Received: Mar. 10, 2005 Revised: Apr. 5, 2005 Accepted: May.13, 2005
Address reprint requests and correspondence to:Dr. Kuan Chou Chen
Department of Urology, Taipei Medical University Hospital, No. 252. Wu-Xing St., Taipei, Taiwan 110, R.O.C.
台灣泌尿醫誌第十六卷第三期(94 年 09 月) 115
Case Analysis
Prostatic Pure Small Cell Carcinoma v.s. Mixed-Type
Small Cell Carcinoma: Analysis of Two Cases
Chih-Kai Hsu
1, Chien-Jui Cheng
2, Kuan Chou Chen
1,
Han-Sun Chiang
1,3, Jan-Show Chu
21
Department of Urology, Taipei Medical University Hospital, Taipei, Taiwan, R.O.C.
2
Department of Pathology, Taipei Medical University, Taipei, Taiwan, R.O.C.
3
College of Medicine, Fu Jen Catholic University, Hsinchuang, Taipei, Taiwan, R.O.C.
We analyzed 2 cases of small cell carcinoma of the prostate. One patient had pure small cell carcinoma with multiple organ metastasis, while the other had a mixed-type carcinoma. The immu-nohistochemical studies revealed positive reactions to chromogranin A, synaptophysin, and cy-tokeratin stains, and negative for PSA stain over both small cell carcinoma foci. These 2 patients were immediately treated, and partial resolution of the previous metastatic bone lesions was noted after receiving 5 courses of chemotherapy with the combination of gemcitabine, carboplatin, and irradiation therapy in case 1, while adjuvant irradiation was scheduled for case 2. (JTUA 16:115-9,
2005)
Key words: prostate, small cell carcinoma, neuroendocrine, immunohistochemical studies.
INTRODUCTION
Small cell carcinomas of the prostate are rare, and their clinical behavior reveals that they are highly ag-gressive neoplasms [1]. Some evidence has suggested that these tumors are heterogeneous and show neuroen-docrine differentiation [2]. Of note, 20% of patients present with small cell carcinoma in association with a regular adenocarcinoma, 30% during the course of pro-gression of a regular adenocarcinoma, and the remaining 50% present with pure small cell carcinoma [3,4]. It seems likely that small cell carcinoma of the prostate arises from pluripotent prostatic epithelial cells, which may have the potential for divergent differentia- tion into neuroendocrine and acinar tumor cells [5]. Here in, we present our experience of 2 cases of small cell carcinomas of the prostate. One of them was pure small cell carcinoma of the prostate with the common characteristics of distant metastasis upon initial diagnosis, while the other was mixed small cell car-
other was mixed small cell car- cinoma and a high-grade acinar adenocarcinoma. The immunohistochemical studies, clinical presentations, and managing strategies related to these 2 different conditions are discussed .
CASE REPORT
Case 1
A 79-year-old male presented with repeated uri-nary retention. He suffered from hypertension, diabetes mellitus, and coronary artery disease. Mild lower urinary tract symptoms were noted without medication control. In addition, no cancer family history was apparent. A digital examination revealed an elastic, moderately enlarged prostate without abnormal nodules. The preop-erative serum PSA level was 1.42 ng/ml, and cystoscopy revealed evident contact between the prostate lateral lobes. Under the impression of benign prostate hyplasia, a transurethral prostatectomy (TUR-P) was
