Impact of body-mass factors on setup displacement in
patients with head and neck cancer treated with
radiotherapy using daily on-line image guidance
Yo-Liang Lai1 Shih-Neng Yang1,4 Ji-An Liang1,2 Yao-Ching Wang1 Chun-Yen Yu1* Ching-Hsiung Su1 Shang-Wen Chen1,2,3
1 Department of Radiation Oncology, China Medical University Hospital,Taichung, Taiwan
2 School of Medicine, China Medical University, Taichung, Taiwan 3 School of Medicine, Taipei Medical University, Taipei, Taiwan
4Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung, Taiwan
*Contributed equally with the first author
Corresponding author
Dr. Shang-Wen Chen
2nd Yuh-Der Rd, North District, Taichung City, Taiwan Tel: 886-4-22052121-7450
Abstract
Background: To determine the impact of body-mass factors (BMF) before
radiotherapy and changes during radiotherapy on the magnitude of setup displacement in patients with head and neck cancer (HNC).
Methods: The clinical data of 30 patients with HNC was analyzed using the
alignment data from daily on-line on-board imaging from image-guided radiotherapy. BMFs included body weight, body height, and the circumference and bilateral thickness of the neck. Changes in the BMFs during treatment were retrieved from cone beam computed tomography at the 10th and 20th fractions. Setup errors for each patient were assessed by systematic error (SE) and random error (RE) through the superior-inferior (SI), anterior-posterior (AP), and medial-lateral (ML) directions, and couch rotation (CR). Using the median values of the BMFs as a cutoff, the impact of
the factors on the magnitude of displacement was assessed by the Mann-Whitney U
test.
Results: A higher body weight before radiotherapy correlated with a greater AP-SE
(p = 0.045), SI-RE (p = 0.023), and CR-SE (p = 0.033). A longer body height was associated with a greater SI-RE (p = 0.002). A performance status score of 1 or 2 was related to a greater AP-SE (p = 0.043), AP-RE (p = 0.015), and SI-RE (p = 0.043). Among the ratios of the BMFs during radiotherapy, the values at the level of mastoid
tip at the 20th fraction were associated with greater setup errors.
Conclusions: To reduce setup errors in patients with HNC receiving RT, the use of
on-line image-guided radiotherapy is recommended for patients with a large body weight or height, and a performance status score of 1-2. In addition, adaptive planning should be considered for those who have a large reduction ratio in the circumference (<1) and thickness (<0.94) over the level of the mastoid tip during the 20th fraction of treatment.
Keywords: Adaptive radiotherapy, body-related factors, head and neck cancer,
image-guided radiotherapy, setup error, image-guided radiotherapy,
Radiation therapy (RT) is commonly used as part of multiple modality treatment for hand and neck cancer (HNC). Intensity-modulated radiation therapy (IMRT) has become increasingly popular because dose escalation to the target can be done while sparing adjacent normal tissues . However, precise patient setup is essential for safe and accurate delivery because IMRT results in steep dose gradients. In HNCs, several factors such as the accuracy of the immobilization device, change in body contours, and tumor regression could lead to setup uncertainties during RT. Causes might be independent or related to the others. Nonetheless, all of these factors need to be minimized with the use of special approaches. Image-guided radiation therapy (IGRT) can be used to correct and quantify geometrical uncertainties for daily setup . Although setup variations can be reduced when using on-line IGRT daily [3, 4], the widespread use of daily IGRT is not always feasible in all clinical settings. Adaptive radiotherapy (ART) is an approach used to correct for anatomic changes caused by tumor shrinkage or body weight loss during RT . However, increased medical costs, higher staff workload, and higher radiation doses to the patients are inevitable. As a result, there is a need to investigate suitable indications for ART for patients with HNCs.
There are few studies reporting on setup displacement due to patient-related factors before and during RT for HNC. The main patient-related factors are
body-mass factors (BMF) because these affect the stability of immobilization. In addition, correlation between these BMFs and quantification of setup errors remain to be clarified. This study was done to determine the impact of BMFs before and during RT on positioning displacement for patients treated for HNCs. We tried to find correlations between BMFs and the magnitude of daily setup errors. The results can help physicians determine who should be considered for on-line IGRT before starting RT, and select those who need ART to reduce setup displacement.
