INTRODUCTION
Small cell carcinoma (SCC) of the prostate is rare and is thought to behave clinically as a highly aggressive neoplasm [1]
. Early diagnosis of SCC is quite difficult, because of early dissemination, rapid growth, and lack of a concordant elevation in serum PSA levels as with a usual acinar adenocarcinoma of the prostate. These cases usually present at a high stage with multiple bone, lymph node, and visceral organ metastases. Because of the rarity of the condition, no standard therapeutic regimen has been developed.
Gemcitabine,afluorine-substituteddeoxycytidine analog, produced a 27% overall response rate in
previously untreated patients of SCC of the lung [2]. The combination of carboplatin and gemcitabine has recently emerged as a relatively new standard regimen for SCC of the lung [3]. A phase III trial of patients with SCC of the lung and a poor prognosis revealed comparable overall response and median survival rates using the combination of carboplatin and gemcitabine with those of etoposide and cisplatin, but less non-hematologic toxicity was seen[3]
.
We present the clinical and pathologic pictures of 1 case of small cell carcinoma of the prostate. The metastatic bone lesions showed a partial responsetothecombinationofgemcitabineandcarboplatin.
Gemcitabine/Carboplatin Chemotherapy for Pure Small
Cell Carcinoma of the Prostate: A Case Report
Kuan Chou Chen
1Allen W. Chiu
1,2Han-Sun Chiang
1,3Jan-Show Chu
4Chien-Jui Cheng
4,*
Small cell carcinoma of the prostate is rare and is thought to behave clinically as a highly aggressive neoplasm. We report on a patient with pure small cell carcinoma of the prostate presenting as multiple organ metastases. Immunohistochemical studies of the tumor cells revealed positive reactions to chromogranin A, synaptophysin, and cytokeratin stains, and a negative reaction to PSA stain. This patient received 5 courses of gemcitabine/carboplatin chemotherapy after transurethral resection of the prostate, and the previous metastatic bone lesions showed partial resolution. (FJJM 2005; 3 (1):25-31 )
Key words: chemotherapy, prostate, small cell carcinoma, neuroendocrine, immunohistochemical studies
Department of Urology, Taipei Medical University Hospital, Taipei, Taiwan1
Taipei Municipal Chung Hsiao Hospital, Taipei, Taiwan2
College of Medicine, Fu Jen Catholic University, Taipei, Taiwan3 Department of Pathology, Taipei Medical University Hospital, Taipei,
Taiwan4
Submitted February, 10, 2004; final version accepted March, 2 , 2005 * Correspondence author: [email protected]
CASE REPORT
A 79-year-old man underwent transurethral resection of the prostate (TURP) due to repeated urinary retention. The pathological report revealed pure small cell carcinoma (SCC) of the prostate. The tumor was composed of small- to medium-sized tumor cells with scanty cytoplasm and inconspicuousnucleoli(Fig.1A).Immunohistochemical studies revealed positive reactions to chromogranin A stain (Fig. 1B), synaptophysin stain, and cytokeratin stain, and a negative reaction to PSA stain. No
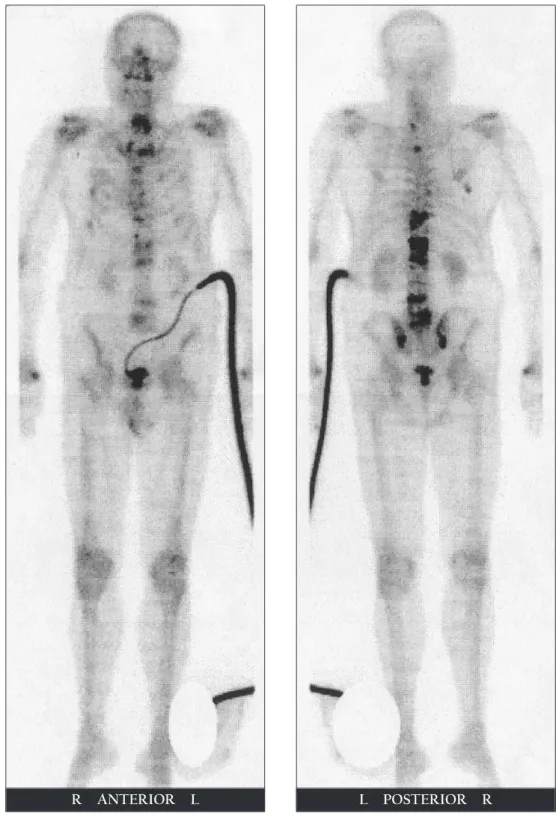
