Schizophrenia is a chronic psychotic illness with significant social function impairment, and social function outcome has been found to be associa-ted with impaired cognitive performances.1It is strongly recommended that cognitive assessments
should be incorporated into individual-based spe-cific pharmacologic and rehabilitation programs.2 On the other hand, cognitive deficits, such as sustained attention, working memory, verbal memory, and perceptual processes, are potential
Patterns and Clinical Correlates of
Neuropsychologic Deficits in Patients with
Schizophrenia
Shi-Kai Liu,1,2Ming-Hsin Hsieh,1Tzung-Jeng Huang,1,3Chi-Ming Liu,1,3Cheng-Chung Liu,1,3 Mau-Sun Hua,4W.J. Chen,1,5Hai-Gwo Hwu1,3*
Background/Purpose: Neuropsychologic deficits are prevalent among schizophrenic patients and are closely associated with pathogenesis and outcome. The pattern, extent, severity and contributing factors to such deficits remain to be examined in Taiwanese schizophrenic patients.
Methods: A total of 122 schizophrenic patients and 94 healthy subjects for comparison were assessed by a comprehensive neuropsychologic test battery covering the eight cognitive domains of verbal ability, visual spatial ability, abstraction/execution, verbal memory, visual memory, perceptual/motor ability, mental con-trol and attention. The relationships among cognitive deficits, demographic characteristics, clinical historical variables and clinical symptoms were further explored by multivariate regression analysis.
Results: A pattern of selective deficits superimposed on a generalized deficit was found for schizophrenic patients as a group. The mean overall deficit was 1.93 standard deviations below the control mean, and abstraction/execution, verbal memory, visual memory and attention were relatively impaired among the eight cognitive domains. However, there was also marked heterogeneity in individual performances in that 24.2%, 46.2% and 29.5% of patients performed at within normal range, moderately impaired and severely impaired levels, respectively. Duration of illness substantially affected the profile and severity of the deficits, suggesting a progressive deteriorating course in neuropsychological performance. The major predictors of cognitive deficits were number of formal years of education achieved and concurrent severity of disorganization symptoms. Conclusion: In a large sample of schizophrenic patients who underwent comprehensive neuropsycho-logic evaluation, the current results confirmed that cognitive deficits were prevalent but not a universal feature within schizophrenia. The selective impairment pattern also confirmed that such deficits were mainly in frontal and frontotemporal related functions. Despite evidence suggesting that disease chronic-ity entailed a decline in selective cognitive domains, the trajectory of the neuropsychologic deficits re-mains to be examined by further longitudinal studies. [J Formos Med Assoc 2006;105(12):978–991] Key Words: disorganization symptom, duration of illness, neuropsychologic deficits, schizophrenia
©2006 Elsevier & Formosan Medical Association . . . . 1Department of Psychiatry, National Taiwan University Hospital; 2Department of Psychiatry, Far Eastern Memorial Hospital; Departments of 3Psychiatry and 4Psychology, and 5Institute of Epidemiology, College of Public Health, National Taiwan University, Taipei, Taiwan.
Received: December 22, 2005 Revised: February 24, 2006 Accepted: July 4, 2006
*Correspondence to: Professor Hai-Gwo Hwu, Department of Psychiatry, National Taiwan University
Hospital, 7 Chung-Shan South Road, Taipei 100, Taiwan. E-mail: [email protected]
endophenotypic markers and useful probes for the complex genetics of schizophrenia.3
The literature shows that cognitive deficits are present in a substantial proportion of both recent onset and chronic schizophrenia patients, and al-most all cognitive domains are affected. These cog-nitive deficits show a pattern of specific deficits superimposed on a background of generalized deficits.4It has also been reported that the first episode and chronic patients demonstrate compa-rable levels of deficits.5–9The clinical variables of current age, age at onset, duration of illness and level of initial neuropsychologic impairment do not seem to systematically affect cognitive perform-ance.5Although certain clinical symptoms tended to parallel the levels of neurocognitive deficits, the improvements in cognitive performances could not be accounted for by changes in symptoms.7,8 The cognitive deficits observed in schizophrenic patients thus seemed stable and were largely inde-pendent of extraneous factors, hence possible the manifestations of a “static encephalopathy”.10
Nevertheless, as schizophrenia is markedly het-erogeneous in its clinical manifestations, disease courses and social functions, analysis of schizo-phrenia as a group might have misleadingly ob-scured the heterogeneity in the severity and profile of neurocognitive performances.9,11,12We wanted to investigate whether or not such deficit patterns are robust for subgroups of schizophrenia patients across disease stages or levels of cognitive impair-ment. Based on these data, we could then hypothe-size on whether the cognitive deficits are the result of a static encephalopathy or a degenerative pro-cess. Furthermore, it is important to address how cognitive performances are affected by individual and disease-associated factors, as substantial vari-ations in the severity of deficits have been found across functional domains both within and be-tween individual patients.4
Up to now, although relationships of selected cognitive domains, including sustained attention and executive function, have been reported for schizophrenic patients in Taiwan,13 there have been no systematic description of cognitive per-formances in schizophrenia. The extent, profile
and severity of cognitive deficits and potential contributing factors remain to be delineated. Over the years, we have followed up a substantial sam-ple of community dwelling schizophrenic patients after their index admissions with yearly neuro-psychologic assessments, using a comprehensive neuropsychologic test battery covering the major cognitive domains. As the patients varied widely in their demographic characteristics, disease course, durations of illness, clinical symptoms and treat-ment history, we were able to examine the effects of demographic and clinical variables on initial cognitive manifestations and subsequent change patterns. This report will focus on the initial cross-sectional cognitive performance, and the longi-tudinal changes will be reported separately. The main issues covered in this report thus include: (1) the pattern and magnitude of deficits in global and domain-specific performances of patients with schizophrenia, hence, to examine whether there are selective impairments among the functional domains; (2) the associations of cognitive deficits with a broad range of demographic and clinical characteristics, especially disease chronicity and severity, hence, to provide descriptive information for factors contributing to the cognitive deficits.