Methods
Patients
With the approval of the local institutional review board, clinical and image data from a cohort of 30 patients treated for HNCs between June 2008 and January 2013 at China Medical University Hospital were reviewed. Twenty-one patients were treated for nasopharyngeal carcinoma, 8 for oropharyngeal cancer, and 1 for hypopharyngeal cancer. Their median age was 53 years (range: 33-77). All patients received IGRT with daily on-line kilovoltage imaging with weekly cone beam computed tomography (CBCT) to correct the treatment position. No patients had ART planning before a prescribed dose of 50 Gy. The characteristics of these patients are listed in Table 1.
Treatment planning
immobilized by a thermoplastic mask (U-shaped Head and Neck Mask, Renfu Medical Equipment, Guangzhou, China) from the bottom of the orbit to the shoulder. Following fabrication of the immobilization device, simulation using a computed tomographic (CT) scan simulator (HiSpeed NX/i, GE Healthcare, Milwaukee, Wisconsin, USA) was made. The scans consisted of a protocol with a 3-mm-slice thickness, and were obtained from the upper orbit to 2 cm below the sternum. Marks on the patients’ skin were drawn using setup lasers to facilitate an accurate daily position.
For patients receiving definitive RT, the clinical target volume (CTV) was defined as the gross tumor volume plus a margin of 1.0 to 1.5 cm. We followed the guidelines for the delineation of an elective nodal CTV . The planning target volume (PTV) was extended 3 mm from the CTV to account for treatment uncertainty. All patients underwent IMRT plans consisting of 7 coplanar fields using 6-MV photons. The prescription dose to the CTV was 50 Gy in 25 fractions followed by a boost to 70-72 Gy to high-risk regions (tumor and involved lymph nodes). All plans were carried out using a commercial radiation treatment planning system (Eclipse version 8.6, Varian Medical Systems Inc, Palo Alto, California, USA).
Treatment verification
(Varian Medical Systems, Palo Alto, California, USA) equipped with an on-line On-Board Imaging (OBI) function including two-dimensional (2D) kilovoltage (kV) images and three-dimensional (3D) CBCT. The technicians set up the patients on a couch in the simulation room according to the marks drawn on their bodies. On-line OBI images (2D kV images daily and 3D CBCT weekly) were taken and sent to the station where they could be registered to digitally reconstructed radiographs from the treatment planning images. Two technicians compared these paired images by correlating the bony anatomy and corrected the difference by shifting the couch translationally before treatment. Then, an attending physician confirmed the corrected on-line images. Anatomic reference landmarks included at least three visible bony structures, the vertebra of the C-spine, nasal septum, and mandible profile.
Anthropometric measures of body-related factors
Patient-related factors consisted of performance status (PS), age, and BMFs. PS was scored according to the Eastern Cooperative Oncology Group. The BMFs included body weight, body height, body mass index (BMI), and circumference and thickness across three specified sections of the head and neck (Figure 1). Level A was labeled on the mastoid tip, the same section as the junction between the skull base and the 1st cervical vertebra. Level B was based on the mandible angle, the same height as the junction between the 2nd to the 3rd cervical vertebrae. Level C was drawn from the
thyroid notch, the same as the 5th cervical vertebra.
BMFs were recorded before RT and at the 10th and 20th fractions during the RT course. Because the circumferences and thicknesses at the three specified levels could not be measured prospectively, the values were retrieved retrospectively according to the CT simulation images and CBCT images during treatment. For circumferences, we first brushed the body contour at a specified section with a fixed thickness to generate a volume. Then, the calculated volumes were divided by the contouring thickness to obtain get the values of the circumferences. The thickness was measured as the maximal transverse distance at the same section as the circumferences. The BMI was calculated as weight in kilograms divided by the square of height in m according to the definition of the World Health Organization.
Patients were monitored weekly and toxicities were recorded according to the Common Terminology Criteria for Adverse Events version 3.0. Ratios of the BMFs during RT were calculated on the three levels. For example, the ratio of the circumference on section A at the 10th treatment was the circumference at level A at the 10th fraction divided by the pretreatment circumference.
Setup displacement
After image registration, quantification of alignment data for daily OBI in the superior-inferior (SI), anterior-posterior (AP), and medial-lateral (ML) directions, and couch rotation (CR) for all patients were collected. For each direction, the
recorded setup displacements were composed of two components, systematic errors (SE) and random errors (RE). The SE was the deviation between the simulated patient position and the average patient position, while the RE was that which occurred between different fractions. The detailed calculation for SE and RE was similar to that used by Remeijer et al .
By analyzing all the alignment data before the 25 fraction s of treatment for each patient, the values of SE and RE for all directions in each patient could be calculated.
