異常的PDGFR-α基因表現對誘發甲狀腺濾泡癌癌化之探討
127
0
0
全文
(2) 異常的 PDGFR-α基因表現 對誘發甲狀腺濾泡癌癌化之探討 The significance of aberrant gene expression of PDGFR-α in the carcinogenesis of follicular thyroid carcinoma. 研 究 生 : 陳 桂 添 指導教授 : 張 正 詹 爾 昌. Student: Kuei-Tien Chen Advisor: C. Allen Chang Err-Cheng Chan. 國 立 交 通 大 學 生 物 科 技 研 究 所 博 士 論 文. A Thesis Submitted to Department of Biological Science and Technology College of Biological Science and Technology National Chiao Tung University in partial Fulfillment of the Requirements for the Degree of Ph. D. in Biological Science and Technology May 2005 Hsinchu, Taiwan, Republic of China. 中華民國 九十四 年 五 月.
(3) 中文摘要: 甲狀腺腫瘤約佔所有腫瘤的 1%。腫瘤會發生在所有的年齡層,而且會隨著年齡的 增加發生率也會增加。女性與男性罹患的比率約 3:1。目前,確定可行的診斷方式,是 藉著組織學的觀察。但臨床上發現,有些早期的吸引性細胞學檢查,有時是不可信賴的, 特別是針對濾泡型的甲狀腺腫瘤。通常濾泡型腫瘤或較少數的乳突型腫瘤,病理學家無 法僅以吸引性細胞學檢查的結果,做出正確的診斷。 為了發展可以早期偵測的分子標的,我們首先藉著描繪出在不同的甲狀腺腫瘤組織 與細胞株的表現具有差異的基因,從其中尋找具有潛力的腫瘤標的基因。cDNA 表現基 因陣列(cDNA expression array)的技術,在本研究中用來描繪出在甲狀腺濾泡癌中,差別 表現的基因,以顯現適合的腫瘤標誌。針對在濾泡型的甲狀腺腫瘤,表現具有差異的基 因,進行進一步的研究,將有助於瞭解,這些基因改變在甲狀腺腫瘤癌化過程中,所扮 演的角色。 在利用了 cDNA 表現基因陣列的技術分析差別表現基因過後,我們發現 PDGF-A 與 PDGFR-α 的 mRNA 相較於良性的結節性增生細胞(nodular hyperplasia cells)而言,在甲 狀腺濾泡癌細胞株中,具有高度表現。因此,這些結果引起我們的動機,想瞭解是否具 有 PDGF 相關的自分泌活化(autocrine activation)的現象,存在甲狀腺腫瘤細胞中且在癌 化過程中,扮演重要角色。PDGFR 本身具有激脢活性(kinase activity),當 PDGF 配位蛋 白(ligand)結合上受體蛋白(receptor)時,可活化位於細胞內激脢活性。已知 PDGFR 活化 與一些細胞的癌化,具有相關性,包含星狀細胞瘤(astrocytomas),寡樹突神經膠質瘤 (oligodendrogliomas),及神經膠質胚胎細胞瘤(glioblastoma)。在 cDNA 表現基因陣列的分 析,我們發現在濾泡癌細胞中,PDGF-A 與 PDGFR-α 之 mRNA,皆會增加表現。之後, 利用西方墨點法分析,確認在濾泡癌細胞中,PDGF-A 與 PDGFR-α 蛋白,也會提升表 現。更進一步,觀察 PDGFR-α 的磷酸化現象,發現利用針對第 720 位置的酪胺酸磷酸 化專一性抗體,在濾泡癌細胞中,可偵測到磷酸化現象。而 PDGFR-α 所具有的酪胺酸 激脢活性,可以被抑制劑 tyrphostin AG1295 所抑制,而且顯現隨著抑制劑劑量的增加,. i.
(4) 而提升抑制腫瘤細胞增生的作用。另一方面,在免疫組織呈色實驗(immunohistochemistry) 中,結果顯示 PDGFR-α 蛋白的表現,主要是呈現在甲狀腺濾泡周邊(thyroid follicle )且 是與惡性的腫瘤階段(tumor stage),呈現統計上的相關性。這些發現暗示,藉著 PDGFR-α 所進行的自分泌活化現象,在甲狀腺細胞的癌化過程中,扮演重要的角色。 進一步為了確認是否能藉著抑制這不正常的訊息傳遞,能夠達到解除癌化的可能 性。我們檢驗 PDGFR-α siRNA 與 tyrphostin AG1295,這兩種方式,來觀察對抑制 CGTH W-1 細胞增生的功效。目前,已知有數種酪胺酸激脢抑制劑,可以阻擋具酪胺酸激脢活 性的受體之訊息傳遞,從而抑制不正常的訊息傳遞。這裡我們設計小而具有干擾特性的 RNA (short interfering RNAs; siRNA)專門針對 PDGFR-α 基因,且達到壓制濾泡型的甲狀 腺腫瘤細胞(CGTH W-1)增生的效果。即時定量聚合脢連鎖反應(real-time quantitative PCR)、流式細胞儀(flow cytometry)測定、免疫螢光細胞染色(immunofluorescence cell staining)及 MTT 測定後,結果顯示送入 PDGFR-α siRNA 的 CGTH W-1 細胞,可達到減 少細胞中 PDGFR-α mRNA 的表現程度。之後,可以達到減少 CGTH W-1 細胞表面受體 的分子數目及最後可以達到抑制細胞增生的效果。而利用 non-silencing siRNA 所進行的 對照組實驗,則不管在 PDGFR-α 基因的表現或者是細胞增生,皆無顯著影響。 最後,我們比較利用 PDGFR-α siRNA 與 tyrphostin AG1295,在抑制 CGTH W-1 細胞增生的影響,發現利用 PDGFR-α siRNA 時,功效的呈現,相對於 tyrphostin AG1295,需要多 24 小時的時間,才能達到顯著的效果;但是它的作用可以達到 240 小時 (第十天)之久。這些發現指示了 PDGFR-α siRNA 可以是一個有潛力的工具,來抑制不正 常的 PDGFR-α 基因表現。另外也進一步的證明,在甲狀腺細胞癌化過程中,PDGFR-α 基因的表現,扮演重要的角色。. ii.
(5) Abstract:. Thyroid cancer accounts for about 1% of all cancers. Thyroid cancer occurs at all ages and increases frequently in each decade. The female:male ratio is about 3:1. Definite diagnosis is possible only by histological examination. Fine needle aspiration cytology (FNAC) reports are sometime unreliable, especially for follicular thyroid tumors. Frequently, the pathologist cannot diagnose follicular carcinoma on FNAC or (to a lesser extent) papillary carcinoma. To develop an early detection method by using biological markers, we have first searched the potent tumor markers by outline the differentially gene expressions in various thyroid tissues or thyroid cell lines. The cDNA expression array technology is utilized herein to profile differentially expressed genes from human follicular thyroid carcinoma and reveals new tumor markers. An expression profile of genes that are associated with malignant process of follicular thyroid cancer was further discussed. Further investigation is required to understand the precise relationship between the altered expression of these genes and the malignant process of follicular thyroid cancer. After analysis of differentially gene expression by a cDNA microarray technique, we found that mRNA of PDGF-A and PDGFR-α were highly expressed in thyroid carcinomas but not in nodular hyperplasia cells. These results cause the motive to understand whether PDGF autocrine activation exists in thyroid cells and play a crucial role in carcinogenesis. Platelet-derived growth factor receptor (PDGFR) possesses a kinase activity and can be activated through binding with PDGF.. The activation of PDGFR is associated with the. carcinogenesis of some cell types, including astrocytomas, oligodendrogliomas, and glioblastoma.. In a cDNA microarray analysis, we discovered the over-expressed mRNA of. both PDGF-A and PDGF α-receptor in thyroid carcinoma cells.. And the elevated protein. expressions of PDGF-A and PDGF α-receptor in thyroid carcinoma cells were confirmed by a iii.
