Myocardial tissue characterization based
on a polarization-sensitive optical coherence
tomography system with an ultrashort pulsed laser
Chia-Wei Sun Yih-Ming Wang National Taiwan University
Graduate Institute of Electro-Optical Engineering Taipei, Taiwan
Long-Sheng Lu National Taiwan University Graduate Institute of Pharmacology Taipei, Taiwan Chih-Wei Lu I-Jen Hsu Meng-Tsan Tsai C. C. Yang Yean-Woei Kiang National Taiwan University
Graduate Institute of Electro-Optical Engineering and
Department of Electrical Engineering No. 1, Section 4, Roosevelt Road Taipei, Taiwan
E-mail: [email protected]
Chau-Chung Wu National Taiwan University
Department of Primary Care Medicine and
Department of Internal Medicine Taipei, Taiwan
Abstract. A polarization-sensitive optical coherence tomography 共PSOCT兲 system using a femtosecond-laser as the broadband light source is implemented with the axial resolution of5m in free space. Through the design of path-length difference between the two polar-ization inputs and the modulation of one of the polarpolar-ization inputs, the PSOCT images of various input and output polarization combina-tions can be distinguished and simultaneously collected. The PSOCT system is then used for in vitro scanning of the myocardium tissues of normal and infarcted rat hearts. The destruction of the birefringence nature of the fiber muscle in the infarcted heart can be clearly observed. © 2006 Society of Photo-Optical Instrumentation Engineers.
关DOI: 10.1117/1.2363358兴
Keywords: medical imaging; microscopy; lasers; optical systems; polarization. Paper 04002RRR received Jan. 5, 2004; revised manuscript received May 12, 2005 and Feb. 15, 2006; accepted for publication May 23, 2006; published online Oct. 20, 2006.
1 Introduction
Biological tissues usually respond to various environmental cues with simultaneous functional and structural changes. The efforts to resolve material properties of living biological tis-sues with physical factors, also known as tissue characteriza-tion, suggested that the material properties of biological tis-sues are more sensitive indicators of prognosis compared with functional parameters in some pathological processes.1,2The micro-architecture and composition of biological tissues are the major determinants of their material properties. Such in-formation is particularly useful in the field of cardiovascular medicine. Cardiovascular death is a major health issue in de-veloped countries. The major component of the heart is bulky myocardium, which is composed of quasi-regularly arranged muscle fibers. The average width of a normal human ventricu-lar muscle fiber is around 23m.3 Most heart diseases are associated with structural changes. For example, after an
acute myocardial infarction, the damaged myocardium be-comes edematous and contractured. Subsequently, the regular muscle fiber arrangement is lost within one week. In this situ-ation, the infarcted area is replaced by randomly oriented fi-brous scar within six weeks. Further pathological remodeling would result in disarrayed and hypertrophied muscle fibers in the remaining working myocardium. Any tool that character-izes detailed myocardial tissue structures can be of great value to evaluate subsequent events after a myocardial infarction for further diagnosis and treatment.
Although physiological measurements can well describe functional alterations as diseases progress, current tools for detecting the corresponding structural changes still greatly rely on post-mortem or in vitro microscopic pathological ex-amination. This technical limitation led to the traditional con-cept that morphological changes occurred later than the func-tional alterations. However, with the development of in vivo tissue characterization techniques, information derived from structural changes seemed to be a more sensitive marker of adaption–maladaptation processes. One of the possible
rea-1083-3668/2006/11共5兲/054016/7/$22.00 © 2006 SPIE Address all correspondence to C. C. Yang, Graduate Institute of Electro-Optical
Engineering, National Taiwan Univ., 1, Roosevelt Road, Section 4, Taipei, 10617 Taiwan; Tel: 886 2 23657624; Fax: 886 2 23652637
sons that material properties more vividly reflect the progress of disease in the early phase is that biological tissues tend to respond to persistent perturbation to maintain functional ho-meostasis at the price of remodeling of tissue micro-architecture and cellular components. These subtle structural cues can be of important clinical implications. In the case of myocardial hypoperfusion, timely revascularization would rescue ischemic but viable myocardial tissue, resulting in less scar formation and better prognosis. The cardiac functional recovery relies on the amount and distribution of viable tis-sues and the success of revascularization. This is indeed a diagnostic challenge for all times. Noninvasive methods to detect these tissue characteristics changes include proton magnetic resonance imaging with gadolinium or dysprosium chelates共e.g., Gd-DTPA兲4,5and detection of released soluble proteins 共e.g., lactate dehydrogenase, creatine kinase, tropo-nin, and myoglobin兲,6 particularly during the procedure of coronary artery bypass surgery. While currently there are ef-fective techniques for noninvasive, in vivo diagnosis of myo-cardial injury, there is a need for effectively monitoring the membrane disruption in exposed hearts共both in the operating room and in research兲. For this need, the aforementioned tech-niques are ineffective.7The damaged myocardium would be-come edematous, contracted, and infiltrated with inflamma-tory cells and would lose regular alignment of muscle fibers. However, to identify most of these early structural changes, spatial resolution up to the sub-mm level is required. Such resolution is beyond the limit of all current systems. There-fore, the development of an adequate diagnostic modality that can characterize the tissue of interest with microscopic reso-lution is needed.