Statistical analysis
We used the Mann-Whitney U test to determine the correlation between the
magnitude of errors and patient-related factors. The median values of the BMFs were used as a cut-off to divide lower and higher groups. We also used the Pearson
correlation coefficient to examine the association between the reduction ratio of body
weight and circumferences or thicknesses. In addition, the same test was used to
examine the relation across the displacement in different directions. A two-sided p
value of < 0.05 was considered statistically significant. All statistical analyses were performed using a commercial software package (SPSS 13.0 for Windows, Chicago, IL, USA).
Results
The median values for various BMFs are listed in Table 1. The mean displacements in the SI, AP, and ML directions for all patients were 1.3 mm, 1.6 mm, and 2.2 mm, respectively. The population SE was, 2.2 mm, 1.1 mm, and 1.6 mm and the RE, 1.5 mm, 0.9 mm and 1.1 mm for the SI, AP and ML directions, respectively. Van Herk et al suggested a CTV- PTV margin of 2.5 SE + 0.7 RE to ensure that 90% of patients in a population receive a minimum cumulative CTV dose of at least 95% of the prescribed dose. Under this definition, the suggested CTV-PTV margins for setup uncertainties in our patients were 3.4, 4.8 and 6.5 mm in the AP, ML and SI directions, respectively. The population SE and RE for CR were 0.31 and 0.36 degrees, respectively.
There was no correlation across the displacement among the three translation directions. However, the SE and RE for the CR showed an association with the ML-SE (r = 0.49, p = 0.007 and r =0.44, p = 0.016).
In addition, we found the correlation was not significant between the ratio of body weight and thickness at level A on the CBCT at the 20th fraction (r = 0.32, p = 0.081), which is depicted in Figure 2. By contrast, there was no correlation between the ratio of body weight and circumference at any level either at the 10th or 20th fraction.
Correlation between pretreatment body-mass factors and setup displacement
displacements in the three translational directions and the BMFs. Of the pretreatment factors, a larger body weight was significantly correlated with a greater AP-SE (p = 0.045) and SI-RE (p = 0.023), and a longer body height was associated with a greater SI-RE (p = 0.002). A PS score of 1 or 2 was associated with a greater AP-SE (p = 0.043), AP-RE (p = 0.015), and SI-RE (p = 0.043).
In addition, body height was associated with the CR-SE (p = 0.033) and marginally correlated with the CR-RE (p = 0.067). For patients with longer and shorter body heights, the mean CR-SE was 0.22 ± 0.21 and 0.40 ± 0.25 degrees, respectively. The other pretreatment factors such as age, and BMI, were not associated with the magnitude of setup errors.
Correlation between reduction ratio of body-mass factors during RT and setup displacement
The alignment data before the CBCT of the 20th fraction were included when investigating the correlation between the setup errors and the change of the BMFs . Among the ratios of the BMFs during RT, t he values at each level were divided into lower and higher 50%. Compared with the ratios of body weight, our result showed certain BMFs can be more useful for initiating ART. At the 10th fraction of CBCT, the ratio of the thickness at level A was correlated with a greater ML-RE (p = 0.043), whereas the ratio of the thickness at level B was associated with a greater ML-RE (p =
0.019) ( Table 3) . At the 20th fraction, the ratio of the circumference at level A had a significant correlation with a greater AP-SE (p = 0.019), AP-RE (p = 0.019), and SI-SE (p = 0.025). The ratio of the thickness at level A was significantly correlated with a greater ML-SE (p =0.013), whereas it showed a marginal impact with the SI-RE (p =0.05) (Table 4). The remaining ratio of the BMFs had no impact on setup errors (Supplemental table).
The ratio of the thickness at level A at the 20th fraction was associated with a greater CR-SE (p = 0.009) and CR-RE (p = 0.019).
Discussion
Several studies have investigated setup uncertainty in HNC patients , which could change the dose distribution to the target volume and organ s at risk . Certainly, IGRT and ART are two solutions for these limitations . Furthermore, according to the International Commission on Radiation Units and Measurements report 62 , an inappropriate definition of the CTV-PTV margin, accounting for organ motion and setup uncertainties, may yield an underdose to the CTV. In order to define this margin for HNC, organ motion could be neglected, while variability due to inadequate setup or deformity must be carefully considered . In clinical practice, extensive use of daily IGRT is not always possible because of limited facilities in some countries as well as
concerns about increased daily doses to patients . Because there is a lack of evidence regarding patients who are vulnerable to setup uncertainty, we first reported the impact of pretreatment patient-related factors on setup displacement. Based on our findings, physicians can select appropriate patients for IGRT, such as those with a large body weight or height, or a PS of 1 or above. For patients who are not able to have IGRT for certain reasons, a sufficient CTV-PTV margin in a specific direction would be required to minimize uncertainties. Currently in our department, PTVs are generated by adding a 3 mm margin to corresponding CTVs; this study disclosed the inadequacy of this approach in certain directions for those prone to setup uncertainty if withholding IGRT. Because there might be great variety in setup accuracy among institutions and some geographical or racial difference in BMFs , an in-house report is imperative to minimize uncertainties. The current study provided a simple approach for this.
