB activity has been recently
described. GC was shown to induce transcription of the IκB gene, and resulted in increased synthesis of the IκBα protein, which interacts with activated NF-κB and thereby terminating the NF-κB response. The suppression of NF-κB activity has been suggested to be the major mechanism of anti-inflammation of GC. On the other hand, NF-κB was suggested to be an important transcription factor related to drug resistance. Over-expression of NF-κB, which turns on genes involved in the body’s response to inflammation, infection, and stress, conferred cancer cells with drug resistance via an uncharacterized mechanism. In our recent studies, we were able to demonstrate that GC enhance the chemosensitivity of a cervical carcinoma cells via suppression of NF-κB.
In non-small cell lung cancer (NSCLC), taxanes and cisplatin are the major
chemotherapeutic agents; and GC has been widely used before and during chemotherapy with these agents to reduce side effects. However, concerns about the effect of GC on tumor growth and chemosensitivity have been raised recently. Several studies have shown diverse effects of GC on chemosensitivity in NSCLC cell lines. GC has been reported to inhibit cell growth and
decrease chemosensitivity in NSCLC cells. On the other hand, it has also been reported that pretreatment with dexamethasone (DEX) may increase antitumor activity of carboplatin and gemcitabine in tumor xenografts possibly due to increased intra cancer cell drug accumulation.
四、研究方法
Cell Culture and Chemicals
SiHa cells (human cervical carcinoma), HeLa, Caski cells (human cervical carcinoma), H460 cells (human lung carcinoma), Hep3B, Hut 7 cells (human hepatocellular carcinoma), and MCF-7 cells (human breast cancer) were obtained from the American Type Culture Collection (Rockville, MD). The MCF-7/MXR1 and MCF-7/TPT300 cells were derived from MCF-7 by selection for growth in increasing concentrations of mitoxantrone or topotecan, respectively. MCF-7/MXR1 cells were gifts from Dr. Kenneth Cowan (National Cancer Institute, USA). MCF-7/TPT300cells were selected as previously described. NPC-TW01 and NPC-TW04 cells (nasopharyngeal cancer) were obtained as previously described. They were maintained in Dulbecco's Modified Eagle's Medium supplemented with 2 mM glutamine, 100 U/ml penicillin and 100 µg/ml streptomycin (Sigma Chemical Co., St. Louis, MO), and 10% heat-inactivated fetal bovine serum (Life Technologies, Inc., Gaithersburg, MD). AGS, N87, and SNU1 cells (human gastric cancer) were obtained from the American Type Culture Collection (Rockville, MD) and maintained in RPMI1640 (Sigma Chemical Co.) supplemented with 2 mM glutamine, 10% fetal bovine serum, 100 U/ml penicillin and 100 µg/ml streptomycin. Cisplatin was obtained
from Pharmacia-Upjohn (Kalamazoo, MI). DEX was purchased from Sigma Chemical Co., and [3H] DEX (specific activity 35-50 Ci/mmol) was from Blossom Biotechnologies Inc (Blossom, TX).
Cytotoxicity Assay
The in vitro growth inhibitory effects of the drugs in all 14 cell lines were determined by the MTT assay as previously described with slight modification. Briefly, cells were plated in 96-well plates at 5 x 103 cells/well. After overnight incubation, various concentrations of drugs were added in triplicate samples to each culture. Cells were exposed to drugs continuously. After 3-4 days of culture, when cells in drug-free wells reached 90% confluency, 50 µl of 2.5 mg/ml MTT (Sigma Chemical Co.) in PBS was added to each well, followed by incubation for 4 hours at 37°C. The formazan crystals were dissolved in DMSO. The absorbance was determined with an ELISA reader at 540 nm. Absorbance values were normalized to the values obtained for the vehicle-treated cells to determine the percentage of survival. Each assay was performed in triplicate.
Measurement of GCR Content
The GCR content was measured by a whole-cell binding assay as previously described with minor modification. Briefly, cells with 90% confluency were subcultured and allowed to grow overnight, and then trypsinized and suspended in culture medium containing 10% fetal bovine serum (pH 7.2) to a density of 1~10 × 106 cells per ml. Cells were exposed to various
concentrations of [3H] DEX from 1 to 100 nM in the presence or absence of 10 µM unlabeled DEX, followed by incubation for 1 hr at 37°C and harvested by centrifugation at 1,200 x g for 1 min. Cells were then washed three times in 3.0 ml of Hank’s balanced salt solution and finally suspended in 1.6 ml of the same solution. A 0.2 ml aliquot of this suspension was used for the determination of cell number, and 1.0 ml was assayed for radioactivity by a liquid scintillation counter. The presence of at least 200-fold excess of unlabeled DEX effectively competed out all of the binding of [3H] DEX to specific GCR. The difference in disintegrations per minute per cell between those samples incubated with [3H] DEX alone and those with 200-fold excess of
unlabeled DEX represented the binding of [3H] DEX to specific GCR. Using the specific activity of [3H] DEX, the number of receptors per cell was calculated, assuming that each receptor binds to one DEX molecule.
Transfection of Reporter Gene and Expression Vector
The human GCR-expressing plasmid, pS-hGR, and the luciferase reporter plasmid, MMTV reporter plasmid were gift from Prof. Chawnshang Chang (George H.Whipple Laboratory for Cancer Research, University of Rochester, Rochester). The MMTV reporter plasmid contains the 1.4-kb MMTV LTR which encompasses the natural GRE sequences, fused to the sequence coding for luciferase. It has been demonstrated previously that GR stimulate the rate of
transcription of MMTV LTR . Moreover, GCR bind specifically to DNA sequences mapped within the MMTV LTR (i.e. GRE), which can confer GC responsiveness to a heterologous promoter. MCF-7, TW01, TW02, AGS, and SiHa cells were transfected by Lipofectamine 2000 (Life Technologies, Inc. [GIBCO BRL], Gaithersburg, MD) according to the manufacturer’s protocol. The stable clones was selected by 400 µg/ml hygromycin for 20 days. Single cell clones were obtained by limiting dilution of the hygromycin-resistant cells. In the MMTV reporter assay, MCF-7, TW01 and TW04 cells were either transiently transfected with MMTV reporter plasmid cells, or co-transfected with MMTV reporter plasmid and pS-hGR (in a ratio of 5:1). Forty eight hours after transfection, 1 x 105 transfected cells were stimulated with 1 µM DEX and incubated for an additional 6 hours. Reporter gene activity was determined with the Reporter Luciferase Assay System (Packard, Netherlands). In the study of increasing the GCR content in AGS cells, the AGS cells were transfected with the pS-hGR. The stable clones were selected by 400 µg/ml hygromycin for 20 days. Single cell clones were obtained by limiting dilution of the
hygromycin-resistant cells.