per-Pure and Mixed-Type Small Cell Carcinomas of the Prostate
118 JTUA Vol.16 No.3, Sep. 2005
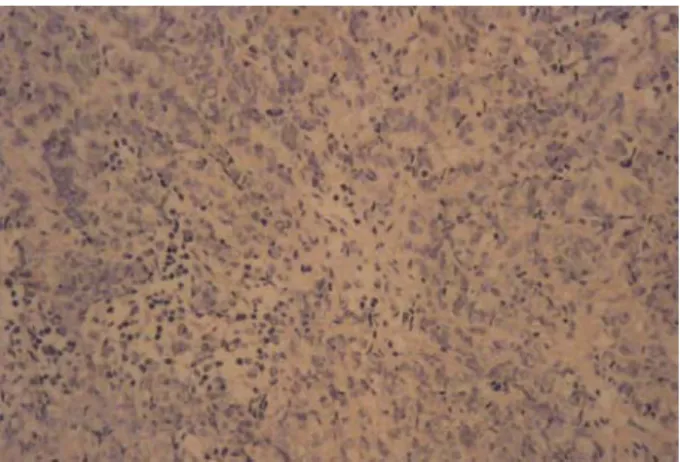
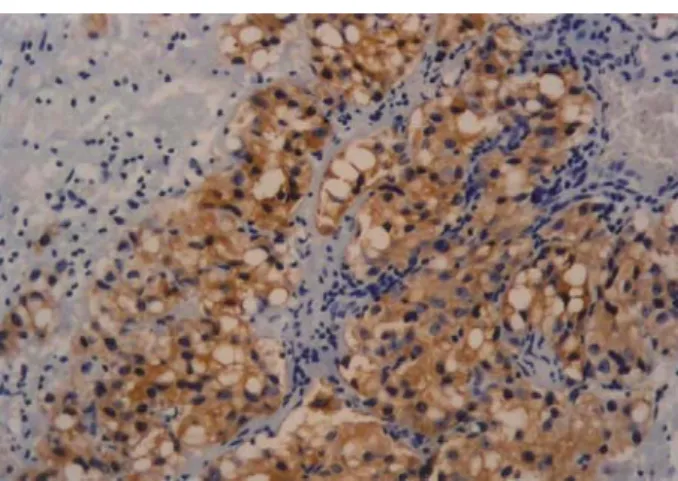
formed. Specimens revealed a picture of neuroendocrine carcinoma in about 20% of the microsection area with a diffuse positive reaction to chromogranin A stain (Fig.1), a focally positive re- action to synaptophysin and cy-tokeratin stains, and a negative reaction to PSA stain (Fig. 2). Pure small cell carcinoma of the prostate was the diagnosis. A computed tomogram (CT) and bone scan were arranged 2 weeks after the TUR-P. The CT revealed liver, spleen, and pelvic lymph node metastatic lesions, and the bone scan showed skeletal metastasis in the ribs, T1-L5 spine, sacrum, and both sacroiliac joints. After receiving 5 courses of chemotherapy with the combination of gemcitabine and carboplatin, and pallia-tive irradiation of 4000 cGy in 10 fractions for the bone lesions, the follow-up bone scan revealed partial resolu-tion of the previous metastatic bone lesions, but the CT revealed that the liver, spleen, and pelvic lymph node metastatic lesions were unchanged. In the meantime, the serum PSA level had dropped to 0.06 ng/ml. He died due to sudden cardiac arrest shortly after the final course of chemotherapy with a partial response and a survival duration of 7.4 months.
Case 2
A 78-years-old male had suffered from micturition difficulty and gross hematuria for 1 month. The digital examination revealed remarkable prostate enlargement with a stony-hard consistency and a serum PSA value of 45.2 ng/ml. The cystoscopic examination revealed a severe kissing prostate with an irregular surface and intravesical invasion. The pelvic CT revealed prostate tumor invasion into the bladder and pelvic side wall with highly suspicious pelvic lymph node metastasis. A pal-liative TUR-P was performed, and the pathology report revealed a group of neuroendocrine carcinomas mixed with a poorly differentiated adenocarcinoma. The poorly
differentiated area of the adenocarcinoma was reactive for prostatic-specific antigen (Fig. 3), while the neuro-endocrine carcinoma presented the pathological charac-teristics of a diffuse positive reaction to chromogranin A stain, focal positive reaction to synaptophysin and cy-tokeratin stains, and a negative reaction to PSA stain. Small cell carcinoma of the prostate was the diagnosis. Irradiation therapy was scheduled after the definitive diagnosis. Whole-pelvis irradiation with 5040 cGy in 28 fractions followed by a boost of 900 cGy for 5 times was given. A good response with the tumor lesion going into nearly total remission was detected on the follow-up CT scan, and the serum PSA value had decreased to 6.24 ng/ml after the irradiation therapy was completed. No hormone or chemotherapy was arranged for this patient, who was lost to follow-up 6 months later.