Patients and Methods
Subjects
Subjects in the current study were participants of the Taiwan Psychopathology Study of Schizophre-nia (TPSS). The TPSS was a prospective follow-up study of schizophrenic patients spanning from August 1993 to June 1998 (TPSS stage 1; previously reported as the Multi-dimensional Psychopatho-logical Group Research Projects14), and which was then extended from July 1998 to December 2001 (TPSS stage 2). The recruitment of subjects, psycho-pathologic instruments/assessments employed and follow-up methods/data schedules for TPSS have been described in detail elsewhere.13,14 Briefly, during TPSS stage 1, consecutively admit-ted schizophrenic patients were recruiadmit-ted from the National Taiwan University Hospital and the
university-affiliated Provincial Taoyuan Psychiatric Center, and Taipei City Psychiatric Center to study their historical characteristics, clinical manifesta-tions, treatment response and post-hospitalization course. Recruited subjects all met the diagnostic criteria of the Diagnostic and Statistical Manual, 4thedition (DSM-IV) of schizophrenia and gave their written informed consent. The diagnosis was confirmed at discharge by three senior psychia-trists independently, using all available caregiver reports, previous medical records, observations made during the index admission, and data gath-ered by structural interview using the Chinese version of the Diagnostic Interview for Genetic Study (DIGS-CH).15If there was any doubt, the final diagnosis was reached through a consensus meeting. Patients with a history of electroconvul-sive therapy during the previous 6 months, mental retardation, trauma-related change in conscious-ness, psychoactive substance abuse, or physical ill-ness that might cast doubt on the diagnosis were excluded. Clinical assessments of clinical symp-toms, treatment response, drug-related adverse effects, and psychosocial function were performed at admission, on discharge and at 3, 6 and 12 months after discharge, and then yearly thereafter. A total of 234 schizophrenic patients were en-rolled during TPSS stage 1, who had been followed-up for 2–4 years at the conclusion of TPSS stage 1. At the start of TPSS stage 2, attempts were made to re-contact all TPSS stage 1 participants; those who renewed their consent were followed-up yearly for a further 2.5 years. In addition to the clinical assessments administered during TPSS stage 1, a comprehensive neuropsychologic test battery (described below) was further incorporated into the yearly assessments. Of the original 234 TPSS subjects who were successfully traced and who completed at least two neuropsychologic eval-uations during the follow-up period, 122 (52.1%) were subjects of this report. Comparisons between the 122 cases included and the 112 cases who failed to be approached or who completed less than two neuropsychologic evaluations showed that there was no significant difference in sex (χ2= 0.07, p = 0.79), age (t= −1.26, p = 0.22), education (t = 0.33,
p= 0.74) and severity of initial clinical symptoms (for all symptom factors, p> 0.05).
For comparison and to provide estimates of the degree of deviation of schizophrenic patients’ neu-ropsychologic performances, 94 healthy subjects were recruited through advertisements and an-nouncements within the hospitals. Although the demographic characteristics could not be matched individually, attempts were made to include con-trols as closely matched in age, sex composition and education levels as possible. The clinical and neuropsychologic assessments of the control sub-jects followed the same protocol as those for the schizophrenic subjects. Evaluation using the DIGS-CH interview was done to rule out neuropsychi-atric illness, DSM-IV axis I disorders and axis II schizophrenia-related personality disorders, men-tal retardation, and alcohol/psychoactive substance use within the past 1 year. The groups had nearly equal gender distribution (48.9% males vs. 50% males for comparison subjects vs. schizophrenic patients, respectively). Compared to schizophrenic patients, comparison subjects were younger (mean age± standard deviation [SD], 28.61 ± 10.98 years vs. 32.89± 7.14 years for comparison subjects vs. schizophrenic patients respectively, p< 0.05) and better educated (mean years of education, 13.52± 2.96 vs. 11.17± 2.82 for comparison subjects vs. schizophrenic patients, respectively, p< 0.05). As the differences in basic characteristics might have confounded the estimation, we made statistical ad-justments to account for the possible effects of age, sex and education in standardizing patients’ neu-rocognitive performance scores (described below).
Clinical assessments
Baseline information regarding age at onset of psy-chiatric symptoms, duration of illness and history of previous medication and hospitalization were collected systematically. The Chinese version of the Positive and Negative Syndrome Schedules (PANSS),16having sufficient interrater reliability,17 was used by trained senior research psychiatrists to assess the clinical psychopathology at baseline and at follow-ups. Antipsychotic-induced movement disorders were assessed by the Extrapyramidal
Syndrome Rating Scale,18which provided global severity measures for tardive dyskinesia (ESRS–TD) and Parkinsonism (ESRS–EPS) on a 0–7-point Likert scale.
Considering that the current sample consisted mainly of community living outpatients with mild clinical symptoms, and most of the general psy-chopathology subscale items of PANSS showed rare occurrences and little variation in ratings, we used seven positive subscale items and seven neg-ative subscale items for symptomatologic analy-ses. Our previous factor-analytic study showed that the 14 PANSS positive and negative subscale items regrouped into four symptom dimensions, i.e. the negative (blunted affect, emotional withdrawal, poor rapport, passive apathetic social withdrawal), disorganization (conceptual disorganization, dif-ficulty in abstract thinking, stereotyped thinking), delusion/hallucination (delusions, hallucinatory behavior, suspiciousness/persecution), and ex-citement (exex-citement, hostility) factors. These symptom dimensions were reported to be more related to cognitive performance than the ori-ginal PANSS subscales.13 We selected these 14 positive and negative subscale items to generate the four mean factor scores for analyses in this study.