Western Blot Analysis
Cells were plated in 6 cm dishes at a density of 1 x 106 cells/dish. After incubation with DEX for the indicated time periods, the cells were harvested. Whole cell lysates and nuclear extracts were prepared according to the method of Staal et al. Protein concentration was determined by Bradford assay. Immunoblotting of GR and β-actin was performed using rabbit polyclonal antibodies purchased from Santa Cruz Biotechnology (Santa Cruz, CA). Signals were visualized with an enhanced chemiluminecence kit followed by exposure to X-ray films.
Electrophoretic mobility shift assay (EMSA) for NF-κB.
[α- 32P]dCTP end-labeled double-strand oligo-deoxyribonucleotides (5’-GGATTGGGACTT TCCCCTCC-3’ and 3’-CCTAACCCTGAAAGGGGAGG-5’ ) were used as the binding
substrates for NF-κB. The preparation of nuclear extracts for EMSA was performed according to the method of Andrews and Faller. Nuclear extracts of SiHa cells (10 µg per assay) were
incubated with 10,000 cpm of probe (0.1 to 0.5 ng) and 1 µg poly(dI-dC) for 30 min at room temperature with a final reaction mixture of 15 µl containing 20 mM HEPES, (pH7.5), 100 mM KCl, 0.2 mM EDTA, 20% glycerol, 1mM dithiothreitol, and 1 µg/µl BSA. Samples were analyzed in a 5% polyacrylamide gel with 0.25 x TBE as running buffer, and run at room temperature at 150 V for 2~ 2.5 h. The nuclear extract from TNF-α-treated SiHa cells was used as positive control. Antibody to p65 (Rel A) was added to the reaction mixture before the addition of labeled probe for supershift analysis. After electrophoresis, gels were dried and
autoradiographed for 12 hours at -70°C.
Transfection of reporter plasmid and measurement of luciferase and reporter gene activity.
The luciferase reporter plasmid, pM-Luc, contains the 1.4-kb MMTV LTR which encompasses
the natural GRE sequences. The other luciferase reporter plasmid, pRκB-Luc, contains five NF-κB sites followed by a TATA box. These plasmids both contain the hygromycin resistance gene from SV2hygro. SiHa cells were transfected by Lipofectamine 2000 (Life Technologies, Inc. [GIBCO BRL], Gaithersburg, MD) according to the manufacturer’s protocol. The stable clone was selected by 400 µg/ml hygromycin for 20 days. Single cell clones were obtained by limiting dilution of the hygromycin-resistant cells. The SiHa/κB-reporter cell line was selected on the basis of TNFα- induced luciferase activity and constitutive β-galactosidase activity. For each time point, 1x105 SiHa/κB-reporter cells were stimulated with 10 ng/ml TNFα or cisplatin (20 and 200 µM) and incubated for an additional 6 hours. Reporter gene activity was determined with the Reporter Luciferase Assay System (Packard, Netherlands).
Transfection of dominant-negative IκBα.
The dominant-negative truncated IκBα (dnIκBα) cDNA was constructed by deletion of amino acids residues 1 to 70, which contain the phosphorylation sites (serine residues 32 and 36) of IκB kinases (IKKs) and ubiquitin binding sites (lysine residues 21 and 22). This cDNA was inserted into the vector pRCMV (purchased from Invitrogen) followed by the CMV promoter. The empty vector was used for the generation of control cells. SiHa cells were transfected by lipofectamine 2000 (Life Technologies, Inc. [GIBCO BRL], Gaithersburg, MD) according to the manufacturer’s protocol. The stably transfected SiHa cells were pooled by hygromycin selection for 20 days after transfection. The experiments examining the effect of DEX on the growth of these cells were performed within 30 days of each transfection.
Examine the corregulator expression in carcinoma cell line
The expression of 27 coregulators were examined by RTPCR. Immunohistochemical stain for GCR and Transfection of GCR RNAi expression vector into MCF-7 and transfection of GCR-Expressing Vector into MCF-7/GCR(-) by Lipofectamine 2000. Chromatin
immuno-precipitate with anti-GCR antibody and then PCR for CBP300, HDAC1, NCOR1, TIF2, GCN5L2, and ARA70.
GR Immunohistochemistry Study
Paraffin sections were dewaxed and rehydrated, and antigens were retrieved by microwaving sections in 0.01M sodium citrate buffer for 20 min. Endogenous biotin was blocked by normal goat serum (DAKO Ltd.). Slides were then incubated with anti-GR antibody (PA1-510A, 511A and 512, Affinity BioReagents, Golden, CO). The DAKO Envision system (Copenhagen,
Denmark) was used to further avoid endogenous biotin contamination. Sites of bound peroxidase were visualized using liquid 3’, 5’-diaminobenzidine (DAKO, Glostrup, Denmark) and
counterstained with hematoxylin. Under this staining condition, only carcinoma cells with high (>10,000 sites/cell) GR content were positively stained (12). Tumor tissue samples were considered to have high GR expression when more than 20% of tumor cells were positively stained.
Statistical Analysis
Fisher’s exact test or chi-square test was used to analyze the correlations between GR immunoreactivity and clinicopathologic variables as well as response to chemotherapy. The Kaplan-Meier method was used to generate survival curves, and differences in survival were analyzed using the log-rank test, based on the GR expression status. Data management and statistical analyses were performed using SPSS software for Windows 11.0 (SPSS, Inc., Chicago, IL). A probability of error < 5% was regarded as significant.
五、結果
DEX Affects Either Growth or Chemosensitivity in 7 of the 14 carcinoma Cell Lines
DEX (0.01-1.0µM) inhibited cell growth in MCF-7, MCF-7/MXR1, MCF-7/TPT300, and HeLa cells. However, DEX alone, up to 20 µM, was not toxic to the other 10 cell lines, including AGS, N87, SNU1, SiHa, Caski, Hep3B, Hut 7, TW01, TW04, and H460. The latter 10 cell lines were further tested for the effect of GC on the chemosensitivity of carcinoma cells toward cisplatin, doxorubicin, 5FU, and taxol. Pretreatment of SiHa cells with 1 µM DEX for 3 hours decreased the IC50 of cisplatin from 18.6±1.9 µM to 9.7±2.0 µM. This cytotoxicity-enhancing effect could be observed even when the concentration of DEX was as low as 1 nM (data not shown). In contrast, DEX slightly decreased chemosensitivity toward cisplatin, doxorubicin, 5-FU, and taxol in H460 and Hep3B cells. DEX had no effect on the chemosensitivity of AGS, N87, SNU1, Hut-7, Caski, NPC-TW01, and NPC-TW04 cells.