(6) western blot analysis. Furthermore, the phosphorylation of PDGF α-receptor measured by an antibody against Tyr 720-phosphate was found in thyroid carcinoma cells. The tyrosine kinase activity of PDGF α-receptor was inhibited by tyrphostin AG1295 and showed a dose-dependent inhibition for cell proliferation.. In an immunohistochemistry study, data. showed that the expression of PDGF α-receptor was primarily localized around the follicle and significantly correlated with malignant tumor stage. These findings imply that autocrine activation of PDGF-α receptor plays a crucial role in the carcinogenesis of thyroid cells. To identify whether inhibition of the aberrant signal transduction could have the potential to dismiss the possibility of carcinogenesis, we examined the efficacy of PDGFR-α siRNA and tyrphostin AG1295 on repressing cell proliferation of follicular thyroid carcinoma cell line (CGTH W-1). Some tyrosine kinase inhibitors have shown to block the tyrosine-like receptors and achieve the inhibition of some aberrant signal transduction. Here we designed short interfering RNAs (siRNA) specific for PDGFR-α to repress cell proliferation in CGTH W-1. Real-time quantitative PCR, flow cytometry, immunofluorescence cell staining, and MTT assay results demonstrated that the transfected CGTH W-1 cells reduce the cellular PDGFR-α mRNA level, reduce the PDGF α-receptor in cell membrane, and repress cell proliferation. While control studies of non-silencing siRNA showed no significant effects in PDGFR-α expression and cell proliferation. Finally, we compared the effects of repressing cell proliferation of CGTH W-1 cells by PDGFR-α siRNA and a tyrosine kinase inhibitor, tyrphostin AG1295. PDGFR-α siRNA required 24 hours more than tyrphostin AG1295 to show significant inhibition of cell proliferation, but the effects last up to 240 hours. The findings indicate that the PDGFR-α siRNA could be a potential tool to suppress aberrant PDGFR-α gene expression and furthermore show that PDGF-α receptor plays a crucial role in the carcinogenesis of thyroid cells.. iv.
(7) Acknowledgements. I would like to convey my gratitude to the following, for their guidance and assistance during the period of my Ph. D. degree. Professor C. Allen Chang and Err-Cheng Chan, for their encouragements, ideas, constructive criticisms and discussions. The committee members: Simon J.T. Mao, Ph.D., C. Allen Chang, Ph.D., Err-Cheng Chan, Ph.D., Hwei-Ling Peng, Ph.D., Hsien-Tai Chiu, Ph.D., Chia-Rui Shen, Ph.D., for their understandings and suggestions. Dr. Err-Cheng Chan and the staff at Medical Biotechnology Lab., Graduate Institute of Medical Biotechnology, Chang Gung University, for their true friendship. My parents and families, for helping me to get where I am today.. Kuei-Tien Chen 2005. v.
(8) Contents 中文摘要……………………………………………….……………………….................. i Abstract………………………………………………………………………..…………... iii Acknowledgements………………………………………………………………………….v Contents………………………………………………...………………………………...…vi List of tables………………………………………………………………………..……… viii List of figures………………………………………………………………………………. ix I. Introduction …………………………………………………………………...………... 1 1.1 Common Thyroid Disorders……………………………………………………..… 1 1.2 Incidence and distribution of thyroid cancer…………………………………….… 1.3 Pathology……………………………………………………………………....…. 1.4 Causes of Thyroid Carcinoma………………………………………………….… 1.5 Oncogenes in thyroid tumors……………………………………..………………. 1.6 Follicular thyroid carcinoma………………………………………………..……... 2 3 5 5 8. 1.7 Hurthle cell tumors……………………………………………………………..…. 9 1.8 Papillary thyroid carcinoma…………………………………………………..…… 10 1.9 The prognosis of thyroid cancer………………………………………………….... 12 1.10 Chemotherapy…………………………………………………………….………. 13 II. Specific aims…………………………………………………………………………. 14 Part I. Identifying differentially expressed genes associated with malignance of thyroid cancer by complementary DNA expression array I. Abstract ………………………………………………………………………………… 16 II. Introduction ………………………………………………………………………...…. 18 III. Materials and Methods……………………………………………………………...… 20 IV. Results………………………………………………………………………...……….. 24 V. Discussion………………………………………………………………………...……..26 Part 2. An aberrant autocrine activation of the platelet-derived growth factor α-receptor in follicular and papillary thyroid carcinoma cell lines I. Abstract………………………………………………………………………………….29 II. Introduction……………………………………………………………………………..30 III. Materials and methods…………………………………………………………………32 IV. Results…………………………………………………………………………...……..37 V. Discussion………………………………………………………………………..……...40. vi.
(9) Part 3. Up-regulation of platelet-derived growth factor α-receptor expression in follicular thyroid carcinoma correlates with malignant tumor stage I. Abstract…………………………………………………………………………….……44 II. Introduction……………………………………………………………………….…….45 III. Materials and methods…………………………………………………………………47 IV. Results………………………………………………………………………………….50 V. Discussion………………………………………………………………………….........52 Part 4. Repression of proliferation in follicular thyroid carcinoma cell line by siRNA –mediated silencing of the PDGFR-α gene I. Abstract……………………………………………………………………………...…..54 II. Introduction…………………………………………………………….…………..…...55 III. Materials and methods………………………………………………………..……..…57 IV. Results…………………………………………………………………………..…..….62 V. Discussion………………………………………………………………………..…..….66 Summary…………………………………………………………………………………..71 References Part of introduction…………………………………………………….……………….78 Part 1……………………………………………………………………………………85 Part 2……………………………………………………………………………………89 Part 3……………………………………………………………………………………95 Part 4……………………………………………………………………………………99 Tables……………………………………………………………………………………..106 Figures……………………………………………………….……………………………116. vii.
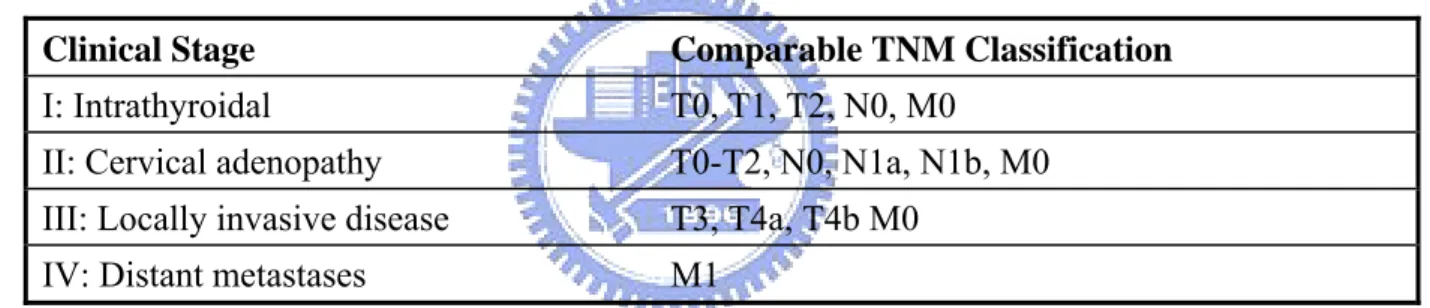
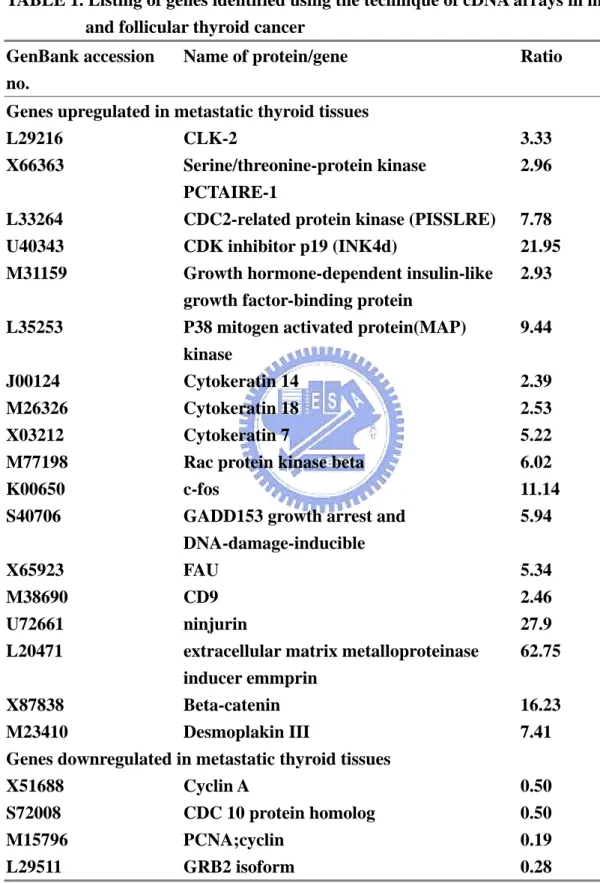
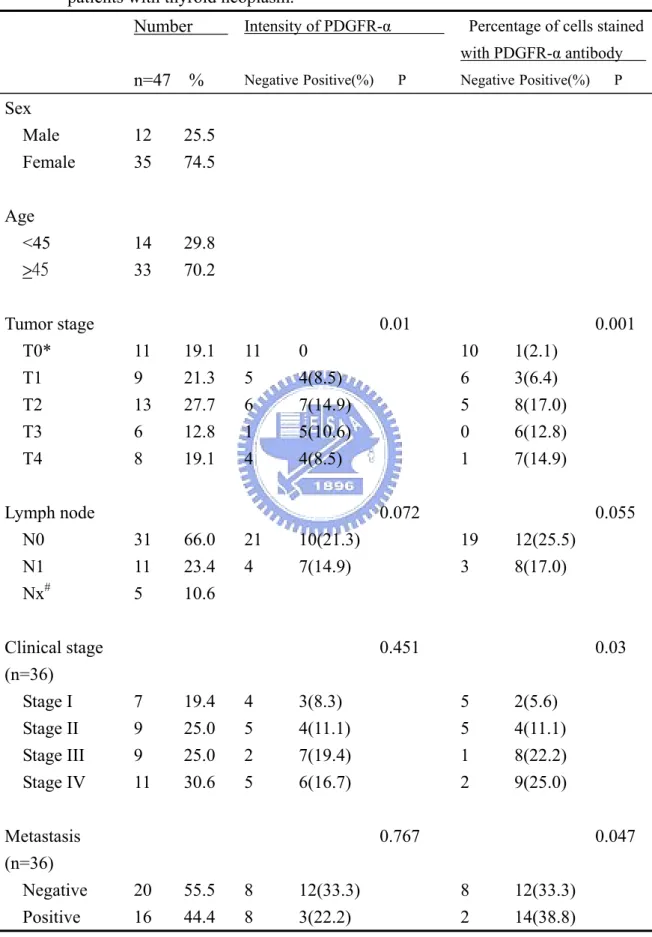
