Treatment
Horng-Yuan Lou, MD
1,2, Herng-Ching Lin, PhD
3,5, and Kuan-Yang Chen, MD
41Department of Internal Medicine, Division of Gastroenterology, Taipei Medical University Hospital, Taipei, Taiwan;2College of Medicine, Department of Internal Medicine, Taipei Medical University, Taipei, Taiwan;3School of Health Care Administration, Taipei Medical University, Taipei, Taiwan;4Ren-Ai Branch, Department of Internal Medicine, Division of Gastroenterology, Taipei City Hospital, Taipei, Taiwan.
BACKGROUND: No study has explored the volume–
outcome relationship for peptic ulcer treatment.
OBJECTIVE: To investigate the association between
peptic ulcer case volume per hospital, on the one hand,
and in-hospital mortality and 14-day readmission
rates, on the other, using a nationwide
population-based dataset.
DESIGN: A retrospective cross-sectional study, set in
Taiwan.
PARTICIPANTS: There were 48,250 peptic ulcer
patients included. Each patient was assigned to one of
three hospital volume groups: low-volume (≤189 case),
medium volume (190–410 cases), and high volume
(≥411 cases).
MEASUREMENTS: Logistic regression analysis
employ-ing generalized estimatemploy-ing equations was used to
examine the adjusted relationship of hospital volume
with in-hospital mortality and 14-day readmission.
MAIN RESULTS: After adjusting for other factors,
results showed that the likelihood of in-hospital
mor-tality for peptic ulcer patients treated by low-volume
hospitals (mortality rate = 0.68%) was 1.6 times (p<
0.05) that of those treated in high-volume hospitals
(mortality rate = 0.72%) and 1.4 times (p<0.05) that of
those treated in medium-volume hospitals (mortality
rate = 0.73%). The adjusted odds ratio of 14-day
readmission likewise declined with increasing hospital
volume, with the odds of 14-day readmission for those
patients treated by low-volume hospitals being 1.5
times (p<0.001) greater than for high-volume hospitals
and 1.3 times (p<0.01) greater than for medium-volume
hospitals.
CONCLUSIONS: We found that, after adjusting for other
factors, peptic ulcer patients treated in the low-volume
hospitals had inferior clinical outcomes compared to
those treated in medium-volume or high-volume ones.
KEY WORDS: ulcer; volume–outcome; mortality. J Gen Intern Med 23(10):1693–7
DOI: 10.1007/s11606-008-0721-y © Society of General Internal Medicine 2008
INTRODUCTION
Bleeding or perforated peptic ulcers represent a life-threatening condition, accounting for 6500 hospital deaths in the US annually.1With the introduction of proton pump inhibitors
and effective regimens for eradication of Helicobacter pylori, admissions for peptic ulcer-related complications have de-clined; however, there are still some subsets of patients suffering from bleeding or perforated peptic ulcers. Despite advances in medical care and endoscopic therapy, the morbidity and death rate from bleeding or perforated ulcers remains high. The management of bleeding or perforated ulcers requires teamwork, both medical and surgical, as well as experience. For this reason, hospital case volume might be related to outcomes for peptic ulcer disease, but we are not aware of any studies on this issue. As far as we know, there is no study at present dealing with this issue. One study by Freeman et al. reported that lower case volume has been associated with worse outcomes following endoscopic retrograde cholangiopancreato-graphy (ERCP).2Other studies have also reported that
high-volume providers are associated with decreased hospital deaths, shorter lengths of stay and lower hospital charges for complex gastrointestinal surgery.3
The aim of this study is to investigate the association between ulcer case volume per hospital on the one hand and in-hospital mortality and 14-day readmission rates on the other, using a Taiwan nationwide population-based dataset, to clarify the influence of case volume on clinical outcomes.