For patients receiving RT for HNCs, anatomical modifications due to tumor regression and body weight loss are easily noted during the RT course. Most physicians plan ART according to body weight changes or an unfitted immobilization device. Meanwhile, the geometric change of tumor volume and organs at risk should also be assessed. Currently, guidelines based on scientific data for initiating ART are still lacking. Although it has been suggested that an ART plan not only improves
dosimetric benefits but also increases tumor control and quality of life , it may increase costs to patients and the workload of clinical staff. Our work is a pilot study correlating changes in BMFs and the magnitude of setup displacements in HNC. Accordingly, ART planning can be initiated to minimize uncertainties for patients with a great reduction of the circumference or thickness at the level of mastoid tip at the 20th fraction of RT. Otherwise, widening of the CTV-PTV margin in the three translation directions should be done. For example, the margin in the SI direction could be expanded up to 7.4 mm for those with large changes in BMFs, according to the formula of Van Herk et al .
Among studies of setup analyses according to time trend, Mo ngioj et al. investigated alignment data from a cohort of 20 patients with nasopharyngeal cancer. They found setup displacements showed no significant changes as therapy progressed, but greater errors were observed when the patient had severe weight loss or tumor node shrinkage. In addition, grade 2 toxicities were associated with great displacement along the AP and SI directions. However, the change of BMFs was not correlated with the setup data. In the future, more studies are essential before these parameters during RT become a reference for initiating ART. In addition, investigations should be done to find the more significant anatomical level when assessing changes in BMFs.
Generally, our study disclosed most patients had a reduction in BMFs with time. However, we found some patients had a ratio of BMFs ≧ 1 during the RT course (shown in Tables 3, 4, and supplemental table), particularly at the 10th fraction of RT. One plausible reason is that shrinkage of soft tissue after RT might lead to an insufficient immobilization effect from the thermoplastic mask. As a result, the credibility of the calculated values across the three levels of the BMFs might be challenged because of displacement of the patient’s neck. In addition, the effect of intravenous fluid overload on neck swelling during concurrent administration of chemotherapy should be investigated further. To circumvent the limitations of the study, daily CBCT should be implemented to verify the reproducibility of the BMFs. Our study should be interpreted with several concerns. First, circumferences and thicknesses were not obtained prospectively by measuring the body with a ruler, but were measured retrospectively from CT images. The absolute values and the ratio of the BMFs might be inconsistent with those acquired from direct measurement. According to previous comparison tests in some patients, the maximal deviation between the two methods was less than 5%. Thus, this approach can be applied in those institutions ready to initiate the analysis. Second, errors due to anatomical changes should be distinguished from those caused by inadequate setup. The problem could be circumvented by the approach reported by Mc Dermott et al. . They
suggested using differences in images created by subtracting the first localization image from that of subsequent fractions was an efficient way to qualitatively detect anatomical changes during RT. Third, t he median value was taken as a cut-off for each measure to create two groups for comparison. As a result, a lot of different groups were created. To achieve more detailed stratification of the BMFs, there is a need to conduct a study with large sample size . Finally, our study did not report the impact of daily CBCT on setup displacement, as well as the weekly dosimetric changes. Although tumor and soft tissue targets could be assessed by CBCT, Li et al. suggested that there were no statistically significant differences in alignment between 2D kV and 3D CBCT images in HNCs. Thus, the consistency between setup errors for the bony structure and the target could be established. Future studies should enroll more patients prospectively, and evaluate subsequent dosimetric changes according to evolution of the BMFs.
Conclusions
This study recommends on-line IGRT for patients with HNC receiving RT who have a large body weight or height, or have a PS score of 1-2. In addition, to deliver more accurate dose to tumor and avoid extra dose to organs at risk due to anatomical change, an adaptive planning should be considered for those who have a large
reduction ratio in the circumference (< 1) and thickness (< 0.94) over the level of the mastoid tip at the 20th fraction of treatment
Competing interests
All authors declare that no actual or potential conflicts of interest were encountered during this study.