(10) List of Tables Part of introduction Table 1. TNM Clinical Classification of Thyroid Cancer………………….….… 106 Table 2. Comparison of Two Clinical Staging Systems………………….……….107 Part I. Identifying differentially expressed genes associated with malignance of thyroid cancer by complementary DNA expression array Table 1. Listing of genes identified using the technique of cDNA arrays in metastatic and follicular thyroid cancer……………………………….108 Table 2. A list of differentially expressed genes identified by using a cDNA array technique in the ratio of follicular thyroid carcinoma cell line to benign tissue (F/B ratio), together with the ratio of papillary thyroid carcinoma cell line to benign tissue (P/B ratio)…………………111 Part 3. Up-regulation of platelet-derived growth factor α-receptor expression in follicular thyroid carcinoma correlates with malignant tumor stage Table 1. Correlation between PDGFR-α expression and clinicopathological parameters in 47 patients with thyroid neoplasm………………………... 115. viii.
(11) List of Figures Part of introduction Figure 1. Possible role of oncogene activation, receptor, G-protein mutation, or tumor supressor gene deletion in the induction of thyroid carcinoma………………………………………………………… 116 Figure 2. The detection methods of thyroid cancer…………………………………. 117 Figure 3. The proposal of studying the PDGFR-α mechanism in thyroid carcinogenesis……………………………………………………. 118 Part I. Identifying differentially expressed genes associated with malignance of thyroid cancer by complementary DNA expression array Figure 1. The quality of total RNA isolated from primary and metastatic follicular thyroid carcinoma………………………………………….…... 119 Figure 2. The procedure of cDNA array experiment in metastatic and primary follicular thyroid carcinoma……………………………………………… 120 Figure 3. Expression pattern of genes in follicular thyroid carcinoma and its pair metastatic tissue……………………………………………………121 Figure 4. Reverse transcription-polymerase chain reaction substantiating the consistency of the cDNA array results………………………………...122 Figure 5. The quality of total RNA isolated from tissue derived from nodular hyperplasia, follicular thyroid carcinoma cell line (CGTH W-1) and papillary thyroid carcinoma cell line (CGTH W-3)………………..… 123 Figure 6. The procedure of cDNA array experiment in nodular hyperplasia (benign tissue), follicular thyroid carcinoma cell line (CGTH W-1) and papillary thyroid carcinoma cell line (CGTH W-3)…………………...124 Figure 7. Expression pattern of genes in follicular thyroid carcinoma cell line, papillary carcinoma cell line and nodular hyperplasia………………….…125 Figure 8. Reverse transcription-polymerase chain reaction confirming the results of the cDNA array…………………………………………………………126 Part 2. An aberrant autocrine activation of the platelet-derived growth factor α-receptor in follicular and papillary thyroid carcinoma cell lines Figure 1. The list of intensity obtained from gene expressions of human cDNA expression arrays under the thyroid carcinoma cell lines and nodular hyperplasia……………………………………………………..127 Figure 2. Expression pattern of genes in follicular thyroid carcinoma cell line, papillary thyroid carcinoma cell line, and nodular hyperplasia……128 ix.
(12) Figure 3. Quantitative PCR reconfirm the tendency towards up-regulation expression of PDGF-A and PDGFR-α in CGTH W-1 and CGTH W-3 cell lines…………………………………………………….129 Figure 4. Detection of PDGF-A and PDGFR-α by western blotting……………….130 Figure 5. Detection of phosphorylated PDGFR-α with immunoprecipitaion followed by western blotting……………………………………………..131 Figure 6. Effects of Tyrphostin A1 (AG9) and Tyrphostin AG1295 on proliferation of CGTH W-1 and CGTH W-3 cell lines…………………………..……132 Part 3. Up-regulation of platelet-derived growth factor α-receptor expression in follicular thyroid carcinoma correlates with malignant tumor stage Figure 1. Immunohistochemical detection of PDGFR-α…………………………....133 Figure 2. Immunofluorescence cell staining of PDGFR-α in follicular thyroid cell line(CGTH W-1)…………………………………………………..…134 Part 4. Repression of proliferation in follicular thyroid carcinoma cell line by siRNA –mediated silencing of the PDGFR-α gene Figure 1. Schematic representation of PDGFR-α siRNA and control siRNA…...….135 Figure 2. PDGFR-α siRNA leads to promote cleavage of the cellular PDGFR-α Mrna………………………………………………………..…136 Figure 3. PDGFR-α siRNA reduce the PDGFR-α protein expression………..…….138 Figure 4. Immunofluorescence localization of PDGFR-α in CGTH W-1 cells…..…139 Figure 5.The inhibition efficacy of tyrphostin AG1295 and PDGFR-α siRNA on thyroid follicular carcinoma cell………………………………………140 Figure 6.CGTH W-1 cell growth suppressed by PDGFR-α siRNA and tyrphostin AG1295…………………………………………………...141. x.
(13) I. INTRODUCTION. The thyroid gland is the biggest gland in the neck and situated in the anterior neck below the skin and muscle layers. The thyroid gland takes the shape of a butterfly with the two wings being represented by the left and right thyroid lobes which wrap around the trachea. The function of the thyroid is to make thyroid hormone. This hormone has an effect on nearly all tissues of the body where it increases cellular activity. The function of the thyroid therefore is to regulate the body's metabolism.. 1.1 Common Thyroid Disorders The thyroid gland is prone to several very distinct disorders, some of which are extremely common. These disorders can be divided into four groups, including those concerning the production of hormone (too much, or too little), those due to increased growth of the thyroid causing compression of important neck structures or simply appearing as a mass in the neck, the formation of nodules or lumps within the thyroid which are worrisome for the presence of thyroid cancer, and those which are cancerous[1]. •. Goiters:. A thyroid goiter is a dramatic enlargement of the thyroid gland. Goiters are. often removed because of cosmetic reasons or, more commonly, because they compress other vital structures of the neck including the trachea and the esophagus making breathing and swallowing difficult. Sometimes goiters will actually grow into the chest where they can cause trouble as well. X-rays will help explain all types of thyroid goiter problems. •. Hyperthyroidism: Hyperthyroidism means too much thyroid hormone. Current methods used for treating a hyperthyroid patient are radioactive iodine, anti-thyroid drugs, or surgery. Each method has advantages and disadvantages and is selected for individual patients. Many times the situation will suggest that all three methods are 1.
