Author's personal copy
Research Letter
Cytogenetic discrepancy between uncultured amniocytes and cultured
amniocytes in mosaic isochromosome 20q detected at amniocentesis
Chih-Ping Chen
a,b,c,d,e,f,*
, Jui-Der Liou
g,h, Chi-Hsin Chiang
g,h, Yi-Ning Su
i,
Schu-Rern Chern
b, Fuu-Jen Tsai
d,j,k, Pei-Chen Wu
a, Yu-Ting Chen
b,
Chen-Chi Lee
a, Wen-Lin Chen
a, Wayseen Wang
b,la
Department of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, Taiwan b
Department of Medical Research, Mackay Memorial Hospital, Taipei, Taiwan c
Department of Biotechnology, Asia University, Taichung, Taiwan d
School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan eInstitute of Clinical and Community Health Nursing, National Yang-Ming University, Taipei, Taiwan
fDepartment of Obstetrics and Gynecology, National Yang-Ming University, Taipei, Taiwan gChang Gung University College of Medicine, Taoyuan, Taiwan
hDepartment of Obstetrics and Gynecology, Chang Gung Memorial Hospital, Taipei, Taiwan iDepartment of Medical Genetics, National Taiwan University Hospital, Taipei, Taiwan jDepartment of Medical Genetics, China Medical University Hospital, Taichung, Taiwan kDepartment of Medical Research, China Medical University Hospital, Taichung, Taiwan
lDepartment of Bioengineering, Tatung University, Taipei, Taiwan Accepted 14 February 2011
A 31-year-old, gravida 2, para 1, woman underwent amnio-centesis at 16 weeks of gestation at a medical center because of an abnormal maternal serum screening result (Down syndrome risk¼ 1/52). In 4 of 17 separated colonies of the cultured amniocytes, an abnormal karyotype of 46,XY,i(20)(q10) was noted, whereas the other 13 colonies had a karyotype of 46,XY. The conventional cytogenetic result of the cultured amniocytes thus was 46,XY,i(20)(q10)[4]/46,XY[13]. The parental karyo-types were normal. The prenatal ultrasound findings were unremarkable. She was referred to the hospital for genetic counseling and repeated amniocentesis. Array comparative genomic hybridization (aCGH), fluorescence in situ hybrid-ization (FISH), and quantitative fluorescent polymerase chain reaction (QF-PCR) were applied to both uncultured and cultured amniocytes after repeated amniocentesis. Molecular cytogenetic analyses of the uncultured amniocytes revealed no abnormal findings. aCGH of the uncultured amniocytes did not manifest any genomic imbalance in chromosome 20
(Fig. 1). Polymorphism DNA marker investigation of the
uncultured amniocytes using microsatellite markers specific for chromosome 20q revealed a diallelic pattern and seemingly equal biparental inheritance of chromosome 20q (Fig. 2).
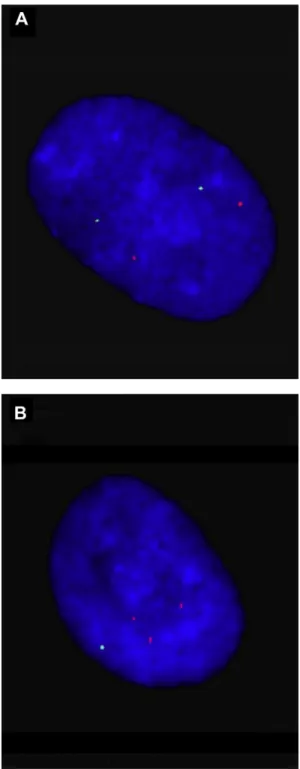
Interphone FISH study of the uncultured amniocytes using 20q13.33-specific probe (RP11-266K16) found two signals in all 50 uncultured amniocytes, indicating no evidence of isochromosome 20q (Fig. 3). On the other hand, molecular cytogenetic analyses of the cultured amniocytes revealed abnormal findings. aCGH of the cultured amniocytes man-ifested genomic imbalance in chromosome 20 with a deletion in chromosome 20p and a duplication in chromosome 20q
(Fig. 1). QF-PCR analysis of the cultured amniocytes revealed
a diallelic pattern with unequal biparental inheritance of chromosome 20q with a dosage ratio of 1:1.3 (maternal alle-le:paternal allele) (Fig. 2). Interphase FISH study of the cultured amniocytes found three 20q-specific signals in 7 of 25 (28%) cultured amniocytes, indicating the presence of mosaic isochromosome 20q in cultured amniocytes (Fig. 4). In 8 of 24 (33.3%) separated colonies of the cultured amniocytes, an abnormal karyotype of 46,XY,i(20)(q10) was noted, whereas 16 of 24 (66.7%) colonies had a karyotype of 46,XY. The conventional cytogenetic result of the cultured amniocytes in repeated amniocentesis was 46,XY,i(20)(q10) [8]/46,XY[16] (Fig. 5). In this case, cytogenetic discrepancy between uncultured and cultured amniocytes in mosaic isochromosome 20q was evident. The woman decided to continue the pregnancy. Level II obstetric ultrasonography revealed normal fetal growth biometry, a normal fetal craniofacial profile, and no structural abnormalities. At 40
* Corresponding author. Department of Obstetrics and Gynecology, Mackay Memorial Hospital, 92, Section 2, Chung-Shan North Road, Taipei, Taiwan.