GC Effect Correlates well with GCR Content of the Cells
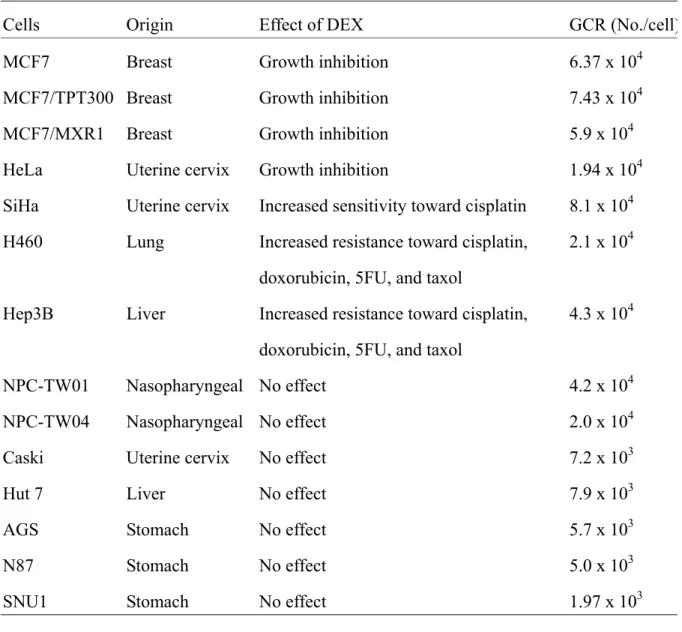
The GCR contents of these 14 cell lines are listed in Table 1. The GCR contents of the 7 cell lines affected by DEX were significantly higher than those of the other 7 cell lines unaffected by DEX (5.2±2.5 ×104 vs. 1.3±1.4 ×104, P=0.005) suggesting GCR is one of the pivotal mediators of the effect of DEX on carcinoma cell. The GCR content of human lymphocytes, the internal control for these experiments, was parallely tested and was within the reported range (2,500 ~ 5,400 sites/cell) [19].
GC-unresponsive GCR-rich Carcinoma Cells Have Dysfunctional GCR
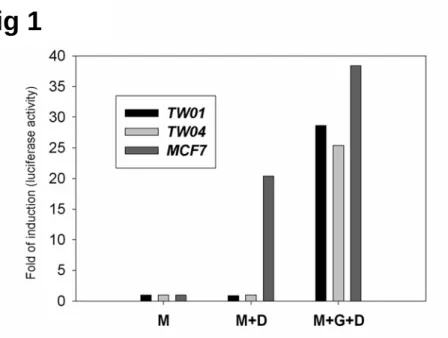
As shown in Table 1, we noticed that DEX had no effect on NPC-TW01 and NPC-TW04, two cell lines with GCR content as high as that of the 7 GC-responsive cell lines. The function of the GCR in these two cell lines was further examined. As shown in Fig. 1, MCF-7 cells contained endogenous DEX-responsive GCR while NPC-TW01 and NPC-TW04 cells did not. Further, when NPC-TW01 and NPC-TW04 cells were co-transfected with MMTV reporter plasmid and pS-GCR, which contains functional human GCR gene, the response to DEX was restored (Fig 1). These data strongly suggested that the function of endogenous GCR of NPC-TW01 and
NPC-TW04 cells was probably impaired.
Expression of GCR in GCR-poor Cells Increases its Responsiveness to DEX
To further examine whether the GCR content is pivotal in mediating the susceptibility to DEX in carcinoma cell, we transfected pS-hGR to AGS cells, a GCR low-expressing cell line. The GCR content in empty vector-transfected AGS cells, and pooled stably pS-hGR-transfected AGS cells were 5.2 x 103/cell and 1.42 x 104/cell, respectively. Treatment of DEX alone has no effect on cell growth in these cells. However, as shown in Fig. 2, pS-hGR transfected AGS cells that expressing high GCR content became susceptible to the effect of DEX with increasing drug resistance toward cisplatin. The GCR content in single cell cloned pS-hGR transfected AGS cells clone 1, 2, and 3 were 1.54 x 104/cell, 1.32 x 104/cell, and 5.8 x 103/cell, respectively. The cells that express high GCR content (clone 1 and clone 2) were susceptible to the effect of DEX with increasing resistance toward cisplatin, but the cells which express low GCR content (clone 3) remained non-susceptible to DEX treatment
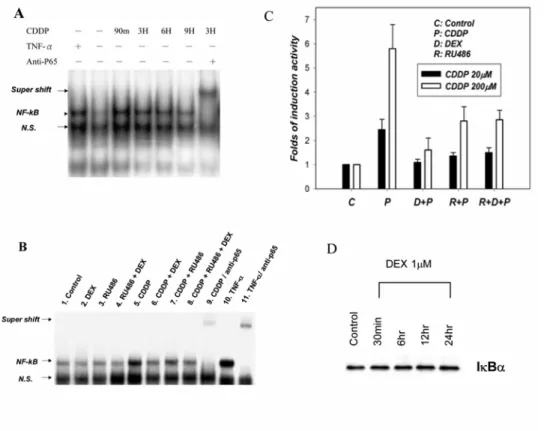
DEX Suppressed Cisplatin-induced NF-κB Activation in SiHa Cells
To explore the mechanism underlying the chemosensitizing effect of DEX in SiHa cells, EMSA assay of NF-κB DNA binding activity and reporter luciferase assay of NF-κB
transcription activity were done. As shown in Fig. 3A, NF-κB DNA binding activity transiently increased after exposure to 20 µM (IC50) cisplatin. This NF-κB DNA binding activity was blocked by pre-incubating the cells with 1 µM DEX (Fig. 3B). While RU486 alone had some intrinsic effect on the suppression of NF-κB, it could only partially reverse the effect of DEX on the suppression of NF-κB DNA binding activity (Fig. 3B). The transactivating activity of NF-κB on its cis elements was further verified in SiHa cells stably transfected by a reporter construct containing five NF-κB binding sites. Treatment with cisplatin (20~200 µM) resulted in the induction of luciferase activity, which could be repressed by pretreatment with DEX. Again, RU486 could partially reverse the effect of DEX on the repression of NF-κB activity, while RU486 alone had some intrinsic effect on the repression of NF-κB activity (Fig. 3C). The effect of DEX on the IκB expression in SiHa cells was also examined. Western blot analysis of
whole-cell protein showed that DEX did not upregulate the expression of IκB in SiHa cells (Fig. 3D). By contrast, in other cell lines, NF-κB was either not activated by TNF-α or cisplatin (H460), or cisplatin-activated NF-κB was not suppressible by DEX (Hep3B, AGS, SNU1, and N87). These data suggest that protein-protein interaction between activated GCR and NF-κB plays a central role in the chemosensitizing effect of DEX in SiHa cells.