Authors’ contributions
YL Lai, CY Yu, and SW Chen were responsible for design of the study, acquisition of data, analysis and interpretation of data, and drafting the article. SN Yang, JA Liang, and CH SU provided some intellectual content. SW Chen approved the version to be submitted.
Acknowledgements
We thank for the study grants received for projects DMR-99-060 issued by China Medical University Hospital.
Figure Legends
Figure 1. Circumference and thickness measured across three specified sections. Level A is labeled on the mastoid tip, the same section as the junction between the skull base and 1st cervical vertebra. Level B is based on the mandible angle, the same height as the junction between the 2nd to the 3rd cervical vertabra. Level C is drawn from the thyroid notch, the same as the 5th cervical vertebra.
Figure 2. The association between the ratio of body weight and thickness at level A during the 20th fraction of cone beam computed tomography (r = 0.32, p = 0.081).
References
1. Eisbruch A, Foote RL, O'Sullivan B, Beitler JJ, Vikram B: Intensity-modulated radiation therapy for head and neck cancer: emphasis on the selection and delineation of the targets. Seminars in radiation oncology 2002, 12:238-249. 2. Li H, Zhu XR, Zhang L, Dong L, Tung S, Ahamad A, Chao KS, Morrison WH,
Rosenthal DI, Schwartz DL, et al: Comparison of 2D radiographic images and 3D cone beam computed tomography for positioning head-and-neck radiotherapy patients. International journal of radiation oncology, biology, physics 2008, 71:916-925.
3. Stock M, Palm A, Altendorfer A, Steiner E, Georg D: IGRT induced dose burden for a variety of imaging protocols at two different anatomical sites. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2012, 102:355-363.
4. Yu Y, Michaud AL, Sreeraman R, Liu T, Purdy JA, Chen AM: Comparison of daily versus nondaily image-guided radiotherapy protocols for patients treated with intensity-modulated radiotherapy for head and neck cancer. Head & neck 2013 [Epub ahead of print] doi: 10.1002/hed.23401.
5. Castadot P, Lee JA, Geets X, Gregoire V: Adaptive radiotherapy of head and neck cancer. Seminars in radiation oncology 2010, 20:84-93.
6. Gregoire V, Coche E, Cosnard G, Hamoir M, Reychler H: Selection and delineation of lymph node target volumes in head and neck conformal radiotherapy. Proposal for standardizing terminology and procedure based on the surgical experience. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2000, 56:135-150. 7. Remeijer P, Geerlof E, Ploeger L, Gilhuijs K, van Herk M, Lebesque JV: 3-D
portal image analysis in clinical practice: an evaluation of 2-D and 3-D analysis techniques as applied to 30 prostate cancer patients. International journal of radiation oncology, biology, physics 2000, 46:1281-1290.
8. De Neve W, Van den Heuvel F, De Beukeleer M, Coghe M, Thon L, De Roover P, Van Lancker M, Storme G: Routine clinical on-line portal imaging followed by immediate field adjustment using a tele-controlled patient couch. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 1992, 24:45-54.
9. Duma MN, Kampfer S, Schuster T, Aswathanarayana N, Fromm LS, Molls M, Andratschke N, Geinitz H: Do we need daily image-guided radiotherapy by megavoltage computed tomography in head and neck helical tomotherapy? The actual delivered dose to the spinal cord. International journal of
radiation oncology, biology, physics 2012, 84:283-288.
10. Mongioj V, Orlandi E, Palazzi M, Deponti E, Marzia F, Stucchi C, Sangalli C, Fallai C, Zonca G, Olmi P, Pignoli E: Set-up errors analyses in IMRT treatments for nasopharyngeal carcinoma to evaluate time trends, PTV and PRV
margins. Acta oncologica (Stockholm, Sweden) 2011, 50:61-71.
11. Pehlivan B, Pichenot C, Castaing M, Auperin A, Lefkopoulos D, Arriagada R, Bourhis J: Interfractional set-up errors evaluation by daily electronic portal imaging of IMRT in head and neck cancer patients. Acta oncologica
(Stockholm, Sweden) 2009, 48:440-445.
12. Samuelsson A, Mercke C, Johansson KA: Systematic set-up errors for IMRT in the head and neck region: effect on dose distribution. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2003, 66:303-311.