METHODS
Database
The study used 2004 hospitalization data from Taiwan’s National Health Insurance Research Database (NHIRD), pub-lished by the National Health Research Institute, Taipei, Taiwan. The NHIRD covers all inpatient medical benefit claims for the Taiwanese population of over 21 million individuals (96% of Taiwan’s population), and includes registries of contracted medical facilities and monthly summaries of inpatient claims. Received August 21, 2007
Revised April 22, 2008 Accepted June 25, 2008 Published online July 22, 2008
The NHIRD is one of the largest and most-comprehensive population-based data sources currently available in the world. This dataset provides a unique opportunity to examine the association of hospital ulcer case volume with clinical quality based upon a national database.
Since these were de-identified secondary data released for public access for research purposes, the study was exempt from full review by the Institutional Review Board.
Study Sample
All inpatient claims with a principal diagnosis of ICD-9-CM codes 531.XX to 533.XX from January 2004 to December 2004 were extracted (n=56,610). Of these, 3,354 hospitalizations were excluded because the patients were discharged against medical advice, transferred to another hospital, or had been transferred in from another hospital. In addition, we limited our study sample to the first-time hospitalizations for the treatment of ulcers (meaning no hospitalization for ulcer treatment within one year prior to the index hospitalization). Ultimately, there were 48,250 ulcer patients included in our study.
Hospital Ulcer Case Volume Groupings
Since unique hospital identifiers are in the claims data, we were able to identify the admitting hospital and classify patients by the hospital’s total case volume for ulcer patients during the study period. Each of the 48,250 patients was assigned to one of three hospital volume groups: low volume (≤189 case volume of their admitting hospital), medium volume (190–410 cases), and high volume (≥411 cases). Based on the method used in a literature review by Rudley et al. that posited specific numbers of procedures would be associated with better outcomes,4 we selected a threshold for defining
low-volume hospitals that included all low-volume hospitals showing no statistically significant differences in in-hospital mortality and 14-day readmission. This method allowed us to identify the minimum hospital volume threshold beyond which outcomes significantly improved. Furthermore, the volume thresholds for medium-volume and high-volume hospitals were determined by dividing the sampled patients into two approximately equal-sized groups. The respective volume groups had 13,227, 17,377, and 17,646 cases.
Statistical Analysis
The SAS package (Version 9.0) was used. Outcomes included in-hospital mortality and 14-day readmission for the treatment of peptic ulcer, with patient as the unit of analysis. The key independent variable was hospital volume, measured at hospital level. Chi-square and one-way ANOVA tests were performed to examine the sociodemographic distributions of the sampled patients among hospital case volume groups. A logistic regression analysis employing generalized estimating equations was used to examine the relationship of hospital volume with in-hospital mortality and 14-day readmission, adjusted for hospital and patient characteristics, including patient severity (clinical severity and co-morbidities), as well as clustering of patients within hospital panels (hospital-level random effect).
The hospitals’ accreditation level, ownership (public, for-profit and not-for-for-profit) and geographic location, patient
demographics (age and gender) and patient severity were included in the regression model. Since there was a high co-linearity between hospitals’ accreditation level and hospital volume group, hospitals’ accreditation level was not included. However, we still analyzed the medium-volume and high-volume groups for medical centers and the medium-high-volume and low-volume groups for district hospitals, to see if there was a volume effect. Patient severity was comprised of ulcer severity (the presence or absence of hemorrhage or perforation) and the presence of co-morbidities. Clinical co-morbidities were measured using the Charlson comorbidity index (CCI), A two-sided p-value of 0.05 was used.
RESULTS
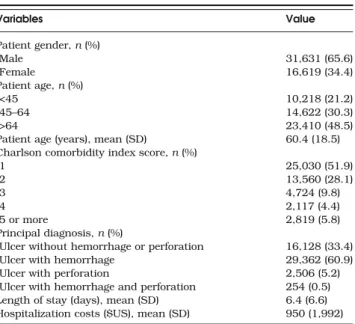
Table1describes the demographic characteristics and princi-pal diagnosis types among the 48,250 inpatients admitted for the treatment of ulcers. Mean length of stay was 6.4 days, the mean cost per discharge was US $950; 65.6% were male, 5.8% had Charlson scores≥ 5, and 33.4% had a principal diagnosis of ulcer without hemorrhage or perforation.