Neuropsychologic tests and construction of neurocognitive functional domain
The neuropsychologic test battery consisted of the Wechsler Adult Intelligence Scale–revised (WAIS–R), Wechsler Memory Scale–revised (WMS–R), Wisconsin Card Sorting Test (WCST) computerized version, Continuous Performance Test (CPT) undegraded AX version, and Trail-making test parts A and B (Trail-A, B). The com-plete neuropsychologic evaluation took about 2.5 hours and was completed in the same day. As the tests were of composite nature and probably mea-sured overlapping neuropsychologic processes, in-dividual items of the tests were re-categorized into constructs of cognitive functional domains that hypothetically reflected basic cognitive proc-esses.11 According to Kremen et al, the cognitive domains and their components included the
following: (1) verbal ability (VA)= information, similarity, comprehension (WAIS–R); (2) visual/ spatial ability (VS)= block design, picture ar-rangement (WAIS–R); (3) abstraction/execution (ABEX)= category achieved, perseverative response (WCST), Trail-B; (4) verbal memory (VEM)= ver-bal paired association, immediate and delayed; (5) visual memory (VIM)= visual reproduction, immediate and delayed (WMS–R); (6) perceptual/ motor (PEMO)= Trail-A, digit–symbol (WAIS–R); (7) mental control (MC)= arithmetic, digit span backward (WAIS–R); (8) attention (ATTN)= sensi-tivity index d’ (CPT), digit span forward (WAIS–R). To adjust for the effects of age, sex and educa-tion on cognitive performance, the predictive scores of individual cognitive test items of a subject were calculated by using the regression coefficients obtained from the regression of the cognitive scores on age, sex and education among the 94 comparison subjects. The difference between the raw score and the predictive score was then standardized by the root mean error of the re-gression and was defined as the adjusted z score of the individual test item. The comparison group’s mean standardized z scores of the cogni-tive domains were adjusted to a mean of 0 and SD of 1. The standardized z scores of the schizo-phrenic patients thus provided the extent of the de-viation from the comparison group and the direction of the z scores was adjusted so that higher scores indicated better performances. From individual item z scores, cognitive domain z scores could be generated by the summed aver-age of the individual z scores of component items within each domain. In turn, an overall neuropsy-chologic performance index (NPI) was calculated for each subject by the summed average of the in-dividual domain z scores. To examine the meaning of clinical heterogeneity in cognitive performance, study subjects were further classified according to the NPI into three severity subgroups: (1) those within normal limits (WNL), NPI > −1 (n = 32, 24.2%); (2) those moderately impaired (MI), NPI between −1 and −2.5 (n = 61, 46.2%); (3) those severely impaired (SI), NPI < −2.5 (n = 39, 29.5%).
Data analysis
Variables significantly associated with cognitive performances were examined by comparisons between subgroups defined according to specific variables (sex, illness duration, type of antipsy-chotics used, NPI). The correlations among demo-graphic, clinical variables and cognitive domain scores were also examined. The χ2test was used for categorical variables and the independent t test or univariate analysis of variances (ANOVA) with Scheffe’s post hoc analysis for continuous variables Correlations among demographic, clinical history, psychopathologic variables and cognitive impair-ments were examined by Pearson’s correlational analysis. For variables with non-normal distribu-tions, root square transformation was undertaken before the correlational analyses. Further multiple regression analyses were used to explore the effects of the demographic and clinical variables on the cognitive variables. NPI and individual cognitive domain mean z scores were regressed on a set of variables that were considered possibly con-tributing to the cognitive performances, includ-ing selective demographic variables (current age, sex, education), clinical historical variables (age at onset, duration of illness), concurrent neuro-logic status (presence of tardive dyskinesia and the severity of EPS) and the scores of the four symptomatologic dimensions. Statistical analyses were performed using SPSS version 10.0 (SPSS Inc., Chicago, IL, USA).
Results
Table 1 shows the descriptive data of clinical his-torical variables, symptomatologic dimensions, medications, extrapyramidal side effects and per-formances in cognitive domains of the patients. Since the current study was an extension from a previous longitudinal follow-up study, no sub-ject was experiencing his/her first episode, and du-ration of illness spanned a wide range (2–30 years) with a mean± SD of 10.09 ± 5.86 years. They were mildly symptomatic as indicated by the low mean PANSS factor scores. All patients were receiving
neuroleptics with a mean± SD dose of 821.00 ± 526.92 mg chlorpromazine equivalents, and 27.0% of subjects were receiving atypical antipsy-chotics (including 13% using clozapine). Patients had poor WAIS–R verbal IQ (mean± SD = 87.22 ± 16.04, compared with the 111.88± 13.26 of the comparison subjects, p< 0.05) and global NPI (mean NPI= −1.93, one sample t test, p < 0.05). When classified by their NPIs, 24.2% (n= 32) of subjects could be considered as performing within the normal range (WNL group); 46.2% (n= 61) were moderately impaired (MI group); and 29.2% (n= 39) were severely impaired (SI group). Patients were substantially impaired across all individual domains (Table 1), with deficits (in z score units, reflecting the number of standard deviations below the mean of comparison subjects) ranging from −1.08 (visual/spatial ability) to −2.49 (verbal memory). Verbal ability and visual/spatial ability were relatively preserved with domain z scores around −1. In contrast, verbal memory, visual memory, abstraction/execution, and attention showed more severe impairments with deviations around 2.5 SD. Male and female schizophrenic pa-tients did not reveal significant difference in demo-graphic and clinical characteristics and severity of clinical symptoms and extrapyramidal side effects (Table 1). Female patients outperformed male pa-tients in verbal ability, visual/spatial ability and verbal memory, with verbal memory showing the greatest gender difference. No significant differ-ence was found between patients using traditional antipsychotics and those using second generation antipsychotics (comparisons across the eight neu-ropsychologic domains were not significant, all ps> 0.05).
Figure 1 reveals the performances in the eight cognitive domains of patient groups with different durations of illness. Patients were subgrouped into those with illness duration < 5 years, i.e. the short duration group (SG, n= 30); those with between 5 and 10 years of illness duration, i.e. the medium duration group (MG, n= 48); and those longer than 10 years of illness duration, i.e. the long duration group (LG, n= 44). There was a general pattern of deterioration in all eight cognitive
ATTEN MC PEMO VIM VEM ABEX VS VA 0.0 –0.5 –1.0 –1.5 –2.0 –2.5 –3.0 –3.5 –4.0 Cognitive performance Mean z score < 5 yr 5–10 yr > 10 yr
Figure 1. Deficits in eight cognitive domains by
groups of patients with short duration (< 5 years), medium duration (5–10 years) and long duration (> 10 years) of illness. VA = verbal ability; VS = visual-spatial ability; ABEX = abstraction/ execution; VEM= verbal memory; VIM = visual memory; PEMO = perceptual/motor ability; MC = mental control; ATTEN = attention.