Optical coherence tomography 共OCT兲 has proven useful for biological tissue monitoring of high resolution and fast scanning.8 With super-continuum light sources, the axial resolution of OCT has been pushed down to around, or even below,1 m.9–12 Also, because of the development of rapid-scanning optical delay line 共RSODL兲 and other tech-niques for fast scanning and data processing, an imaging speed as high as more than 16 frames per sec共100⫻50 pix-els兲 has been reported.13–15 OCT has been widely applied to scanning various portions of biological tissues and the diag-noses of various diseases, including urinary bladder,16 esophagus,17 central corneal epithelial,18 gastrointestinal tissue,19atherosclerosis,20and human mucosa.21Recently, at-tention to OCT development has focused on the use of the polarization discrimination techniques for monitoring the an-isotropy characteristics of biological tissues.22–25 Such a method has shown its great potential, particularly for diagnos-ing filamentous tissues. Arranged structures in biological tis-sues, in either the macroscopic or microscopic level, can re-flect tissue birefringence. The anisotropy of proteins such as collagen, which builds up the extracellular matrix, leads to the birefringence nature. The molecular packing structure of the collagen fibers results in a higher index of refraction along the length of the fiber, when compared with that in the direction of their cross-section, leading to linear birefringence. Also, the myosin, which is contained in thick filaments of skeletal muscle, and elastin, which is contained in extracellular fiber, reveal anisotropy and hence contribute to the birefringence nature in myocardial tissues. Actually, birefringence can occur with anisotropic structures in other tissues, such as tendons,
muscles, nerves, bones, cartilage, and teeth. In many situa-tions, such a tissue loses its inherent birefringence character-istics due to a microstructure alteration with a certain disease. Polarization-sensitive OCT共PSOCT兲 has been used for re-cording two-dimensional images of the change in polarization of circularly incoming light backscattered from a biological sample with birefringence.26,27In such a system, the detected backscattered signals of the sample not only provide the in-formation of the sample structure but also reveal sample bire-fringence as a function of depth. With a systematic analysis of the backscattered light from biological tissues, the Stokes–
Muller formalism can be built based on PSOCT
measurements.28–32For easier alignment and handling, fiber-based PSOCT systems were usually used.33–35To increase the scanning speed, we demonstrated the use of the spectral do-main PSOCT scheme.36,37 Based on the Linnik microscope instrument, the full-field PSOCT was also developed to achieve micron-scale resolution with a thermal-light source.38,39Because PSOCT enables us to detect the polariza-tion states of backscattered signals, it can be used as a sensi-tive indicator of disorganization and degradation of tissues for biomedical diagnosis, including tendons and ligaments,40 cartilage,41,42dentin and enamel,43,44burn lesions of skin,45–47 cornea,48,49retina,50retinal nerve fibers,51coronary tissue,52,53 and invasive basal cell carcinoma.54
In a PSOCT system, the simultaneous collection of OCT images of various polarization combinations can help in scan-ning efficiency and data consistency. Two identical light sources were simultaneously used for implementing such PSOCT image scanning. In this effort, so far the used light source is restricted to super-luminescence diodes共SLDs兲. Al-though an SLD has the advantages of stability, compactness, and portability, it usually has a relatively lower power and narrower spectral width when compared with an ultrashort pulsed solid-state laser or a super-continuum source pumped with such a laser. With an ultrashort pulsed solid-state laser, the broader spectrum leads to higher resolution and the higher output power results in higher sensitivity.
In this paper, we report the implementation of a PSOCT system and its application to diagnosing myocardium tissues. In the system, a relative delay of the pulsed signals between the two input polarization components is designed to avoid their interference. Also, modulation of signals in one of the input polarization paths is used for distinguishing the inter-fered signals at the detectors between the two polarization conditions. With such a setup, the OCT images of various polarization combinations can be obtained simultaneously. The PSOCT system is then applied to diagnosing the differ-ences of myocardium tissues between the normal and inf-arcted rat hearts. To determine the optimal therapy for such diseases, it is important to understand the structure of abnor-mal myocardium tissues. Therefore, the anisotropy informa-tion from PSOCT images of such a tissue is quite helpful.
