270
Unplanned Extubation in Surgical Patients:
Clinical Outcomes and Risk Factors for Reintubation
Ming-Shian Lu*, Yu-Kai Cheng**, Ting-Chung Wang**, Wen-Shih Huang***, Li-Ying Chiu****, Yao-Kuang Huang*, Li-Ying-Huang Tsai*****
Objectives: To determine the clinical outcomes of unplanned extubation (UE), and the incidence and risk factors of reintubation in surgical patients.
Design: Retrospective medical chart and electronic database review.
Materials and Methods: All adult patients admitted to the Surgical and Neurosurgical Intensive Care Unit of Chang Gung Memorial Hospital, Chiayi, from January 2007 to December 2009 were included. The medical charts and electronic records, cross-matched with the quality practice database of the Critical Care Audit Committee, were reviewed.
Results: There were 50 episodes of UE involving 42 patients (29 males) from among 2,165 intubated patients during this period. The median age was 61.4 years. UE was categorized as intentional in 42 episodes (84%). The following factors were associated with reintubation in univariate analysis: accidental UE (p=0.03), time on mechanical ventilation (p=0.021), and PaO2/FIO2 (p=0.002). In multivariate analysis, accidental UE (p=0.004) and PaO2/FIO2 (p≤0.001) remained as significant risk factors for reintubation. Reintubation was mandatory in 71.4% of patients within 1 hour of UE. Reintubated patients spent an average of 11.7 more days in the intensive care unit (ICU) and had 31.0 more days of hospital stay. Reintubation correlated strongly with ICU stay (p<0.001), hospital stay (p<0.001) and mortality (p<0.001).
Conclusion: The incidence of UE in surgical patients is low. Reintubations occur more frequently within one hour of UE. Accidental extubations are more likely to require reintubation. (Thorac Med 2012; 27: 270-275)
Introduction
Weaning from mechanical ventilator sup-port always starts after stabilization of acute
respiratory failure due to either surgical or medical causes. Although the average stay in surgical intensive care units (ICUs) tends to be short because acute respiratory failure is not *Division of Thoracic and Cardiovascular Surgery, Chang Gung Memorial Hospital, Chiayi, Chang Gung University, Taiwan; **Division of Neurosurgery, Chang Gung Memorial Hospital, Chiayi; ***Division of Colon and Rectal Surgery, Chang Gung Memorial Hospital, Chiayi; ****Department of Nursing, Chang Gung Memorial Hospital, Chiayi; *****Division of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Chiayi Address reprint requests to: Dr. Ying-Huang Tsai, Division of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Chiayi, 6, West Sec., Chiapu Road, Pu-tze City, Chiayi County, Taiwan
the most common reason for admission to these units, the occasional occurrence of unplanned extubation (UE) complicates the clinical course of these patients. Since the effects of UE in sur-gical patients have not been explored in detail, we wanted to determine which risk factors are associated with reintubation, as well as the out-come of UE in a cohort of surgical patients.
Materials and Methods
The investigation and research board of
Chang-Gung Memorial Hospital approved
this clinical investigation. Informed consent
from individual patients was waived in the
absence of any intervention for the
purpose of this re-view.
The clinical record of all patients (>18 years) admitted to the surgical and neurosurgical ICUs at Chang-Gung Memorial Hospital, Chiayi Cen-ter, from January 2007 to December 2009, were reviewed retrospectively. The monthly quality practice data submitted by each ICU to the Crit-ical Care Audit Committee were cross-matched for accuracy. Patients ventilated through trache-ostomies were excluded.
