R
doi: 10.2306/scienceasia1513-1874.2010.36.130
Association of toll-like receptor 4 gene polymorphisms
with primary membranous nephropathy in a high
prevalence renal disease area in Taiwan
Shih-Yin Chena,b, Wen-Chi Chena,b, Yung-Hsiang Chenb, Cheng-Hsu Chenc, Yu-Chuen Huanga,b, Po-Hsun Huangd, Yi-Wen Linb, Huey-Yi Chena,b, Wen-Ling Liaob, Fuu-Jen Tsaia,b,∗
a Genetics Centre, Department of Medical Research, Department of Urology,
Department of Obstetrics and Gynecology, and Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan
b Graduate Institute of Integrated Medicine, Graduate Institute of Acupuncture Science,
School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan
c Division of Nephrology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung,
Taiwan
d Division of Cardiology, Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan ∗Corresponding author, e-mail: [email protected]
Received 3 Feb 2010 Accepted 7 May 2010 ABSTRACT: Membranous glomerulonephritis (MGN) is one of the most common causes of idiopathic nephrotic syndrome in adults. TLR4 gene polymorphisms have been reported to be associated with many inflammatory diseases. The objective of this study was to clarify the relationship between TLR4 gene polymorphisms and the pathogenesis of MGN. We recruited a cohort of 134 biopsy-diagnosed MGN patients and 263 healthy subjects that served as controls. Genotyping of TLR4 gene polymorphisms was performed using allele-specific polymerase chain reaction methods. We then analysed associations between TLR4 gene polymorphisms and clinical manifestations and pathogenesis of MGN. There was statistically significant difference of TLR4 gene rs10983755 A/G (p < 0.001) and rs1927914 A/G (p < 0.05) polymorphisms between controls and patients with MGN. The distributions of rs10759932 C/T and rs11536889 C/T polymorphisms were significantly different. A higher level of triglyceride was found in the non-GG group than in the GG group. The genotype of the non-AA group had a significantly higher ratio of proteinuria than that of the AA group. In addition, the distribution of haplotype frequencies of the TLR4 gene in 4 genetic variants revealed no statistical difference between normal patients and controls. The results demonstrated that patients with MGN have a different genotype distribution of the TLR4 gene from the normal controls. Our observations suggest that those polymorphisms contribute to the genetic background of MGN pathogenesis.
KEYWORDS: glomerulonephritis, inflammation, proteinuria, triglyceride
INTRODUCTION
Membranous glomerulonephritis (MGN) is a common primary or idiopathic nephropathy1,2. MGN also appears as a disease secondary to other conditions (approximately 25%), mainly infections, neoplasms, and systemic lupus erythematosus (SLE)3. Although
inflammatory cells are not usually detected, an in-flammatory process is evident of trapping of immune complexes. Therefore, inflammation is highly related to this disease4. MGN may be a cause of chronic
kidney disease and a final result of end-stage renal disease (ESRD)5. Taiwan has the highest prevalence
of ESRD in the world and MGN may be one of the causes4,6,7. The study of inflammatory factors
associated with MGN is helpful in elucidating and preventing of ESRD8.
MGN is an immune complexes mediated disease as evidenced by the presence of immunoglobulins and complement components in capillary walls (sub-epithelial), and the morphological and immunopatho-logical similarities between the experimental MGN and immunological glomerular diseases9. However,
the aetiology and origin of the antigens that cause MGN remain unclear. The deposits may come from circulating immune complexes, form in situ, or come from foreign antigens previously deposited there10.
Although MGN is a multi-factorial disease, an inflam-matory pathway might play an important role in the pathogenesis of MGN4,9.
Toll-like receptors (TLRs), a key element of hu-man innate immune response, up-regulate proinflam-matory cytokines and co-stimulatory molecules as a first line host defence11. TLRs have been identified
as key components of the pathogen-recognition pro-cess that mediates inflammatory responses12. TLR4 interacts with some ligands such as heat-shock pro-teins13–15, hyaluronan, fibronectin, fibrinogen, hep-aran lung surfactant protein-A16, and high mobility group box 117. Polymorphisms of the TLR4 gene have
been reported to be associated with many inflamma-tory diseases and the formation of cancers such as Crohn’s disease18, ulcerative colitis19, and cervical
cancer20. However, there are few reports about TLR4
in MGN21,22. In this study, we investigated the
association of TLR4 gene variants in Taiwan MGN patients by comparing them with matched controls.