Table 1. Descriptive data of clinical historical variables, symptomatologic dimensions, extrapyramidal
symptoms and cognitive performances in schizophrenic patients*
Male (n= 61) Female (n= 61) Total (n= 122) Clinical history variables
Current age (yr) 32.69± 6.69 33.08± 7.61 32.89± 7.14
Education (yr) 10.93± 2.61 11.41± 3.02 11.17± 2.82
Age at onset (yr) 21.92± 6.01 23.95± 6.69 22.94± 6.42
Duration of illness (yr) 10.79± 6.58 9.39± 5.00 10.09± 5.86
Symptomatologic dimensions Negative symptoms 2.46± 1.14 2.46± 1.27 2.46± 1.20 Delusion-hallucination symptoms 2.52± 1.24 2.34± 1.21 2.45± 1.22 Cognitive symptoms 2.85± 1.20 2.69± 1.53 2.81± 1.37 Excitement symptoms 1.44± 0.71 1.50± 0.80 1.50± 0.78 Medication Neuroleptics (mg/d) 883.33± 598.75 760.12± 444.57 821.00± 526.92 Anticholinergics (mg/d) 10.31± 5.17 10.89± 3.82 10.67± 2.34
Extrapyramidal system side effects
ESRS–tardive dyskinesia 0.34± 0.87 0.37± 6.80 0.35± 0.83 ESRS–Parkinsonism 1.31± 1.10 1.38± 1.22 1.34± 1.16 Cognitive performances NPI −2.11 ± 1.08 −1.78 ± 1.17 −1.93 ± 1.13 Verbal ability† −1.40 ± 0.99 −0.93 ± 1.00 −1.16 ± 1.01 Visual-spatial ability† −1.35 ± 0.91 −0.75 ± 1.05 −1.08 ± 1.01 Abstraction/execution −2.38 ± 1.11 −2.27 ± 1.07 −2.32 ± 1.12 Verbal memory† −3.04 ± 2.73 −2.04 ± 2.63 −2.49 ± 2.71 Visual memory −2.53 ± 2.30 −2.33 ± 2.16 −2.41 ± 2.19 Perceptual/motor −2.19 ± 1.70 −1.74 ± 2.08 −1.95 ± 1.89 Mental control −1.85 ± 0.81 −1.64 ± 0.79 −1.72 ± 0.81 Attention −2.21 ± 1.69 −2.54 ± 2.17 −2.38 ± 2.00
*Data presented as mean ± standard deviation;†significant difference between male and female (p = 0.05). ESRS = Extrapyramidal Syndrome Rating Scale; NPI = overall neuropsychologic performance index.
domains in the disease course in that patients with longer duration of illness tended to have poorer performances in the majority of cognitive domains (Figure 1). Among the domains, verbal memory, vi-sual memory and attention showed overt progres-sive deteriorations with increased chronicity, with z scores of −1.72 to −3.34, −2.34 to −3.02, and −1.56 to −2.96 respectively. The other two domains that showed a mild degree of decline were perceptual/ motor and mental control. The corresponding z score changes were z values of −1.30 to −2.32, and −1.42 to −1.96, respectively. Although the overall pattern of relative deficits in abstraction/ execution, visual memory, verbal memory and at-tention were largely preserved across subgroups, it was notable that verbal ability, visual/spatial ability and abstraction/execution were almost identical for the MG and SG subgroups, indicat-ing no further worsenindicat-ing in subjects in the later disease stages. The results suggest that although abstraction/execution was affected in patients in the early phase of the disease, it remains stationary and does not further deteriorate as the disease pro-gresses to the later stages. In contrast, verbal mem-ory, visual memory and attention performances declined with the passage of time, probably in the first 5 years within disease onset.
Figure 2 shows the performance in the eight cognitive domains of patient groups with different degrees of impairment in overall NPI. Across sub-groups with different severities of cognitive deficits,
the differences in each cognitive domain were, as expected, significant among the three subgroups (ANOVA with Scheffe’s post hoc comparisons, all ps< 0.01). However, it was notable that differences
among the subgroups in magnitudes of deficits in verbal ability, visual/spatial ability and abstraction/ execution were relatively small, while large rela-tive deficits in verbal memory, visual memory and attention were found. The deficits in these three domains were most profound in the SI group (Figure 2), which gave rise to the overall relative deficit pattern of the profile of the total sample. WNL patients and SI patients were further com-pared for possible differences in clinical history variables, treatment-related side effects and clinical symptom profiles. The WNL group was signifi-cantly better educated (t= 4.46, p < 0.001), with older age at disease onset (t= 2.20, p = 0.03), shorter duration of illness (t= −2.13, p = 0.04), less severity of EPS (t= −2.34, p = 0.02), lower antipsy-chotic dosage (t= −2.72, p = 0.009), and with fewer negative and disorganized symptoms (t= −2.78, p= 0.007; t = −5.10, p < 0.001, respectively).
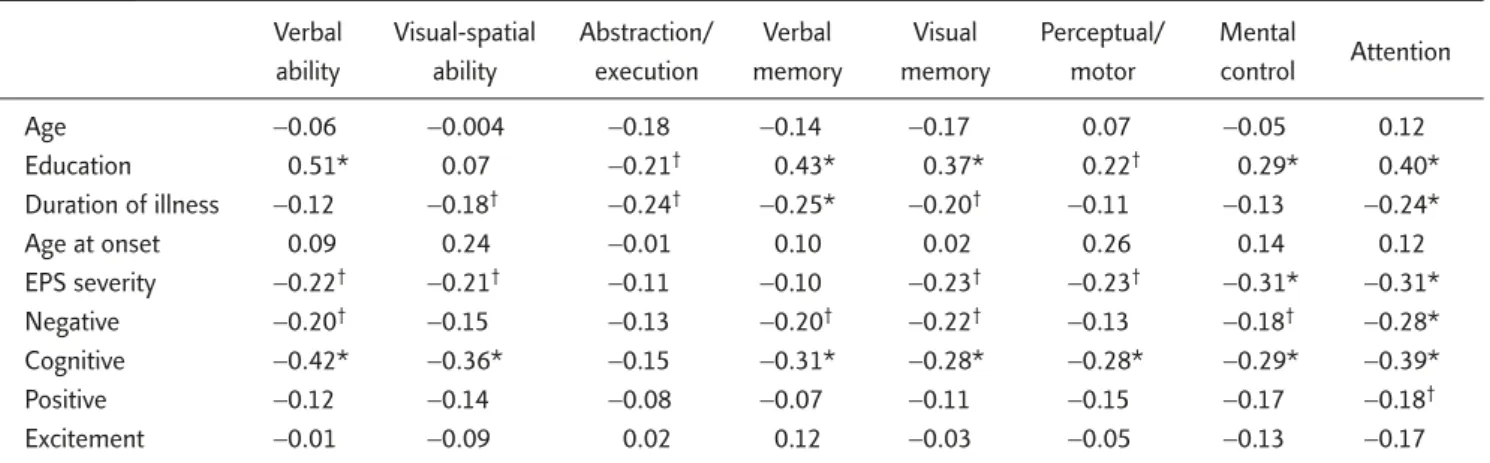
Table 2 reveals the correlations among clinical historical variables, clinical symptoms and deficits in individual cognitive domains. The data showed that there was a general pattern that poorer per-formances were associated with less education, longer duration of illness, severer clinical negative, disorganization symptoms and EPS. It was nota-ble that current age, age at onset, positive and
ATTEN MC PEMO VIM VEM ABEX VS VA 0.0 –0.5 –1.0 –1.5 –2.0 –2.5 –3.0 –3.5 –4.0 MI WNL Cognitive performance Mean z score TOTAL
SI Figure 2. Deficits in eight neurocognitive do-mains by subgroups of patients with normal per-formance (WNL), mild impairment (MI) and severe impairment (SI) in overall neuropsycho-logic performance index. VA = verbal ability; VS = visual-spatial ability; ABEX = abstraction/ execution; VEM = verbal memory; VIM = visual memory; PEMO = perceptual/motor ability; MC = mental control; ATTEN = attention.
