Internal Medicine Journal 2005; 35: 188–190
B
RIEF
C
OMMUNICATION
Risk estimates for drugs suspected of being associated with
Stevens-Johnson syndrome and toxic epidermal necrolysis:
a case-control study
M.-S. LIN,1,3 Y.-S. DAI,2 R.-F. PWU,4 Y.-H. CHEN3 and N.-C. CHANG5
1Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, Departments of 2Dermatology and 3Pharmacy, National Taiwan University Hospital, 4iSTAT Healthcare Consulting Co. Ltd and 5Department of Internal Medicine, Taipei Medical University Hospital, Taipei, Taiwan
Abstract
The purpose of this case-control study is to estimate the risks of Stevens-Johnson syndrome or toxic epidermal necrolysis associated with the use of specific drugs. The suspected cases were identified from the computerized hospital discharge file. We calculated crude relative risks and adjusted them for confounding by multivariate anal-ysis. The analysis was based on 35 cases and 105
con-trols. This study showed that the use of carbamazepine, phenytoin and allopurinol is most associated with the risks in the oriental population. (Intern Med J 2005; 35: 188–190)
Key words: case-control study, Stevens-Johnson
syndrome, toxic epidermal necrolysis, adverse drug reaction, relative risk.
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare, but life-threatening cuta-neous reactions. Both disorders are characterized by high fever, malaise, blistering macules, erosions of the mucous membranes, extensive detachment of epidermis and severe constitutional symptoms. SJS represents cases of less than 10% body surface area involvement, TEN indicates more than 30% and those in between are labelled SJS–TEN ‘overlap’. The incidence rates are 1–6 cases/106 person-years (SJS), and 0.4–1.2 cases/106 person-years (TEN), respectively.1 Death occurs in up to 18% of patients with SJS, and up to 50% of patients with TEN.2,3 The aetiology of SJS and TEN is usually drug-related (80–95% of patients with TEN, >50% with SJS).3–7 Many drugs, including sulphonamides, anti-convulsant agents, chlormezanone, piroxicam, allo-purinol and aminopenicillins are consistently reported with these severe conditions.8 A case-series study conducted in Taiwan7 found that each of three drugs, carbamazepine, phenytoin and allopurinol, had more than three cases of SJS/TEN reported and were highly suspected to be associated with SJS/TEN occurrence. Thus, it is important for drug safety to estimate the risk for SJS/TEN.
We conducted a case-control study to estimate the relative risks of SJS/TEN associated with certain selected
drugs. The source of data was the admission database of a university teaching hospital from January 1998 through June 2001. Based on International Classification of Diseases-Clinical Modification coding,9 suspected cases of SJS or TEN were identified from the computerized hospital discharge file. Medical charts review was carried out by a pharmacist, and cases were validated with standardized diagnosis of SJS and TEN3,10,11 by a dermatologist who was not given the data on the patients’ drug exposure. Control subjects with an acute illness not suspected of being related to drug use (e.g. acute infections, traumatic injury) were randomly sampled from the same database. Control subjects with drug-related E-codes (e.g. accidental poisoning E850-E869, therapeutic use E930-E949, suicide attempt E950-E952, assault E961-E962, undetermined E980-E982) were excluded. Three control subjects were matched to cases by age (±2 years old), sex and calendar month of admission.
Data collected included: sex, age, calendar month of admission, diagnoses (International Classification of Diseases–ninth revision–Clinical Modification (ICD-9-CM)), E-code, drug exposure, potential confounding factors, drug history, onset after drug intake and disease outcome. The potential confounders1,4 we collected included radiotherapy (V58.0), collagen vascular disease (9-CM 446.20), infections with HIV (V08 or ICD-9-CM 042), recent herpes infection (ICD-ICD-9-CM 053 or 054) and autoimmune disease (ICD-9-CM 279.4). In addition, we assessed Naranjo scores12 for each case patient. According to Naranjo scores, an individual case was classified as definite (Naranjo score >9), probable (Naranjo score 5–8), possible (Naranjo score 1–4), or no association of adverse drug reaction.