MATERIALS AND METHODS Study population
A total of 134 patients with previously renal biopsy-approved MGN and 263 healthy subjects serving as controls were recruited in Taichung Veterans General Hospital, Taiwan. Patients with malignancy, chronic infection diseases (including infections with hepatitis B and C viruses), lupus nephritis, or drug-induced secondary MGN were excluded from the study. The general data (gender, body weight, systolic/diastolic pressure, and body height) and medical information (duration of follow-up, renal failure, and herbal use, etc.) of all the patients were reviewed. Patient char-acteristics included demographic variables, clinical and laboratory data in the disease courses, vascular events (cardiovascular disease and peripheral vascu-lar events), and treatment regimens as well as their responses. The study was approved by the Institu-tional Review Board (No. C08159) of China Medical University Hospital in adherence with the Declaration of Helsinki and all participating individuals signed an informed consent.
The selection of treatment modality, either sup-portive or aggressive with immunosuppressants was decided by the treating physician. The supportive therapy usually included diuretics, angiotensin con-verting enzyme inhibitors and/or angiotensin II recep-tor blockers dependening on patient symptoms. The immunosuppressive therapies were any of the follow-ing regimens: (1) prednisolone 1 mg/kg/day alone, (2) a six-month course of corticosteroids alternated with chlorambucil at dose of 0.2 mg/kg per day every other month4,23 or cyclophosphamide 1.5–2.0 mg/kg
per day, (3) cyclosporine A (CyA, Neoral, Norvatis)
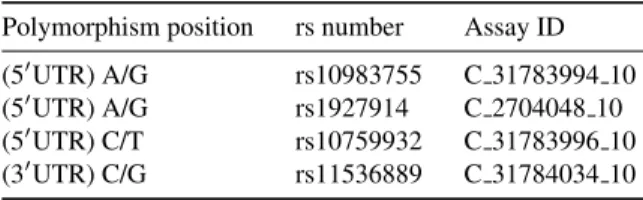
Table 1 Genetic polymorphism sites of TLR4 gene. Polymorphism position rs number Assay ID
(50UTR) A/G rs10983755 C 31783994 10
(50UTR) A/G rs1927914 C 2704048 10
(50UTR) C/T rs10759932 C 31783996 10
(30UTR) C/G rs11536889 C 31784034 10
3–5 mg/kg per day with or without prednisolone. Responses and outcomes
The responses to therapy were defined as the follows: (1) no response, (2) partial remission: a proteinuria reduction of more than 50% or a final proteinuria between 0.2 to 2.0 g/day, and (3) complete remission: proteinuria less than 0.2 g/day. The ‘progression of renal disease’ was defined as a doubling of baseline serum creatinine (Cr) values or ESRD. ESRD was defined as patient requiring renal replacement therapy. Genomic DNA extraction and determination of TLR4 polymorphisms
Genomic DNA was extracted from peripheral blood leukocytes (Genomic DNA kit, Roche). Genotypes of four SNPs (rs10983755, rs1927914, and rs10759932) representing 50UTR A/G, 50UTR A/G, and 50UTR C/T polymorphism, respectively, and rs11536889 30UTR C/G polymorphism in the TLR4 gene (Table 1) were performed using the SNP genotyping assay (Applied Biosystems Inc. (ABI), Foster City). The primers and probes to detect for SNPs were from the ABI assay on demand kit. Reactions were carried out according to the manufacturer’s protocol. Briefly, PCR was performed in the presence of 2× TaqMan Universal PCR Master Mix (ABI), assay mix (Applied Biosystems) and genomic DNA (15 ng). The probe for fluorescence signal detection was from the ABI Prism 7900 Real Time PCR System.
Statistical analyses
The Hardy-Weinberg equilibrium was tested for each marker using a χ2-test. A χ2test or Fisher’s exact test were used to determine statistically significant differ-ences in allele/genotype frequencies. The haplotype combination of 4 polymorphisms in the TLR4 gene was estimated using HAPLOVIEW version 4.1 based on an accelerated EM algorithm24. The differences in
the distribution of the haplotype frequencies between the two groups were assessed using a χ2-test. Odds
ratios (ORs) and 95% confidence intervals (95% CIs) were obtained using logistic regressions to determine associations. All data were analysed with SPSS 15.0 and p < 0.05 was considered statistically significant.