(14) appropriate, while other circumstances will dictate a single best therapeutic option. Surgery is the least treatment selected for hyperthyroidism. •. Hypothyroidism:. Hypothyroidism means too little thyroid hormone and is a. common problem. In fact, hypothyroidism is often present for a number of years before it is recognized and treated. Hypothyroidism can even be associated with pregnancy. Treatment for all types of hypothyroidism is usually straightforward. •. Thyroid Cancer: Thyroid cancer is a fairly common malignancy, however, the vast majority have excellent long term survival.. 1.2 Incidence and distribution of thyroid cancer The annual incidence of thyroid cancer varies considerably in different registries, ranging from 1.2-2.6 per 100,000 individuals in men and from 2.0-3.8 per 100,000 in women [2, 3]. It is particularly elevated in Iceland and Hawaii, being nearly two times higher than in North European countries, Canada and the USA. In Hawaii, the incidence rate of thyroid cancer in each ethnic group is higher than that registered in their country of origin [4], and it is particularly common among Chinese males and Filipino females. Most of the differences are probably due to ethnic or environmental factors (such as spontaneous background radiation) or dietary habits [5], but different standards of medical expertise and health care may also play a role in the efficiency of cancer detection. The American Cancer Society indicated incidence in the USA of nearly 10/100,000 population in 2003. The reported incidence has been increasing at more than 5% every year for a decade. In sharp contrast with these data concerning the incidence of clinical thyroid cancer, is the prevalence found in autopsy series or screening programs. Autopsy studies indicate a surprising frequency ranging from 0.01 to over 2.0% [6, 7]. A survey of consecutive autopsies. 2.
(15) found 2.7% of thyroids to harbor unsuspected thyroid cancer [7]. Another 2.7% had discrete benign adenomas, and nearly half showed nodularity. The high prevalence was attributed to careful examination of the gland, but probably also reflects a highly selected group of older patients dying in a hospital. Up to 6% of thyroid glands in autopsied adults in the United States, and over 20% in Japan, also harbor microscopically detectable foci of thyroid carcinoma, which are believed to be of no biologic significance. Altogether autopsy studies suggest that thyroid cancer is in many instances not diagnosed during life or is not the immediate cause of death. Both suggestions are in accord with the rather leisurely growth of the majority of thyroid tumors, especially the frequent papillary types. The annual mortality from thyroid cancer in 2003 was 5 per million for men and 6 per million for women [8]. The discrepancy between incidence and mortality reflects the good prognosis for most thyroid cancers. Recent statistics suggest about 6 deaths /million in the USA. Thyroid tumors are rare in children and increase in frequency in each decade. The variety of tumor is also related to age. Carcinomas are three times as frequent in women as in men. In the past, it was generally believed that thyroid tumors were more frequent in areas of endemic goiter, and reports from Colombia and Austria support this association [9]. More recent studies suggest that in iodine deficient countries the number of nodules is increased and, as a consequence, also the number of thyroid cancers is increased [10]. Surveys conducted in the United States found no relation between usual geographic residence and incidence of thyroid cancer.. 1.3 Pathology Pathologists are agreed that there are peculiar difficulties in the classification and diagnosis of malignant tumors of the thyroid. The histologic changes required for diagnosis of carcinoma include absence of a true capsule, invasion of surrounding normal tissue, invasion 3.
(16) of blood and lymph channels, loss of normal follicular architectural arrangements, and cellular abnormalities such as an increase in the ratio of nucleus to cytoplasm, enlarged vesicular nuclei, nuclear folding, increased mitoses, and hyperchromasia of the nucleus. Obviously the presence of distant metastases is the most certain criterion. Most studies of the disease agree that the ordinary criteria of malignancy have little prognostic value in thyroid tumors, except perhaps in the wildly growing anaplastic tumors. The general experience of pathologists has been that, in the absence of irradiation, the substrate in which thyroid tumor forms is usually like normal thyroid tissue or displays the changes of multinodular goiter or adenoma in approximately the proportion found in any sampling of the general population [11]. There is a slightly increased frequency of association with benign adenomas and with Hashimoto's thyroiditis [12]. Lymphomas are associated with Hashimoto's thyroiditis, and there is considerable evidence that lymphoma actually evolves from a gland with thyroiditis [13].. Multicentricity is a common feature of thyroid cancer, especially papillary cancer. Innumerable separate foci are sometimes found. Estimates of multicentricity range from 20 to 80% [14, 15]. Whether this phenomenon represents truly multicentric sites of origin or intrathyroidal dissemination is not clear. This multifocality is thought to be one cause of recurrences in patients treated by subtotal rather than total thyroidectomy. Both papillary and follicular tumors may appear as small (less than 1.5-cm) tumors surrounded by a densely fibrotic reaction. Although it is frequently said that these "occult" (because they may be found incidentally at operation) tumors are benign, the original report by Hazard [16] and subsequent studies show that cervical lymph node metastases occur [17]. Occasionally pathologic examination suggests conversion of differentiated papillary or follicular cancers into anaplastic forms or conversion of an adenoma into a carcinoma.. 4.
(17) 1.4 Causes of Thyroid Carcinoma Most, if not all, thyroid adenomas are monoclonal, as, presumably, are most carcinomas [18]. Colloid nodules may be either mono- or poly-clonal. Thus, tumors represent the persistent proliferation of the progeny of one cell which has somehow escaped the mechanisms which maintain normal cell division[19]. The process of carcinogenesis is thought to be a series of events induced by genetic and environmental factors which alter growth control. These factors may be considered as "initiators" and "promoters". Initiators include such agents as chemicals and irradiation which induce tumors, and promoters are agents such as phenobarbital, which in rats augments TSH secretion and radically increases tumor development. In man x-ray treatment is the sole known initiator, and other than elevated TSH, no promoters are known. Compounds such as phenobarbital, Dilantin and polychlorinated biphenyls (PCBs), which are known thyroid tumor promoters in animals through liver microsomal hormone degrading enzyme induction leading to increased thyroid hormone metabolism, do not appear to have a detectable adverse effect in man in doses usually employed [20].. 1.5 Oncogenes in thyroid tumors More than 30 "oncogenes" have been recognized in the human genome. These genes, normally silent, can become activated by chromosomal translocations, deletions, or mutations, and then can transform normal cells into a condition of uncontrolled poliferation. Most oncogenes appear to be closely related to normal growth factors, genes that control cell division, or to hormone receptors. In general, these genes, when turned on, promote cell growth and cell division and repress differentiation. Typically activation of one such gene 5.
(18) may not be enough to produce malignancy, but if accompanied by expression of another oncogene, or if gene mutation or reduplication occurs, the cell may progress toward a malignant potential. Information on expression of oncogenes in human thyroid tissue is rapidly accumulating. Expression of c-myc is stimulated in normal thyroid cells by TSH, and the proto-oncogene is expressed in adenomas and carcinomas. Activating mutations of h-ras at codons 12, 13, and 61, and over-expression of h-ras, are found in adenomas and carcinomas, but h-ras mutations are also found in nodular goiter tissue [21], suggesting that h-ras mutations could be an early event in carcinogenesis [21, 22]. Other studies, it should be noted, find ras mutations unusual [23]. Vecchio and co-workers [24] cloned an oncogene which is frequently and specifically expressed in papillary thyroid cancers. This oncogene is found on chromosome 10 (the area of the MEN I gene as well), and involves an intrachromosomal rearrangement of the tyrosine kinase domain of the ret oncogene so that it is attached to one of three different promoters, producing retPTC-1, retPTC-2, and retPTC-3. One of these translocation products is found in 20-70% of papillary cancers. This rearrangement leads to constitutive expression of the oncogene. It has been shown that intra-thyroidal expression of the ret/PTC1 oncogene can induce thyroid cancer [25]. BRAF mutations are also frequent in papillary carcinoma, and undifferentiated cancers that have arisen form papillary tumors[26]. Recently a mutational change has been associated with follicular thyroid cancers. In 5 of 8 follicular thyroid cancers, Kroll et al [27] found translocation of the DNA binding domain of PAX8 to domains A-F of the peroxisome proliferator-activater receptor (PPAR) gamma1 gene. The fusion oncogene is able to transform thyrocytes, so appears to be able to produce malignancies[28]. Although initially thought to be exclusively present in follicular cancers, it is now known to be also present in follicular adenomas [29]. Mutation or deletion of the p53 tumor suppressor gene is found in some differentiated thyroid cancers, and many 6.