UE was defined as the premature removal of an artificial airway. UE was considered “intentional” when the endotracheal tube was removed by the patient and “accidental” when it occurred during the routine care process or transportation of the patient. Reintubation was defined as any intubation within 48 hours of UE (≤30 minutes was considered immediate). Restraints were used when deemed necessary by the nursing staff and surgical resident under the strict nursing restraint protocol. The use of intravenous sedation was not mandatory, and was at the discretion of the attending surgeon or critical care specialist. O2
supplementa-tion by mask with an FIO2 of 50% was given immediately post-UE, and arterial blood gas analysis was assessed 30 minutes thereafter. The decision to reintubate was at the discre-tion of the senior duty resident and attending
physician. The following clinical and labora-tory parameters were collected: age, gender, ICU allocation, admission APACHE II score, admission SAPS II score, time under mechani-cal ventilation support, Glasgow Coma Smechani-cale post-extubation, event nature of UE (intentional or accidental), work shift (morning: 8am-4pm, evening: 4pm-12pm or night: 12pm-8am) and day of the week UE occurred (weekend: Satur-day 12pm- MonSatur-day 8am vs. weekSatur-day), weaning condition, rapid shallow breathing index (RSBI) before UE, partial pressure of arterial oxygen (PaO2) and carbon dioxide (PCO2), PaO2/FIO2 ratio, fluid balance 48 hours before UE, time to reintubation, ICU and hospital stay, and clinical outcome. Respiratory parameters and ventila-tor settings were extracted from the respiratory therapist record sheet. The PaO2, PaCO2, PaO2/ FIO2 and respiratory rate to tidal volume ratios were calculated based on the last entry by the respiratory therapist. PaCO2 was grouped as normocapnea (35-44.9 mmHg) and hypo/hyper-capnea (≤34.9 / ≥44.9 mmHg).
The incidence rate of UE was calculated as follows: [(number of patients with UE) / (num-ber of intubated patients)] × 100.
Statistics
Continuous variables were expressed as mean ± standard deviation, and non-parametric variables as percentages. Student’s t test was used to compare continuous variables. Differ-ences in proportions were compared using the chi-square or Fisher’s exact test, depending on cell size. Multinominal logistic regression
analysis was used for risk factor stratification of significant factors in univariate analysis. Data were analyzed using SPSS software (12.0, SPSS Inc, Chicago, Illinois).
Results
There were 50 episodes of UE involving 42 patients from among 2,165 intubated patients during this period (29 males, 34 episodes). The incidence of UE was 1.9%. The mean age of the cohort was 61.4 years (range 23-95 years). The mean APACHE II score and SAPS II score on admission were 14.5 (range 6-30) and 32.5 (range 13-52), respectively (Table 1). The mean mechanical ventilation time before the UE epi-sode was 76.9 hours. Forty-two episodes (84%) were classified as intentional, and 27 (54%) occurred during the night shift. Forty-three episodes occurred while the patient was being restrained, and 33 episodes during the weaning process (66%).
The incidence of reintubation was 33% (14/42 patients). Reintubation was mandatory in 10 patients within 1 hour, and 3 cases were con-sidered immediate; 85.7% (12/14 patients) were reintubated within 24 hours of UE. The reasons for reintubation were hypoxemia (n=9, 64.2%), tachypnea (n=4, 28.5%) and the general anes-thesia effect (n=1). Five of 8 episodes (62.5%) of accidental extubation required reintubation, and only 9 of 42 episodes (21.4%) of intentional self-extubation required reintubation (p=0.03). Reintubated patients had an average ICU stay of 18.7 ± 12.4 days and hospital stay of 55.8
± 36.4 days, and patients who did not require reintubation had an ICU stay of 6.9 ± 10.1 days and hospital stay of 24.8 ± 19.4 days, respec-tively. Seven patients died during hospitaliza-tion, and 6 of them had been reintubated within
48 hours. Reintubation correlated strongly with ICU stay (p<0.001), hospital stay (p<0.001) and mortality (p<0.001). No death was directly related to UE or reintubation events.