13. van Lin EN, van der Vight L, Huizenga H, Kaanders JH, Visser AG: Set-up improvement in head and neck radiotherapy using a 3D off-line EPID-based correction protocol and a customised head and neck support. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2003, 68:137-148.
14. Bujold A, Craig T, Jaffray D, Dawson LA: Image-guided radiotherapy: has it influenced patient outcomes? Seminars in radiation oncology 2012, 22:50-61.
15. Bethesda: ICRU report 62, Prescribing, recording and reporting photon beam therapy (supplement to ICRU report 50). 1999.
16. Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, Singh GM, Gutierrez HR, Lu Y, Bahalim AN, et al: National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 2011, 377:557-567.
17. Schwartz DL, Garden AS, Shah SJ, Chronowski G, Sejpal S, Rosenthal DI, Chen Y, Zhang Y, Zhang L, Wong PF, et al: Adaptive radiotherapy for head and neck cancer--dosimetric results from a prospective clinical trial. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2013, 106:80-84.
18. Yang H, Hu W, Wang W, Chen P, Ding W, Luo W: Replanning during intensity modulated radiation therapy improved quality of life in patients with nasopharyngeal carcinoma. International journal of radiation oncology, biology, physics 2013, 85:e47-54.
fractionated intensity modulated radiotherapy for nasopharyngeal
carcinoma. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2011, 98:23-27.
20. McDermott LN, Wendling M, Sonke JJ, van Herk M, Mijnheer BJ: Anatomy changes in radiotherapy detected using portal imaging. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2006, 79:211-217.
Tables
Table 1 Patient characteristics before radiotherapy Age (y)
median (range) 53 (30-77)
Body weight (kilogram) mean (range) median 66.9 (41-90.3) 65 Body height (cm) mean (range) 166.2 (153-177)
median 167.2 BMI mean (range) median 24.1 (17.5-29.1) 23.8 ECOG performance status
0 1-2 17 13 CCRT/RT alone (number) CCRT RT alone 28 2 Tumor origin (number)
Nasopharynx Oropharynx Hypopharynx 21 8 1 Circumference Al (cm) Mean ± SD (Range) 55.2 ± 3.7 (48.1-62.9) Thickness A (cm) Mean ± SD (Range) 16.3 ± 1.3 (14.2-17.9) Circumference B(cm) Mean ± SD (Range) 48.4 ± 3.8 (42.2-57.2) Thickness B(cm) Mean ± SD (Range) Circumference C (cm) Mean ± SD (Range) Thickness C (cm) Mean ± SD (Range) 14.5 ± 1.5 (11.8-18.4) 41.9 ± 4.5 (33.7-50.6) 13.6 ± 1.8 (11.0-17.6)