Inhibition of NF-κB Activation Blocks the Cytotoxicity-enhancing Effect of DEX in SiHa
Cells
To further examine the role of NF-κB in the cytotoxicity-enhancing effect of DEX, we generated a re-combinant plasmid containing dominant negative IκBα (dnIκBα) gene. This dnIκBα protein does not contain the residues necessary for signal-induced phosphorylation and proteasome-mediated degradation of IκBα, thereby preventing dissociation and translocation of NF-κB to the nucleus. The expression of the dnIκBα in pooled stably transfected SiHa cells was verified by Western blot analysis. As shown in Fig. 4A, the control-pRCMV-transfected SiHa
cells contained only the endogenous wild-type IκBα protein, while the dnIκBα-pRCMV-transfected SiHa cells contained an additional band representing the truncated exogenous IκBα protein. Results of EMSA showed that NF-κB binding activity was markedly suppressed in the dnIκBα-pRCMV-transfected cells after either TNF-α or cisplatin treatment (Fig. 4B). In addition, as shown in Fig. 4C, the cytotoxicity-enhancing effect of DEX in dnIκBα-pRCMV-transfected SiHa cells was abolished. The dnIκBα-pRCMV-transfected SiHa cells had also become more sensitive to cisplatin as compared to the control-pRCMV-transfected SiHa cells(Fig. 4C). These data confirmed that NF-κB plays a central role in the chemosensitizing effect of DEX in SiHa cells. We also examined the protein-protein interaction by immunoprecipitation study. We found that the expression of IkB was not influenced by the treatment of DEX. However, the immunoprecipitate study did show that the GCR physically interact with the NFkB in SiHa cells. The histidine tag pull-down assay showed that there is interaction between the C-terminal of GCR and the NFkB.
Expression Profiles of the Co-regulators the 14 Carcinoma Cell Lines
In order to explore the mechanism and the determinant factor on the diverse effect of DEX effect on the cancer cells, we examined the expression of 21 steroid receptor co-regulators in these 14 carcinoma cell lines. The 14 carcinoma cancer cells represented 4 groups of different DEX responses; including growth inhibitory, increase chemsensitivity, decrease chemosensitivity, and DEX non-responsive. The co-regulators including: coactivators: SRC1, (NCOA1), TIF2a (NCOA2), AIB1 (NCOA3), ARA70 (NCOA4), ARA54 (RNF14), TIF1, CARM1, SRCAP P300 (EP300), CBP (CREBBP), GCN5L2, PCAF, BRG1(SMARCA4), hBRM (SMARCA2), SNF5 (SMARCB1), BAF60b (SMARCD2), Corepressors: NCOR1, SMRT (NCOR2), REA, HDAC1, HDAC2, HDAC3, SIN3B (KIAA0700), SAP18, SAP30, MTA1, MTA1L1. We found that the expression levels of these co-regulators are different in different groups of cancer cells. The correlation of these different expressions in co-regulator there the diverse DEX responsiveness are under further investigation. We also found that the expression of some of the co-regulator is regulated by the GCR. The detail pathway of the regulation is under investigation.
Expression of GCR in Carcinoma Cell Lines and Human Cancer Tumor Samples
Glucocorticoids (GC) enhance p21 expression and induce G1 phase cell cycle arrest in MCF-7 cells. The possible role of GC receptors and their co-regulator
We found that dexamethasone (DEX), at clinically achievable concentration (0.01-1.0µM) inhibits cell growth of MCF-7 cells while induces no cellular apoptosis.
DEX induced p21 up-regulation and caused G1 phase arrest of MCF-7. Addition of excess amounts of a structure homologue of DEX, RU486, completely abolished the growth suppression effect of DEX, suggesting that DEX act via GCR-related signal transduction pathways. Furthers, DEX has no effect on the growth of MCF-7/GCR(-), an MCF-7 subclone contains vary low levels of GCR (<1x103/cell). Compared with MCF-7, MCF-7/GCR(-) contains no detectable level of CBP300, HDAC1, and significantly lower levels of NCOR1, TIF2, GCN5L2, and ARA70.
Transfection of GCR RNAi to MCF-7 cells also resulted in no detectable level of CBP300,
HDAC1, and significantly lowers levels of NCOR1, TIF2, GCN5L2, and ARA70. Transfection of human GCR to MCF-7/GCR(-) restored the expression of GCR and all these co-regulators and sensitivity to DEX in MCF-7/GCR(-) cells. Chromosome IP with anti-GCR antibody and PCR study showed positive result with TIF-2, imply the possibility of direct regulation of TIF-2 expression by GCR.
Tumor tissues of common human carcinomas may express high level of GR
GR expression was examined by immunohistochemical stain in the carcinoma cell lines, and tumor tissue samples of human breast cancer and human non-small cell lung cancer (NSCLC). Positive GR immunoreactivity (representing high GR content) was observed in 5 of the 45 tumor samples (11.1%) of breast cancer and 43 of the 85 tumor samples (51%) of non-small cell lung cancer patients. The GR expression in various tumor tissues was listed in Table 2.
In tumor tissue samples of human NSCLC, positive GR immunoreactivity, as defined in our previous report, was observed in 43 of the 85 tumor samples (51%) of NSCLC patients. The clinicopathological features of the 85 patients are examined and the difference in tumor GR expression was not associated with cell type (squamous cell carcinoma vs. adenocarcinoma or large cell carcinoma), gender, age, or stage. Correlation of tumor GR expression with NSCLC patient’s outcome were examined. Outcome was significantly superior for patients whose tumors showed high GR expression compared to those with either low or non-expression of GR. The progression-free survival and overall survival are shown in Fig. 5A and Fig. 5B. The median progression-free survival was 8.0 vs. 5.6 months (p=0.039 by the log-rank test) and overall survival was 18.1 vs. 10.2 months, (p=0.003 by the log-rank test), respectively. The
chemotherapy response (complete remission and partial remission) rate was 26.2% vs. 44.3% (p=0.083 by chi-square test). These results suggest that tumor GR expression may affect the outcome of patients with advanced NSCLC. However, as almost all patients (83/85, 97.6%) received GC treatment before chemotherapy as antiemetics or allergic preventive treatment, we could not determine whether the better prognosis of NSCLC patients whose tumors showed high GR expression was related to the effect of GC on chemosensitivity.
六、討論
This study has demonstrated that GC affects either growth or chemosensitivity in a
substantial portion of carcinoma cells. Since GCs are commonly co-administered with anticancer drugs such as taxanes and platinums, how GC alter the effect of chemotherapy may have to be taken into consideration in clinical practice. As shown in this study, it may not be difficult to identify those carcinoma patients of whom tumor response is going to be affected by GC, since only cells with high GCR content are affected. However, how GC will actually affect the growth of tumors of these cancer patients remains uncertain since the effects of GC, as disclosed in this study, are extremely diverse and without useful cellular or molecular predictors.