This paper is organized as follows: in Section 2, we de-scribe the experimental setup, experimental procedures, and sample preparation. Experimental results are discussed in Sec-tion 3. Finally, discussions and conclusions are drawn in Section 4.
2 Experimental Procedures and Sample
Preparation
The setup of the PSOCT system is shown in Fig. 1. It was built with a Verdi-laser-pumped mode-lockedTi: sapphire la-ser 共Femtosource Compact Pro, FEMTOLASERS, Austria兲, which provided12 fs, 76-MHz pulses with the central wave-length at800 nm. The full-width-at-half-maximum共FWHM兲 of the laser spectrum ranged from 80 to 100 nm, depending on the mode-locking condition. Such a spectral width corre-sponds to the axial resolution between 2.8 and3.5m in free space. The output of theTi: sapphire laser was horizontally polarized. It was rotated into 45° linear polarization through a half-wave plate共QWPO-780-10-2-R10, CVI兲. Then the laser beam was split into two branches of the horizontal and verti-cal polarization with different path lengths by a polarization beam splitter共PBSH-670-980-100, CVI兲. The path-length dif-ference meant to avoid the interdif-ference of signals between the two polarization inputs. A chopper was used for 4-kHz modu-lation to differentiate the signals of the vertical polarization input from the other. The two input beams were merged with a nonpolarization beam splitter 共50/50 splitting ratio; BBS-650-1100-1025-45, CVI兲. About 600 mW of the average power of laser pulses was applied to the free-space Michelson interferometer. Optical signals in the reference arm passed through a zeroth-order quarter-wave plate 共QWPO-780-10-4-R10, CVI兲, set at 22.5° with respect to the horizontal direc-tion, such that the signal polarization was rotated by 45° on reflection from the RSODL. In the reference arm, after return-ing from the RSODL and doubly passreturn-ing through the quarter-wave plate, the horizontal polarization component of the in-cident light was converted into the 45° polarization while the vertical polarization component of the incident light was con-verted into the −45° direction. The RSODL in the reference arm was built for phase modulation and depth scanning. The diffraction efficiencies of the used grating共400 lines/mm, Ri-chardson Grating Laboratory兲 in the RSODL are 73% and 77% for the horizontal and vertical polarization components, respectively. Such a difference does not affect the operation of the PSOCT system. For dispersion compensation of the OCT system, we adjusted the separation between the diffractive grating and the lens in the used RSODL.55Another quarter-wave plate, set at 45° with respect to the horizontal direction, was placed in the sample arm such that circularly polarized light was incident upon the sample. The polarization states at the sample surface of the two incident polarization directions were right- and left-hand circular polarization, respectively.
The reference beam combined with the backscattered sample beam through the nonpolarization beam splitter. A polariza-tion beam splitter was used before optical signal detecpolariza-tion for output polarization discrimination. The two polarization out-puts of interfered signals were detected by two photo-detectors共model 2001, New Focus兲, D1 and D2, respectively. The signals were then processed with two bandpass filters 共FV-665, NF Electronic Instruments兲 to extract the OCT im-ages of various polarization combinations. Because of the use of the chopper, the central frequency of the bandpass filter for the vertical polarization input was shifted by4 kHz from that for the other polarization. The transverse resolution of the PSOCT system was about 10m. The sensitivity was esti-mated to be about80 dB. It can be improved if a more stable laser source is used. The focused laser-beam diameter on the tissue samples was around3.5 mm. The real power applied to the samples was only5 mW, corresponding to 52 mW/ cm2
in average power density. It should be safe for in vivo mea-surements with such a power density.
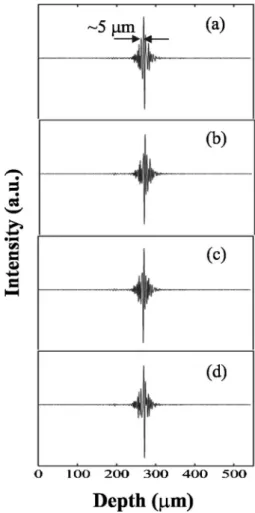
The four parts of Fig. 2 show the interference fringe pat-terns of the four polarization combinations recorded with the reflection from a glass surface. Parts共a兲–共d兲 correspond to the cases of HH, HV, VH, and VV, respectively. The first共second兲 letter represents the input 共output兲 polarization direction. H and V mean the horizontal and vertical directions,
respec-Fig. 1 Setup of the PSOCT system. PBS: polarization beam splitter; BS:
beam splitter; M: mirror; C: chopper; HWP: half-wave plate; QWP: quarter-wave plate; D1 and D2: photo-detectors.
