Received: 2010, 6, 24. Accepted: 2010, 8, 3.
Address reprint request to: Dr. Man-Gang Lee., Department of Urology, Zuoying Armed Forces General Hospital., No. 553 Junxiao Rd, Zuoying District, Kaohsiung City, Taiwan, R.O.C.
MAILGNANT LYMPHOMA INVOLVING THE PROSTATE: A CASE REPORT
Li-Min Sun1, Eng-Yen Huang2, Nai-Jen Chang3, Li-Min Chung4, Chiao-Yi Lu5,Ji-An Liang6,7 and Man-Gang Lee8
Departments of Radiation Oncology1, Pathology 3, Medical Oncology4, Radiology5, and Urology8, Zuoying Armed Forces General Hospital
2Department of Radiation Oncology, Kaohsiung Chang-Gung Memorial Hospital 6Department of Radiation Therapy and Oncology, China Medical University Hospital 7School of Medicine, China Medical University
Malignant lymphoma of the prostate gland, either primary or secondary, is rare. We report a 74-year-old male who was diagnosed with disseminated lymphoma including involvement of the prostate gland with the initial presentation of urinary retention. Digital rectal examination revealed mildly enlarged prostate gland with smooth and rubbery consistency. He received transurethral resection of the prostate under the impression of benign prostatic hyperplasia. The pathology found diffused infiltration of atypical lymphoid cells infiltration. The immunohistochemical staining revealed positive for CD20, and consistent with malignant B cell lymphoma. Systemic work-up found that his disease has disseminated many areas. Back mass biopsy showed small to medium atypical lymphoid cells diffused infiltration with immunohis-tochemical staining for CD3(-), CD5(-), CD10(+), CD20(+), CD23(-), and Cyclin D1(-). The diagnosis of follicular lymphoma was made. The patient received four cycles of chemotherapy with rituximab, cyclophosphamide, etoposide, vincristine and pred-nisone (R-CEOP). After temporarily partial response, tumor regrowing was noted. Salvage chemotherapy followed by the radiotherapy (RT) to the enlarged paraaortic lymph nodes was given. The patient did not finish the RT course because of exacer-bated condition. He died with the disease 9 months after diagnosis.
[Therapeut Radiol Oncol 2011; 18(1): 69-75]
Key words: Malignant lymphoma, Prostate gland, Immunohistochemistry
INTRODUCTION
Primary prostatic lymphoma is rare. It accounts for approximately 0.2 to 0.8% of extranodal site of malignant lymphoma and 0.1% of all prostatic neoplasms [4, 11, 13]. Secondary prostatic lymphoma from other
sites is also uncommon [2]. Due to its rarity, prostatic lymphoma is less considered in situ-ation of urinary obstruction. Besides, prostatic carcinoma may also mimic lymphoma histo-logically [12]. We reported an elderly male with initial presentation of urinary obstruction and enlargement of the prostate gland. The
showed the atypical lymphoid cells infiltra-tion. The microscopic findings of back mass biopsy composed of small to medium atypical lymphoid cell diffused infiltration (Figure 4). Immunohistochemical staining for the lymphoid cells showed CD3 (-), CD5 (-), CD10 (+), CD20 (+), CD23 (-), and Cyclin D1 (-).
Besides, elevated lactate dehydrogenase (LDH) level up to 320 IU/L was noted. The diagnosis was confirmed by histopathology
with immunohistochemistry as secondary prostatic lymphoma.