usual acinar adenocarcinoma was seen after all tissues were submitted for a diagnosis. Computed tomography (CT) revealed multiple metastases, including to the liver, spleen, pelvic lymph nodes, and bones. A bone scan demonstrated multiple bone metastases to the ribs, all thoracic and lumbar vertebrae, the sacrum, and bilateral sacroiliac joints (Fig. 2A). After 5 courses of gemcitabine/carboplatin chemotherapy, the previous metastatic bone lesions in the T11, T12, L1, L2, L4, and L5 vertebrae showed partial resolution (Fig. 2B), but the other metastatic lesions remained unchanged. During the 5 courses of chemotherapy, the most-common side effects were a poor appetite, nausea, and vomiting, and these could be well controlled by administration of corticosteroids. Pancytopenia was also noted after every course of chemotherapy, but it was always reversible within 2 weeks. A check of the PSA value was omitted before the TURP, but the PSA value after the final course of chemotherapy was 0.06 ng/ml. He died shortly after the final course of chemotherapy due to sudden cardiac arrest with a survival duration of 7.4 months.
DISCUSSION
Primary SCC is well known in the lung, but SCC of the prostate is a very rare condition, comprising 0.5%~2% of prostate cancers[4]
. These extrapulmonary SCCs are indistinguishable from SCC of the lung by light microscopic, ultrastructural, and immunohistochemical examinations.
Neuroendocrine differentiation of prostate cancer includes pure SCC, carcinoid and carcinoid-liketumors,andaconventionalprostateadenocarcinoma with focal neuroendocrine differentiation[5]. Pure SCC has a more-aggressive clinical course with a dismal prognosis.
SCC of the prostate was proposed to arise from amine precursor uptake decarboxylation
(A)
(B)
Fig. 1 (A) Small- to medium-sized tumor cells with scanty cytoplasm and inconspicuous nucleoli (H&E stain, 400x). (B) Tumor cells reactive to chromogranin A. (ABC stain, 400x).
Fig. 2 (A) Bone scan showing skeletal metastases in the ribs, T1-L5 spine, sacrum,
and both sacroiliac joints.
Fig. 2 (B) Follow-up bone scan revealing partial resolution of the previous metastatic lesions in the T11, T12, L1, L2, L4, and L5.
(APUD) cells of local endodermal origin[6]or from dedifferentiation of prostatic adenocarcinomas [7]. But the most-widely accepted view is that prostatic SCC, similar to lung cancer, arises from totipotential stem cells of the prostate, which have the ability todifferentiateintoeither epithelialor neuroendocrine type carcinomas[8,9]
. This concept is supported by the similarity of the histopathologic pictures and immunohistochemical studies, and by the presence ofsomeparaneoplasticsyndromes.Immunohistochemical studies often show multidirectional differentiation alongepithelial, neuroendocrine, and/or mesenchymal lines of these poorly differentiated prostate cancers [10,11].
In contrast to a prostatic adenocarcinoma, PSA is an unreliable tumor marker for SCC and is usually normal, even when there is metastatic disease.Onestudysuggestedthatthecarcinoembryonic antigen is a more-reliable marker, because increases and decreases in antigen levels are found with disease progression and regression,respectively[9].
SCC of the prostate has a propensity to metastasize to visceral organs, including the liver, bones, lungs, central nervous system, and pericardium, and regionally to pelvic lymph nodes, the rectum, and bladder[9]
.
The small cell lung cancer (SCLC) of prostate cancer has the same unfavorable outcome as other SCC counterparts [12]
. SCC of the prostate has a highly aggressive course and a poor prognosis, with no successful treatment to the present. SCC of the prostate, as distinct from an adenocarcinoma, has been found to be unresponsive to hormone therapy. Despite chemotherapy with different combinations of reagents, the prognosis of SCC is extremely poor, and the median survival is 7 months[13].