Correspondence to: Nen-Chung Chang, School of Medicine, Taipei Medical University Hospital. 252, Wu-Hsing Street, Taipei 105, Taiwan. Email: [email protected]
Received 15 June 2004; accepted 30 October 2004. Funding: None
Risk for drugs related SJS or TEN 189
Internal Medicine Journal 2005; 35: 188–190
An index day was estimated for each of the study subjects. The index day of case patients was defined as the date of skin reaction. The index day of control patients was defined as the date that their illness started. The subjects who took a certain drug with elimination half-life less than 24 h (e.g. phenytoin) within 1 week before the index day were defined as exposed to that drug. The exposure interval was extended to 2 weeks for drugs with elimination half-lives between 24 and 72 h (e.g. allopurinol, carbamazepine, chlormezanone, oxicam non-steroidal anti-inflammatory drugs (NSAIDs)), and 3 weeks for drugs with elimination half-lives longer than 72 h (e.g. phenobarbital).13–15
Data were analyzed by SAS (version 8.1) (SAS Insti-tute Inc., Cary, NC, USA). The crude relative risks and 95% confidence intervals (CI) were estimated by uni-variate analysis. We used conditional logistic analysis to consider drugs simultaneously being taken by at least three case patients, adjusting for the effects of potential confounders. The potential confounders in the model included: radiotherapy, with one case patient (3%) and four controls (4%); collagen vascular disease, infections with HIV and recent herpes infection, with 0 case patient and 0 control and autoimmune disease, with one case patient (3%) and 0 control. The other drugs that had less than three case patients (i.e. sulfa drugs, antibiotics, oxicam anti-inflammatory agents), suspected of being associated with SJS or TEN, were grouped and included in the models.
The analysis of total subjects was based on 35 cases and 105 controls. There were 30 cases of SJS (16 males and 14 females) and five cases of TEN (three males and two females). Among these, three cases of STS and two cases of TEN died. The death rate was 10% and 40%, respectively. The mean age (± standard deviation) of SJS and TEN was 53.4 ± 21.15 and 36 ± 30.39, respectively. The average onset of these severe conditions after initial
drug administration was 15 days, and only one case occurred after longer than 8 weeks. Among the 35 cases, one (3%) was classified as definite, 32 (91%) were clas-sified as probable association, one (3%) was clasclas-sified as possible, and the remaining one (3%) had no association with any suspect drugs.
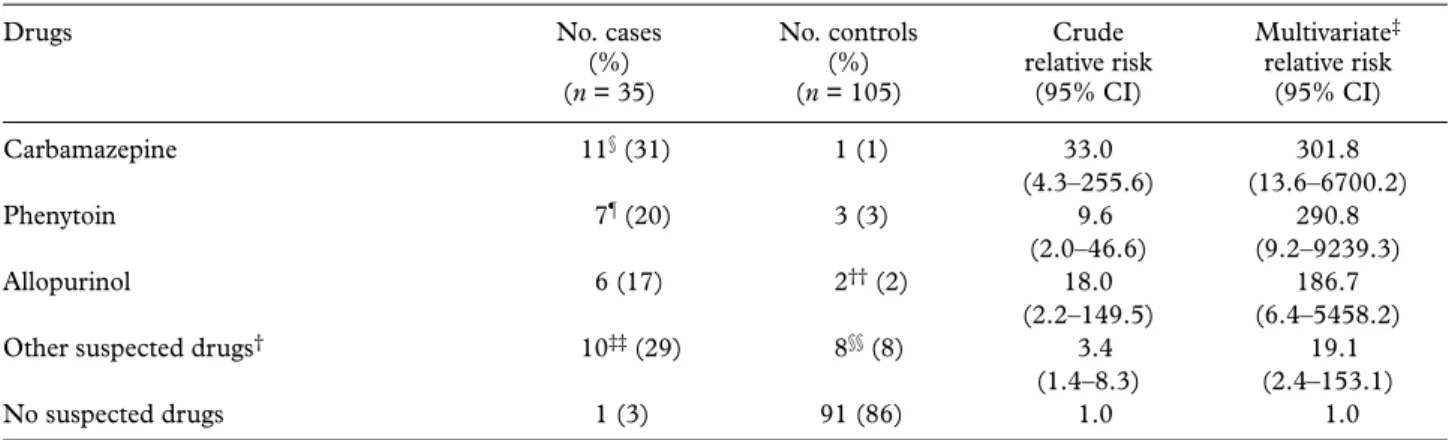
According to our exposure definition, 34 (97%) of the 35 cases, and 14 (13%) of the 105 controls were exposed to at least one drug. Within the exposure interval preceding the index day for each subject, 11 (31%) cases (three cases co-administered with other suspect drugs) and one (1%) control took carbamazepine; seven (20%) cases (two cases coadministered other suspect drugs) and three (3%) controls took phenytoin; six (17%) cases and one (1%) control took allopurinol; one case (3%) and 91 controls (86%) had no intake of suspect drugs; and the remainder of cases (29%) and controls (9%) took other suspect drugs, with less than three cases for each drug. (Table 1)
Only three drugs (carbamazepine, phenytoin, allo-purinol) were exposed in more than three cases and Table 1 demonstrates that they were highly associated with SJS or TEN. Although the relative risks of these three suspected drugs had wide CI because we could only identify 35 cases, the lower limit of their 95%CI for the relative risk was significantly greater than ‘1.0’.