excitement symptoms were not associated with any cognitive performance.
Table 3 shows the predictive variables of cogni-tive deficits using multivariate regression analysis. The predictive variables included demographic characteristics (age, sex, education), duration of illness, motor side effects (severity of EPS and tardive dyskinesia) and the four clinical symptom dimensions. The analytical model was significant for all cognitive domains (R2= 0.22−0.42) except abstraction/execution (R2= 0.16, p = 0.08). Many
of the variables with significant correlations in uni-variate analyses were not significant on multivari-ate analysis, indicating complex intercorrelations among the variables. Disorganization symptoms and education were the two most robust contri-buting factors to cognitive domain performances in terms of the number of domains involved (five and four domains respectively) and the relatively large regression coefficients. Duration of illness, gender and severity of EPS also had scattered asso-ciations with verbal ability, visual/spatial ability, perceptual/motor and attention.
Discussion
This study described in detail the profiles of cog-nitive deficits in 122 community living stable schizophrenic patients. The results showed that schizophrenic patients as a group had significant impairments in neuropsychologic function with
a mean global deficit of 1.93 SDs relative to the comparison subjects, after adjusting for age, sex and education (Table 1). The mean deficits of around 2 SDs in the current schizophrenic sample are comparable to those reported in chronic schiz-ophrenic patients,19but larger in magnitude than the 0.5–1.5 SDs reported for patients experiencing their first episode.20We thus emphasize that there might be cognitive function deteriorations along the clinical course in schizophrenic patients, which is substantiated by the data shown in Figure 1, where a progressive pattern of cognitive function impairment was clearly shown, especially in verbal memory, visual memory, perceptual/motor, men-tal control and attention. A relative deficit pattern was also found in that more severe impairments could be observed in verbal memory, visual/spatial memory, abstraction/execution and attention func-tions (mean z scores around −2.5) than in verbal ability and visual/spatial ability (mean z scores around −1).
The generalized deficits with disproportionate impairments in attention, frontal-based executive functions, and temporal-based memory found in the current study replicate those reported in the literature20–23and this also supports that cognitive impairments in schizophrenia might be character-ized by selective involvement of frontotemporal functions superimposed on a generalized disabil-ity.4,20,21The functional deficits were also associated with changes in prefrontal and temporal structure and volume in schizophrenic patients.23–25
Table 2. Correlations among demographic, clinical variables and z scores of performances in the eight cognitive domains
Verbal Visual-spatial Abstraction/ Verbal Visual Perceptual/ Mental
Attention
ability ability execution memory memory motor control
Age −0.06 −0.004 −0.18 −0.14 −0.17 0.07 −0.05 0.12 Education 0.51* 0.07 −0.21† 0.43* 0.37* 0.22† 0.29* 0.40* Duration of illness −0.12 −0.18† −0.24† −0.25* −0.20† −0.11 −0.13 −0.24* Age at onset 0.09 0.24 −0.01 0.10 0.02 0.26 0.14 0.12 EPS severity −0.22† −0.21† −0.11 −0.10 −0.23† −0.23† −0.31* −0.31* Negative −0.20† −0.15 −0.13 −0.20† −0.22† −0.13 −0.18† −0.28* Cognitive −0.42* −0.36* −0.15 −0.31* −0.28* −0.28* −0.29* −0.39* Positive −0.12 −0.14 −0.08 −0.07 −0.11 −0.15 −0.17 −0.18† Excitement −0.01 −0.09 0.02 0.12 −0.03 −0.05 −0.13 −0.17
T
able 3.
Pr
edictive variables of cognitive deficits using multivariate r
egr ession analysis* NPI V erbal ability V isual-spatial Abstr action/ V erbal memory V isual memory P er ceptual/ Mental contr ol Attention ability execution † motor Adjusted R 2 0.38 § 0.42 § 0.24 § 0. 16 0.29 § 0.22 § 0.21 § 0.25 § 0.38 § Standar dized r egr ession coefficient β ‡ Age – – – – – – – – – Sex – 0. 16 || 0.26 || –– – – – – Education 0.33 § 0.43 § – – 0.32 § 0.34 § – 0.25 § 0.37 § Dur ation of illness − 0.21 || – − 0.20 || – − 0. 18 || – − 0.25 || − 0. 19 || − 0.20 || EPS − 0.20 || − 0. 19 || –– – – – − 0.32 § − 0.25 § TD – – – – – – – – – Negative – – – – – – – – – Disor ganization − 0.37 § − 0.38 § − 0.37 § – − 0.23 || – − 0.24 || – − 0.27 || Delusion/hallucination – – – – – – – – – Excitement – – – – – – – – – *Individual neur
ocognitive domain performance was r
egr
essed on demogr
aphic char
acteristics (age, sex, education), dur
ation of i
llness and curr
ent pathologic manifestations (severity of EPS, severity of TD,
and the four clinical symptom dimensions);
†the over
all model was not statistically significant so the r
egr
ession coefficients ar
e not shown;
‡only the statistically significant (p
< 0.05) standar dized b s ar e shown; §p < 0.005; ||p < 0.05. NPI = over all neur
opsychologic performance index; EPS
=
extr
apyr
amidal system side effects fr
om antipsychotic medications; TD
=
tar
Despite the evidence, there remains concern that as the difficulty and complexity levels of the tasks for individual cognitive domains were often unmatched, the relative deficit pattern might have simply reflected the difficulty levels rather than genuine domain-specific impairments. Moreover, a generalized deficit or a slowing in general pro-cessing speed, rather than possible domain-specific or task-specific deficits could have accounted for the uneven performance pattern,26since tasks with selective attention/inhibition components and those with a lexicon component were demon-strated to be affected by the general processing speed to a greater extent than those without in schizophrenic patients.27,28Indeed, negative symp-toms and severity of extrapyramidal sympsymp-toms, both clinical indicators for possible psychomotor slowing, was associated with poorer performances in those neurocognitive domains that were time-bound and speed-dependent.