DISCUSSION
We describe the clinical characteristics and patho-logic findings of pure small cell carcinoma of the pros-tate and combined small cell and a usual acinar adeno-carcinoma of the prostate. As case 1 typifies, early di-agnosis of pure small cell carcinoma of the prostate is more difficult, because of a lack of concordant elevation of PSA with an acinar adenocarcinoma of the prostate. Primary small cell carcinoma is well known in the lung, but small cell carcinoma of the prostate is a very rare condition, comprising 0.5%~2% of all prostate cancers [6]. These extrapulmonary small cell carcinomas can be distinguished from small cell lung carcinoma (SCLC) by light microscopic, ultrastructural, and im-munohistochemistry examinations. Neuroendocrine dif-ferentiation of prostate cancer includes pure small cell carcinoma, carcinoid and carcinoid-like tumors and
Fig. 1 Immunohistochemistry study positive for chromogranin A (400X).
Fig. 2 Immunohistochemistry study negative for prostatic-specific antigen (400X).
CK Hsu, CJ Cheng, KC Chen, et al.
台灣泌尿醫誌第十六卷第三期(94 年 09 月) 117
conventional prostate adenocarcinomas with focal neu-roendocrine differentiation [7]. The concordance of prostatic small cell carcinoma with an acinar adeno- carcinoma also resulted from recurrence of a previous adenocarcinoma after hormone therapy [8].
Three theories of histogenesis have been proposed. First, it was suggested that prostatic small cell carcino-mas arise from amine precursor uptake decarboxylation (APUD) cells of local endodermal origin [9]. Second, it was proposed that prostatic small cell carcinomas arise from dedifferentiation of prostatic adenocarcinomas, suggesting that prostatic small cell carcinoma is part of a spectrum of prostatic adeno- carcinomas rather than a separate disease entity [10]. Third, due to similarities of the histologic pictures and neuroendocrine paraneoplas-tic syndromes with SCLC, the most-widely accepted view is that prostatic small cell carcinomas arise from totipotential stem cells of the prostate, which have the ability to differentiate into either epithelial, or neuroen-docrine-type carcinomas [11,12]. Immunohistochemical studies have shown multidirectional differentiation along with epithelilal, neuroendocrine, and/or mesen-chymal differentiation of poorly-differentiated prostate cancers [13,14]. The dia- gnosis of a neuroendocrine carcinoma is mainly based on a definitive histological examination, but sometimes a confident categorization of the tumor may be difficult.
In contrast to prostatic adenocarcinomas, PSA, an unreliable tumor marker for pure prostatic small cell carcinoma, is usually normal, even when there is metas-tatic disease. One study suggested that the carcinoem-bryonic antigen is a more-reliable marker, because in-creases and dein-creases in antigen levels are found with disease progression and regression, respectively [12].
Prostatic small cell carcinoma has a propensity to
metastasize to visceral organs, including the liver, bone, lungs, central nervous system, and pericardium, and regionally to the pelvic lymph nodes, rectum, and blad-der [12].
Prostatic small cell carcinoma has the same unfa-vorable outcome as other SCLC counterpart [15]. As in our case 1, prostatic small cell carcinoma has a highly aggressive course and a poor prognosis. Despite treat-ment with chemotherapy, the prognosis of prostatic small cell carcinoma is extremely poor, and the median survival is 7 months [16]. Sometimes, patients with prostatic small cell carcinoma show some paraneoplastic syndromes, such as limbic encephalitis [17], ina- ppriate secretion of antidiuretic hormone [18], and pro-duction of adrenocorticotrophic hormone [18].
Because of the rarity of the condition, no standard therapeutic regimen has been developed. In addition, prostatic small cell carcinoma, in contrast to adeno- car-cinomas, has been found to be unresponsive to hormone therapy. It is the most-aggressive variant of prostate cancer with no successful treatment to the present. By combining gemcitabine and carboplatin with irradiation therapy, we achieved a partial response to the metastatic bone lesions in case 1. Pelvic irradiation alone achieved almost complete remission in case 2. According to our experience, irradiation therapy seemed to be effective in controlling locally advanced lesions of mixed adeno- and small cell carcinomas of the prostate. Furthermore, even in patients with multiple metastatic lesions of pure small cell carcinoma of the prostate, irradiation can be palliative therapy for painful metastatic bone lesions. The combination of carboplatin and gemcitabine has emerged as a standard regimen for SCLC [19], but ad-justment and modification of the regimens and dosages in small cell carcinoma of prostate are still necessary to achieve a more-effective response.