Table 2 Genotypic and allelic frequencies of TLR4 genetic polymorphisms in the patients with MGN and controls.
dbSNP ID Patients Control OR (95% CI) p value with MGN rs10983755 n = 134 n = 265 Genotype AA 8 (6.0) 12 (4.5) 2.03 (0.78–5.23) 0.0006 AG 75 (56.0) 98 (37.0) 2.33 (1.50–3.60) GG 51 (38.1) 155 (58.5) Reference Allele freq. A 91 (34.0) 122 (23.0) 1.72 (1.24–2.38) 0.001 G 177 (66.8) 408 (77.0) Reference rs1927914 n = 134 n = 265 Genotype AA 44 (32.8) 121 (45.7) Reference 0.045 AG 67 (50.0) 104 (39.2) 1.77 (1.12–2.81) GG 23 (17.2) 40 (15.1) 1.58 (0.85–2.93) Allele freq. A 155 (57.8) 346 (65.3) Reference 0.040 G 113 (42.2) 184 (34.7) 1.37 (1.01–1.85) rs10759932 n = 134 n = 263 Genotype CC 8 (6.0) 12 (4.6) 1.47 (0.57–3.75) 0.465 CT 56 (41.8) 97 (36.9) 1.27 (0.82–1.96) TT 70 (52.2) 154 (58.6) Reference Allele freq. C 72 (26.9) 121 (23.0) 1.23 (0.88–1.72) 0.230 T 196 (73.1) 405 (77.0) Reference rs11536889 n = 133 n = 261 Genotype CC 6 (4.5) 11 (4.2) 1.16 (0.42–3.26) 0.560 CT 45 (33.8) 75 (28.7) 1.28 (0.81–2.01) TT 82 (61.7) 175 (67.0) Reference Allele freq. C 57 (21.4) 97 (18.6) 1.19 (0.83–1.72) 0.341 T 209 (78.6) 425 (81.4) Reference RESULTS
There was a statistically significant difference of the TLR4 gene rs10983755 A/G (p < 0.001) and rs1927914 A/G (p < 0.05) polymorphisms between controls and patients with MGN (Table 2). The fre-quency of the ‘AA’ genotype in patients with MGN (6.0%) was higher than in the control group (4.5%). By comparing with ‘GG’ genotype, the OR of ‘AA’ was 2.03 (95% CI = 0.78–5.23). The frequency of the ‘AG’ genotype in patients with MGN (56.0%) was also higher than in the control group (37.0%). By comparing with the ‘GG’ genotype, the OR of AG was 2.33 (95% CI = 1.50–3.60). The allelic frequency of ‘A’ in patients with MGN (34.0%) was higher than in the control (23.0%). The OR for the ‘A’ allele was 1.72 (95% CI = 1.24–2.38, p = 0.001).
For the distribution of rs1927914 A/G polymor-phism, the ‘GG’ genotype was higher in the patient’s group (17.2%) than in the control (15.1%) with an OR of 1.58 (95% CI = 0.85–2.93). The frequency of the the ‘AG’ genotype in patients with MGN (50.0%) was also higher than in the control group (39.2%) with an OR of 1.77 (95% CI = 1.12–2.81). The allelic
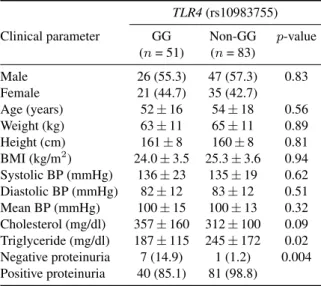
Table 3 Characteristics of clinical parameters for the GG and non-GG (rs10983755) of polymorphisms of the TLR4 gene in patients with MGN.