There are reasons to believe that the pattern of differential deficits revealed by the current study is not likely to be an artifact, as schizophrenic and comparison subjects were equally exposed to the task-difficulty effects which were controlled for by the standardization of the cognitive data. The comparisons of the z scores within schizophrenia thus reflected the degree of relative domain-specific differences after weighting against comparison subjects rather than direct comparisons between the domain performances within schizophrenia subjects. In addition, neurocognitive ability was considered as a composite construct of complex cognitive processes, hence not likely to be ex-plained by a general ability.29Besides, the parsing of neurocognitive function into distinct independ-ent dimensions has been verified psychometrically by previous factor or cluster analytic studies30and external validity was provided through their differ-ential associations with historical variables and clinical characteristics, especially the negative and disorganization symptoms.29,31,32 More specifi-cally from the current study, the cognitive domains did show differential patterns of associations with other noncognitive factors, supporting their rela-tive independence.
Analysis of schizophrenia as a group might have misleadingly obscured the heterogeneity in severity and profile of cognitive performances.11,12 Indeed, schizophrenic subjects in the current study varied greatly in global severity of cognitive impair-ments. Around 24.2% (n= 32) could be described as performing without over impairment, 46.2% (n= 61) as moderately impaired, and 29.2% (n=39) as remarkably impaired. The relative deficit pattern of the entire group was less conspic-uous among subgroups with less global impair-ments and became apparent in those with the most severe global impairments due to the very poor performances in verbal memory, visual memory and attention. Subgroups defined by subjects’ length of illness also revealed a similar pattern of selective deficits. In the group with remarkable impairment, the association of severe cognitive impairments with lower educational achievement, earlier age at onset, longer duration of illness, more severe EPS, negative and disorganized symp-toms, provided evidence for a separate subtype within schizophrenia, e.g. the deficit type of schizo-phrenia.33 Another intriguing finding was that these subgroups also differed in their deficit pro-files. For those with least impairments, selective impairment was most apparent for the abstraction/ execution function, while for those with more severe global deficits, the deficits in abstraction/ execution remained at about the same level as those less severely impaired, and the worst perfor-mances were found in verbal memory, mental con-trol and attention. Ceiling effects in abstraction/ execution might have accounted for the findings. In multivariate analyses, sex, education, dura-tion of illness, disorganizadura-tion symptoms and severity of extrapyramidal symptoms were found to contribute to individual domain performances except for the domain of abstraction/execution, independently. The pattern of relative abstraction/ execution, verbal memory/visual memory and at-tention impairments was largely preserved for all groups with different disease chronicity. Moreover, the poorer performances in verbal memory, visual memory and attention manifested by patients with longer duration of illness suggested that decline
in performances in these domains might have occurred over the passage of time. The possible decline might not be simply age-related, since current age and age at onset were not associated with performance. The duration effects remained robust for visual/spatial ability, verbal memory, perceptual/motor, mental control and attention after potential confounding factors were con-trolled for in multiple regression analysis. The find-ings were in contrast to results from first episode patients that performances in most neurocognitive domains remained stable or even improved.22,34 Considering that first episode subjects were mainly younger aged with follow-up periods limited to the immediate post-psychotic years, the evaluation might have missed the critical period of cognitive decline.35The current finding of possible neuro-cognitive declines was nonetheless limited by its cross-sectional nature; further longitudinal studies of patient samples stratified according to disease chronicity and followed-up for sufficient periods of time are required to solve this issue. Moreover, should there be true decline, it should not be taken as direct evidence of an ongoing neurode-generative process, since natural age-related decline in cognitive functions, cumulated treatment-related side effects and environmental factors might com-plicate the picture.36
Disorganization symptoms were the only clini-cal symptoms showing consistent associations with cognitive domain deficits in the current study. Despite the attempts to explain clinical symptoms in terms of cognitive dysfunction, they neverthe-less exhibited complex relationships and the find-ings were inconsistent. Variability in the nature of cognitive domains under investigation, clinical characteristics of the subjects, symptom definition and classifications might have contributed to the inconsistent findings.37,38Studies in first episode cases did not reveal consistent associations with clinical symptoms even with large sample size up to 301 subjects,9,34but during subsequent follow-up, associations with negative symptoms were observed,7,39 indicating that clinical symptoms in the early stage might be poorly representative of cognitive deficits, while persistent symptoms
manifested in stable clinical states are related to underlying cognitive dysfunction. This is sup-ported by findings in stable patients with longer duration of illness that correlations with severity of negative and disorganized symptoms were more consistently reported.37,40,41Nevertheless, the cor-relations were modest at best, and clinical symp-toms contributed to only 10–15% of the variance in cognitive performances, and the longitudinal development of cognitive dysfunction did not par-allel the change in clinical symptoms, suggesting that psychopathology and cognitive deficits in schizophrenia only partially overlap and might be caused by distinct pathophysiologic processes.42
In the current study, negative symptoms were associated with cognitive measures in primary analysis but not in multivariate analysis. It is plau-sible that the negative symptoms were defined relatively narrowly, focusing on aspects of dimin-ished affective expression, diminution in interper-sonal contacts and social interests, while those more directly reflective of cognitive dysfunction, such as positive formal thought disorder, language performances and abstract thinking ability, were categorized as disorganization symptoms. In this regard, the results concurred with previous reports that syndromes of alogia, attentional impairment, and positive formal thought disorder that reflected primarily a disorganization of thought are more closely associated with cognitive performances than syndromes of affective flattening, avolition/ apathy, and anhedonia.43 Another possibility is that it was often difficult to distinguish between primary negative symptoms and extrapyramidal symptoms. This appeared to be the case in the cur-rent study, since negative symptoms and extrapyra-midal symptoms were moderately correlated (r= 0.47, p < 0.001) and the profiles of associa-tions with cognitive deficits in primary analyses were rather similar.