Abbreviation: BMI = body mass index; ECOG = Eastern Cooperation Oncology Group; CCRT = concurrent chemoradiotherapy; SD = standard deviation.
Note: Level A was labeled on the mastoid tip, the same section as the junction between the skull base
and the 1st cervical vertebra. Level B was based on the mandible angle, the same height as the junction
between the 2nd to the 3rd cervical vertebrae. Level C was drawn from the thyroid notch, the same as the
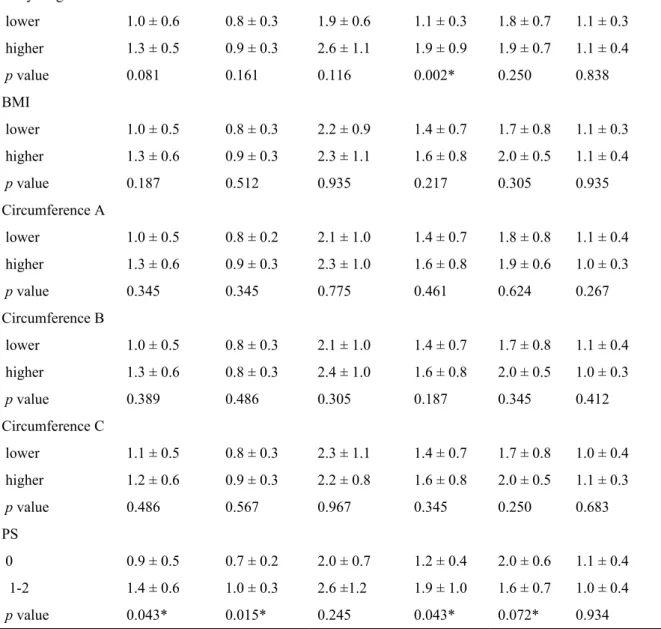
Table 2 Setup displacement (mean ± standard deviation in mm) in three translational directions according to lower and higher 50% percentile of body-related factors before RT
Variable AP-SE AP-RE SI-SE SI-RE ML-SE ML-RE
Body weight lower higher p value 0.9 ± 0.5 1.3 ± 0.6 0.045* 0.8 ± 0.3 0.9 ± 0.3 0.250 2.1 ± 0.9 2.4 ± 1.0 0.567 1.2 ± 0.4 1.8 ± 0.9 0.023* 1.8 ± 0.8 1.9 ± 0.6 0.436 1.1 ± 0.3 1.0 ± 0.4 0.461
Body height lower higher p value 1.0 ± 0.6 1.3 ± 0.5 0.081 0.8 ± 0.3 0.9 ± 0.3 0.161 1.9 ± 0.6 2.6 ± 1.1 0.116 1.1 ± 0.3 1.9 ± 0.9 0.002* 1.8 ± 0.7 1.9 ± 0.7 0.250 1.1 ± 0.3 1.1 ± 0.4 0.838 BMI lower higher p value 1.0 ± 0.5 1.3 ± 0.6 0.187 0.8 ± 0.3 0.9 ± 0.3 0.512 2.2 ± 0.9 2.3 ± 1.1 0.935 1.4 ± 0.7 1.6 ± 0.8 0.217 1.7 ± 0.8 2.0 ± 0.5 0.305 1.1 ± 0.3 1.1 ± 0.4 0.935 Circumference A lower higher p value 1.0 ± 0.5 1.3 ± 0.6 0.345 0.8 ± 0.2 0.9 ± 0.3 0.345 2.1 ± 1.0 2.3 ± 1.0 0.775 1.4 ± 0.7 1.6 ± 0.8 0.461 1.8 ± 0.8 1.9 ± 0.6 0.624 1.1 ± 0.4 1.0 ± 0.3 0.267 Circumference B lower higher p value 1.0 ± 0.5 1.3 ± 0.6 0.389 0.8 ± 0.3 0.8 ± 0.3 0.486 2.1 ± 1.0 2.4 ± 1.0 0.305 1.4 ± 0.7 1.6 ± 0.8 0.187 1.7 ± 0.8 2.0 ± 0.5 0.345 1.1 ± 0.4 1.0 ± 0.3 0.412 Circumference C lower higher p value 1.1 ± 0.5 1.2 ± 0.6 0.486 0.8 ± 0.3 0.9 ± 0.3 0.567 2.3 ± 1.1 2.2 ± 0.8 0.967 1.4 ± 0.7 1.6 ± 0.8 0.345 1.7 ± 0.8 2.0 ± 0.5 0.250 1.0 ± 0.4 1.1 ± 0.3 0.683 PS 0 1-2 p value 0.9 ± 0.5 1.4 ± 0.6 0.043* 0.7 ± 0.2 1.0 ± 0.3 0.015* 2.0 ± 0.7 2.6 ±1.2 0.245 1.2 ± 0.4 1.9 ± 1.0 0.043* 2.0 ± 0.6 1.6 ± 0.7 0.072* 1.1 ± 0.4 1.0 ± 0.4 0.934
Abbreviation: AP = anterior-posterior, SI = superior-inferior, ML = medial-lateral, SE = systemic error, RE = random error, BMI = body mass index, PS = performance status.