CASE REPORT
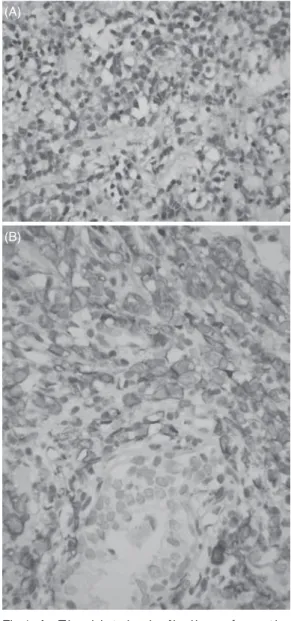
A 74-year-old male visited our outpa-tient department of urology with the chief complaints of acute urinary retention with insertion of Foley catheter for 13 days. He also suffered from progressive urinary frequency with urgency, weak stream, dribbling, and nocturia for years. Physical examination including digital rectal examination was done and mildly enlarged prostate gland with smooth and rubbery consistency was found. Performance Status showed ECOG I. Besides, several enlarged lymph nodes (LNs) were palpable over the left neck. PSA level was 0.86 ng/mL. Urinary analysis revealed 3+ occult blood. Chest x-ray plain film displayed wide-ness of mediastinum. Under the impression of benign prostatic hyperplasia with acute urinary obstruction, he received transurethral resec-tion of the prostate (TURP). Subsequently, the pathology of TURP revealed diffused infiltra-tion of neoplastic cells (Figure 1A). Immuno-histochemical staining for tumor cells showed cytokeratin (-), prostate specific antigen (-), leukocyte common antigen (+), CD3 (-) and CD20 (+) (Figure 1B). Final pathologic diag-nosis is malignant B cell lymphoma.
Tumor staging work-up was arranged, and Gallium scan showed several areas of increased gallium uptake in the right axillary region, left posterior lower neck and left anterior abdomen (Figure 2). Computed tomography (CT) scan of the head and neck, chest and abdomen found lymphoma lesions involving neck, mediastinum, and paraaortic region (Figure 3). Gastroscopy was done and scattered small shallow ulcers at the great curvature of the stomach were found. Excision biopsy of upper back mass and gastric ulcer both also
Fig 1. A . T h e h i s t o l o g i c f i n d i n g s f r o m t h e TURP specimen revealed diffused infil-tration of neoplastic cells (400X). B. Immunohistochemical stain for tumor cells showed positive for CD20 (400X).
(B) (A)
bone morrow biopsy was done and showed free of malignant lymphoma involvement. His B-symptoms were not obvious and the final diagnosis was disseminated diffused large B cell lymphoma with prostate gland, stomach, back soft tissue, and multiple areas LNs involvement. Staged IVE was made according to the Ann Arbor classification system. Four out of 5 risk factors including age 60 years, elevated LDH, 2 extranodal sites of disease, and Ann Arbor Stage III or IV were found based on the prognostic indices used in non-Hodgkin’s lymphoma from International Prognostic Index [15].
He received four cycles of chemotherapy with rituximab, cyclophosphamide, etoposide, vincristine and prednisone (R-CEOP). Regres-sion of the left neck LNs and abdominal LNs were noted after chemotherapy. However, three months later, lower back pain both-ered him. Abdominal CT showed relapse of
lymphadenopathy over the retroperitoneum from the level of kidney to presacral space. He received salvage one cycle of chemo-therapy with CEOP regimen followed by the radiotherapy (RT) to the paraaortic masses. The planned dose was 45 Gy in 25 fractions. RT was discontinued at 21.6 Gy in 12 frac-tions because of exacerbation of his condition. He only survived 9 months after the initial diagnosis.
DISCUSSION
Adenocarcinoma accounts for more than 90% of all prostatic malignancies. Other histological subtypes of prostatic cancers represent only 5 to 10%. For the diagnosis of primary prostatic lymphoma, three criteria need to meet: 1) presenting symptoms attrib-utable to prostatic enlargement; 2) involve-ment of the prostate predominantly, with or
Fig 2. Gallium tumor scan displayed several areas of increased gallium uptake areas in the right axillary region, left posterior lower neck and left anterior abdomen.
without involvement of adjacent tissue; and 3) absence of involvement of the liver, spleen, or LNs within 1 month of diagnosis of pros-tatic involvement [8]. We demonstrated a case of disseminated lymphoma with multiple
extranodal organs and LNs involvement. His disease did not fit the criteria for the primary prostatic lymphoma, and should be considered as a secondary prostatic lymphoma.