A direct correlation between GCR content of the cells and the magnitude of physiologic response to GC has been reported in hematologic malignancies. The sensitivity of many lymphoid cell lines to GC-induced growth arrest and apoptosis is directly proportional to
intracellular receptor content. Several studies also identified a correlation between reduced GCR expression and a poor treatment response as well as poor prognosis in patients with acute
lymphocytic leukemia, suggesting that reduced GR expression could lead to clinical
glucocorticoid resistance. Our study demonstrated that the susceptibility to the effect of DEX on cell growth or chemosensitivity in carcinoma cells is also correlate well with the level of GCR content. However, the GCR contents of the GC-responsive carcinoma cells are almost 10 times higher than that of lymphoid cells, suggesting that the cellular contexts or the signal transduction pathways for the interaction of GC and GCR are probably different between these two groups of cells.
In this study, the only two cell lines, NPC-TW01 and NPC-TW04, which have relatively high GCR content but not susceptible to the growth regulatory effect of DEX, were found to have non-functional endogenous GCR. Previous studies on both human and mouse cell lines have shown that somatic mutation in the GCR gene is the principal mechanism for in vitro acquisition of GC resistance. Whether NPC-TW01 and NPC-TW04 contain GCR gene mutations needs to be further elucidated.
The [3H] labeled DEX ligand binding assay has been the standard method to measure the GR content in cell lines and in vivo human leukemia samples. The GR amount measured by [3H] labeled DEX ligand binding assay is expressed as GR number per cell. However, this method is hard to apply to solid tumor tissue samples since it is difficult to quantify the cell number in tissue samples. There were other methods to detect the expression of GR in the in vivo solid tumor samples, including cytosol DCC-competitive (dextran-coated charcoal) protein binding assay, and RT-PCR. These methods all use tissue homogenizer and the results were normalized by the total protein or RNA amount. Therefore, the result was the average of the GR content of the whole tissue sample, which including the cancer cells as well as the stroma cells and adjacent normal tissues component. Besides, the cytosol DCC-competitive protein binding assay required fresh frozen tissue which limited its applicability. In this study, we have shown an ideal staining condition by which only cancer cells with high GR content were stained positively (Figure 4). We have also demonstrated that a substantial portion of common human carcinoma do express high level of GR, and therefore are potentially susceptible to the growth and
chemosensitivity-regulatory effect of GC.
Activated GCR may activate or suppress gene expression through interaction with respective positive or negative cis-acting regulatory elements in the promoters regions. Activated GR can also regulate the expression of GC responsive genes indirectively through protein-protein interactions with other transcription factors such as NF-κB and AP-1. Inactivation of NF-κB or AP-1 has been shown to alter the vulnerability of cancer cells to several cytotoxic agents. Activation of NF-κB has been implicated in mediating drug resistance of cancer cells. NF-κB
could be activated by a variety of stresses, including oxidative stress and DNA damage. Activated NF-κB may prevent the triggering of apoptosis, and thus result in drug resistance against
DNA-damaging agents. The molecular mechanism of NF-κB-mediated protection of cells remains unclear, but may involve the up-regulation of caspase inhibitors. In this study, we have provided evidence that NF-κB plays an important role in mediating the drug resistance of SiHa cells. Suppression of NF-κB activity by dnIκBα not only abolished the chemosensitizing effect of DEX, but also increased the chemosensitivity of SiHa cells to cisplatin. DEX had no effect on cells without discernable changes of NF-κB. However, it remains to be clarified why certain carcinoma cell lines do not have an NF-κB response to cisplatin or have an NF-κB response which cannot be attenuated by DEX.
Our preliminary data have indicated that suppression of NF-κB is one of the major mechanism of interacting cisplatin sensitivity in SiHa cell. However, it remains difficult to explain the diverse effect of GC on GCR-rich carcinoma cells. Although high-GCR content is necessary for a response of the cells to GC, the diversified and even contradictory effects of GC on these cells cannot be simply explained by the amount of GCR. Our findings suggest that an upstream switch point at the level of GC-GCR interaction may work to segregate the direction of downstream pathways. Recent studies on the action of androgen receptor (AR) may provide a possible example for the diverse effects of GC on carcinoma cells. Co-regulators of AR have played crucial roles in determining the ultimate activity of AR, and the presence or absence of certain co-regulators may even change the activity of anti-androgens to become androgens. Several novel co-regulators of GC have also been found to play important roles in the signaling pathway of the GCR. The possibilities that the specific presence of certain co-regulators of GCR in different carcinoma cells may dictate the ultimate effect of GC need to be clarified.
After a single oral dose of 7.5 mg of DEX, the serum concentration of DEX was found to be around 0.12 µM lasting for 1~3 hours. However, the serum concentration of DEX may reach 2 µM after a single intravenous infusion of 80~100 mg of DEX. Since the administration of
relatively high-dose DEX, at the range of 10-50 mg/day, or its equivalents, is widely used for the prevention of cisplatin-induced nausea/vomiting and taxanes-induced allergic reactions, the possible effect of GC on the chemosensitivity of some cancer patients needs to be seriously considered. In summary, the results of this study suggest that GC exerts a GCR-dependent effect on the growth or chemosensitivity in a substantial portion of carcinoma cells. The clinical relevance and the cellular mechanisms that dictate the disparate effects of GC need to be further clarified.
This study also demonstrated that tumor samples expressed high levels of GR in about half of the patients with advanced NSCLC, and this high expression of GR was correlated with better outcome in terms of progression-free survival and overall survival. This study also demonstrated that DEX has heterogeneous effects on growth or chemosensitivity to cisplatin, gemcitabine, and paclitaxel in NSCLC cell lines with high GR expression. The reason why patients with advanced NSCLC whose tumors showed high tumor GR expression had better prognosis remains unknown. In addition, since most of the patients received GC treatment as a part of antiemetic or allergic prevention before chemotherapy in this study, we could not assess whether GC treatment is safe in patients with NSCLC.