The combination of carboplatin and gemcitabine has emerged as a standard regimen for SCC lung cancer[3]
. By combining gemcitabine and carboplatin, we achieved a partial response to the metastatic
bone lesions, but adjustments and modifications of the regimens and dosages are still necessary to achieve a more-effective response.
REFERENCES
1. Bolton DM, Chiu ST, Clarke S, et al. Primary small cell carcinoma of the prostate: unusual modes of presentation. Aust NZ Surg 1994;64:91-94. 2. CormierY,EisenhauerE,MuldalA,etal.Gemcitabine is an active new agent in previously untreated extensive small cell lung cancer (SCLC). A study of the National Cancer Institute of Canada Clinical Trials Group. Ann Oncol 1994;5:283-285. 3. Simon M, Argiris A, Murren JR. Progress in the
therapy of small cell lung cancer. Crit Rev Oncol Hematol. 2004;49:119-133.
4. Helpap B, Kollermann J, Oehler U. Neuroendocrine differentiation in prostatic carcinomas: histogenesis, biology, clinical relevance, and future therapeutical perspectives. Urol Int 1999;62:133-138.
5. di Sant'Agnese PA. Neuroendocrine differentiation in carcinoma of the prostate. Diagnostic, prognostic, andtherapeuticimplications.Cancer1992;70:254-268. 6. di Sant'Agnese PA, Cockett AT. Neuroendocrine differentiation in prostatic malignancy. Cancer 1996;78:357-361.
7. Schron DS, Gipson T, Mendelsohn G. The histogenesis of small cell carcinoma of the prostate. An immunohistochemical study. Cancer 1984;53: 2478-2480.
8. Aygun C. Small cell carcinoma of the prostate: a case report and review of the literature. MD Med J 1997;46:353-356.
9. Rubenstein JH, Katin MJ, Mangano MM et al. Small cell anaplastic carcinoma of the prostate: seven new cases, review of the literature, and discussion of a therapeutic strategy. Am J Clin Oncol 1997;20:376-380.
of the prostate with small cell features: immunohistochemical subtyping and reflections on histogenesis. Virchows Arch 1999;434:385-391. 11. Weaver MG, Abdul-Karim FW, Srigley JR. Paneth cell-like change and small cell carcinoma of the prostate. Two divergent forms of prostatic neuroendocrine differentiation. Am J Surg Pathol 1992;16:1013-1016.
12. Jelbert ME, Russell PJ, Russell P. The biology and management of small cell undifferentiated carcinoma of prostate. In: Williams CJ, Krikarian JG, Green MR, Rayhaven D, eds. Textbook of Uncommon Cancer. London: Wiley; 1998:249-262.
13. Patel A, Ball J, Chappell M. Pure primary small cell carcinoma of the prostate. Br J Urol 1993;72: 380-381.
Gemcitabine 及 Carboplatin 的複合性化學治療
治療單純前列腺小細胞癌
陳冠州
1邱文祥
1,2江漢聲
1,3朱娟秀
4鄭建睿
4,*
前列腺小細胞癌為少見的前列腺惡性疾患。我們報告一位病人為單一細胞型態的 單純小細胞癌,診斷時已合併骨骼及多重器官之轉移。病灶病理切片組織免疫特殊染 色呈現chromogranin A, synaptophysin, and cytokeratins 陽性,及陰性的 PSA 染色。病
人在經尿道前列腺切除手術做出診斷後給予gemcitabine 及 carboplatin 的複合性化學治 療,其骨骼轉移病灶得到部分改善。(輔仁醫學期刊2005;3 (1) :25-31 ) 關鍵詞:攝護腺,小細胞癌,神經內分泌,組織免疫染色 臺北醫學大學附設醫院泌尿科1 臺北市立聯合醫院忠孝院區泌尿科2 私立輔仁大學醫學院3 臺北醫學大學附設醫院病理科4 投搞日期:2005 年 2 月 10 日;接受日期:2005 年 3 月 2 日 * 通訊聯絡作者:電子郵件:[email protected]