REFERENCES
1.Bolton DM, Chiu ST, Clarke S, Angus D. Primary small cell carcinoma of the prostate: unsual modes of presentation. Aust NZ Surg 1994;64:91-4.
2.Amato RJ, Logothetis CJ, Hallinan R, Ro JY, Sella A, Dexesu FH. Chemotherapy for small cell carcinoma of prostate origin. J Urol 1992;147:935-7.
3.Yu DS, Chang SY, Wang J, et al. Small cell carcinoma of the urinary tract. Br J Urol 1990;66:590-5.
4.Oesterling JE, Hauzeur CG, Farrow GM. Small cell anaplastic carcinoma of the prostate: a clinical, patho- logical and immunohistological study of 27 patients. J Urol 1992;147:804-7.
5.Jennifer RB, Tad JW, Kitt S, Ravi S. Small cell
can-Fig. 3 Poorly differentiated adenocarcinoma of the prostate positively reactive to prostatic- spe-cific antigen (400X).
Pure and Mixed-Type Small Cell Carcinomas of the Prostate
118 JTUA Vol.16 No.3, Sep. 2005
cers, and an unusual reaction to chemotherapy. J Clin Oncol 2003;21:2437-43.
6.Helpap B, Kollermann J, Oehler U. Neuroendocrine differentiation in prostatic carcinomas: histogenesis, biology, clinical relevance, and future therapeutical perspectives. Urol Int 1999;62:133-8.
7.di Sant'Agnese PA. Neuroendocrine differentiation in carcinoma of the prostate. Diagnostic, prognostic, and therapeutic implications. Cancer 1992;70 (Suppl 1): 254-68.
8.Miyoshi Y, Uemura H, Kitami K, Satomi Y, Kubota Y, Hosaka M. Neuroendocrine differentiated small cell carcinoma presenting as recurrent prostate cancer after androgen deprivation therapy. Br J Urol Int 2001; 88: 982-3.
9.di Sant'Agnese PA, Cockett AT. Neuroendocrine dif-ferentiation in prostatic malignancy. Cancer 1996; 78:357-61.
10.Schron DS, Gipson T, Mendelsohn G. The histoge- nesis of small cell carcinoma of the prostate. An im-munohistochemical study. Cancer 1984; 53: 2478- 80.
11.Aygun C. Small cell carcinoma of the prostate: a case report and review of the literature. Maryland Med J 1997;46:353-6.
12.Rubenstein JH, Katin MJ, Mangano MM, et al. Small cell anaplastic carcinoma of the prostate: seven new cases, review of the literature, and discussion of a therapeutic strategy. Am J Clin Oncol 1997; 20: 376- 80.
13.Helpap B, Kollermann J. Undifferentiated carcinoma of the prostate with small cell features: immuno- his-tochemical subtyping and reflections on histogenesis. Virchows Arch 1999;434:385-91.
14.Weaver MG, Abdul-Karim FW, Srigley JR. Paneth cell-like change and small cell carcinoma of the prostate. Two divergent forms of prostatic neuroen-docrine differentiation. Am J Surg Pathol 1992;16:1013-6.
15.Jelbert ME, Russell PJ, Russell P, Rayhovon D. The biology and management of small cell un- differenti-ated carcinoma of prostate. In: Williams CJ, Kri-karian JG, Green MR, Rayhaven D, editors. Text-book of Uncommon Cancer. London: Wiley, 1998:249-62.
16.Patel A, Ball J, Chappell M. Pure primary small cell carcinoma of the prostate. Br J Urol 1993;72:380-1. 17.Stern RC, Hulette CM. Paraneoplastic limbic
en-cephalitis associated with small cell carcinoma of the prostate. Mod Pathol 1999;12:814-8.
18.Kawai S, Hiroshima K, Tsukamoto Y, et al. Small cell carcinoma of the prostate expressing prostate- specific antigen and showing syndrome of ina-
ppro-priate secretion of antidiuretic hormone: an autopsy case report. Pathol Int 2003;53:892-6.
19.Simon M, Argiris A, Murren JR. Progress in the therapy of small cell lung cancer. Crit Rev Oncol Hematol 2004;49:119-33.