these studies have correlated clinicopathological features with GR expression in tumors. Using the cytosol DCC-competitive (dextran-coated charcoal) protein binding assay, Beattie et al. found that 75% of NSCLC expressed GR, while Chaudhuri et al. found that 30% of NSCLC expressed GR. No standard threshold for receptor positivity has been established. Besides, the cytosol DCC-competitive protein binding assay used in these studies required tissue homogenizing and the results were normalized by the total protein amount. Therefore, the result was the average of the GR content of the whole tissue sample, which included the cancer cells as well as the stroma cells and adjacent normal tissues component. Using immunohistochemistry, Kaiser et al. found that 94% (49 cases) of primary lung cancer tissues expressed GR. However in their study, all the NSCLC cell lines tested were positive for GR expression using the same immunocytochemical staining procedure, and their GR content assessed by ligand binding assay ranged from only 1100 sites/cell to 314000 sites/cell. The level of GR content may be important to the GR physiologic function of GR in malignant cells. A direct correlation between cellular GR content and the magnitude of physiologic response to GC has been reported in hematologic malignancies. Several studies also identified a correlation between reduced GR expression and a poor treatment
response as well as poor prognosis in patients with acute lymphocytic leukemia, suggesting that reduced GR expression could lead to clinical glucocorticoid resistance. In those studies, the thresholds for defining reduced GR expression were set below 8000 or 10000 sites/cell. Our previous study demonstrated that DEX exerts a GR-dependent effect on growth or
chemosensitivity in a substantial portion of carcinoma cells. Only GR-rich carcinoma cells lines (more than 10,000 sites/cell) were susceptible to DEX treatment. We also showed an ideal staining condition by which only cancer cells with high GR content were stained positively. In this study, the results of immunocytochemical staining and ligand binding assay were
well-correlated in NSCLC cell lines.
Several studies have shown diverse effects of GC on chemosensitivity in NSCLC cells. DEX has been reported to inhibit cell growth and decrease chemosensitivity in some NSCLC cell lines. Further, DEX induced cisplatin and gemcitabine resistance were observed in primary cultures of human lung carcinoma. On the other hand, pretreatment with DEX may increase antitumor activity of carboplatin and gemcitabine in tumor xenografts due to increased intra cancer cell drug accumulation. In this study, we assessed GR expression and the effect of DEX on the growth and chemosensitivity of five NSCLC cell lines. Similar to the results of our previous study in other common carcinoma cells, we found that DEX has heterogeneous effects on the growth and chemosensitivity of NSCLC cells with high levels of GR expression. It remains difficult to explain the diverse and even contradictory effect of GC on GR-rich carcinoma cells. The possibility that the specific presence of certain co-regulators of GR in different carcinoma cells may dictate the ultimate effect of GC may be worthy of exploration.
七、計畫成果自評
In the present study, we examined the effects and mechanisms of DEX on the chemosensitivity of 14 carcinoma cell lines. We also explored the expression profiles of steroid co-regulators in these cells, and examined the expression of GCR in human cancer tissue samples. The results of
this study indicate that, while GC may be co-administered with anti-cancer drugs for other reasons, the possible effect of GC on the chemosensitivity of some selected cancers may be clinically significant and requires further investigation.
The current results have been submitted for publication in the peer-reviewed journal. One of them has been accepted in World Journal of Gastroenterology and the other is considered to be accepted in Journal of Endocrinology with minor revision.
Table 1 Correlation of glucocorticoid receptor content with the effect of dexamethasone carcinoma cells
Cells Origin Effect of DEX GCR (No./cell)
MCF7 Breast Growth inhibition 6.37 x 104
MCF7/TPT300 Breast Growth inhibition 7.43 x 104
MCF7/MXR1 Breast Growth inhibition 5.9 x 104
HeLa Uterine cervix Growth inhibition 1.94 x 104
SiHa Uterine cervix Increased sensitivity toward cisplatin 8.1 x 104 H460 Lung Increased resistance toward cisplatin,
doxorubicin, 5FU, and taxol
2.1 x 104
Hep3B Liver Increased resistance toward cisplatin, doxorubicin, 5FU, and taxol
4.3 x 104
NPC-TW01 Nasopharyngeal No effect 4.2 x 104
NPC-TW04 Nasopharyngeal No effect 2.0 x 104
Caski Uterine cervix No effect 7.2 x 103
Hut 7 Liver No effect 7.9 x 103
AGS Stomach No effect 5.7 x 103
N87 Stomach No effect 5.0 x 103
SNU1 Stomach No effect 1.97 x 103
Fig. 1. Functional assay of the GCR in NPC-TW01 and NPC-TW04 cells. NPC-TW01,
NPC-TW04, and MCF-7 cells were transiently transfected with MMTV reporter plasmid (lane M and lane M+D) or co-transfected with MMTV reporter plasmid and pS-hGR (lane M+G). The cells were then treated with 1 µM DEX for 6 hours (lane M+D and M+G+D). Then the luciferase activity was assayed and represented in terms of folds of the induction activity of the control (lane M). All values represent means ± standard deviation of 3 experiments.
Fig. 2. Increased drug resistance to cisplatin in pS-hGR-transfected AGS. AGS cells were
transfected with pS-hGR and MTT assay was performed. a Western blot analysis for GR and β-actin in whole cell lysate of transfected AGS cells. Lane1: AGS/GCR-pool, lane 2: AGS/empty vector, lane 3: AGS/GCR-c1, lane 4: AGS/GCR-c2, lane 5: AGS/GCR-c3. b, c, and d
Pretreatment with DEX 1 µM for 3 hrs diminished cisplatin cytotoxicity in AGS/GCR-pool, AGS/GCR-c1, and AGS/GCR-c2 cells. e and f Pretreatment with DEX 1 µM for 3 hrs had no effect on the cisplatin cytotoxicity in AGS/empty vector cells and AGS/GCR-c3. AGS/GCR-pool: AGS cells transfected with pS-hGR, pooled cells. AGS/empty vector: AGS cells transfected with empty vector. AGS/GCR-c1 to c3: AGS cells transfected with pS-hGR, single cell cloned, clone 1 to clone 3. All values represent mean ± standard deviation of 6 separate wells.
13
Fig 2
Fig. 3. Effect of DEX and RU486 on cisplatin-induced NF-κB activity. A, Nuclear extract was
prepared and EMSA was performed as described in the Materials and Methods. Exposure of SiHa cells to cisplatin 20 µM for 3 hours resulted in activation of NF-κB activity. The TNF-α lane represents positive control. Supershift by anti-p65 antibody verifies the correct band of NF-κB. B, SiHa cells were pretreated with or without 1 µM DEX and with or without 1 µM RU486 for 24 hours. Cells were then exposed to 20 µM cisplatin for 3 hours. DEX and RU486 had no effect on NF-κB (lane 2,3,and 4). Cisplatin activated NF-κB (lane 5), but DEX pretreatment completely abolished cisplatin-induced NF-κB activation (lane 6). RU486 partially abrogated the effect of DEX, but RU486 also had some intrinsic effect in reversing cisplatin-induced NF-κB activation. C, SiHa cells were stably transfected with luciferase reporter plasmid containing five NF-κB sites as described in Materials and Methods. The SiHa/κB-reporter cells were pretreated with or without 1 µM DEX and with or without 1µM RU486 for 24 hours. Cells were then exposed to 20 or 200 µM cisplatin for 3 hours. The luciferase activity was assayed and represented in terms of folds of the induction activity of the control. All values in Fig. 3C represent means ± standard deviation of 3 experiments. D, Effect of DEX on IκBα expression. SiHa cells were exposed to 1 µM DEX for different durations before harvesting. Western blot analysis of the whole cell lysates was performed. The protein amount of IκBα was not changed after DEX treatment. Abbreviations: CDDP, cisplatin; TNF-α, tissue necrosis factor-α, N.S., non-specific binding.