E-mail address:[email protected](C.-P. Chen).
Available online at www.sciencedirect.com
Taiwanese Journal of Obstetrics & Gynecology 50 (2011) 245e248
www.tjog-online.com
1028-4559/$ - see front matter CopyrightÓ 2011, Taiwan Association of Obstetrics & Gynecology. Published by Elsevier Taiwan LLC. All rights reserved. doi:10.1016/j.tjog.2011.04.006
Author's personal copy
weeks of gestation, a 3,395-g healthy male baby was delivered uneventfully. Cytogenetic analysis of the blood lymphocytes (100 cells) of the baby revealed a karyotype of 46,XY. At a routine pediatric follow-up examination at 3 months of age, the infant showed normal growth and normal psychomotor development.
The present case provides evidence for cytogenetic discrep-ancy between uncultured and cultured amniocytes in mosaic isochromosome 20q detected at amniocentesis and shows that mosaic isochromosome 20q in cultured amniocytes can be a tissue-limited cell culture artifact. Our observation may explain the clinical findings that most reported cases with prenatally detected mosaicism for isochromosome 20q resulted in normal pregnancy outcomes[1e3]. Robinson et al[3]suggested that the isochromosome 20q presumably arises through a postzygotic error and can persist only in a few specific cell types.
Although there is a predominantly normal outcome of prenatally detected isochromosome 20q, genetic counseling for mosaic isochromosome 20q detected at amniocentesis still should be done cautiously. Detailed fetal ultrasound
evaluation and molecular cytogenetic investigation of uncul-tured amniocytes may be helpful for genetic counseling when parents decide to continue the pregnancy. To date, at least four reports with mosaic isochromosome 20q detected at amnio-centesis have been described to be associated with phenotypic abnormalities [1,4e6]. Chevrons et al [4] reported prenatal diagnosis of mosaic isochromosome 20q with a mosaic chro-mosome constitution of 8 of 13 colonies of cultured amnio-cytes having the abnormal karyotype of 46,XX,i(20q). The fetus was associated with diaphragmatic hernia, ventricular dilation, a large calvarium, anophthalmia, craniofacial dys-morphism, and a single umbilical artery. Pfeiffer et al [5]
reported prenatal diagnosis of mosaic isochromosome 20q with a mosaic chromosome constitution of 24 of 26 colonies of cultured amniocytes having the abnormal karyotype of 46,XY,i(20q). The blood, placenta, and skin had the karyotype of 46,XY. The umbilical cord had the karyotype of 46,XY,i(20q)[13]/46,XY[18]. FISH of interphase nuclei pre-sented three signals of 20q13-specific probe in 6% of buccal epithelium and in 13.7% of urinary sediment. The infant
Fig. 1. BAC-based aCGH of (A) uncultured amniotic fluid cells and (B) cultured amniotic fluid cells using CMDX BAC-based aCGH CA3000 Chips (CMDX, Irvine, CA, USA) shows no genomic imbalance in chromosome 20 of uncultured amniocytes and genomic imbalance in chromosome 20 of cultured amniocytes with a deletion in chromosome 20p and a duplication in chromosome 20q. aCGH¼ array comparative genomic hybridization; BAC ¼ bacterial artificial chromosome. 246 C.-P. Chen et al. / Taiwanese Journal of Obstetrics & Gynecology 50 (2011) 245e248
Author's personal copy
manifested with scars on the scalp, orbital cysts, coloboma of the papilla, and dyssegmentation of the thoracic spine. Chen
[1] reported prenatal diagnosis of mosaic isochromosome 20q with a mosaic chromosome constitution of 14 of 28 colonies of cultured amniocytes having the abnormal karyo-type of 46,XX,i(20q). The blood, placenta, skin, and liver had the karyotype of 46,XX. The infant manifested with
Fig. 2. Representative electrophoretograms of quantitative fluorescent poly-merase chain reaction assays. The marker D20S606 (20q13.2) shows two peaks (maternal:paternal, 148 bp:164 bp) of equal fluorescent activity from two different parental alleles in uncultured amniocytes and two peaks of unequal fluorescent activity in cultured amniocytes with a dosage ratio of 1:1.3 (maternal:paternal). (A) Father; (B) mother; (C) amniotic fluid cells (uncul-tured); (D) amniotic fluid cells (cultured).