Involvement of the prostate gland by malignant lymphoma should be considered as one of the late manifestations of advanced nodal disease although it is uncommon. An autopsy series of 6000 male patients who died of cancer revealed only 185 (3.1%) with metas-tasis to prostate gland, of which only 49 (0.8%) were non-Hodgkin’s lymphoma [16]. Bost-wick et al. performed a study to investigate 62 cases of malignant lymphoma involving the prostate gland and found the secondary involvement was more common than primary involvement (65% vs. 35%). In this study, the patients with secondary involvement were, on average, six years younger than those with primary lymphoma (median age of 60 years vs. 66 years) [2]. Both the characteristics are similar in secondary and primary lymphoma of the bladder and ovary [7, 10]. Our patient was a little bit older than the average.
The clinical manifestation of the pros-tatic lymphoma is difficult to distinguish from other diseases of the prostate gland causing lower urinary tract obstructive symptoms. Urgency, frequency, and nocturia were most
Fig 4. The histologic findings of back mass composed of small to medium atypical lymphoid cells diffused infiltration (400X).
Fig 3. CT scan showed suspected disseminated lymphoma involving neck (A), mediastinum (B), and paraaortic region (C) LNs.
(A)
(B)
common presenting symptoms [2, 11, 14]. Our patient had the typical clinical presen-tation of urinary symptoms. Because the clinical symptoms/signs mimicked benign prostatic hyperplasia, our patient, like most other patients, underwent TURP for the diag-nosis. Systemic symptoms including fever, chills, night sweats, and weight loss were not commonly seen [2]. Our patient did not have any B-symptoms, either. Histopathology for primary or secondary prostatic lymphoma was mostly non-Hodgkin’s lymphoma, and the majority was diffused lymphoma [2, 3, 5]. Our patient had follicular lymphoma with progres-sion to diffused large B cell lymphoma. For secondary prostatic lymphoma, LNs were still the most common site for extraprostatic involvement, followed by spleen, bone and liver [2]. Our patient had LNs, soft tissue, and gastric involvement besides the prostate gland. In the study of Bostwick et al., specific survival of the lymphoma was 64% at 1 year, 50% at 2 years, and 33% at 5 years. Patients with primary and secondary prostatic lymphoma did not differ in the duration of survival (P = 0.97). However, Bostwick et al. found poor prognosis of prostatic lymphoma regardless of patient age, histologic type, treatment, or clinical stage of disease at presentation [2]. Because prostatic lymphoma is rare, the suggested standard management is optimal chemotherapy with rituximab or doxorubicin based regimen as reported in previous studies [1, 14]. Due to advanced stage of disseminated lymphoma of our case, this patient was expected to have a grave outcome. He received four cycles of chemo-therapy with R-CEOP regimen and got partial response of his disease. For stage IE primary prostatic lymphoma, some studies reported good response treated by RT [6, 9]. In our case, RT was not used as major treatment because this patient was stage IVE lymphoma with prostatic involvement at the time of
diagnosis. According to the NCCN guidelines, systemic chemotherapy should be better for him as category I recommendation. We only performed salvage RT to the enlarged para-aortic LNs for symptoms relief. However, his condition was still in progression during RT and did not finish the RT course.
CONCLUSION
We report a rare case with disseminated malignant lymphoma involving the prostate gland at the beginning. He received standard chemotherapy as the major treatment, but only survived 9 months after the initial diagnosis. For elderly men with symptoms of urinary tract obstruction and abnormal digital rectal examination, we should consider the prostatic lymphoma in the differential diagnosis, and early application of RT for symptoms relief as well.
REFERENCES
1. Antumes AA, Dall’ogilo M, Srougi M: Primary lymphoma of the prostate: a rare cause of urinary obstruction. International Braz J Urol 2004; 30: 410-412.
2. Bostwick DG, Iczkowski K A, Amin MB, Discigil G, Osborne B: Malignant lymphoma involving the prostate: report of 62 cases. Cancer 1998; 15: 732-738.