(19) undifferentiated cancers. This genetic deletion may be one of the final steps leading to anaplastic cancer growth (Fig.1). Simian virus 40-like sequences are found in many thyroid cancers, as well as other cancers, and the Tag gene sequence found is known to be oncogenic in animal models [30]. Mutated and non-functional thyroid hormone receptors are recognized in up to 90% of PTC, suggesting a role in oncogenesis, but other workers find these mutations to be rare. [31,32]. The tumor suppressor gene TSG101 is over-expressed in most PTCs [33]. Overexpression of many other genes, including galectin-3, Thymosin beta-10, hTERT, CD97, CD26, VEGF, has been detected, but a question is whether these changes represent the result of carcinogenesis. Mutations in the proteins involved in the TSH receptor-G protein-adenyl cyclase kinase signal transduction pathway also play a role in tumor formation. Activating TSH receptor mutations have been found by Vassart and co-workers [34] to be the cause of most hyperfunctional nodules, and are now known to be common in "hot" nodules in patients with multi-nodular goiter. These mutations involve the extracellular loops of the transmembrane domain and the transmembrane segments, and are proven to induce hyperfunction by transfection studies. However these mutations are not associated with cancer formation. Mutations in the stimulatory GTP binding protein subunit are also present in some patients with hyperfunctioning thyroid adenomas [35]. TSH-R mutations are, however, unusual in thyroid cancer [36], excepting hyperfunctional adenomas. TSH-R expression tends to be lost as cancers de-differentiate, and persistence of expression is associated with a better prognosis [37]. In addition to positive genetic factors, carcinogenesis frequently involves loss function of tumor suppressor genes. This has been proven in hereditary retinoblastoma. These genes are normally present on both sets (maternal and paternal) of chromosomes. In retinoblastoma the inherited lack of one suppressor (RB) gene does not cause disease, but if a genetic event 7.
(20) (deletion, recombination, mutation, etc.) causes failure of expression of the second allele, cancer derives. Deletion of the tumor suppressor genes, p53 and the RB gene, have been found in differentiated and undifferentiated thyroid cancer [38]. Many chromosomal rearrangements are found in Hurthle cell tumors, and correlate with tumor recurrence [39].. 1.6 Follicular thyroid carcinoma Follicular thyroid carcinoma has a top incidence in the fifth decade of life in the United States and accounts for about one-quarter of all thyroid carcinomas [40-42]. In past decades, follicular carcinomas arrived up to 50% of thyroid malignancies in Europe. The high incidence may partly be explained by iodine deficiency, but, more likely, was due to histological miss-classification when the follicular variant of papillary thyroid carcinoma was not recognized as papillary but rather was classified as follicular. It is a slowly growing tumor and frequently is recognized as a nodule in the thyroid gland before metastases appear. Variation in the cellular pattern ranges from an almost normal-appearing structure to anaplastic tissue that forms no follicles or colloid. The insular variant of follicular tumor tends to be more aggressive [43]. The carcinoma is three times as common in women as in men. At operation one-half to two-thirds of these tumors are resected. Tumors that are small and well circumscribed tend to be less lethal than those actively infiltrating local structures. Local direct invasion of strap muscles and trachea is characteristic of the more aggressive tumors [44]. Resection depends on this feature, and death may be caused by local invasion and airway obstruction. The patients of minimally invasion have a better prognosis than those of highly invasion. Follicular carcinomas tend to invade locally and metastasize distantly, rather than to local nodes, and are especially prone to metastasize to bone or lung. In a Massachusetts 8.
(21) General Hospital series [45], one-half of patients with metastases at the time have been diagnosed to possess metastasis. Bone metastases are usually osteolytic, rarely osteoblastic, and the alkaline phosphatase level is rarely elevated. The tumor and metastases often retain an ability to accumulate and keep iodide, and are therefore sometimes susceptible to treatment with radioactive iodine(RAI). Indeed, some metastatic tumors synthesize thyroid hormone in normal or even excessive amounts. RAI therapy could improve survival in these patients [46]. Occasionally the primary lesion of a follicular tumor appears to be entirely benign, but distant metastases are found. Invasion of blood vessels or the capsule, apart from the metastasis, is the only reliable criterion of malignancy. This variant has been called the benign metastasizing struma or malignant adenoma. It has a more prolonged course than do other varieties of follicular tumor, and is the type that has offered the best opportunity for the therapeutic use of 131I. The mortality attributable to follicular cancer in the 10 - 15 years after diagnosis is 30 50% [42, 45, 46]. Of the patients dying from the lesion, three-fourths cause death from the effect of distant metastases and the remainder from locally invasive disease.. 1.7 Hurthle cell tumors Hurthle cell tumors are histologically distinct from other follicular tumors, but they pursue a similar course. They tend to invade and metastasize locally and have a strong propensity to recur after surgery. The course tends to be prolonged. These carcinomas often do not accumulate. 131. I. However, in a large survey, Caplan et al. [47] found that 4.4% of. Hurthle cell neoplasms were hot on scan and 8.9% were warm. Serum TG levels may be normal or elevated. Cheung et al. recently studied the presence of ret/PTC gene rearrangements in Hurthle cell tumors and found that many expressed ret/PTC, and also had 9.
(22) other evidence of a papillary cancer origin, including focal nuclear hypochromasia, grooves, and nuclear inclusions. Tumors with the ret/PTC gene rearrangement tended to have lymph node metastases, rather than hematogenous spread. Thus Hurthle cell tumors can be classified into Hurthle cell adenomas, Hurthle cell carcinomas, and Hurthle cell papillary thyroid carcinoma [48].. 1.8 Papillary thyroid carcinoma Papillary carcinoma has a peak incidence in the third and fourth decades [41]. It occurs three times more frequently in women than in men, and accounts for 60-70% of all thyroid cancers in adults and about 70% of those found in children. The disease tends to remain localized in the thyroid gland and in time metastasizes locally to the cervical or upper mediastinal nodes. The lesions are multicentric in 20% or more of patients, especially in children. Using rigid pathologic criteria, two-thirds of predominantly papillary thyroid cancers are found to have follicular elements. The natural history of these tumors is similar to that of pure papillary lesions [49]. Papillary thyroid tumor tends to be indolent and may exist for decades without killing the patients. In a Mayo Clinic series of papillary tumors that were detected because of lymph node metastasis or found incidentally during surgery of the thyroid gland, all the patients were unaffected by the tumors over several decades [41]. The term occult has been used in a variety of ways, including reference to tumors with malignant nodes but no obvious primary, or in reference to any tumor under 1.5 cm in diameter. Mayo Clinic reports of papillary tumors under 1.5 cm in diameter, treated with conservative subtotal thyroidectomy and node dissection, have stressed their nonlethal nature, but a 1980 follow-up report on 820 patients treated by this group notes that 6 patients 10.