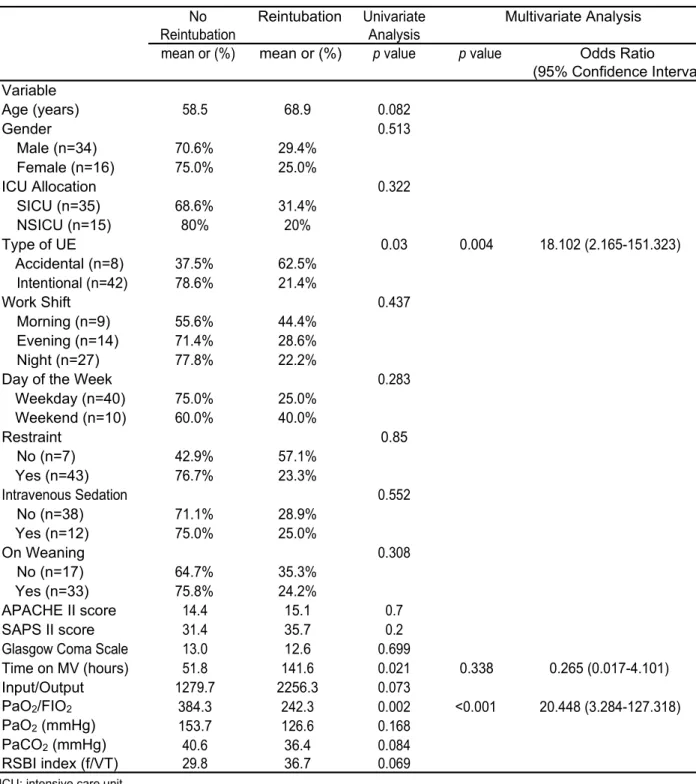
In univariate analysis, the following factors were correlated with the need for reintubation: accidental UE (p=0.03), time on mechanical ventilation (p=0.021), and PaO2/FIO2 (p=0.002). Multivariate analysis revealed that acciden-tal UE (p=0.004, OR 18.102, 95% CI 2.165-151.323) and PaO2/FIO2 (p≤0.001, OR 20.448, 95% CI 3.284-127.318) were factors that were strongly correlated to reintubation, but time on mechanical ventilation did not reach statistical significance p(=0.338).
Discussion
In this report, the incidence of unplanned extubation was only 1.9%. An appropriate explanation for this is the fast track for extu-bation adopted for our patients in the surgical ICU. The weaning process in our institution is guided by a supervised non-mandatory respira-tory therapist-driven protocol, yet the decision to extubate is at the discretion of the primary care physician. In this study, a weaning trial per se was not a significant risk factor for reintuba-tion, in contrast to a previous study by Betbese et al. [1]. A possible reason for this is that there were twice as many cases under a weaning trial as those under controlled ventilation; therefore, more cases were needed to reach a statistically significant level. A higher proportion of UE cases occurred during the night shift and week-days, but without statistical significance. Pub-lished studies have discordant results regarding the effects of work shifts or workdays on UE [2-4]. Other insignificant risk factors in our study included the Glasgow Coma Scale (GCS)
Risk Factors and Clinical Outcomes of Reintubation in Unplanned Extubation 273
Table 1. Demographic characteristics and statistical analysis
No Reintubation Univariate Multivariate Analysis
Reintubation Analysis
mean or (%) mean or (%) p value p value Odds Ratio
(95% Confidence Interval) Variable Age (years) 58.5 68.9 0.082 Gender 0.513 Male (n=34) 70.6% 29.4% Female (n=16) 75.0% 25.0% ICU Allocation 0.322 SICU (n=35) 68.6% 31.4% NSICU (n=15) 80% 20% Type of UE 0.03 0.004 18.102 (2.165-151.323) Accidental (n=8) 37.5% 62.5% Intentional (n=42) 78.6% 21.4% Work Shift 0.437 Morning (n=9) 55.6% 44.4% Evening (n=14) 71.4% 28.6% Night (n=27) 77.8% 22.2%
Day of the Week 0.283
Weekday (n=40) 75.0% 25.0% Weekend (n=10) 60.0% 40.0% Restraint 0.85 No (n=7) 42.9% 57.1% Yes (n=43) 76.7% 23.3% Intravenous Sedation 0.552 No (n=38) 71.1% 28.9% Yes (n=12) 75.0% 25.0% On Weaning 0.308 No (n=17) 64.7% 35.3% Yes (n=33) 75.8% 24.2% APACHE II score 14.4 15.1 0.7 SAPS II score 31.4 35.7 0.2
Glasgow Coma Scale 13.0 12.6 0.699
Time on MV (hours) 51.8 141.6 0.021 0.338 0.265 (0.017-4.101) Input/Output 1279.7 2256.3 0.073 PaO2/FIO2 384.3 242.3 0.002 <0.001 20.448 (3.284-127.318) PaO2 (mmHg) 153.7 126.6 0.168 PaCO2 (mmHg) 40.6 36.4 0.084 RSBI index (f/VT) 29.8 36.7 0.069
ICU: intensive care unit
SICU: surgical intensive care unit NSICU: neurosurgical intensive care unit UE: unplanned extubation
MV: mechanical ventilation