As expected, patients with better education per-formed better in most domains except perceptual/ motor and abstraction/execution. One plausible explanation was that levels of academic achieve-ment simply reflected differences in premorbid in-tellectual ability, hence the differences in cognitive
performances. However, it is complicated by the fact that schizophrenia often develops insidiously during critical periods of academic achievement and that some attenuation is expected and the de-gree of decrement cannot be exactly determined.44 In the current study, when the 22 (12.5%) sub-jects who developed schizophrenia before com-pleting their highest education were excluded, the results of analysis were similar to those obtained from the whole sample, indicating that the effects of possible underestimation of baseline intellec-tual ability by their educational achievement did not significantly influence the results. In addi-tion, the association between verbal IQ, which is considered to be relatively well preserved in schiz-ophrenia and approximates premorbid intellec-tual ability,4and education was modest (r= 0.55). Education thus might have independent contri-butions to cognitive performances other than gen-eral intellectual ability. It might be hypothesized that performances in tasks with at least some com-ponents that are well learned before the onset of disease are associated with education, such as ver-bal ability and verver-bal memory, whilst those involv-ing mainly visual-spatial ability and perception are not. The unexpected finding of the negative con-tribution of education to abstraction/execution remains to be further explored.
The selective versus generalized issue might not be of mere academic interest. Although the rela-tionships between cognitive domain perform-ances and subsequent psychosocial functioning in the current sample are yet to be reported, as types and severity of individual cognitive domain deficits were associated with unique functional outcome dimensions, they were important targets of clinical assessments and treatment.45Generally, cognitive deficits did predict subsequent social functioning, independent daily living and disabil-ity level,46–48and measures of cognitive function-ing accounted for more variance in functional capacity than did psychiatric ratings of symp-toms.47More specifically, verbal memory was asso-ciated with all types of functional outcome;49 vigilance was related to social problem solving and skill acquisition;50 and executive function
predicted community functioning but not social problem solving.49 Since the current sample showed overt deficits in all these domains, it would be possible to examine whether they are in-deed associated with different aspects of social and community functions and predicted subsequent functionality.
In conclusion, this study has provided informa-tion on the severity and profile of neurocognitive deficits in schizophrenic patients. Heterogeneity in neurocognitive capacity was clearly demonstrated and several potential contributing factors were found. Subjects with different durations of illness manifested specific patterns of deficits, and memory-related functions seemed to deteriorate with the passage of time, implying different trajec-tories taken by individual domains. The further development of neurocognitive deficits awaits confirmation from the results of longitudinal follow-up studies.
References
1. Dickerson F, Boronow JJ, Ringel N, Parente F. Social func-tioning and neurocognitive deficits in outpatients with schiz-ophrenia: a 2-year follow-up. Schizophr Res 1999;37:13–20. 2. Bilder RM. Neurocognitive impairment in schizophrenia and how it affects treatment options. Can J Psychiatry 1997;42:255–64.
3. Glahn D, Therman S, Manninen M, et al. Spatial working memory as an endophenotype for schizophrenia. Biol Psychiatry 2003;53:624–6.
4. Heinrichs RW, Zakzanis KK. Neurocognitive deficit in schizophrenia: a quantitative review of the evidence. Neuro-psychology 1998;12:426–45.
5. Heaton R, Gladsjo J, Palmer B, et al. Stability and course of neuropsychological deficits in schizophrenia. Arch Gen Psychiatry 2001;58:24–32.
6. Moritz S, Andresen B, Perro C, et al. Neurocognitive per-formance in first-episode and chronic schizophrenic pa-tients. Eur Arch Psychiat Clin Neuroscience 2002;252:33–7. 7. Gold S, Arndt S, Nopoulos P, et al. Longitudinal study of cognitive function in first-episode and recent-onset schiz-ophrenia. Am J Psychiatry 1999;156:1342–8.
8. Hughes C, Kumari V, Soni W, et al. Longitudinal study of symptoms and cognitive function in chronic schizophrenia. Schizophr Res 2003;59:137–46.
9. Rund BR, Melle I, Friis S, et al. Neurocognitive dysfunc-tion in first-episode psychosis: correlates with symptoms,
premorbid adjustment, and duration of untreated psychosis. Am J Psychiatry 2004;161:466–72.
10. Goldberg TE, Hyde TM, Kleinman JE, Weinberger DR. Course of schizophrenia: neuropsychological evidence for a static encephalopathy. Schizophr Bull 1993;19:797–804. 11. Kremen W, Seidman L, Faraone S, et al. Heterogeneity of schizophrenia: a study of individual neuropsychological pro-files. Schizophr Res 2004;71:307–21.
12. Palmer B, Heaton R, Paulsen J, et al. Is it possible to be schiz-ophrenic yet neuropsychologically normal? Neuropsychology 1997;11:437–46.
13. Liu SK, Hwu HG, Chen WJ. Clinical symptom dimensions and deficits on the Continuous Performance Test in schiz-ophrenia. Schizophr Res 1997;25:211–9.
14. Hwu HG, Chen CH, Hwang TJ, et al. Symptom patterns and subgrouping of schizophrenic patients: significance of nega-tive symptoms assessed on admission. Schizophr Res 2002; 56:105–19.
15. Chen WJ, Liu SK, Chang CJ, et al. Sustained attention deficit and schizotypal personality features in nonpsychotic rela-tives of schizophrenic patients. Am J Psychiatry 1998;155: 1214–20.
16. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull 1987;13:261–76.
17. Cheng JJ, Ho H, Chang CJ, et al. Positive and Negative Syndrome Scale (PANSS): establishment and reliability study of a Mandarin Chinese language version. Chin Psychiatry 1996;10:251–8.