(23) eventually died after spread of tumor from such "occult" primaries [50]. Patients with appropriately treated Clinical Class I or II lesions have 96-100% survival even after 15-30 years. Survival lowers to 87% for Class III and 35% for Class IV lesions at 15 years. While the disease may be aggressive in children, it is distinctly less aggressive in young adults, as compared to patients over age 40 [51]. Young patients tend to have small primary lesions and extensive adenopathy, but even with local invasion, but their survival is good. When papillary thyroid cancer occurs in persons over the age of 45, it may show several areas of undifferentiation, and pursue a highly malignant clinical course. The lesions tend to be larger and more infiltrative, and to have fewer local metastases [45]. It is possible that persons dying in older age actually have had their disease since youth, and that it has evolved into a more malignant phase [42, 52]. Papillary carcinoma tends to metastasize locally to lymph nodes, and occasionally produces cystic structures near the thyroid that are difficult to diagnose because of the paucity of malignant tissue. The presence of nodal metastasis correlates with recurrence [42,52,53] but has little effect on mortality in patients under age 45. In some studies, cervical adenopathy even seems to confer a protective effect on young people [42]. In patients over 45, the presence of nodes is associated with greater recurrence rates and more deaths [54, 55]. The tumors often metastasize elsewhere, especially to lung or bones. Papillary tumors may metastasize to the lungs and produce a few nodules, or the lung fields may have a snowflake appearance throughout. These tumors are amazingly well tolerated and may allow relatively normal physical activity for 10-30 years. At times the pulmonary metastases are active in forming thyroid hormone, and may even function as the sole source of hormone supply after thyroidectomy. The metastases may progress gradually to obstructive and restrictive pulmonary disease. They also may develop arteriovenous shunts, 11.
(24) with hypoxia or cyanosis. Such shunts become more prominent during pregnancy, perhaps as an effect of the increased supply of estrogens. The usual net extra mortality in papillary cancer is not great when compared to that of a control population - perhaps 10-20% over 20-30 years [42,53,55]. Mortality is rare in patients diagnosed before age 40, and is much greater in the patients found to be in clinical stages III and IV (Tables 1 and 2) at initial diagnosis (Fig. 2). However, Frazell and Duffy [56] have noted that papillary carcinoma is not always benign; they reported 35 patients with "invasive papillary carcinoma," which had a very malignant course.. 1.9 The prognosis of thyroid cancer Most thyroid cancers are very curable. In fact, the most common types of thyroid cancer (papillary and follicular) are the most curable [57]. In younger patients, both papillary and follicular cancers can be expected to have better than 95% cure rate if treated appropriately[58]. Both papillary and follicular cancers are typically treated with complete removal of the lobe of the thyroid which harbors the cancer, plus, removal of most or all of the other side. Medullary cancer of the thyroid is significantly less common, but has a worse prognosis. Medullary cancers tend to spread to large numbers of lymph nodes very early on, and therefore requires a much more aggressive operation than does the more localized cancers such as papillary and follicular. This cancer requires complete thyroid removal plus a dissection to remove the lymph nodes of the front and sides of the neck. The least common type of thyroid cancer is anaplastic cancer which has a very poor prognosis. It tends to be found after it has spread and is not cured in most cases. Often an operation cannot remove all the tumor. 12.
(25) 1.10 Chemotherapy Thyroid cancer is unique among cancers, in fact, thyroid cells are unique among all cells of the human body. They are the only cells which have the ability to absorb Iodine. Iodine is required for thyroid cells to produce thyroid hormone, so they absorb it out of the bloodstream and concentrate it inside the cell. Most thyroid cancer cells retain this ability to absorb and concentrate iodine[59]. This provides a perfect "chemotherapy" strategy. Radioactive Iodine is given to the patient and the remaining thyroid cells (and any thyroid cancer cells retaining this ability) will absorb and concentrate it. Since all other cells of our bodies cannot absorb the toxic iodine, they are unharmed. The thyroid cancer cells, however, will concentrate the poison within themselves and the radioactivity destroys the cell from within[60]. Not all patients with thyroid cancer need radioactive iodine treatments after their surgery. Others, however, should have it if a cure is to be expected. Patients with medullary cancer usually do not need iodine therapy, because medullary cancers almost never absorb the radioactive iodine. Some papillary cancers treated with a total thyroidectomy may not need iodine therapy as well. These cancers are often cured with complete surgical therapy alone[61].. 13.
(26) II. Specific aims: Thyroid cancer is the most common endocrine cancer and is one of the few cancers that has increased in incidence rates over the past several years. Its incidence has increased by about 3% per 100,000 people per year. The American Cancer Society estimates that there will be about 23,600 new cases of thyroid cancer in the U.S. in 2004. Of these new cases, about 17,640 will occur in women and about 5,960 will occur in men. About 1,460 people (840 women and 620 men) will die of thyroid cancer in 2004. Many patients, especially in the early stages of thyroid cancer, do not experience symptoms. However, as the cancer develops, symptoms can include a lump or nodule in the front of the neck, hoarseness or difficulty speaking, swollen lymph nodes, difficulty swallowing or breathing, and pain in the throat or neck. There are several types of thyroid cancer: papillary, follicular, medullary, anaplastic, and variants. Papillary and follicular thyroid carcinomas are referred to as well-differentiated thyroid cancer and account for 80–90% of all thyroid cancers. Their treatment and management are similar. If detected early, most papillary and follicular thyroid cancer can be treated successfully. However, follicular thyroid cancer is a slowly growing tumor and frequently is recognized as a nodule in thyroid gland before metastases appear. Therefore, the development of more genetic or protein marker for early detection is highly desirable. Some of gene variants have been recognized in thyroid cancer, including mutations of h-ras in throid adenoma and carcinoma, retPTC of chromosomal rearrangement in papillary cancers, overexpression of galectin-3, hTERT, CD 97,VEGF in thyroid cancer, but a question is whether these genetic changes represent the result of carcinogenesis. Thus, we adduce here a four-part experimental plan and prove that the aberrant expression of PDGFR-α is observed in follicular and papillary thyroid carcinoma cell, involves in providing a proliferation. 14.
(27) potential in thyroid cells, statistically correlates with malignant tumor stage and finally repressed by PDGFR-α siRNA causing follicular thyroid cell to reduce proliferation (Fig. 3). In part I, we used the cDNA expression array technology to profile differentially expressed genes from human follicular thyroid carcinoma and reveal new genetic markers as well as target genes for therapeutic intervention. In Part II, to discover the over-expressed mRNA of both PDGF-A and PDGF α-receptor in thyroid carcinoma cells and imply that autocrine activation of PDGF-α receptor plays a role in the carcinogenesis of thyroid cells. In Part III, to evaluated the immunohistochemical expressions of PDGFR-α in a consecutive series of 47 resected follicular thyroid neoplasms and shows that up-regulated expression of PDGFR-α appeared in follicular thyroid carcinomas. In Part IV, to prove the phenomenon further by genetic method, RNA interference. We designed short interfering RNAs (siRNA) specific for PDGFR-α to repress cell proliferation in follicular thyroid carcinoma cell line( CGTH W-1), compared the effects of repressing cell proliferation of CGTH W-1 cells by PDGFR-α siRNA and a tyrosine kinase inhibitor, tyrphostin AG1295 and find that PDGFR-α siRNA required 24 hours more than tyrphostin AG1295 to show significant inhibition of cell proliferation, but the effects last up to 240 hours. These experiments provided us with a better understanding of the role of PDGFR-α on thyroid carcinogenesis.. 15.
(28) Part I Identifying Differentially Expressed Genes Associated with Malignance of Thyroid Cancer by Complementary DNA Expression Array. I. Abstract Patients with follicular thyroid carcinoma had a high incidence of metastasis at the time thyroid cancer was diagnosed. Thus far, there is limited clinical factors can be used to early diagnose the presence of follicular thyroid cancer. In part 1, we used the cDNA expression array technology to profile differentially expressed genes from human follicular thyroid carcinoma and reveal new tumor markers. Tissue samples or thyroid carcinoma cell lines were obtained during surgical resection of the patients with thyroid tumor. Hybridization of identical AtlasTM human cDNA expression arrays was performed with probes derived from RNA of thyroid cancers.. 32. P-labeled cDNA. Parallel analysis of the hybridized signals. enables us to identify the alteration of gene expression in the malignant process.. We. identified 18 genes significantly over-expressed and 40 genes significantly under-expressed in the metastatic thyroid cancer. In addition, analyzing the gene expression pattern of follicular and papillary thyroid carcinoma cell lines, it was found that compared with benign tissues of thyroid nodular hyperplasia, 41 genes in CGTH W-1 exhibited more than 2-fold upregulation, while 38 genes exhibited more than 2-fold downregulation. Compared with nodular hyperplasia tissues, 35 genes in CGTH W-3 exhibited more than 2-fold upregulation, while 22 genes exhibited more than 2-fold downregulation. Genes that showed altered expression were associated with the processes of cell cycle regulation, apoptosis, DNA damage response, angiogenesis, cell adhesion and mobility, invasion, and immune response. In conclusion, we identified expression profiles of genes that are associated with malignant process of follicular thyroid cancer. Further investigation (in Part 2) is needed to understand the precise 16.