RSBI index: rapid shallow breathing index
APACHE II: acute physiology and chronic health evaluation II score SAPS II: simplified acute physiology score II
and restraint. The explanation for the lack of association of the GCS is that all our patients had a high GCS, which differs completely from earlier studies [5-6]. The effect of physical re-straint on UE remains controversial [5,7].
Three risk factors were associated with reintubation in univariate analysis (Table 1). Only lower PaO2/FIO2 ratios and accidental UE
were found to be significant in multivariate analysis. The reason for reintubation following lower PaO2/FIO2 ratios is self-explanatory, as
hypoxemia per se is an indication for reintuba-tion [4,8-9]. Accidental UE as an independent risk factor for reintubation is a finding compat-ible with published articles [9-11], and is un-derstandable because the underlying causes of acute respiratory failure are usually not under control. Re-intubated cases are associated with increased length of ICU and hospital stay, and hospital mortality.
Conclusion
The incidence of UE in surgical patients
is low. Reintubations occur more frequently
within 1 hour of UE. Accidental extubations
are more likely to require reintubation.
References
1. Betbese AJ, Perez M, Bak E, et al. A prospective study of unplanned endotracheal extubation in intensive care unit
patients. Crit Care Med 1998; 26: 1180-6.
2.Boulain T. Unplanned extubations in the adult intensive care unit. A prospective multicenter study. Am J Respir Crit Care Med 1998; 157: 1131-7. 3.Chevron V, Menard JF, Richard JC, et al.
Unplanned extubation: risk factors of development and predictive criteria for reintubation. Crit Care Med 1998; 26: 1049-53.
4.Listello D, Sessler CN. Unplanned extubation clinical predictors for reintubation. Chest 1994; 105: 1496-503.
5. Chang LY, Wang KWK, Chao YF. Influence of physical restrain on unplanned extubation of adult intensive care patients: a case-control study. Am J Crit Care 2008; 17: 408-15.
6.Namen AM, Ely EW, Tatter SB, et al. Predictors of succ-essful extubation in neurosurgical patients. Am J Respir Crit Care Med 2001; 163: 658-64.
7.Tanios MA, Epstein SK, Livelo J, et al. Can we identify patients at high risk for unplanned extubation? A large-scale multidisciplinary survey. Respiratory Care 2010; 55: 561-8.
8.Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS: Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149: 818-24.
9.Razek T, Gracias V, Sullivan D, et al. Assessing the need for reintubation: a prospective evaluation of unplanned endotracheal extubation. J Trauma 2000; 48: 466-9.
10. de Groot RI, Dekkers OM, Herold IH, et al. Risk factors and outcome after unplanned extubations in the ICU: a case-control study. Crit Care 2011; 15: R19.
11. Curry K, Cobb S, Kutash M, et al. Characteristics associa-ted with unplanned extubations in a surgical intensive care unit. Am J Crit Care 2008; 17: 45-51.
Risk Factors and Clinical Outcomes of Reintubation in Unplanned Extubation 275