TLR4(rs10983755)
Clinical parameter GG Non-GG p-value
(n = 51) (n = 83) Male 26 (55.3) 47 (57.3) 0.83 Female 21 (44.7) 35 (42.7) Age (years) 52 ± 16 54 ± 18 0.56 Weight (kg) 63 ± 11 65 ± 11 0.89 Height (cm) 161 ± 8 160 ± 8 0.81 BMI (kg/m2) 24.0 ± 3.5 25.3 ± 3.6 0.94 Systolic BP (mmHg) 136 ± 23 135 ± 19 0.62 Diastolic BP (mmHg) 82 ± 12 83 ± 12 0.51 Mean BP (mmHg) 100 ± 15 100 ± 13 0.32 Cholesterol (mg/dl) 357 ± 160 312 ± 100 0.09 Triglyceride (mg/dl) 187 ± 115 245 ± 172 0.02 Negative proteinuria 7 (14.9) 1 (1.2) 0.004 Positive proteinuria 40 (85.1) 81 (98.8)
Data are expressed as n (%) or mean ± SD BMI = body mass index, BP = blood pressure
frequency of ‘G’ in patients with MGN (42.2%) was higher than the control (34.7%) with an OR of 1.72 (95% CI = 1.01–1.85, p < 0.05).
The distribution of rs10759932 C/T and rs11536889 C/T polymorphisms were also shown. There was no significant difference of genotype frequency between these two groups.
The characteristics of clinical parameters in TLR4 gene (rs10983755) A/G polymorphism revealed no difference except triglyceride (p = 0.024) between GG and non-GG genotype in MGN patients (Table 3). A higher level of triglyceride was found in the non-GG group than in the non-GG group (245 ± 172 and 187 ± 115 mg/dl, respectively). Non-GG genotype (98.8%) had a significantly (p = 0.004) higher per-centage of proteinuria than the GG genotype (85.1%). Other parameters including renal failure, mortality, vascular event, CCr, C3, C4, immunoglobulins, re-sults of biopsy (fibrosis or intima fibroplasia), disease progression and chronic kidney disease grade did not differ for the GG and non-GG genotype of rs10983755 in the TLR4 gene.
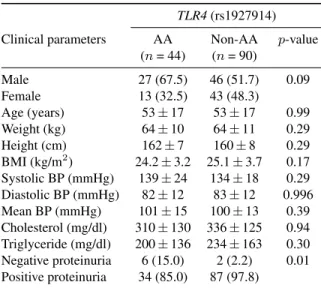
There was also a statistically significant differ-ence between the rs1927914 A/G polymorphism and the proteinuria parameter (Table 4). The genotype of the non-AA group (97.8%) had a significantly (p = 0.011) higher ratio of proteinuria than the AA group (85.0%). No statistically significant differences of rs10759932 C/T and rs11536889 C/T polymorphisms between TT and non-TT genotypes were found in the
Table 4 Characteristics of clinical parameters between AA and non AA (rs1927914) polymorphism of TLR4 gene in patients with MGN.
TLR4(rs1927914)
Clinical parameters AA Non-AA p-value
(n = 44) (n = 90) Male 27 (67.5) 46 (51.7) 0.09 Female 13 (32.5) 43 (48.3) Age (years) 53 ± 17 53 ± 17 0.99 Weight (kg) 64 ± 10 64 ± 11 0.29 Height (cm) 162 ± 7 160 ± 8 0.29 BMI (kg/m2) 24.2 ± 3.2 25.1 ± 3.7 0.17 Systolic BP (mmHg) 139 ± 24 134 ± 18 0.29 Diastolic BP (mmHg) 82 ± 12 83 ± 12 0.996 Mean BP (mmHg) 101 ± 15 100 ± 13 0.39 Cholesterol (mg/dl) 310 ± 130 336 ± 125 0.94 Triglyceride (mg/dl) 200 ± 136 234 ± 163 0.30 Negative proteinuria 6 (15.0) 2 (2.2) 0.01 Positive proteinuria 34 (85.0) 87 (97.8)
Table 5 Distribution of TLR4 haplotype frequencies in the patients with MGN and controls.
Haplotypea Patient with Control OR (95% CI) p-value MGNb (n = 138) (n = 265) G-A-T-G 32.0% 37.9% 0.77 (0.57–1.06) 0.10 A-G-C-G 26.0% 22.5% 1.22 (0.87–1.72) 0.27 G-A-T-C 20.3% 23.9% 0.80 (0.56–1.15) 0.24 G-G-T-G 13.3% 14.8% 0.89 (0.58–1.36) 0.57 aOrder of single nucleotide polymorphisms
compris-ing the TLR4 haplotypes: rs10983755, rs1927914, rs10759932, and rs11536889.
bPercentages may not add to 100% because of the
pres-ence of rare haplotypes (< 5%) not presented here.
clinical parameters (data not shown).