The characteristics of the hospitals and the patients, stratified by hospital volume, are presented in Table 2. The 385 hospitals admitted a mean of 412 ulcer patients per hospital in 2004. The vast majority of the hospitals (77.1%) fell into the low-volume group, with virtually none of the hospitals in this group being medical centers. In addition, all high-volume hospitals were teaching hospitals.
There were significant relationships between hospital volume groups and patient age, CCI, ulcer severity and the rate of endoscopic treatment (all p<0.001), but not gender. Patients treated by high-volume hospitals were more likely to be younger, CCI≥ 5 and had a principal diagnosis of ulcer with perforation.
The 14-day readmission rates decreased with increasing hospital volume; they were 2.66%, 2.15% and 1.80% for LVH, MVH and HVH, respectively. The in-hospital mortality rates
Table 1. Characteristics of Patients Admitted for Ulcer Treatments in Taiwan in 2004 (n=48,250) Variables Value Patient gender, n (%) Male 31,631 (65.6) Female 16,619 (34.4) Patient age, n (%) <45 10,218 (21.2) 45–64 14,622 (30.3) >64 23,410 (48.5)
Patient age (years), mean (SD) 60.4 (18.5)
Charlson comorbidity index score, n (%)
1 25,030 (51.9) 2 13,560 (28.1) 3 4,724 (9.8) 4 2,117 (4.4) 5 or more 2,819 (5.8) Principal diagnosis, n (%)
Ulcer without hemorrhage or perforation 16,128 (33.4)
Ulcer with hemorrhage 29,362 (60.9)
Ulcer with perforation 2,506 (5.2)
Ulcer with hemorrhage and perforation 254 (0.5)
Length of stay (days), mean (SD) 6.4 (6.6)
Hospitalization costs ($US), mean (SD) 950 (1,992) Note: * Total patient sample = 48,250
were 0.77%, 0.68% and 0.67% for low, medium, and high-volume hospitals, respectively. Mortality rates for patients with and without endoscopy were 0.39% and 1.09%, respectively, while 14-day readmission rates for patients with and without endoscopy were 1.59% and 2.84%, respectively.
The adjusted odds ratios for in-hospital mortality and 14-day readmission according to hospital ulcer volume groups are shown in Table 3. After adjusting for patients’ demographic characteristics, clinical severity of the ulcer and presence of comorbidities, the likelihood of in-hospital mortality for ulcer patients treated by low-volume hospitals was 1.6 times (p<0.05) that of patients treated in high-volume hospitals and 1.5 times (p<0.05) that of patients treated in medium-volume hospitals. As expected, the odds of in-hospital mortality increased with patients’ age and the Charlson score level. In hospital mortality for patients with both hemorrhage and perforation was markedly
higher relative to patients without these complications—a 25-fold difference.
The adjusted odds ratio of 14-day readmission also declined with increasing hospital volume, with odds of 14-day readmis-sion being 1.4 times (p<0.001) greater at low-volume than high-volume hospitals, and 1.3 times (p<0.01) greater at low-volume than at medium-low-volume hospitals.