Fig. 2 Interference fringe patterns from surface reflection with parts
共a兲–共d兲 for the input and output polarization combinations HH, HV, VH, and VV, respectively.
tively. The fringe envelopes of the four polarization combina-tions look similar and all have the FWHM around 5 m, corresponding to a resolution of about3.57m in biological tissues. With this result, we believe that the dispersion mis-match is essentially compensated for in this free-space PSOCT system.
The PSOCT system was then used for scanning normal and abnormal myocardium tissues of rats. Sample preparation was conducted in accordance with the R.O.C. Animal Protec-tion Law 共Scientific Application of Animals兲, 1998. After a bolus of intraperitoneal pentobarbital共50 mg/kg兲, the left an-terior descending coronary artery of an adult WKY rat was ligated. The ligation was kept for eight weeks for the infarc-tion to become mature. A sham operainfarc-tion was performed on the other rat as on the normal sample for comparison. To harvest the hearts, a lethal dose of sodium pentobarbital was administered. The animals were retrogradely perfused with heparinized PBS 共10 units/ml兲 for 15 min. The hearts were then quickly removed and fixed onto the sample stage of the PSOCT system. The midventricular myocardium around the left anterior descending artery was scanned.
3 Experimental Results
Parts 共a兲–共f兲 of Fig. 3 show the PSOCT images of normal
myocardial tissue of a rat for the structure, phase retardation, HH, HV, VH, and VV polarization combinations, respectively. In the images, the sporadic vertical line structures are attrib-uted to laser instability. As mentioned before, the birefrin-gence characteristics of myocardial tissue originate from its anisotropic fiber architecture.56The phase retardation between 0 to, as shown in Fig. 3共b兲, indicates the polarization evo-lution in the myocardium. In a tissue sample of isotropic scat-tering, the nonpolarized backscattered light should lead to a continuous-phase retardation distribution in image. In the four polarization-resolved images 关Figs. 3共c兲–3共f兲兴, a smooth epi-cardial contour with a layered pattern can be seen. A middle layer of a weak signal can be clearly seen in the HV and VH components of the PSOCT images of the normal heart, as indicated with the white arrows in Figs. 3共d兲 and 3共e兲. The dark layer is supposed to originate from the variation of fiber muscle orientation along the sample depth. The orientation of the muscle bundles rotates by approximately 180° from epi-cardium to endoepi-cardium when examined in a midventricular cross-section. Hence, the muscle fibers in the middle part of the ventricular wall are approximately perpendicular to those in the epi- and endocardium. The dark layer in the OCT im-ages corresponded to this topography. Because the structure image 关Fig. 3共a兲兴 shows quite a continuous distribution, we can conclude that the HV and VH images关Figs. 3共d兲 and 3共e兲兴 reflect real tissue birefringence.
On the other hand, the PSOCT images acquired from an infarcted heart displayed a significant difference. Figures 4共a兲–4共f兲 show the PSOCT images of the infarcted heart for the structure, phase retardation, and HH, HV, VH, and VV polarization combinations, respectively. Here, one can see that the layered patterns in Fig. 3 disappear. In the macroscopic observation, the epicardial surface of the scanned area was contracted and uneven. The scarred ventricular wall was also less elastic, compared with the rest of the heart. The PSOCT images show an exaggerated border in the epicardial surface. In addition, the patchy pattern of the PSOCT images suggests the presence of marked heterogeneities in the sample. In the sample, the repair process was almost complete, and the or-derly arranged muscle structure was replaced with randomly oriented collagen bundles.31 Hence, this corresponds well to our finding that in the scar region of the infarcted heart, the patchy pattern replaced the layered pattern in the PSOCT im-ages, as shown in Fig. 4.
4 Discussions and Conclusions
We have demonstrated that the PSOCT technique could dif-ferentiate scars from normal myocardium in vitro. Such a technique has the potential for providing real-time informa-tion about myocardial viability, which can assist the decision of revascularization during percutaneous coronary interven-tion. Such information is particularly important in the cases of delayed presentation of a myocardial infarction 共post-infarction angina兲, previously undetected multivessel dis-eases, and multiple stenosis with occluded proximal seg-ments. Currently, these issues are addressed with the functional data such as intracoronary flow velocity and pres-sure. The PSOCT imaging provides an alternative source of information based on myocardial morphology. The possible application of this technique would not and should not be
Fig. 3 PSOCT images of the myocardium tissue of the normal rat heart
with parts共a兲–共f兲 for the structure, phase retardation, and input and output polarization combinations HH, HV, VH, and VV, respectively.
limited to the evaluation of myocardial viability. Since this technique is sensitive to interstitial collagen deposition, early diagnosis of hereditary cardiomyopathy, transplant rejection, and cardiac fibrosis would also be potential fields of application.