(29) relationship between the altered expression of these genes and the malignant process of follicular thyroid cancer.. 17.
(30) II. Introduction Patients with follicular thyroid carcinoma have a higher incidence of metastasis when thyroid cancer is diagnosed than patients with papillary thyroid carcinoma [1-4]. In addition, the metastasis of follicular thyroid carcinoma occurred earlier and is more likely to be associated with mortality than that of papillary thyroid carcinoma at diagnosis for a large group of patients [4]. The tumor cells must successfully complete a series of steps that include separation from the primary site, invasion into the lymphatics and/or blood stream, survival from host immunological responses, invasion into distant sites, and colonization of the new tissue or organ in order to form metastatic colonies, and several reviews have discussed the many variables associated with the cascading processes [5-8]. Understanding the process of follicular thyroid cancer malignance may lead to early and effective treatment and better prognosis. Comparing gene expression of cells in pathological changes that arise in tumor malignance provides the underlying information related to the malignant processes [9,10]. The malignant process may include altered expression of specific genes such as those encoding proto-oncogenes, tumor suppressors, cell cycle regulatory proteins, intracellular signal transducers, apoptosis-associated proteins, DNA synthesis/repair/recombination proteins, transcription factors, cellular adhesion proteins, molecular chaperon proteins, invasion associated proteins, cytokines. Thus far, the general profiles for the altered expression of such genes in thyroid cancer cells are not available. However, the following methods can be used to identify genes that are expressed at different stages in cancer cells: subtractive hybridization, large-scale sequencing, expressed-sequence-tag analysis, serial analysis of gene expression and differential display [11-14]. These techniques produce a considerable number of cDNA representing differentially expressed genes that must be further studied. Several high throughput and hybridization-based methods have been used to quantify the expression levels of genes. Among those techniques, the cDNA expression array derived 18.
(31) from the “reverse-northern” dot blots technique, provides a rapid and highly effective means for high throughput screening the differential expression of many genes in pathogenic cells [15, 16]. In Part 1, the cDNA microarray technology and the appropriate thyroid samples to analyze genes that are differentially expressed in different thyroid tissues were utilized to observe complex alteration of gene expression involved in tumor malignance.. 19.
(32) III. Materials and Methods 3.1 Tissue samples and cell cultures. Benign and malignant tissue samples were obtained during surgical resection of thyroid hyperplastic nodules and follicular thyroid carcinoma from the Department of Pathology, Chang Gung Memorial Hospital, Taiwan. The tissue specimens were frozen in liquid nitrogen and then stored at -70℃ until RNA extraction. In order to provide materials for the thyroid cancer study, Lin et al.[17] have built various thyroid cell lines, including CGTH W-1 (derived from metastatic follicular thyroid carcinoma) and CGTH W-3(derived from papillary thyroid carcinoma), which were obtained from the Division of Endocrinology and Metabolism, Chang Gung Memorial Hospital, Taiwan. Monolayer cultures of CGTH W-1 and CGTH W-3 were grown in RPMI medium 1640 (Gibco BRL, Life Technology) supplemented with 10% fetal calf serum, 2 g/L sodium bicarbonate (Sigma), 1% (v/v) nonessential amino acid (Gibco BRL, Life Technology), 1 mM sodium pyruvate (Gibco BRL, Life Technology), 100 U/mL penicillin G sodium, and 100 µg/mL streptomycin(Gibco BRL, Life Technology).. 3.2 Total RNA isolation. Total RNA was obtained by extracting tissues and cell lines in Trizol reagent (INVITROGEN Life Technologies, Invitogen Corporation, CA) according to the manufacturer’s instructions. Thyroid tissues (~100 mg each) and thyroid carcinoma cell lines (~5×106 cells) were homogenized in Trizol solution (1 mL). Homogenates were incubated for 5 minutes at 25℃, and then 0.2 volume of chloroform was added to the homogenates. The inorganic phase was separated by centrifugation at 12,000 g for 20 minutes at 4℃ after vigorous agitation for 5 minutes. RNA was then precipitated in the presence of 0.5 volume of isopropanol. RNA pellets were washed with 70% ice-cold ethanol and then dissolved in RNase-free water. Total RNA concentration was assessed with UV spectrophotometer (Gene Quant II, Pharmacia Biotech, Sweden) at 260 nm absorbency. RNA. 20.
(33) quality was confirmed and visualized as 18s and 28s bands in the agarose gel without a smearing pattern (Fig. 1 & 5).. 3.3 Poly A+ RNA enrichment. Poly A+ RNA enrichment and cDNA probe synthesis were performed from 50µg total RNA preparations by AtlasTM Pure Total RNA Labeling system(CLONTECH, CLONTECH Laboratories, Inc., CA) according to the manufacturer’s instructions. The total RNA labeling system includes streptavidin-coated magnetic beads and biotinylated oligo(dT) which allow to carry out both poly A+ RNA enrichment and probe synthesis in a single procedure. The total RNA thoroughly mix with biotinylated oligo(dT), then incubated with streptavidin-coated magnetic beads. Using the magnetic particle separator separate beads, discard supernatant. After wash the magnetic beads with poly A+ RNA, resuspend beads in 6µl dH2O.. 3.4 Synthesis and Hybridization of cDNA Probe. cDNA probe preparation and membrane hybridization were performed according to the manufacturer’s instructions for AtlasTM human cancer cDNA expression array (CLONTECH). Briefly, 1 µg polyA RNA was reverse-transcribed into cDNA by MMLV reverse transcriptase in the presence of CDS primer mix and α-32P-dATP (3000 Ci/mmol, Amersham Pharmacia, Hong Kong). Labeled cDNA was purified. from. unincorporated. nucleotides. using. a. CHROMA SPIN-200. column. (CLONTECH). The human cDNA expression arrays were prehybridized at 68℃ for 30 minutes in ExpressHyb solution (CLONTECH) to which 0.1 mg/mL salmon sperm DNA (Gibco BRL, Invitrogen Corporation, NY) had been added. The cDNA probes were then hybridized to the arrays at 68℃ overnight. The membranes were washed 4 times with 2x SSC solution containing 1% sodium dodecyl sulfate (SDS) and twice with 0.1x SSC solution containing. 21.
(34) 0.5% SDS for 30 min at 68℃ in all cases and then exposed to a phosphor screen. The images and quantitative data of gene expression levels were analyzed with a Phosphoimager (Molecular Dynamics, Sunnyvale, Calif).. 3.5 Reverse Transcription-PCR Analysis. Complementary DNA was synthesized from 2 µg of total RNA in a 25 µl reaction mixture containing 1x reverse transcriptase reaction buffer (Promega, Promega Corporation, WI), 200 µM. dNTPs, 10 ng oligo (dT)15 primer, 8 mM. dithiothreithol, 40 U Rnasin (Promega) and 100 U MMLV reverse transcriptase (Promega). The mixture was incubated at 37℃ for 50 min, heated to 80℃ for 10 min, and then chilled on ice.. Amplification of each specific genes was performed using a 2 µl aliquot of cDNA in a 50. µl amplification mixture containing 200 mM dNTPs, 0.2 µM forward and reverse primers, 2.5 units Taq DNA polymerase and 1x Taq reaction buffer. In the first experiment, PCR amplification for GAPDH was performed for 22 cycles (94o C for 30 sec, 50 o C for 30 sec, 72 o C for 30 sec) after a first denaturing step (94 o C for 2 min). For the other genes, PCR amplification was performed for 20 to 30 cycles (94 o C for 30 sec, 55 o C for 30 sec, 72 o C for 30. sec).. The. specific. primers. used. for. PCR. were. as. follows:. 5’-GTCAACGGATTTGGTCGTAT-3’ and 5’-AGTCTTCTGGGTGGCAGTGA-3’ for human. glyceraldehyde-3-phosphate. dehydrogenase. (GAPDH);. 5’-TGATGGGTTACTGTGAGCAGG-3’ and 5’-GAAATC CGCTGTCTTCACACAAC-3’ for CDC-RPK; 5’-CAAGCCCAT TCCATCCCAAC-3’ and 5’-ATCACCTCCATTCACCCACC-3’ for c-fos; 5’-CCAACTACAACTTCTTCCCTC-3’ and 5’-AAGGTCCATAGCTCATCGTC-3’ for. Gelatinase. A;. 5’-AAAAGCAGTGTCGCCCTTCC-3’. and. 5’-GCCGCCTAAGTCACAAAGTC-3’ for growth hormone-dependent insulin-like growth factor-binding protein (IGFBP BP-53).. After amplification, the PCR products were separated. in a 1.5% agarose gel and stained with ethidium bromide. In the second experiment, the specific primers used for PCR were as follows: 22.
