I
NTERESTING
I
MAGE
The Characteristics of FDG PET/CT Imaging in Pulmonary
Langerhans Cell Sarcoma
Yu-Wen Chen, MD,*† Chin-Chuan Chang, MD,* Po-Nian Hou, MD,* Sin-Lin Yin, MD,‡
Yung-Chang Lai, PhD,*§ and Ming-Feng Hou, MD¶
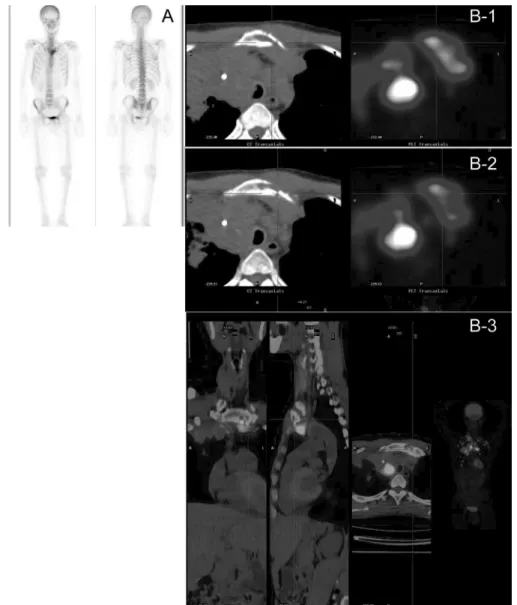
Abstract: A 53-year-old man, who was a heavy smoker, presented with recent severe cough. Radiography demonstrated a large pulmonary mass in the right upper lung. FDG PET/CT demonstrated heterogeneous high-grade activity in the pulmonary mass located in the right upper lung (standardized uptake value of 20), with central necrosis, bilateral upper mediastinal lymphadenopathy, right supraclavicular lymphadenopathy, direct left sternal manubrium invasion, and distal bilateral peripheral lung metastasis. Histol-ogy revealed significant malignant cytologic features and CD1a- and S-100-positive cells by immunohistochemistry staining, typical for Langerhans cell sarcoma.
Key Words: pulmonary, langerhans cell sarcoma, FDG, PET, CT (Clin Nucl Med 2012;37: 495– 497)
REFERENCES
1. Favara BE, Feller AC, Pauli M, et al. Contemporary classification of histio-cytic disorders. The WHO committed on histiocystic/reticulum cell prolifer-ations. Reclassification working group of the histiocyte society. Med Pediatr
Oncol. 1997;29:157–166.
2. Wood C, Wood GS, Deneau DG, et al. Malignant histiocytosis X. Report of a rapidly fatal case in an elderly man. Cancer. 1984;54:347–352. 3. Elleder M, Fakan F, Hula M. Pleiomorphous histiocytic sarcoma arising in a
patient with histiocytosis X. Neoplasma. 1986;33:117–128.
4. Itoh H, Miyaguni H, Kataoka H, et al. Primary cutaneous Langerhans cell histiocytosis showing malignant phenotype in an elderly woman: report of a fatal case. J Cutan Pathol. 2001;28:371–378.
5. Delabie J, De Wolf-Peeters C, De Vos R, et al. True histiocytic neoplasm of Langerhans’ cell type. J Pathol. 1991;16:217–223.
6. Lauritzen AF, Delsol G, Hansen NE, et al. Histiocytic sarcomas and mono-blastic leukemias. A clinical, histologic, and immunophenotypical study.
Am J Clin Pathol. 1994;102:45–54.
7. Pileri SA, Grogan TM, Harris NL, et al. Tumours of histiocytes and accessory dendritic cells: an immunohistochemical approach to classification from the International Lymphoma Study Group based on 61 cases. Histopathology. 2002;41:1–29.
8. Tani M, Ishii N, Kumagai M, et al. Malignant Langerhans cell tumour. Br J
Dermatol. 1992;126:398 – 403.
9. Julg BD, Weidner S, Mayer D. Pulmonary manifestation of a Langerhans cell sarcoma: case report and review of the literature. Virchows Arch. 2006;448: 369 –374.
10. Nakayama M, Takahashi K, Hori M, et al. Langerhans cell sarcoma of the cervical lymph node: a case report and literature review. Auris Nasus Larynx. 2010;37:750 –753.
11. Travis WD, Brambilla E, Mu¨ller-Hermelink HK, et al. WHO, Pathology &
Genetics. Tumours of the Lung, Pleura, Thymus and Heart. Lyon, France:
IARC Press; 2004.
12. Benz MR, Dry SM, Eilber FC, et al. Correlation between glycolytic pheno-type and tumor grade in soft-tissue sarcomas by 18F-FDG PET. J Nucl Med. 2010;51:1174 –1181.
13. Djouad F, Bouffi C, Ghannam S, et al. Mesenchymal stem cells: innovative therapeutic tools for rheumatic diseases. Nat Rev Rheumatol. 2009;5:392– 399.
14. Ruan K, Bao S, Ouyang G. The multifaceted role of periostin in tumorigen-esis. Cell Mol Life Sci. 2009;66:2219 –2230.
15. Bouffi C, Djouad F, Mathieu M, et al. Multipotent mesenchymal stromal cells and rheumatoid arthritis: risk or benefit? Rheumatology (Oxford). 2009;48: 1185–1189.
16. Goda T, Shimo T, Yoshihama Y, et al. Bone destruction by invading oral squamous carcinoma cells mediated by the transforming growth factor-beta signaling pathway. Anticancer Res. 2010;30:2615–2623.
17. Roodman GD. Mechanisms of bone metastasis. N Engl J Med. 2004;350: 1655–1664.
Received for publication January 17, 2011; revision accepted June 3, 2011. From the *Department of Nuclear Medicine, Kaohsiung Medical University
Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan; †Department of Nuclear Medicine, School of Medicine, Kaohsiung Medical University, Ka-ohsiung, Taiwan; ‡Department of Pathology, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan; §Department of Public Health, College of Health Sciences, Kaohsiung Medical Univer-sity, Kaohsiung, Taiwan; and ¶Cancer Center, Kaohsiung Medical Uni-versity Hospital, Kaohsiung Medical UniUni-versity, Kaohsiung, Taiwan. Conflicts of interest and sources of funding: none declared.
Reprints: Yung-Chang Lai, PhD, Department of Nuclear Medicine, Kaohsiung Medical University, No. 100, Tzyou 1st Rd, Kaohsiung City, 80756 Taiwan. E-mail: [email protected].
Copyright © 2012 by Lippincott Williams & Wilkins ISSN: 0363-9762/12/3705-0495