DISCUSSION
This is the first nationwide population-based study to explore the volume–outcome relationship for peptic ulcer treatment. In our study, we found that after adjusting for patients’ demo-graphic characteristics, severity of disease and clinical comor-bidities, peptic ulcer patients treated in high-volume or Table 2. Hospital and Patient Characteristics by Hospital Ulcer Volume Groups in Taiwan in 2004
Variable Low (1–189) Medium (190–410) High (≥411) P-value
No. % No. % No. %
Hospital ulcer volume group (n=385 hospitals) Hospital characteristics
Total No. of hospitals 297 77.1 62 16.1 26 6.8
Hospital ulcer volume mean, (SD) 44.5 (49.2) 280.3 (55.7) 678.7 (248.4) <0.001
Hospital level – Medical center – – 7 11.3 10 38.5 Regional hospital 18 6.1 38 61.3 15 57.7 District hospital 279 93.9 17 27.4 1 3.9 Teaching status – Yes 47 15.8 53 85.5 26 100 No 250 84.2 9 14.5 – – Hospital ownership <0.001 Public 51 17.2 24 38.7 6 23.1 Private not-for-profit 32 10.8 25 40.3 13 50.0 Private for-profit 214 72.1 13 21.0 7 26.9 Geographic location – Northern 87 29.3 26 41.9 8 30.8 Central 83 28.0 16 25.8 7 26.9 Southern 115 38.7 16 25.8 11 42.3 Eastern 12 4.0 4 6.5 – – Patient characteristics
Total No. of patients 13,227 27.4 17,377 36.0 17,646 36.6
Age of patients, mean, SD 61.8 (17.9) 60.6 (18.3) 59.0 (19.0) <0.001
Patient gender 0.520 Male 8,638 65.3 11,448 65.9 11,545 65.4 Female 4,589 34.7 5,929 34.1 6,101 34.6 Patient age <0.001 <45 2,621 19.8 3,562 20.5 4,035 22.9 45–64 3,908 29.6 5,259 30.3 5,455 30.9 >64 6,698 50.6 8,556 49.2 8,156 46.2
Hospital ulcer volume group (n=48,250 patients) Patient characteristics
Charlson comorbidity index score <0.001
1 7,009 53.0 9,010 51.9 9,011 51.1 2 3,727 28.2 4,852 27.9 4,981 28.3 3 1,335 10.1 1,702 9.8 1,687 9.6 4 607 4.6 775 4.5 735 4.2 5 or more 549 4.2 1,038 6.0 1,232 7.0 Principal diagnosis <0.001
Ulcer without hemorrhage or perforation 4,552 34.4 5,390 31.0 6,186 35.1
Ulcer with hemorrhage 8,261 62.5 10,913 62.8 10,188 57.7
Ulcer with perforation 333 2.5 990 5.7 1,183 6.7
Ulcer with hemorrhage and perforation 81 0.6 84 0.5 89 0.5
Endoscopic treatment <0.001
Yes 6,502 49.2 9,826 56.6 9,947 56.4
No 6,725 50.8 7,551 43.5 7,699 43.6
medium-volume hospitals had lower in-hospital mortality than those treated in the low-volume hospitals. Similarly, the odds of 14-day readmission decreased with increasing hospital case volume. Our study results echo volume–outcome relation-ships reported by others, which consistently found inferior clinical outcomes associated with low provider volume for a variety of surgical procedures.5–9This implies that if patients
with peptic ulcers are treated at higher-volume hospitals, better outcomes would be obtained.
One potential explanation for our findings is the“practice makes perfect” hypothesis-that a larger volume of patients enables hospitals to attain more experience caring for certain types of patients, and this enhanced experience accounts for improved outcomes. According to this hypothesis, low-volume hospitals with poor outcomes can improve their clinical performance by increasing patient volume. How many patients
is enough? We found a significant decrease in in-hospital mortality rate and 14-day readmission rate when the annual volume of ulcer patients exceeded 190. Additional increases in volume were not associated with further improvement in outcomes. Unfortunately, simply recommending that hospitals increase their case volume may have adverse effects. To reach a higher volume target, low-volume hospitals may be tempted to artificially lower the entry criteria for ulcer hospitalization.
How might higher volumes translate into decreased mortal-ity? In our study, we found that the use of endoscopic treatment was associated with decreased in-hospital mortality rate and 14-day readmission, but that this did not account for all the benefit of higher volume. The benefits of endoscopy to stabilize bleeding from peptic ulcers have been fully demon-strated.10The success of endoscopic treatment also depends
on the location of the ulcer, the clinical condition of the patient and the techniques that the endoscopist is most familiar with. It may be that higher-volume hospitals, which are generally better equipped, are more likely to meet most endoscopists’ needs by making different endoscopic hemostasis tools avail-able, thereby increasing the rate of achieving successful hemostasis. Moreover, endoscopists in higher-volume hospi-tals more frequently encounter “difficult” cases and thereby gain greater experience.