Fig. 4. Effect of DEX on cisplatin-induced NF-κB activity in dominant negative IκB transfected SiHa cells. A,
Western blot analysis for IκBα in whole cell lysate of control-pRCMV-transfected SiHa cells and
dnIκBα-pRCMV-transfected SiHa cells. An additional band in the lane of dnIκBα-pRCMV-transfected SiHa cells represents of the exogenous truncated IκBα protein. B, Nuclear extract was prepared and EMSA was performed as described in Materials and Methods. Exposure of control-pRCMV-transfected cells to cisplatin 20µM 3 hours or TNF-α 30 minutes resulted in activation of NF-κB (lane 3, 4), which was suppressible by DEX 1 µM pretreatment (lane 8). Super-shift by anti-p65 antibody verifies the correct band of NF-κB (lane 1). The NF-κB activity was not increased in dnIκBα-pRCMV-transfected SiHa cells exposed to TNF-α and cisplatin (lane 6, 7). C, Effect of DEX on the chemosensitivity in dominant negative IκB transfected SiHa cells. Cell numbers were measured by MTT assay and plotted as a percentage of the control (cells not exposed to the drugs). The control-pRCMV-transfected SiHa cells pretreated with DEX for 24 hours were still more sensitive to cisplatin. However, the cytotoxicity-enhancing effect of DEX in dnIκBα-pRCMV-transfected SiHa cells was abolished.
Table 2
Figure 5
17
High GR expression Low (or - )GR expression
NSCLC 43 52 NPC 42 65 Cervical cancer Squamous 23 7 Adenocarcinoma 0 8 Breast cancer adenocarcinoma 5 39 phyllodes sarcoma 11 2
Metaplastic carcinoma 15* (in non-adenocarcinoma part) 1
Esophageal cancer
Squamous 12 6
Adenocarcinoma 0 11
八、參考文獻
1. Haskell, C. M. Antineoplastic agents. In: Haskell, C. M., Break, J. S.(eds.), Cancer Treatment, forth edition, pp. 105-106. Philadelphia: W. B. Saunders, 1995.
2. Wood, A. C., Waters, C. M., Garner, A., and Hickman, J. A. Changes in c-myc expression and the kinetics of dexamethasone-induced programmed cell death and apoptosis in human
lymphoid leukemia cells. Br. J. Cancer, 69: 663-669, 1994.
3. Schwartzman, R. A. and Cidlowski, J. A. Mechanism of tissue-specific induction of
internucleosomal deoxyribonucleic acid cleavage activity and apoptosis by glucocorticoids. Endocrinology, 133: 591-599, 1993.
4. Wright, A. P., Zilliacus, J., McEwan, I. J., Dahlman-Wright, K., Almlof, T., and
Carlstedt-Duke, J. Structure and function of the glucocorticoid receptor. J. Steroid Biochem. Mol. Biol., 47: 11-19, 1993.
5. Schwartzman, R. A. and Cidlowski, J. A. Glucocorticoid-induced apoptosis of lymphoid cells. Int. Arch. of Allergy Immunol., 105: 347-354, 1994.
6. McEwan, I. J., Wright, A. P., and Gustafsson, J. A. Mechanism of gene expression by the glucocorticoid receptor: role of protein-protein interactions. Bioessays, 19: 153-160, 1997. 7. Wolff, J. E., Denecke, J., and Jurgens, H. Dexamethasone induces partial resistance to
cisplatinum in C6 glioma cells. AntiCancer Res., 16: 805-809, 1996.
8. Weller, M., Schmidt, C., Roth, W., and Dichgans, J. Chemotherapy of human malignant glioma: prevention of efficacy by dexamethasone? Neurology, 48: 1704-1709, 1997. 9. Naumann, U., Durka , S., and Weller , M. Dexamethasone-mediated protection from drug
cytotoxicity: association with p21 WAF1/CIP1 protein accumulation? Oncogene, 17: 1567-1575, 1998.
10. Benckhuijsen, C., Osman , A. M., Hillebrand, M. J., and Smets, L. A. "Glucocorticoid effect on melphalan cytotoxicity, cell-cycle position, cell size, and [3H]uridine incorporation in one of three human melanoma cell lines". Cancer Res., 47: 4814-4820, 1987.
11. Yang, C. H., Schneider, E., Kuo, M. L., Volk, E. L., Rocch, E., and Chen, Y. C.
BCRP/MXR/ABCP expression in topotecan-resistant human breast carcinoma cells. Biochem. Pharmacol., 60: 831-837, 2000.
12. Lin, C.T., Wong, C.I., Chan, W.Y., Tzung, K.W., Ho, J. K. C., Hsu, M.M. & Chuang, S.M. (1990). Establishment and characterization of two nasopharyngeal carcinoma cell lines. Lab. Investig. 62, 713-724.
13. Lin, C.-T., Chan, W.-Y., Chen, W., Huang, H.-M., Wu, H.-C., Hsu, M.-M., Chuang, S.-M. & Wang, C.-C.(1993). Characterization of seven newly established nasopharyngeal carcinoma cell lines. Lab. Investig. 68, 716-727.
14. Carmichael, J., DeGraff, W. G., Gazdar, A. F., Minna, J. D., and Mitchell, J. B. Evaluation of a tetrazolium-based semiautomated colorimetric assay: assessment of chemosensitivity testing. Cancer Res., 47: 936-942, 1987.
15. Harmon, J. M. and Thompson, E. B. Isolation and characterization of
dexamethasone-resistant mutants from human lymphoid cell line CEM-CT. Mol. Cell Biol., 1: 512-521, 1981.16
16 Scheidereit, C., Geisse, S., Westphal, H. M., and Beato, M. The glucocorticoid receptor binds to defined nucleotide sequences near the promoter of mouse mammary tumour virus. Nature 304: 749-752, 1983.
17. Staal, F. J., Roederer, M., Herzenberg, L. A., and Herzenberg, L. A. Intracellular thiols regulate activation of nuclear factor kappa B and transcription of human immunodeficiency virus. Proc. Natl. Acad. Sci. USA, 87: 9943-9947, 1990.
18. Bradford, M. M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem., 72: 248-254, 1976. 19. Lippman, M. E., Yarbro, G. K., and Leventhal, B. G. Clinical implications of glucocorticoid
receptors in human leukemia. Cancer Res., 38: 4251-4256, 1978.