18. Chouinard G, Ross-Chouinard A, Annable L, Jones B. The Extrapyramidal Symptom Rating Scale. Can J Neuroscience 1980;(7):233.
19. Andia AM, Zisook S, Heaton RK, et al. Gender differences in schizophrenia. J Nerv Ment Dis 1995;183:522–8. 20. Szeszko PR, Gunning-Dixon F, Goldman RS, et al. Lack of
normal association between cerebellar volume and neu-ropsychological functions in first-episode schizophrenia. Am J Psychiatry 2003;160:1884–7.
21. Saykin AJ, Shtasel DL, Gur RE, et al. Neuropsychological deficits in neuroleptic naive patients with first-episode schizophrenia. Arch Gen Psychiatry 1994;51:124–31. 22. Hill SK, Beers SR, Kmiec JA, et al. Impairment of verbal
memory and learning in antipsychotic-naive patients with first-episode schizophrenia. Schizophr Res 2004;68:127–36. 23. Cirillo MA, Seidman LJ. Verbal declarative memory dysfunc-tion in schizophrenia: from clinical assessment to genetics and brain mechanisms. Neuropsychol Rev 2003;13:43–77. 24. Gur RE, Cowell PE, Latshaw A, et al. Reduced dorsal and or-bital prefrontal gray matter volumes in schizophrenia. Arch Gen Psychiatry 2000;57:761–8. [Erratum in: Arch Gen Psychiatry 2000;57:858.]
25. Seidman LJ, Yurgelun-Todd D, Kremen WS, et al. Relation-ship of prefrontal and temporal lobe MRI measures to neu-ropsychological performance in chronic schizophrenia. Biol Psychiatry 1994;35:235–46.
26. Mohamed S, Paulsen JS, O’Leary D, et al. Generalized cognitive deficits in schizophrenia: a study of first-episode patients. Arch Gen Psychiatry 1999;56:749–54.
27. Schatz J. Cognitive processing efficiency in schizophrenia: generalized vs. domain specific deficits. Schizophr Res 1998;30:41–9.
28. Brebion G, Gorman JM, Malaspina D, et al. Clinical and cognitive factors associated with verbal memory task per-formance in patients with schizophrenia. Am J Psychiatry 2001;158:758–64.
29. Heinrichs RW, Ruttan L, Zakzanis KK, Case D. Parsing schiz-ophrenia with neurocognitive tests: evidence of stability and validity. Brain Cognition 1997;35:207–24.
30. Jaeger J, Czobor P, Berns SM. Basic neuropsychological di-mensions in schizophrenia. Schizophr Res 2003;65:105–16. 31. Friis S, Sundet K, Rund BR, et al. Neurocognitive dimensions characterising patients with first-episode psychosis. Br J Psychiatry 2002;43:S85–90.
32. Hill SK, Ragland JD, Gur RC, Gur RE. Neuropsychological profiles delineate distinct profiles of schizophrenia, an in-teraction between memory and executive function, and uneven distribution of clinical subtypes. J Clin Exp Neuro-psychology 2002;24:765–80.
33. Cohen AS, Docherty NM. Deficit versus negative syndrome in schizophrenia: prediction of attentional impairment. Schizophr Bull 2004;30:827–35.
34. Bilder R, Goldman R, Robinson D, et al. Neuropsychology of first-episode schizophrenia: initial characterization and clinical correlates. Am J Psychiatry 2000;157:549–59. 35. Harvey P, Lombardi J, Kincaid M, et al. Cognitive
function-ing in chronically hospitalized schizophrenic patients: age-related changes and age disorientation as a predictor of impairment. Schizophr Res 1995;17:15–24.
36. Kurtz MM. Neurocognitive impairment across the lifespan in schizophrenia: an update. Schizophr Res 2005;74:15–26. 37. Chen EY, Lam LC, Chen RY, Nguyen DG. Negative symp-toms, neurological signs and neuropsychological impairments in 204 Hong Kong Chinese patients with schizophrenia. Br J Psychiatry 1996;168:227–33.
38. Mahurin RK, Velligan DI, Miller AL. Executive-frontal lobe cognitive dysfunction in schizophrenia: a symptom subtype analysis. Psychiat Res 1998;79:139–49.
39. Censits DM, Ragland JD, Gur RC, Gur RE. Neuropsycho-logical evidence supporting a neurodevelopmental model of schizophrenia: a longitudinal study. Schizophr Res 1997; 24:289–98.
40. Takahashi H, Iwase M, Nakahachi T, et al. Spatial working memory deficit correlates with disorganization symptoms and social functioning in schizophrenia. Psychiat Clin Neuro-sciences 2005;59:453–60.
41. Shean G, Burnett T, Eckman FS. Symptoms of schizophrenia and neurocognitive test performance. J Clin Psychology 2002;58:723–31.
42. Heydebrand G, Weiser M, Rabinowitz J, et al. Correlates of cognitive deficits in first episode schizophrenia. Schizophr Res 2004;68:1–9.
43. Bilder RM, Mukherjee S, Rieder RO, Pandurangi AK. Symp-tomatic and neuropsychological components of defect states. Schizophr Bull 1985;11:409–19.
44. Kremen WS, Seidman LJ, Faraone SV, et al. The paradox of normal neuropsychological function in schizophrenia. J Abn Psychology 2000;109:743–52.
45. Green MF, Braff DL. Translating the basic and clinical cogni-tive neuroscience of schizophrenia to drug development and clinical trials of antipsychotic medications. Biol Psychiatry 2001;49:374–84.
46. Dickinson D, Coursey RD. Independence and overlap among neurocognitive correlates of community functioning in schizophrenia. Schizophr Res 2002;56:161–70.
47. Evans JD, Heaton RK, Paulsen JS, et al. The relationship of neuropsychological abilities to specific domains of functional capacity in older schizophrenia patients. Biol Psychiatry 2003;53:422–30.
48. Addington J, Addington D. Neurocognitive and social functioning in schizophrenia: a 2.5 year follow-up study. Schizophr Res 2000;44:47–56.
49. Green MF. What are the functional consequences of neuro-cognitive deficits in schizophrenia? Am J Psychiatry 1996; 153:321–30.
50. Addington J, Addington D. Neurocognitive and social functioning in schizophrenia. Schizophr Bull 1999;25: 173–82.