As we pointed out earlier, the major strength of this tech-nique is the high spatial resolution in comparison to PET, CT, MR, and dobutamine stress echocardiography共DSE兲. Another advantage of this technique is its capability to determine the supply artery of injured myocardium without the assumption of normal segmental supply pattern. Currently, the available imaging methods, including PET, DSE, and thallium scan, all detect possible infarct-related artery with the principle of seg-mental supply of coronary arteries. However, these methods do not work well in the cases of watershed, extensive collat-eral formation, variants of coronary supply pattern, and poor flow. Approaching the proximity of injured myocardium and detecting its viability in the stenosed artery with PSOCT can help in solving such a problem.
In summary, we have implemented a PSOCT system with a femtosecond laser as the broadband light source. The axial resolution reached 5m in free space. With the design of a path-length difference between the two polarization inputs and the modulation of one of the polarization inputs, the
PSOCT images of various input and output polarization com-binations could be well distinguished and simultaneously col-lected. The PSOCT system was then successfully used for in
vitro characterization of normal and infarcted myocardial
tis-sues. To avoid the huge calculations with the Stokes–Mueller formalism in a PSOCT system, we used the phase-retardation images to describe the birefringence effect of myocardium. Therefore, this system can provide real-time information about the changes of the anisotropic structures in heart tissues. Although only in vitro experiments were reported in this pa-per, this PSOCT system could offer a potential diagnostic mo-dality for in vivo tissue characterization. Future work includes the construction of a fiber-based PSOCT system of higher stability for in vivo diagnosis of abnormal myocardium tissues.55,56In this new PSOCT system, a light source with the central wavelength around 1300 nm will be used for deeper tissue penetration. Also, the implementation with a catheter and/or endoscopic system will be investigated in future research.
Acknowledgment
This research was supported by the National Health Research Institute, The Republic of China, under Grant NHRI-EX94-9220EI.
References
1. V. Giglio, V. Pasceri, L. Messano, F. Mangiola, L. Pasquini, A. Dello Russo, A. Damiani, M. Mirabella, G. Galluzzi, P. Tonali, and E. Ricci, “Ultrasound tissue characterization detects preclinical myocar-dial structural changes in children affected by Duchenne muscular dystrophy,” J. Am. Coll. Cardiol. 42, 309–316共2003兲.
2. C. C. Wu, Y. B. Liu, L. C. Lin, Y. L. Ho, C. S. Liau, and Y. T. Lee, “Ultrasonic tissue characterization with integrated backscatter during isotropic stimulation,” Ultrasound Med. Biol. 26, 1413–1420共2000兲. 3. O. M. Hess, J. Schneider, H. Nonogi, J. D. Carroll, K. Schneider, M. Turina, and H. P. Krayenbuehl, “Myocardial structure in patients with exercise-induced ischemia,” Circulation 77, 967–977共1988兲. 4. S. M. Eleff, I. J. McLennan, G. K. Hart, Y. Maruki, R. J. Traystman,
and R. C. Koehler, “Shift reagent enhanced concurrent 23Na and 1H magnetic resonance spectroscopic studies of transcellular sodium dis-tribution in the dog brain in vivo,” Magn. Reson. Med. 30, 11–17 共1993兲.
5. M. Saeed, “New concepts in characterization of ischemically injured myocardium by MRI,” Exp. Biol. Med. 226, 367–376共2001兲. 6. R. N. Johnson, N. L. Sammel, and R. M. Norris, “Depletion of
myo-cardial creatine kinase, lactate dehydrogenase, myoglobin and K1 after coronary artery ligation in dogs,” Cardiovasc. Res. 15, 529–537 共1981兲.
7. S. P. Nighswander-Rempel, R. A. Shaw, B. Kuzio, and V. V. Kupriy-anov, “Detection of myocardial cell damage in isolated rathearts with near-infrared spectroscopy,” J. Biomed. Opt. 9, 779–787共2004兲. 8. D. Huang, E. A. Swanson, C. P. Lin, J. S. Schuman, W. G. Stinson,
W. Chang, M. R. Hee, T. Flotte, K. Gregory, C. A. Puliafito, and J. G. Fugimoto, “Optical coherence tomography,” Science 254, 1178–1181 共1991兲.