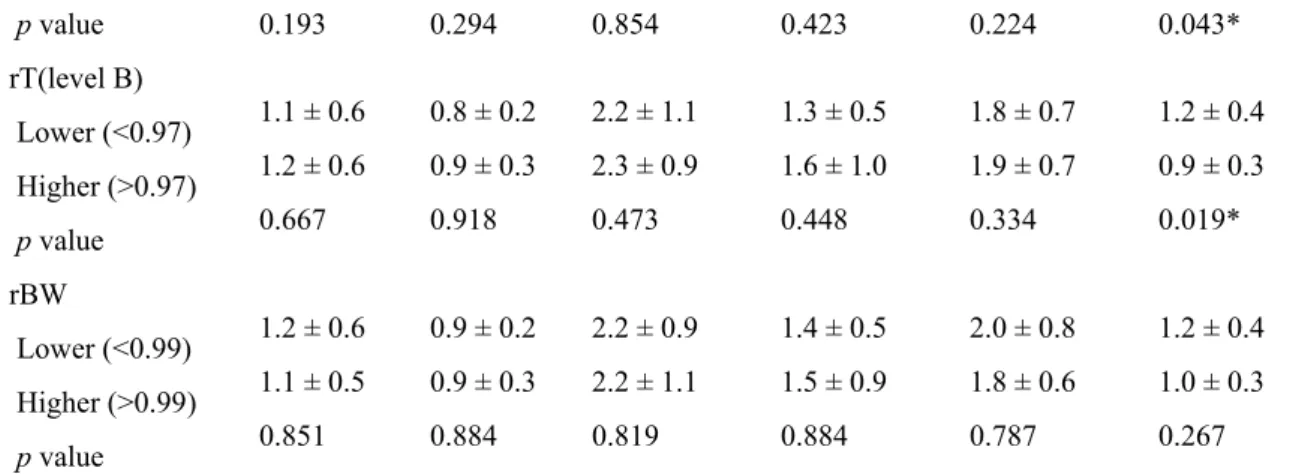
Table 3 Setup displacement (mean ± standard deviation in mm) in three translational directions according to lower and higher 50% percentile of body-related factors during RT (10th fraction)
Variable AP-SE AP-RE SI-SE SI-RE ML-SE ML-RE
rT(level A) Lower (<0.98) Higher (>0.98) 1.0 ± 0.6 1.2 ± 0.5 0.8 ± 0.3 0.9 ± 0.3 2.3 ± 1.2 2.1 ± 0.8 1.6 ± 0.8 1.4 ± 0.7 2.0 ± 0.6 1.7 ± 0.7 1.2 ± 0.4 1.0 ± 0.3
p value 0.193 0.294 0.854 0.423 0.224 0.043* rT(level B) Lower (<0.97) Higher (>0.97) p value 1.1 ± 0.6 1.2 ± 0.6 0.667 0.8 ± 0.2 0.9 ± 0.3 0.918 2.2 ± 1.1 2.3 ± 0.9 0.473 1.3 ± 0.5 1.6 ± 1.0 0.448 1.8 ± 0.7 1.9 ± 0.7 0.334 1.2 ± 0.4 0.9 ± 0.3 0.019* rBW Lower (<0.99) Higher (>0.99) p value 1.2 ± 0.6 1.1 ± 0.5 0.851 0.9 ± 0.2 0.9 ± 0.3 0.884 2.2 ± 0.9 2.2 ± 1.1 0.819 1.4 ± 0.5 1.5 ± 0.9 0.884 2.0 ± 0.8 1.8 ± 0.6 0.787 1.2 ± 0.4 1.0 ± 0.3 0.267
Abbreviation: rT = ratio of thickness, during-RT / pre-RT; rBW = ratio of body weight, during-RT / pre-RT; AP = anterior-posterior, SI = superior-inferior; ML = medial-lateral; SE = systematic error; RE = random error.
Note: asterisk respresents statistical significance.
Table 4 Setup displacement (mean ± standard deviation in mm) in three translational directions according to lower and higher 50% percentile of body-related factors during RT (20th fraction)
Variable AP-SE AP-RE SI-SE SI-RE ML-SE ML-RE
rC(level A)
Higher (>1) p value 0.9 ± 0.5 0.019* 0.7 ± 0.2 0.019* 2.0 ± 1.0 0.093 1.2 ± 0.5 0.025* 2.0 ± 0.6 0.101 1.1 ± 0.4 0.854 rT(level A) Lower (<0.94) Higher (>0.94) p value 1.3 ± 0.6 1.0 ± 0.5 0.325 0.9 ± 0.3 0.8 ± 0.2 0.325 2.5 ± 1.2 2.0 ± 0.6 0.461 1.7 ± 0.8 1.3 ± 0.7 0.050 2.2 ± 0.6 1.5 ± 0.6 0.013* 1.1 ± 0.3 1.0 ± 0.4 0.217 rBW Lower (<0.95) Higher (>0.95) p value 1.2 ± 0.5 1.1 ± 0.6 0.377 0.9 ± 0.2 0.9 ± 0.3 0.608 2.5 ± 1.0 2.0 ±1.0 0.193 1.5 ± 0.5 1.5 ± 1.0 0.334 1.8 ± 0.6 1.9 ± 0.7 0.790 1.1 ± 0.4 1.0 ± 0.3 0.608
Abbreviation: rC = ratio of circumference, during-RT / pre-RT; rT = ratio of
thickness, during-RT / pre-RT; rBW = ratio of body weight, during-RT / pre-RT; AP = anterior-posterior, SI = superior-inferior; ML = medial-lateral; SE = systematic error; RE = random error.