(35) 5’-GTCAACGGATTTGGTCGTAT-3’. and. 5’-AGTCTTCTGGGTGGCAGTGA-3’. for. human glyceraldehyde-3-phosphate dehydrogenase (GAPDH); 5’-TTCCCCGCAATTATG TCACCCC-3’. and. 5’-TTTAAATCCAACGCCCCCTCCC-3’. for. growth. factor. receptor-bound protein 2 isoform (GRB2 isoform) ; 5’-GTGCTCCAGTAGTTTCTCAG CC-3’ and 5’-TTTCCCCTCGTTGCTCTTGTTC-3’ for c-myc binding protein MM-1 (c-myc MM-1); 5’-TTGCATCATTGGCCGCACAC-3’ and 5’-TGGGCGATCCCAATTACACC AC-3’ for cytosolic superoxide dismutase 1(SOD1); 5’-AAAGTTCATGGTTCCCTGGC CC-3’ and 5’-TTGTACTGCATCCGCCGCTTAG-3’ for fau. After amplification, the PCR products were separated in a 1.5% agarose gel and stained with ethidium bromide.. 23.
(36) IV. Results 4.1 RNA expression pattern in follicular thyroid carcinoma. The AtlasTM human cDNA expression array is a positively charged nylon membrane on which the DNA fragments representing 588 genes, nine housekeeping genes, and negative control sequences were spotted in duplicate dots. In the first experiment, cDNA probes derived from mRNA of primary and metastatic follicular thyroid carcinoma were hybridized to identical membrane. Several genes changed their expression levels in metastasis of follicular thyroid cancer were identified by comparing the hybridization pattern appearing on the two membranes (Fig. 2 & 3). Table 1 summarizes that 18 genes were up-regulated and 40 genes were down-regulated in metastasis process. Only those genes with larger than two-fold alterations were listed. The proteins encoded by the altered genes are associated with cell cycle regulators, growth regulators, intermediate filament markers, apoptosis, oncogenes, tumor suppressors, DNA damage responses, cell adhension and mobility, angiogenesis, invasion regulators, cell-cell interactions, immune responses. Nine housekeeping genes were used as internal controls to correct the mRNA abundance. Among these housekeeping genes, gapdh, tubulin α, β-actin, gene of 23-kDa highly basic protein, and gene of ribosomal protein S9, which showed similar relative intensities of signals in both hybridized membranes, were used to normalize the target genes. The signals of other housekeeping genes (hprt, phospholipase A2, and MHC) were either not detected or too weak to act as a useful reference. No detectable signal appeared at the sites of M13, λ-DNA, and pUC18 DNA, which served as negative control for DNA contamination of sample. In the second experiment, analyzing the gene expression pattern of follicular (CGTH W-1) and papillary (CGTH W-3) thyroid carcinoma cell lines with cDNA microarray, it was found that compared with benign tissues of thyroid nodular hyperplasia (Fig. 6 & 7), 41 genes in CGTH W-1 exhibited more than 2-fold upregulation, while 38 genes 24.
(37) exhibited more than 2-fold downregulation (Table 2). Compared with nodular hyperplasia tissues, 35 genes in CGTH W-3 exhibited more than 2-fold upregulation, while 22 genes exhibited more than 2-fold downregulation. The 13.4% (79 of 588) in CGTH W-1 cell line and 9.7% (57 of 588) in CGTH W-3 cell line of the gene elements were differentially regulated at an expression threshold of 2-fold difference.. 4.2 RT-PCR Analysis. To confirm the differential expression of genes identified on the cDNA expression arrays, total RNAs derived from thyroid carcinoma and metastatic tissue were subjected to RT-PCR analysis for five interesting genes (GAPDH, CDC-RPK, c-fos, Gelatinase A, IGFBP) in the first experiment. As shown in Figure 4, these genes studied showed the same expression pattern by gene-specific RT-PCR as observed using the cDNA expression arrays. No signal was detected by RT-PCR analysis when the cDNA synthesis step was carried out without adding reverse transcriptase, indicating that the genomic DNA contamination is negligible in our analysis condition. In the second experiment, total RNAs derived from a tissue of nodular hyperplasia, follicular thyroid carcinoma cell line and papillary thyroid carcinoma cell line were subjected to RT-PCR analysis for five interesting genes (GAPDH, GRB2 isoform, c-myc MM-1, SOD1, fau). As shown in Figure 8, the gene expressions of c-myc MM-1, SOD1 showed the same expression pattern by gene-specific RT-PCR as observed using the cDNA expression arrays.. 25.
(38) V. Discussion. Most of previous studies were undertaken to clarify biological and morphologic characteristics in human thyroid tumorigenesis.. Expression genetics is a conceptually. different approach to cancer diagnosis and prognosis. To understand the functional significance of specific gene products involved in tumor progression, it is practicable to define differential gene expression profiles by comparing the expression patterns of different tumor stages. RT-PCR and Northern blot analysis have been widely used for expression analysis, however, these studies are time-consuming and are only applicable to a restricted number of genes. Thus, a systematic approach for simultaneously analyzing large numbers of genes is required. Recently, the cDNA microarray technology has been developed for parallel analysis of the differential expression of specific genes in an entire cDNA population.. The. human cDNA expression array system provides an effective method for profiling the expression of 588 human genes in single experiment. The analytic technique is based on reverse northern blot hybridization. Each cDNA clone was immobilized in duplicate onto the nylon membrane, and each cDNA fragment length was ranged from 200 to 500 bp. The cDNA was designed without a poly-A tail, repetitive elements, and highly homologous sequences to avoid cross-hybridization and nonspecific binding. The expression pattern can be analyzed by an autoradiography after hybridization and a high-stringency wash. Seven genes (IGFBP BP-53, Gelatinase A, c-fos, CDC-RPK, GAPDH, c-myc MM-1, SOD1) analyzed agree in their expression pattern as observed in the Atlas human cDNA expression arrays according to the gene-specific RT-PCR technique. Some of the genes differentially expressed in metastatic tissue, as compared with the thyroid follicular carcinoma, were some previously implicated in cancer development [18]. For example, cell cycle regulators such as cyclin-dependent kinase (CDK) and the 26.
數據

Outline
相關文件
Samples of oral fibrous hyperplasia were used as positive controls for E-cadherin and vimentin staining. In addition, samples of normal cardiac striated muscle and
Persons with a phenotype mediated by one of these MC1R genetic variants are at greater risk of UV-induced skin cancers, because pheomelanin not only provides less effective
Lingual thyroid is defined as an ectopic thyroid gland tissue located in the midline of the tongue base and it is uncommonly observed in clinical practice and is rare in children..
The predicted expression profiles of 24 chemokines and immunosuppressive biomarkers for SCC4, SCC15, and SCC25 were used in a decision tree format to sort cell lines into those
The isolated case showed typical features, including fibrocystic breast disease, benign thyroid nodules, and multiple papillomatous lesions in the face and oral cavity, and the
Papillary thyroid carcinoma, the commonest histopathologic variant of thyroid cancer, has minimal potential for distant metastasis, and most reported metastatic thyroid carcinomas
Clear Cell carcinoma of palatal minor salivary gland harboring a novel EWSR1-ATF1 fusion gene: report of a case and review of the literature. Head
Several recent reports have described an adamantinoma-like Ewing sarcoma (ALES) arising in the thyroid gland, based on the identification of EWSR1 rearrangement in neoplasms