9. W. Drexler, U. Morgner, F. X. Kärtner, C. Pitris, S. A. Boppart, X. D. Li, E. P. Ippen, and J. G. Fujimoto, “In vivo ultrahigh-resolution optical coherence tomography,” Opt. Lett. 24, 1221–1223共1999兲. 10. B. Povazay, K. Bizheva, A. Unterhuber, B. Hermann, H. Sattmann,
A. F. Fercher, and W. Drexler, “Submicrometer axial resolution op-tical coherence tomography,” Opt. Lett. 27, 1800–1802共2002兲. 11. K. Bizheva, B. Považay, B. Hermann, H. Sattmann, W. Drexler, M.
Mei, R. Holzwarth, T. Hoelzenbein, V. Wacheck, and H. Peham-berger, “Compact, broad-bandwidth fiber laser for sub-2-m axial resolution optical coherence tomography in the 1300-nm wavelength region,” Opt. Lett. 28, 707–709共2003兲.
12. Y. Wang, Y. Zhao, J. S. Nelson, Z. Chen, and R. S. Windeler, “Ultrahigh-resolution optical coherence tomography by broadband continuum generation from a photonic crystal fiber,” Opt. Lett. 28,
Fig. 4 PSOCT images of the myocardium tissue of the infarcted rat
heart with parts共a兲–共f兲 for the structure, phase retardation, and input and output polarization combinations HH, HV, VH, and VV, respectively.
182–184共2003兲.
13. Z. Ding, Y. Zhao, H. Ren, J. S. Nelson, and Z. Chen, “Real-time phase-resolved optical coherence tomography and optical Doppler tomography,” Opt. Express 10, 236–245共2002兲.
14. V. Westphal, S. Yazdanfar, A. M. Rollins, and J. A. Izatt, “Real-time, high velocity-resolution color Doppler optical coherence tomogra-phy,” Opt. Lett. 27, 34–36共2002兲.
15. M. J. Cobb, Xiumei Liu, and Xingde Li, “Continuous focus tracking for real-time optical coherence tomography,” Opt. Lett. 30, 1680– 1682共2005兲.
16. T. Q. Xie, M. L. Zeidel, and Y. T. Pan, “Detection of tumorigenesis in urinary bladder with optical coherence tomography: Optical charac-terization of morphological changes,” Opt. Express 10, 1431–1443 共2002兲.
17. R. V. Kuranov, V. V. Sapozhnikova, I. V. Turchin, E. V. Zagainova, V. M. Gelikonov, V. A. Kamensky, L. B. Snopova, and N. N. Prodanetz, “Complementary use of cross-polarization and standard OCT for dif-ferential diagnosis of pathological tissues,” Opt. Express 10, 707–713 共2002兲.
18. J. Wang, J. Thomas, I. Cox, and A. Rollins, “Noncontact measure-ments of central corneal epithelial and flap thickness after laser in situ keratomileusis,” Invest. Ophthalmol. Visual Sci. 45, 1812–1816 共2004兲.
19. A. M. Rollins, R. Ung-Arunyawee, A. Chak, C. K. Wong, K. Koba-yashi, M. V. Sivak, and J. A. Izatt, “Real-time in vivo imaging of human gastrointestinal ultrastructure by use of endoscopic optical coherence tomography with a novel efficient interferometer design,”
Opt. Lett. 24, 1358–1360共1999兲.
20. M. E. Brezinski, G. J. Tearney, B. E. Bouma, J. A. Izatt, M. R. Hee, E. A. Swanson, J. F. Southern, and J. G. Fujimoto, “Optical coher-ence tomography for optical biopsy,” Circulation 93, 1206–1213 共1996兲.
21. A. M. Sergeev, V. M. Gelikonov, G. V. Gelikonov, F. I. Feldchtein, R. V. Kuranov, N. D. Gladkova, N. M. Shakhova, L. B. Snopova, A. V. Shakov, I. A. Kuznetzova, A. N. Denisenko, V. V. Pochinko, Y. P. Chumakov, and O. S. Streltzova, “In vivo endoscopic OCT imaging of precancer and cancer states of human mucosa,” Opt. Express 1, 432–440共1997兲.
22. M. J. Everett, K. Schoenenberger, B. W. Colston Jr., and L. B. Da Silva, “Birefringence characterization of biological tissue by use of optical coherence tomography,” Opt. Lett. 23, 228–230共1998兲. 23. S. Guo, J. Zhang, L. Wang, J. S. Nelson, and Z. Chen,
“Depth-resolved birefringence and differential optical axis orientation mea-surements with fiber-based polarization-sensitive optical coherence tomography,” Opt. Lett. 29, 2025–2027共2004兲.