Furthermore, higher-volume hospitals usually employ more endoscopists, and are more likely to provide early endoscopy (i.e. within 24 hours of admission). Although the benefit of early endoscopy for upper gastrointestinal tract hemorrhage is not entirely established, patients may benefit from prompt diagnosis, severity stratification and most importantly, im-proved hemostasis, which profoundly reduces the chance of rebleeding and the need for surgery.11,12
Differences in surgical expertise might also explain some of the benefit of volume. Perforated ulcers almost inevitably require surgical intervention. Delayed surgical treatment can result in sepsis and death. Previous investigations confirm the link between greater case volume and better surgical outcomes in a variety of procedures.3Surgical treatment involving bleeding or
perforated ulcers is usually carried out in emergency conditions, and it demands more critical care experience than other elective surgeries. Higher-volume hospitals may be more apt to possess specialized staff, equipment, and experienced surgeons.
A couple of limitations of this study arise mainly from the nature of the administrative data used. Firstly, although we adjusted for patient comorbidities and the presence of hemor-rhage or perforation, we had limited ability to account for differences in ulcer severity. However, studies by Tu et al. and Jones et al. have demonstrated that a relatively small number of clinical variables are sufficient to enable a fair comparison of risk-adjusted mortality rates across hospitals.13,14 Secondly,
peptic ulcer patients are only admitted for treatment in hospitals when their condition is severe enough, and the entry criteria may vary among hospitals. It is possible that hospitals that admit only the most severe cases are more likely to have greater numbers of in-hospital case mortalities vis-à-vis other hospitals admitting a greater proportion of patients with less severe conditions.
In summary, we found that after adjusting for patients’ demographic characteristics, severity of disease and clinical comorbidities, ulcer patients treated in hospitals with fewer than 190 ulcer cases per year had inferior clinical outcomes compared to those at other hospitals. Although endoscopy may Table 3. Adjusted Odds Ratios for In-hospital Mortality and 14-day
Readmission, by Hospital Ulcer Volume Groups and the Characteristics of the Hospital and Paatient
Variables In-hospital mortality 14-day readmission Adjusted ORa
(95% CI)
Adjusted ORa (95% CI) Hospital ulcer volume
≤189 1.000 1.000 190–410 0.647*(0.451–0.927) 0.798**(0.682–0.935) ≥411 0.625*(0.410–0.952) 0.695***(0.589–0.821) Hospital ownership Public 1.234 (0.887–1.718) 1.205* (1.027–1.414) Private not-for-profit 0.590** (0.412–0.845) 0.898 (0.757–1.065) Private for-profit 1.000 1.000 Geographic location Northern 1.000 1.000 Central 0.421*** (0.304–0.583) 1.195* (1.023–1.396) Southern 0.624*** (0.481–0.811) 0.858 (0.731–1.007) Eastern 0.920 (0.530–1.597) 0.708 (0.487–1.030) Patient gender Male 1.000 1.000 Female 1.283* (1.006–1.635) 1.073 (0.940–1.226) Charlson comorbidity index score 1 1.000 1.000 2 1.127 (0.848–1.500) 0.947 (0.815–1.100) 3 1.673** (1.174–2.385) 1.094 (0.887–1.349) 4 2.297*** (1.521–3.467) 1.169 (0.881–1.551) 5 or more 3.836*** (2.722–5.406) 1.082 (0.823–1.422) Patient age <45 1.000 1.000 45–64 2.624*** (1.508–4.568) 1.043 (0.860–1.265) >64 6.573*** (3.912–11.042) 1.444*** (1.212–1.721) Endoscopic treatment Yes 0.538***(0.417–0.694) 0.624*** (0.547–0.712) Principal diagnosis Ulcer without hemorrhage or perforation 1.000 1.000 Ulcer with hemorrhage 3.263*** (2.176–4.892) 1.177* (1.019–1.359) Ulcer with perforation 17.538*** (11.037–27.868) 1.926*** (1.499–2.474) Ulcer with hemorrhage and perforation 25.464*** (13.370–48.499) 2.555*** (1.464–4.460) Note: *p<0.05; **p<0.01; ***p<0.001
Adjusted for patient’s gender, age, Charlson Comorbidity Index score, endoscopic treatment, principal diagnosis, hospital ownership, geograph-ic location and hospital random effect
play a role, the exact explanation for better outcomes could not be identified from our data. Further investigations should be undertaken to identify the clinical approaches and techniques among endoscopists and surgeons in high-volume hospitals that result in superior outcomes; the results of such studies could help lower-volume hospitals to improve the quality of their patient care.