In addition, compared with the haplotype fre-quencies between patient and control groups, the distribution of haplotype frequencies of TLR4 gene in 4 genetic variants revealed no statistical difference between MGN patients and controls (Table 5). DISCUSSION
MGN is a multiple factorial disease with immunologic expressions that may arise in genetically susceptible individuals4,9. However, little information is available
for the polymorphic gene sequences of inflamma-tory genes known to be involved in pathogenesis of MGN25–27. In this study, we focused on the
vari-ants of TLR4 which had previously been investigated for diabetic neuropathy28, severe virus infections29,
cervical cancer susceptibility30, and chronic allograft
nephropathy31. According to our data, we found a
statistically significant association between MGN and the TLR4 gene, rs10983755 A/G, and rs1927914 A/G polymorphisms.
The genetic basis of MGN is not fully under-stood. MGN patients show significantly lower re-nal expression of tumour necrosis factor (TNF-α) than patients with minimal change disease, diabetes nephropathy, IgA nephropathy, or other diseases32. A recent report shows that the TNF-α gene G-308A polymorphism is a risk factor for the devel-opment of MGN33. Other reports show no
rela-tionship between severity or progression of the dis-ease and any of the tested single genotypes [HLA-DR3, TNF-α gene G-308A, angiotensin-converting enzyme insertion/deletion (ACE I/D), angiotensin II receptor 1 (AT1R 1166A/C), angiotensinogen (AGT M235T), and NOS (ecNOS4b/a)]34,35, perhaps due to
the smaller number of patients and short observation periods.
The renal function changes and the course of MGN are more strongly correlated with the degree of tubulointerstitial damage than with the extent of the glomerular lesion36. However, the pathogenesis of the interstitial inflammation and fibrosis is unclear. The most frequent presentation is proteinuria in the nephrotic range, with or without the other findings of the complete nephrotic syndrome. A variable per-centage of cases present as asymptomatic proteinuria, with microscopic haematuria in most of the patients, but macrohaematuria is rare. Exceptionally it can appear with isolated haematuria. The renal function can be slightly altered at the time of the diagnosis in many cases, but renal failure is unusual at presenta-tion. Furthermore, MGN may be influenced by risk factors such as microalbuminuria or hypoglycaemia. Because these risk factors were found to be distributed differently in the groups (TLR4 gene rs10983755 A/G and rs1927914 A/G) in this study, it seems that the effects of these TLR4 genotypes on MGN are related to these risk factors in these patients.
The amino acid polymorphisms determine the differences in the structure and thus the pattern recog-nition of the TLR4 receptor37. One might suggest that
an abnormality in the TLR regulation might increase the susceptibility for diseases because of a reduced defence against invading pathogens38. Diagnosis of
MGN can only be made after excluding secondary causes. Therefore, for proper diagnosis, investigations based on history, serology, and histology are equally important as a deficiency could arise at any level. MGN has a histological appearance, which could be due to factors such as heavy metal exposure, hepatitis B or C39,40, Epstein-Barr virus41, parasites,
Heli-cobacter pylori infection42, SLE, or even neoplastic
conditions43. To date, no data are available
concern-ing the function and expression of TLR4 in MGN. The pattern recognition receptor TLR4 is known to activate the proinflammatory transcription factor (NF)-κB and subsequent gene expression of NF-κB-regulated genes such as cytokines and adhesion molecules. This indicates that a TLR-4 polymorphism that prevents ligand binding and subsequent cellular signalling would result in lower NF-κB activation and subsequent NF-κB-dependent proinflammatory gene expression44. Hence, further studies are required to
show whether the polymorphisms are associated with a reduced activation of NF-κB, cytokine expression, and expression of adhesion molecules in MGN pa-tients.