24. M. Pircher, E. Goetzinger, R. Leitgeb, and C. K. Hitzenberger, “Three-dimensional polarization sensitive OCT of human skin in vivo,” Opt. Express 12, 3236–3244共2004兲.
25. J. Zhang, S. Guo, W. Jung, J. S. Nelson, and Z. Chen, “Determination of birefringence and absolute optic axis orientation using polarization-sensitive optical coherence tomography with PM fibers,”
Opt. Express 11, 3262–3270共2003兲.
26. M. R. Hee, D. Huang, E. A. Swanson, and J. G. Fujimoto, “Polarization-sensitive low-coherence reflectometer for birefringence characterization and ranging,” J. Opt. Soc. Am. B 9, 903–908共1992兲. 27. J. F. de Boer, T. E. Milner, M. J. van Gemert, and J. S. Nelson, “Two-dimensional birefringence imaging in biological tissue by PS-OCT,” Opt. Lett. 22, 934–936共1997兲.
28. J. F. de Boer, T. E. Milner, and J. S. Nelson, “Determination of the depth-resolved Stokes parameters of light backscattered from turbid media by use of polarization-sensitive optical coherence tomogra-phy,” Opt. Lett. 24, 300–302共1999兲.
29. S. Jiao and L. V. Wang, “Two-dimensional depth-resolved Mueller matrix of biological tissue measured with double-beam polarization-sensitive optical coherence tomography,” Opt. Lett. 27, 101–103 共2002兲.
30. H. Ren, Z. Ding, Y. Zhao, J. Miao, J. S. Nelson, and Z. Chen, “Phase-resolved functional optical coherence tomography: Simultaneous im-aging of in situ tissue structure, blood flow velocity, standard devia-tion, birefringence, and Stokes vectors in human skin,” Opt. Lett. 27, 1702–1704共2002兲.
31. M. Todorovic´, S. Jiao, and L. V. Wang, “Determination of local po-larization properties of biological samples in the presence of diattenu-ation by use of Mueller optical coherence tomography,” Opt. Lett. 29, 2402–2404共2004兲.
32. S. Jiao and L. V. Wang, “Jones-matrix imaging of biological tissues with quadruple-channel optical coherence tomography,” J. Biomed.
Opt. 7, 350–358共2002兲.
33. C. E. Saxer, J. F. de Boer, B. H. Park, Y. Zhao, Z. Chen, and J. S. Nelson, “High-speed fiber-based polarization-sensitive optical coher-ence tomography of in vivo human skin,” Opt. Lett. 25, 1355–1357 共2000兲.
34. M. C. Pierce, B. H. Park, B. Cense, and J. F. de Boer, “Simultaneous intensity, birefringence, and flow measurements with high-speed fiber-based optical coherence tomography,” Opt. Lett. 27, 1534–1536 共2002兲.
35. B. H. Park, M. C. Pierce, B. Cense, and J. F. de Boer, “Jones matrix analysis for a polarization-sensitive optical coherence tomography system using fiber-optic components,” Opt. Lett. 29, 2512–2514 共2004兲.
36. Y. Yasuno, S. Makita, Y. Sutoh, M. Itoh, and T. Yatagai, “Birefrin-gence imaging of human skin by polarization-sensitive spectral inter-ferometric optical coherence tomography,” Opt. Lett. 27, 1803–1805 共2002兲.
37. Y. Yasuno, S. Makita, T. Endo, M. Itoh, T. Yatagai, M. Takahashi, C. Katada, and M. Mutoh, “Polarization-sensitive complex Fourier do-main optical coherence tomography for Jones matrix imaging of bio-logical samples,” Appl. Phys. Lett. 85, 3023–3025共2004兲. 38. J. Moreau, V. Loriette, and A.-C. Boccara, “Full-field birefringence
imaging by thermal-light polarization-sensitive optical coherence to-mography. I. Theory,” Appl. Opt. 42, 3800–3810共2003兲.
39. J. Moreau, V. Loriette, and A.-C. Boccara, “Full-field birefringence imaging by thermal-light polarization-sensitive optical coherence to-mography. II. Instrument and results,” Appl. Opt. 42, 3811–3818 共2003兲.
40. S. D. Martin, N. A. Patel, S. B. Adams, M. J. Roberts, S. Plummer, D. L. Stamper, J. G. Fujimoto, and M. E. Brezinski, “New technology for assessing microstructural components of tendons and ligaments,”
Int. Orthop. 27, 184–189共2003兲.