Conflict of Interest: None disclosed.
Corresponding Author: Herng-Ching Lin, PhD; School of Health Care Administration, Taipei Medical University, 250 Wu-Hsing St., Taipei 110, Taiwan (e-mail: [email protected]).
REFERENCES
1. Sonnenberg A. Peptic ulcer. In: Everhart, JE, eds. Digestive diseases in the United States: epidemiology and impact. Washington, DC: US Department of Health and Human Services, Public Health Service, National Institutes of Health; 1994:359–408NIH publication no. 94–1447.
2. Freeman ML. Adverse outcomes of endoscopic retrograde cholangio-pancreatography: Avoidance and management. Gastrointest Endosc Clin N Am. 2003;13:775–98.
3. Gordon TA, Bowman HM, Bass EB, et al. Complex gastrointestinal surgery: impact of provider experience on clinical and economic out-comes. J Am Coll Surg. 1999;189:46–56.
4. Dudley RA, Johansen KL, Brand R, et al. Selective referral to high-volume hospitals: estimating potentially avoidable deaths. JAMA. 2000;283:1159–66.
5. Jollis JG, Peterson ED, DeLong ER, et al. The relation between the volume of coronary angioplasty procedures at hospitals treating Medi-care beneficiaries and short-term mortality. N Engl J Med. 1994;334: 1625–9.
6. Jollis JG, Peterson ED, Nelson CL, et al. Relationship between physician and hospital coronary angioplasty volume and outcome in elderly patients. Circulation. 1997;95:2485–91.
7. Hannan EL, Racz M, Ryan TJ, et al. Coronary angioplasty volume– outcome relationships for hospitals and cardiologists. JAMA. 1997;277: 892–8.
8. McGrath PD, Wennberg ED, Dickens JD, et al. Relation between operator and hospital volume and outcomes following percutaneous coronary interventions in the era of the coronary stent. JAMA. 2000;284:3139–44.
9. Varadarajulu S, Kilgore ML, Wilcox CM, et al. Relationship among hospital ERCP volume, length of stay, and technical outcomes. Gastro-intest Endosc. 2006;64:338–47.
10. Sacks HS, Chalmers TC, Blum AL, et al. Endoscopic hemostasis. An effective therapy for bleeding peptic ulcers. JAMA. 1990;264:494–9. 11. Cooper GS, Chak A, Connors AF, et al. The effectiveness of early
endoscopy for upper gastrointestinal hemorrhage. Med Care. 1998;36: 462–74.
12. Cooper GS, Chak A, Way L, et al. Early endoscopy in upper gastroin-testinal hemorrhage: association with recurrent bleeding, surgery, and length of hospital stay. Gastrointest Endosc. 1999;49:145–52. 13. Tu JV, Sykora K, Naylor CD. Assessing the outcomes of coronary artery
bypass graft surgery: how many risk factors are enough? Steering Committee of the Cardiac Care Network of Ontario. J Am Coll Cardiol. 1997;30:1317–23.
14. Jones RH, Hannan EL, Hammermeister KE, et al. Identification of preoperative variables needed for risk adjustment of short-term mortality after coronary artery bypass graft surgery. The Working Group Panel on the Cooperative CABG Database Project. J Am Coll Cardiol. 1996;28: 1478–87.