In the present study, clinical features of 129 patients regarding vascular events (including unstable angina, coronary artery disease, ischaemic heart dis-ease, renal artery or vein thrombosis, deep vein throm-bosis and cranial vascular events) were available for review and data analysis. We observed all MGN pa-tients had high levels of cholesterol (reference: 150– 240 mg/dl) and 46% (59/129) MGN patients with vas-cular events problem (38% (18/47) with GG genotype at rs10983755; 50% (41/82) with Non-GG genotype at rs10983755). Comparing intergroup genotype (GG and Non-GG) gave statistically significant differences in triglycerides level for rs10983755 SNP (p = 0.024) in MGN patients. Data indicated triglycerides as ‘at-risk’ for vascular event development in MGN patients with Non-GG genotype. On the other hand, patients with MGN presented varied signs and symptoms, most commonly haematuria (75%), proteinuria (50%), and oedema (38%), consistent with other publications. Patients may have hypoalbuminaemia but most have hypercholesterolemia45. The value of proteinuria is as a marker for the MGN patients’ responses to therapy.
The interpretation of our study results is limited because the patients were recruited from just one centre in Taiwan. Our results strongly suggest a significant role of TLR4 gene polymorphisms in the risk of developing MGN of Taiwan. To the best of our knowledge, this is the first report on TLR4 gene polymorphisms in MGN patients. However, the identification of TLR4 as genetic risk factors for MGN susceptibility in Taiwan may be further evaluated as prognostic markers for predictive clinical testing in MGN worldwide, especially in ethnically disparate populations. Additionally, the study lacks functional genetics, the functional activity of the two identified polymorphisms in peripheral blood lymphocytes or the expression of TLR-4 in renal biopsies of MGN
patients and other glomerulopathies should be further studied. More recently, Hwang et al showed the importance of TLR4 in the pathogenesis of acute rejection in kidney transplantation, although there was no difference in transcriptional activity between wild-type and variant promoter of TLR446. This means that there is no functional significance in this promoter SNPs of TLR4. The DNA variant responsible for the difference in the genetic background of MGN pathogenesis remains to be identified.
In summary, our study firstly demonstrated the different genotype distribution between normal con-trols and patients with MGN of the TLR4 gene. The data show that TLR4 gene may be associated with a disease clinical cause of MGN especially with respect to the clinical parameters of proteinuria and serum triglyceride levels. The TLR4 gene is one of a number of important inflammatory related genes. Our obser-vations suggest that these polymorphisms contribute to the genetic background of MGN pathogenesis. Acknowledgements: This study was supported by grants from National Science Council of Taiwan (NSC 98-2314-B-039-023-MY3 and NSC 97-2320-B-039-022-MY3) and China Medical University (CMU97-CMC-003 and DMR-97-125), Taichung, Taiwan. The authors thank Miss Chi-Hsiang Wei for manuscript preparation.
REFERENCES
1. Appel AS, Appel GB (2009) An update on the use of mycophenolate mofetil in lupus nephritis and other primary glomerular diseases. Nat Clin Pract Nephrol 5, 132–42.
2. Mok CC (2009) Membranous nephropathy in systemic lupus erythematosus: a therapeutic enigma. Nat Rev Nephrol5, 212–20.
3. Glassock RJ (1992) Secondary membranous glomeru-lonephritis. Nephrol Dial Transplant 7 Suppl 1, 64–71. 4. Ponticelli C (2007) Membranous nephropathy.
J Nephrol20, 268–87.
5. Philibert D, Cattran D (2008) Remission of proteinuria in primary glomerulonephritis: we know the goal but do we know the price? Nat Clin Pract Nephrol 4, 550–9.
6. Chen KH, Chang CT, Hung CC (2006) Glomeru-lonephritis associated with chronic inflammatory de-myelinating polyneuropathy. Ren Fail 28, 255–9. 7. Yen TH, Huang JY, Chen CY (2003) Unexpected IgA
nephropathy during the treatment of a young woman with idiopathic dermatomyositis: case report and re-view of the literature. J Nephrol 16, 148–53.
8. Lo WY, Chen SY, Wang HJ, Shih HC, Chen CH, Tsai CH, et al (2010) Association between genetic polymorphisms of the NPHS1 gene and membranous
glomerulonephritis in the Taiwanese population. Clin Chim Acta411, 714–8.
9. Couser WG, Nangaku M (2006) Cellular and molecular biology of membranous nephropathy. J Nephrol 19, 699–705.
10. Ronco P, Debiec H (2006) New insights into the patho-genesis of membranous glomerulonephritis. Curr Opin Nephrol Hypertens15, 258–63.