41. W. Drexler, D. Stamper, C. Jesser, X. D. Li, C. Pitris, and K. Saun-ders, “Correlation of collagen organization with polarization sensitive imaging in cartilage: Implications for osteoarthritis,” J. Rheumatol.
28, 1311–1318共2001兲.
42. X. Li, S. D. Martin, C. Pitris, R. Ghanta, D. L. Stamper, M. Harman, J. G. Fujimoto, and M. E. Brezinski, “High-resolution optical coher-ence tomography imaging of osteoarthritic cartilage during open knee surgery,” Arthritis Res. Ther. 7, R318–R323共2005兲.
43. A. Baumgartner, S. Dichtl, C. K. Hitzenberger, H.Sattman, B.Robl, A.Moritz, A. F.Fercher, and W.Sperr, “Polarization sensitive optical coherence tomography of dental structures,” Caries Res. 34, 59–69 共2000兲.
44. Y. Chen, L. Otis, D. Piao, and Q. Zhu, “Characterization of dentin, enamel, and carious lesions by a polarization-sensitive optical coher-ence tomography system,” Appl. Opt. 44, 2041–2048共2005兲. 45. B. H. Park, C. Saxer, S. M. Srinivas, J. Stuart Nelson, and J. F. de
Boer, “In vivo burn depth determination by high-speed fiber-based polarization sensitive optical coherence tomography,” J. Biomed.
Opt. 6, 474–479共2001兲.
46. S. Jiao, W. Yu, G. Stoica, and L. V. Wang, “Contrast mechanisms in polarization-sensitive Mueller-matrix optical coherence tomography and application in burn imaging,” Appl. Opt. 42, 5191–5197共2003兲. 47. S. M. Srinivas, J. F. de Boer, H. Park, K. Keikhanzadeh, H. L. Huang, J. Zhang, W. Q. Jung, Z. Chen, and J. S. Nelson, “Determination of burn depth by polarization-sensitive optical coherence tomography,”
J. Biomed. Opt. 9, 207–212共2004兲.
48. M. G. Ducros, J. F. de Boer, H.-E. Huang, L. C. Chao, Z. Chen, J. S. Nelson, T. E. Milner, and H. G. Rylander III, “Polarization sensitive optical coherence tomography of the rabbit eye,” IEEE J. Sel. Top.
Quantum Electron. 5, 1159–1167共1999兲.
49. E. Götzinger, M. Pircher, M. Sticker, A. F. Fercher, and C. K. Hitzen-berger, “Measurement and imaging of birefringent properties of the human cornea with phase-resolved, polarization-sensitive optical co-herence tomography,” J. Biomed. Opt. 9, 94–102共2004兲.
50. M. G. Ducros, J. D. Marsack, H. G. Rylander III, S. L. Thomsen, and T. E. Milner, “Primate retina imaging with polarization-sensitive op-tical coherence tomography,” J. Opt. Soc. Am. A 18, 2945–2956 共2001兲.
51. B. Cense, T. C. Chen, B. H. Park, M. C. Pierce, and J. F. de Boer, “In vivo depth-resolved birefringence measurements of the human retinal nerve fiber layer by polarization-sensitive optical coherence
tomog-raphy,” Opt. Lett. 27, 1610–1612共2002兲.
52. S. D. Giattina, B. K. Courtney, P. R. Herz, M. Harman, S. Shortkroff, L. Debra, D. L. Stamper, B. Liu, J. G. Fujimoto, and M. E. Brezinski, “Measurement of coronary plaque collagen with polarization sensi-tive optical coherence tomography 共PS-OCT兲,” Cardiovascular Re-vascularization Therapies Mtg. Washington, D.C., p. 609共2005兲. 53. M. C. Pierce, M. Shishkov, B. H. Park, N. A. Nassif, B. E. Bouma,
G. J. Tearney, and J. F. de Boer, “Effects of sample arm motion in endoscopic polarization-sensitive optical coherence tomography,”
Opt. Express 13, 5739–5749共2005兲.
54. J. Strasswimmer, M. C. Pierce, B. H. Park, V. Neel, and J. F. de Boer, “Polarization-sensitive optical coherence tomography of invasive basal cell carcinoma,” J. Biomed. Opt. 9, 292–298共2004兲. 55. W. K. Niblack, J. O. Schenk, B. Liu, and M. E. Brezinski,
“Disper-sion in a grating-based optical delay line for optical coherence to-mography,” Appl. Opt. 42, 4115–4118共2003兲.
56. C. W. Sun, L. S. Lu, C. C. Yang, Y. W. Kiang, and M. J. Su, “Myo-cardial tissue characterization based on the time-resolved Stokes– Mueller formalism,” Opt. Express 10, 1347–1353共2002兲.