3. Fang T: Clinical Analysis of 29 Cases with Primary Malignant Lymphoma of the Pros-tate. Chinese J Clin Oncol 2007; 4: 129-132. 4. Freeman C, Berg JW, Cutler SJ: Occurrence
and prognosis of extranodal lymphomas. Cancer 1972; 29: 252-260.
5. Fukutani K, Koyama Y, Fujimori M, Ishida T: Primary malignant lymphoma of the prostate: report of a case achieving complete response to combination chemo-therapy and review of 22 Japanese cases. Jpn J Urol 2003; 94: 621-625.
the prostate. Leuk Lymphoma 2001; 41: 445-449.
7. Kempton CL, Kurtin PJ, Inwards DJ, Wollan P, Bost wick DG: Malig nant lymphoma of the bladder: evidence from 36 cases that low grade lymphoma of MALT type is the most common primary bladder lymphoma. Am J Surg Pathol 1997; 21: 1324-1333.
8. King LS, Cox TR: Lymphosarcoma of the prostate. Am J Pathol 1951; 27: 801–823. 9. Leung TW, Tung SY, Sze WK, et al.:
Primary non-Hodgkin’s lymphoma of the prostate. Clin Oncol 1997; 9: 264-266. 10. Monterroso V, Jaffe ES, Merino MJ,
Medieros LJ: Malignant lymphomas involving the ovary: a clinicopathologic analysis of 39 cases. Am J Surg Pathol 1993; 17: 154-170.
11. Patel DR, Gomez GA, Henderson ES, Gamarra M: Primary prostatic involvement in non Hodgkin lymphoma. Urology 1988; 32: 96-98.
13. Sarris A, Dimopoulos M, Pugh W, Caba-nillas F: Primary lymphoma of the prostate: good outcome with doxorubicin-based combination chemotherapy. J Urol 1995; 153: 1852-1854.
14. Taleb A, Ismaili N, Belbaraka R, et al.: Primary lymphoma of the prostate treated with rituximab-based chemotherapy: a case report and review of the literature. Cases Journal 2009; 2: 8875.
15. T h e I n t e r n a t i o n a l N o n - H o d g k i n' s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodg-kin's lymphoma. N Engl J Med 1993; 329: 987-994.
16. Zei n TA, Huben R , La ne W, et al.: Secondary tumors of the prostate. J Urol 1985; 133: 615-616.
侵犯攝護腺之惡性淋巴瘤:一病例報告
孫立民1 黃英彥2 張乃仁3 鍾立民4 陸教義5 梁基安6,7 李蠻剛8 國軍左營總醫院 放射腫瘤科1 病理科3 血液腫瘤科4 放射診斷科5 泌尿科8 高雄長庚醫院 放射腫瘤科2 中國醫藥大學附設醫院 腫瘤治療科6 中國醫藥大學 醫學院7 發生於攝護腺之惡性淋巴瘤,不論是原發性或繼發性,都是非常罕見的。我們報告一位 74 歲男性因急性尿滯留的症狀求醫,進而被診斷出罹患侵犯攝護腺癌之彌散性惡性淋巴瘤。肛門 指診發現光滑而有彈性之輕微攝護腺肥大。在良性攝護腺肥大之初步診斷之下,病患接受了經 尿道攝護腺刮除術。病理報告發現充滿腫瘤細胞之浸潤。特殊之免疫組織化學染色顯示 CD20 為陽性,符合為惡性B 細胞淋巴瘤。全身性檢查發現疾病散佈多區域。背部腫塊切片發現廣泛 浸潤中小非典型淋巴細胞,特殊之免疫組織化學染色顯示 CD10 及 CD20 為陽性,診斷為濾泡型淋巴瘤。病患接受了四次的 rituximab, cyclophosphamide, etoposide, vincristine and prednisone (R-CEOP) 化學治療,但腫瘤很快復發。病患再接受補救性化學治療及主動脈旁腫大之淋巴結的
放射治療。由於病情惡化病患沒能完成全程之放射治療,病患於最初診斷後的 9 個月帶病死亡。
[ 放射治療與腫瘤學 2011; 18(1): 67-75]