Fig. 3. Fluorescence in situ hybridization analysis of uncultured interphase amniocytes using a 20q-specific probe RP11-266K16 (20q13.33) (spectrum red) and a 6q-specific probe RP11-448N11 (6q11.1eq11.2) (spectrum green) as internal control shows two signals of the 20q-specific probe.
Fig. 4. Fluorescence in situ hybridization analysis of cultured interphase amniocytes using a 20q-specific probe RP11-266K16 (20q13.33) (spectrum red) and a 20p-specific probe RP11-530N10 (20p13) (spectrum green) shows (A) a normal cell with two normal chromosomes 20 (two red signals and two green signals) and (B) an abnormal cell with isochromosome 20q (three red signals and one green signal).
247 C.-P. Chen et al. / Taiwanese Journal of Obstetrics & Gynecology 50 (2011) 245e248
Author's personal copy
arthrogryposis multiplex congenita, amyoplasia, and a single umbilical artery, which were likely a casual relationship with the mosaic i(20q). Goumy et al[6]reported a prenatal diagnosis of mosaic isochromosome 20q with a mosaic chromosome constitution of 14 of 15 colonies of cultured amniocytes having the abnormal karyotype of 46,XY,i(20q). Interphase FISH study revealed two signals of 20q12-specific probe in all 20 uncul-tured amniocytes and three signals in 24% of 260 culuncul-tured amniocytes. aCGH study of cultured amniocytes revealed no genomic imbalance. The pregnancy was terminated, and the fetus manifested with hydrocephalus, spinal malformation, craniofacial dysmorphism, and clubfeet. However, there was no successful fetal tissue sampling for confirmation. The pheno-typeegenotype correlation in that case was inconclusive.
This is the first report of prenatal molecular cytogenetic investigation of mosaic isochromosome 20q using interphase FISH, aCGH, and QF-PCR on both uncultured and cultured amniocytes. This report confirms that cytogenetic discrepancy occurs between uncultured and cultured amniocytes in mosaic isochromosome 20q detected at amniocentesis and implies that mosaic isochromosome 20q detected at amniocentesis can be a cell culture artifact. We suggest that prenatal diagnosis of mosaic isochromosome 20q by amniocentesis without fetal anomalies and without mosaic i(20q) on uncultured amnio-cytes is likely to result in a normal fetal outcome.
Acknowledgments
This work was supported by research grants 96-2314-B-195-008-MY3, 97-2314-B-195-006-MY3, and NSC-99-2628-B-195-001-MY3 from the National Science Council and MMH-E-100-04 from Mackay Memorial Hospital, Taipei, Taiwan.
References
[1] Chen C-P. Detection of mosaic isochromosome 20q in amniotic fluid in a pregnancy with fetal arthrogryposis multiplex congenita and normal karyotype in fetal blood and postnatal samples of placenta, skin, and liver. Prenat Diagn 2003;23:85e7.
[2] Chen C-P. Second-trimester diagnosis of mosaic idic(20)(p11) confined to amniocytes without an abnormal phenotype. Genet Couns 2003;14:439e41. [3] Robinson WP, McGillivray B, Friedman JM. Pregnancy and postnatal outcome of mosaic isochromosome 20q. Prenat Diagn 2007;27:143e5. [4] Chernos JE, McLeod DR, Cox DM. Prenatal diagnosis of mosaic
isochromosome 20q associated with abnormal phenotype. Am J Hum Genet 1992;51:A288.
[5] Pfeiffer RA, Ulmer R, Rauch A, Trautmann U, Beinder E, Rupprecht T, et al. True fetal mosaicism of an isochromosome of the long arm of a chromosome 20: the dilemma persists. Prenat Diagn 1997;17:1171e5. [6] Goumy C, Beaufre`re AM, Francannet C, Tchirkov A, Laurichesse Delmas H,
Geissler F, et al. Prenatal detection of mosaic isochromosome 20q: a fourth report with abnormal phenotype. Prenat Diagn 2005;25:653e5.
Fig. 5. (A) A karyotype of 46,XY. (B) A karyotype of 46,XY,i(20)(q10). (C) Corresponding metaphase FISH finding of a cultured amniocyte with 46,XY. (D) Corresponding metaphase FISH finding of a cultured amniocyte with 46,XY,i(20)(q10). Red signal: RP11-266K16 (20q13.33); green signal: RP11-530N10 (20p13). FISH¼ fluorescence in situ hybridization.