11. Lee CH, Wu CL, Shiau AL (2010) Toll-like receptor 4 signaling promotes tumor growth. J Immunother 33, 73–82.
12. Medzhitov R, Janeway C, Jr (2000) The Toll receptor family and microbial recognition. Trends Microbiol 8, 452–6.
13. Lin FY, Chen YH, Chen YL, Wu TC, Li CY, Chen JW, et al (2007) Ginkgo biloba extract inhibits endotoxin-induced human aortic smooth muscle cell proliferation via suppression of toll-like receptor 4 expression and NADPH oxidase activation. J Agr Food Chem 55, 1977–84.
14. Lin FY, Chen YH, Tasi JS, Chen JW, Yang TL, Wang HJ, et al (2006) Endotoxin induces toll-like receptor 4 expression in vascular smooth muscle cells via NADPH oxidase activation and mitogen-activated protein kinase signaling pathways. Arterioscler Thromb Vasc Biol 26, 2630–7.
15. Lin FY, Chen YH, Lin YW, Tsai JS, Chen JW, Wang HJ, et al (2006) The role of human antigen R, an RNA-binding protein, in mediating the stabilization of toll-like receptor 4 mRNA induced by endotoxin: a novel mechanism involved in vascular inflammation. Arterioscler Thromb Vasc Biol26, 2622–9.
16. Beg AA (2002) Endogenous ligands of Toll-like re-ceptors: implications for regulating inflammatory and immune responses. Trends Immunol 23, 509–12. 17. Liu PL, Tsai JR, Hwang JJ, Chou SH, Cheng YJ, Lin
FY, et al (2009) HMGB1-Mediated MMP-9 Expression in Non-Small Cell Lung Cancer Contributes to Tumor Cell Invasiveness. Am J Respir Cell Mol Biol. 18. Zouiten-Mekki L, Kharrat M, Karoui S, Serghimi
M, Fekih M, Matri S, et al (2009) Tolllike recep-tor 4 (TLR4) polymorphisms in Tunisian patients with Crohn’s disease: genotype-phenotype correlation. BMC Gastroenterol9, 62.
19. Rigoli L, Romano C, Caruso RA, Lo Presti MA, Di Bella C, Procopio V, et al (2008) Clinical significance of NOD2/CARD15 and Toll-like receptor 4 gene sin-gle nucleotide polymorphisms in inflammatory bowel disease. World J Gastroenterol 14, 4454–61.
20. Cristofaro P, Opal SM (2006) Role of Toll-like recep-tors in infection and immunity: clinical implications. Drugs66, 15–29.
21. Brown HJ, Lock HR, Wolfs TG, Buurman WA, Sacks SH, Robson MG (2007) Toll-like receptor 4 ligation on intrinsic renal cells contributes to the induction of antibody-mediated glomerulonephritis via CXCL1 and CXCL2. J Am Soc Nephrol 18, 1732–9.
22. Robson MG (2009) Toll-like receptors and renal dis-ease. Nephron Exp Nephrol 113, e1–7.
23. Passerini P, Ponticelli C (2003) Corticosteroids, cy-clophosphamide, and chlorambucil therapy of membra-nous nephropathy. Semin Nephrol 23, 355–61. 24. Barrett JC, Fry B, Maller J, Daly MJ (2005) Haploview:
analysis and visualization of LD and haplotype maps. Bioinformatics21, 263–5.
25. Baek JI, Choi SJ, Park SH, Choi JY, Kim CD, Kim YL, et al (2009) Identification of novel variants in the COL4A4 gene in Korean patients with thin base-ment membrane nephropathy. Indian J Med Res 129, 525–33.
26. Chen CH, Shu KH, Wen MC, Chen KJ, Cheng CH, Lian JD, et al (2008) Impact of plasminogen ac-tivator inhibitor-1 gene polymorphisms on primary membranous nephropathy. Nephrol Dial Transplant 23, 3166–73.
27. Rana K, Wang YY, Buzza M, Tonna S, Zhang KW, Lin T, et al (2005) The genetics of thin basement membrane nephropathy. Semin Nephrol 25, 163–70.