The incidence of SJS or TEN is very low, but the conditions are often unpredictable and life-threatening. The literature suggests that these conditions are highly associated with drug intake.1–8 Previous studies on a series of cases in Taiwan could not estimate the relative risks of SJS and TEN associated with specific drugs.5,7 Prescribing patterns may vary with different countries. Thus, it was important in Taiwan to conduct a case-control study to estimate the relative risks ratios of suspect drugs.
Table 1 Frequency distribution of reported intake of selected drugs in cases and controls
Drugs No. cases
(%) (n = 35) No. controls (%) (n = 105) Crude relative risk (95% CI) Multivariate‡ relative risk (95% CI) Carbamazepine 11§ (31) 1 (1) 33.0 301.8 (4.3–255.6) (13.6–6700.2) Phenytoin 7¶ (20) 3 (3) 9.6 290.8 (2.0–46.6) (9.2–9239.3) Allopurinol 6 (17) 2†† (2) 18.0 186.7 (2.2–149.5) (6.4–5458.2)
Other suspected drugs† 10‡‡ (29) 8§§ (8) 3.4 19.1
(1.4–8.3) (2.4–153.1)
No suspected drugs 1 (3) 91 (86) 1.0 1.0
†The drugs other than allopurinol, carbamazepine or phenytoin; ‡adjusted for the potential confounders those include other suspected drugs,
radiotherapy, collagen vascular disease, infections with HIV, recent herpes infection, and autoimmune disease; §one case: coadministration of
carbamazepine and chlorzoxazone, one case: coadministration of carbamazepine and chlorzoxazone, one case: coadministration of carbamazepine and tenoxicam; ¶one case: coadministration of phenytoin, cefotiam and nabumetone; one case: coadministration of phenytoin and cefadroxil; ††one
control: coadministration of nambumetone, allopurinol and ampicillin; ‡‡two cases: futraful, two cases: meloxicam, one case: cephazolin, one case:
amoxicillin, one case: coadministration of cephalosporin and lincomycin, one case: phenobarbital, one case: adem savi (Indonesian drug), one case: sulfasalazine §§one control: coadministration of meloxicam, sulfasalazine, methotrexate and naproxen, one control: coadministration of
nabumetone and amoxicillin/clavulanate, one control: meloxicam, one control: phenobarbital; one control: coadministration of tiaprofenic acid and cefazolin, one control: amoxicillin/clavulanate, one control: coadministration of nabumetone and chlorzoxazone, one control: cefazolin.
190 Lin et al.
Internal Medicine Journal 2005; 35: 188–190
The suspect drugs (i.e. carbamazepine, phenytoin and allopurinol) of case patients in our study were similar to the findings of Li et al. in 1996.7 The mortality rates in our study were similar to previous literature.1,3 The list of suspect drugs is subject to change with region and time.8 Our study observed that the use of carba-mazepine, phenytoin and allopurinol is associated with significant increases in the risk of SJS or TEN. This finding was consistent with the theory that most cases of SJS and TEN are drug-related. Other drugs such as sulfa drugs, phenobarbital, aminopenicillins, NSAIDs and lamotrigine, are well-documented in the literature as causal agents of SJS/TEN. 1,4,8 Only two case patients in our study were attributed to the use of NSAIDs, both to meloxicam, a cyclooxygenase-2, despite many patients, particularly the elderly, using drugs of this class. The finding that the onset of disease on average was 15 days is similar to the study by Rzany et al.4
Coding of ICD-9-CM 695.1 (erythema multiforme) includes erythema iris, herpes iris, Lyell’s syndrome, scalded skin syndrome, SJS and TEN,9 so it is not specific to identify cases of SJS or TEN.16–18 The means used to ascertain cases was a sensitive, but not a specific method. To ensure that cases of SJS and TEN identified by this method actually had these conditions, we had the cases reviewed by a dermatologist. The dermatologist did not know the patients’ drug history. In our study, using the method of the dermatologist’s review, the positive predictive value of discharge diagnosis for SJS/ TEN was only 60% (35/58). It is possible that despite our thorough review, some cases were either missed or still not correctly diagnosed as the diagnosis of these conditions relies on subjective clinical judgement. The cases in our study were severe conditions that either led to admission or occurred while in hospital, and milder cases treated only in the outpatient clinics were not included. These milder cases are probably less important in assessing a drug’s risk, so the influence of excluding them should be small.