20. Vanderbilt, J. N., Miesfeld, R., Maler, B. A., and Yamamoto, K. R. Intracellular receptor concentration limits glucocorticoid-dependent enhancer activity. Mol. Endocrinol., 1: 68-74, 1987.
21. Gehring, U., Mugele, K., and Ulrich, J. Cellular receptor levels and glucocorticoid responsiveness of lymphoma cells. Mol. Cell Endocrinol., 36: 107-113, 1984.
22. Bourgeois, S. and Newby, R. F. Diploid and haploid states of the glucocorticoid receptor gene of mouse lymphoid cell lines. Cell, 11: 423-430, 1977.
23. Chapman, M. S., Askew, D. J., Kuscuoglu, U., and Miesfelt, R. L. Transcritional control of steroid-regulated apoptosis in murine thymoma cells. Mol. Endocrinol., 10: 967-978, 1996. 24. Bloomfield, C. D., Smith, K. A., Peterson, B. A., and Munck, A. Glucocorticoid receptors in
adult acute lymphoblastic leukemia. Cancer res., 41: 4857-4860, 1981.
25. Pui, C. H., Dahl, G. V., Rivera, G., Murphy, S. B., and Costlow, M. E. The relationship of blast cell glucocorticoid receptor levels to response to single-agent steroid trial and remission response in children with acute lymphoblastic leukemia. Leuk. Res., 8: 579-585, 1984. 26. Pui, C. H., and Costlow, M. E. Sequential studies of lymphoblast glucocorticoid receptor
levels at diagnosis and relapse in childhood leukemia: an update. Leuk. Res. 10: 227-229, 1986.
27. Wells, R.J., Mascaro, K., Young, P. C., and Cleary, R. E. Glucocorticoid receptors in the lymphoblasts of patients with glucocorticoid-resistant childhood acute lymphoblastic leukemia. Am. J. Pediatr. Hematol. Oncol., 3: 259-264, 1981.
28. Powers, J. H., Hillmann, A. G., Tang, D. C., and Harmon, J. M. Cloning and expression of mutant glucocorticoid receptors from glucocorticoid-sensitive and glucocorticoid-resistant human leukemic cells. Cancer Res., 53: 4059–4065, 1993.
29. Reichardt, H. M., and Schutz, G. Glucocorticoid signalling–multiple variations of a common theme. Mol. Cell. Endocrinol., 146: 1–6, 1998.
30. McEwan, I. J., Wright, A. P. H., and Gustafsson, J-Å. Mechanism of gene expression by the glucocorticoid receptor: role of protein-protein interactions. Bioessays, 19: 153–160, 1997. 31. Dumont, A., Hehner, S. P., Schmitz, M. L., Gustafsson, J-Å., Liden, J., Okret, S., van der
Saag, P. T., Wissink, S., van der Burg, B., Herrlich, P., Haegeman, G., De Bosscher, K., and Fiers, W. Cross-talk between steroids and NF-k: what language? Trends Biochem. Sci., 23: 233–235, 1998.
32. Gottlicher, M., Heck, S., and Herrlich, P. Transcriptional cross-talk, the second mode of steroid hormone receptor action. J. Mol. Med., 76: 480–489, 1998.
33. Van Antwerp, D. J., Martin, S. J., Kafri, T., Green, D. R., and Verma, I. M. Suppression of TNF-alpha-induced apoptosis by NF-kappa B. Science, 274: 787-789, 1996.
34. Sen, C. K. and Packer, L. (1996) Antioxidant and redox regulation of gene transcription. FASEB J. 10, 709-720.
35. Friedberg, E. C., Walker, G. C., and Siede, W. (1995) DNA repair and mutagenesis. pp. 14-19. ASM Press: Washington D.C.
36. Bertoncini, C. R. and Meneghini, R. (1995) DNA strand breaks produced by oxidative stress in mammalian cells exhibit 3'-phosphoglycolate termini. Nucleic Acids Res. 23, 2995-3002. 37. Van Antwerp, D. J., Martin, S. J., Kafri, T., Green, D. R., and Verma, I. M. (1996)
Suppression of TNF-alpha-induced apoptosis by NF-kappa B. Science 274, 787-789. 38. Beg, A. A. and Baltimore, D. (1996) An essential role for NF-kappaB in preventing
TNF-alpha-induced cell death. Science 274, 782-784.
39. Baringo M. (1996) A life-death balance within the cell. Science 274, 724.
40. Wang, C. Y., Mayo, M. W., and Baldwin, A. S. (1996) TNF-alpha and cancer therapy-induced apoptosis: potentiation by inhibition of NF-κB. Science 274, 784-787.
41. Chu, Z. L., McKinsey, T. A., Liu, L., Gentry, J. J., Malim, M. H., and Ballard, D. W. (1997) Suppression of tumor necrosis factor-induced cell death by inhibitor of apoptosis c-IAP2 is under NF-kappaB control. Proc. Natl. Acad. Sci. USA 94, 10057-10062.
42. Lu, Y. S., Yeh, P. Y., Chuang, S. E., Yeh, K. H., Yang, C. H., Kuo, M. L., and Cheng, A. L. Glucocorticoids Affect Growth and Chemosensitivity of Carcinoma Cells via Diverse Glucocorticoid Receptor-related Pathways. Proc. American Association for Cancer Res. 42: 2951, 2001.
43. Wang, C. Y., Mayo, M. W., and Baldwin, A. S. TNF-alpha and cancer therapy-induced apoptosis: potentiation by inhibition of NF-κB. Science, 274: 784-787, 1996.
44. Kang, H. Y., Yeh, S., Fujimoto, N., and Chang, C. " Cloning and characterization of human prostate coactivator ARA54, a novel protein that associates with the androgen receptor". J. Biol. Chem., 274: 8570-8576, 1999.
45. Kino, T., Gragerov, A., Kopp, J. B., Stauber, R. H., Pavlakis, G. N., and Chrousos, G. P. The HIV-1 virion-associated protein vpr is a coactivator of the human glucocorticoid receptor. J. Exp. Med., 189: 51-62, 1999.
46. McKenna, N. J., Lanz, R. B., and O'malley, B. W. Nuclear receptor coregulators: cellular and molecular biology. Endocr. Reviews, 20: 321-344, 1999.
47. Weijtens, O., Schoemaker, R. C., Cohen, A. F., Romijn, F. P., Lentjes, E. G., and Van Rooij, J. Dexamethasone concentration in vitreous and serum after oral administration. Am. J.
Ophthalmol., 125: 673-679, 1998.
48. Brady, M. E., Sartiano, G. P., Rosenblum, S. L., Zaglama, N. E., and Bauguess, C. T. The pharmacokinetics of single high doses of dexamethasone. Eur. J. Clin. Pharmacol., 32: 593-596, 1987.