28. Rudofsky G, Jr, Reismann P, Witte S, Humpert PM, Isermann B, Chavakis T, et al (2004) Asp299Gly and Thr399Ile genotypes of the TLR4 gene are associated with a reduced prevalence of diabetic neuropathy in pa-tients with type 2 diabetes. Diabetes Care 27, 179–83. 29. Tulic MK, Hurrelbrink RJ, Prele CM, Laing IA, Upham
JW, Le Souef P, et al (2007) TLR4 polymorphisms mediate impaired responses to respiratory syncytial virus and lipopolysaccharide. J Immunol 179, 132–40. 30. Pandey S, Mittal RD, Srivastava M, Srivastava K, Singh
S, Srivastava S, et al (2009) Impact of Toll-like recep-tors [TLR] 2 (-196 to -174 del) and TLR 4 (Asp299Gly, Thr399Ile) in cervical cancer susceptibility in North Indian women. Gynecol Oncol 114, 501–5.
31. Mutlubas F, Mir S, Berdeli A, Ozkayin N, Sozeri B (2009) Association between Toll-like receptors 4 and 2 gene polymorphisms with chronic allograft nephropa-thy in Turkish children. Transplant Proc 41, 1589–93. 32. Wu TH, Tsai CY, Yang WC (1998) Excessive
expres-sion of the tumor necrosis factor-alpha gene in the kid-neys of patients with membranous glomerulonephritis. Zhonghua Yi Xue Za Zhi (Taipei)61, 524–30.
33. Bantis C, Heering PJ, Aker S, Siekierka M, Kuhr N, Grabensee B, et al (2006) Tumor necrosis factor-alpha gene G-308A polymorphism is a risk factor for the development of membranous glomerulonephritis. Am J Nephrol26, 12–5.
34. Stratta P, Bermond F, Guarrera S, Canavese C, Carturan S, Dall’Omo A, et al (2004) Interaction between gene polymorphisms of nitric oxide synthase and renin-angiotensin system in the progression of membra-nous glomerulonephritis. Nephrol Dial Transplant 19, 587–95.
35. Cattran DC (2001) Idiopathic membranous glomeru-lonephritis. Kidney Int 59, 1983–94.
Freislederer A, Ohlschlegel C, et al (1989) Long-term prognosis of chronic idiopathic membranous glomeru-lonephritis. An analysis of 334 cases with particular regard to tubulo-interstitial changes. Clin Nephrol 31, 67–76.
37. Arbour NC, Lorenz E, Schutte BC, Zabner J, Kline JN, Jones M, et al (2000) TLR4 mutations are associated with endotoxin hyporesponsiveness in humans. Nat Genet25, 187–91.
38. Schwartz DA (2002) TLR4 and LPS hyporesponsive-ness in humans. Int J Hyg Environ Health 205, 221–7. 39. Tang S, Lai FM, Lui YH, Tang CS, Kung NN, Ho
YW, et al (2005) Lamivudine in hepatitis B-associated membranous nephropathy. Kidney Int 68, 1750–8. 40. Ozdemir BH, Ozdemir FN, Sezer S, Colak T, Haberal
M (2006) De novo glomerulonephritis in renal allo-grafts with hepatitis C virus infection. Transplant Proc 38, 492–5.
41. Araya CE, Gonzalez-Peralta RP, Skoda-Smith S, Dharnidharka VR (2006) Systemic Epstein-Barr virus infection associated with membranous nephropathy in children. Clin Nephrol 65, 160–4.
42. Nagashima R, Maeda K, Yuda F, Kudo K, Saitoh M, Takahashi T (1997) Helicobacter pylori antigen in the glomeruli of patients with membranous nephropathy. Virchows Arch431, 235–9.
43. Dash SC, Al-Muhanna FA (2005) Unresolved is-sues and current concepts in management of primary glomerulonephritis. Ann Saudi Med 25, 329–34. 44. Mezzano SA, Barria M, Droguett MA, Burgos ME,
Ardiles LG, Flores C, et al (2001) Tubular NF-κB and AP-1 activation in human proteinuric renal disease. Kidney Int60, 1366–77.
45. Chen A, Frank R, Vento S, Crosby V, Chandra M, Gau-thier B, et al (2007) Idiopathic membranous nephropa-thy in pediatric patients: presentation, response to therapy, and long-term outcome. BMC Nephrol 8, 11. 46. Hwang YH, Ro H, Choi I, Kim H, Oh KH, Hwang JI,
et al (2009) Impact of polymorphisms of TLR4/CD14 and TLR3 on acute rejection in kidney transplantation. Transplantation88, 699–705.