Stevens-Johnson syndrome and TEN are rare, but severe drug-related cutaneous reactions. This study demonstrated the relationship between these conditions and the use of carbamazepine, phenytoin and allo-purinol. A larger study could potentially confirm the relationship with other drugs.
ACKNOWLEDGEMENTS
The authors wish to thank the Department of Pharmacy and Chart Management in National Taiwan University Hospital for offering the datasets, and Dr Wen Chung Lee and Dr K. Arnold Chan for consulting.
REFERENCES
1 Roujeau JC, Kelly JP, Naldi L, Rzany B, Stern RS, Anderson T
et al. Medication use and the risk of Stevens-Johnson syndrome or toxic epidermal necrolysis. N Engl J Med 1995; 333: 1600–7.
2 Huff JC. Erythema multiforme. In: Sams WM, Lynch PJ, eds. Principles and Practice of Dermatology, 2nd edn. New York: Churchill Livingstone; 1996; 483–90.
3 Fritsch PO, Ruiz-Maldonado R. Erythema multiforme. In: Freedberg IM, Eisen AZ, Wolff K et al. eds. Fitzpatrick’s Dermatology in General Medicine, 5th edn. New York: McGraw-Hill; 1999, 636–44.
4 Rzany B, Correia O, Kelly J, Naldi L, Anquier A, Stern R. Risk of Stevens-Johnson syndrome and toxic epidermal necrolysis during first weeks of antiepileptic therapy: a case-control study. Lancet 1999; 353: 2190–4.
5 Chou BL, Chou CT, Lee CF. A clinical analysis of the Stevens-Johnson syndrome. J Med Sci 1988; 9: 131–8.
6 Schöpf E, Stühmer A, Rzany B, Victor N, Zentgraf R, Kapp JF. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Arch Dermatol 1991; 127: 839–42.
7 Li TH, Chan YC, Sun CC. Erythema multiforme, Stevens-Johnson syndrome and toxic epidermal necrolysis – antecedent drug exposures in 99 hospitalized patients. Dermatol Sinica 1996; 14: 119–25.
8 Fritsch PO, Ruiz-Maldonado R. Stevens-Johnson syndrome – toxic epidermal necrolysis. In: Freedberg IM, Eisen AZ, Wolff K
et al. eds. Fitzpatrick’s Dermatology in General Medicine, 5th edn. New York: McGraw-Hill; 1999; 644–54.
9 Practice Management Information Corporation. International Classification of Diseases. 9th revision. Clinical Modification, 6th edn. Los Angeles: PMIC; 2001; 391.
10 Chan HL, Stern RS, Arndt KA, Langlois J, Jick SS, Jick H et al.
The incidence of erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis. Arch Dermatol 1990; 126: 43–7.
11 Kelly JP, Auquier A, Rzany B, Naldi L, Bastuji-Garin S, Correia O
et al. An international collaborative case-control study of severe cutaneous adverse reactions (SCAR). Design and methods. J Clin Epidemiol 1995; 48: 1099–108.
12 Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA
et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther 1981; 30: 239–45. 13 Rzany B, Mockenhaupt M, Baur S, Schroder W, Stocker U,
Mueller J et al. Epidemiology of erythema exsudativum multiforme majus, Stevens-Johnson syndrome, and toxic epidermal necrolysis in Germany (1990–1992): structure and results of a population-based registry. J Clin Epidemiol 1996; 49: 769–73.
14 Steven KH, Kenneth HK, Teri HB, Kirsten KN, Wendy LB, Sara LS et al. eds. Facts and Comparisons: Drug Facts and Comparisons, 55th edn. St. Louis: Facts and Comparisons; 2001; 377–9.
15 Steven KH, Kenneth HK, Teri HB, Kirsten KN, Wendy LB, Sara LS et al. eds. Facts and Comparisons: Drug Facts and Comparisons, 55th edn. St. Louis: Facts and Comparisons; 2001; 1028–9.
16 Strom BL, Carson JL, Halpern AC, Schinnar R, Snyder ES, Shaw M et al. A population-based study of Stevens-Johnson syndrome. Arch Dermatol 1991; 127: 831–8.
17 Strom BL, Carson JL, Halpern AC, Schinnar R, Snyder ES, Stolley PD et al. Using a claims database to investigate drug-induced Stevens-Johnson syndrome. Stat Med 1991; 10: 565–76. 18 Steven KH, Kenneth HK, Teri HB, Kirsten KN, Wendy LB,
Sara LS et al. eds. Facts and Comparisons: Drug Facts and Comparisons, 55th edn. St. Louis: Facts and Comparisons; 2001; 1039–42.