Sharing patient care records over the World Wide Web
Chien-Tsai Liu
a,c,*, Ann-Ging Long
a, Yu-Chuan Li
a, Kuo-Ching Tsai
b,
Hsu-Sung Kuo
baGraduate Institute of Medical Informatics, Taipei Medical Uni6ersity, Taipei, Taiwan bDepartment of Health, The Executi6e Yuan, Taipei, Taiwan
cDepartment of Information Systems, Taipei Medical College Uni6ersity-Wanfang Hospital, Taiwan
Abstract
In order to obtain appropriate medical care, patients can be referred or transported from one hospital to another based on the capacity, capability and quality of medical care provided by hospitals. Therefore, enabling patient care records to be shared among hospitals is essential not only in delivering the quality of medical care services but also in saving medical expenses. Currently, most patient care records are paper-based and not well organized. Hence, they are usually incomplete and can hardly be accessed in time. The authors in this paper present methods to structure and represent patient care records, design mechanisms for interpreting and integrating the XML-based patient care records into the existing hospital information systems. More importantly, in our approach, each significant piece of medical record is associated with a tag based on the syntax and semantics of the XML. The XML-based medical records enable a computer to capture the meaning and structure of the document on the web. The authors have developed a unified referral information system in which patient care records can be shared among hospitals over the Internet. It can not only facilitate the referral process but also maintain the integrity of a patient’s medical record from distributed hospitals. The workflow of the system basically follows the existing manual system and can easily be adapted. The working group on integration of municipal hospital information systems, Department of Health, Taipei City Government, has decided to adapt this system for referral practice among the municipal hospitals. © 2001 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Electronic patient record; Hospital information systems; Referral systems; XML
1. Introduction
Hospitals (or healthcare providers) are ranked based on their capacity and capability in providing the quality of medical care in Taiwan. There are three major categories of hospitals, namely, district hospital, regional hospital and the medical center. The district
* Corresponding author. No. 111, Sec. 3, Hsinlung Rd. Taipei, Taiwan, PR China. Tel.: + 886-2-29307930, ext. 8910; fax: + 886-2-29334823.
E-mail addresses: [email protected] (C.-T. Liu), [email protected] (A.-G. Long), [email protected] (Y.-C. Li), [email protected] (K.-(Y.-C. Tsai), [email protected] (H.-S. Kuo).
1386-5056/01/$ - see front matter © 2001 Elsevier Science Ireland Ltd. All rights reserved. PII: S 1 3 8 6 - 5 0 5 6 ( 0 1 ) 0 0 1 4 1 - 1
hospitals can provide only minimum medical services such as general outpatient services, health consultation, preventive medicine and so on. They usually do not provide emer-gency care. The medical centers on the con-trary, can provide full services not only for outpatient but also for inpatient and emer-gency care. They are ranked the highest and can perform all kinds of medical services depending on their facilities and the ability of the medical professionals. The capacity and capability of medical services provided by the regional hospitals are in between the services provided by district hospitals and the medical centers.
In order to obtain appropriate medical care, patients can be referred or transported from one hospital to another among the dif-ferent ranks. The referred or emergency transported patients (or in general terms, re-ferrals) are required to carry their referral initiation forms (RIF) in which the chart summary of the referrals’ medical records (or patient care records) describing the patients’ symptoms and the medical services that have been performed on that patients are included. From a continual medical care point of view, the chart summary is essential to the medical professionals (or accepting physicians) who accept the referrals. Upon reviewing a pa-tient’s chart summary, the accepting
physi-cians can quickly understand the
development of the patient’s syndrome, the previous diagnosis and the performed medi-cal services. Therefore, a complete referral’s chart summary can help a physician make the appropriate treatment plan, and avoid per-forming redundant medical services.
In practice, the description of a chart sum-mary in a referral initiation form is usually incomplete and may not reflect the medical care in the referring hospitals. There are three main reasons. Firstly, there is little incentive to encourage sharing patient care records
among hospitals under the current payment policy established by the Bureau of National Health Insurance (BNHI) [1]. Secondly, most patient care records are paper-based and not well organized. Hence, they are usually in-complete and can hardly be accessed timely [2 – 5]. Thirdly, there is a lack of legal support to use electronic medical records, thus com-plicating the process of sharing and exchang-ing patient care records among hospitals.
However, there are drives to encourage sharing patient care records. First of all, as computer and communication technology ad-vances [6 – 13], applications on the Internet are booming and the population of the Word Wide Web (or web, for short) is increasing [10,14]. Most hospital users are familiar with the operations of web browsers such as Inter-net Explorer™ or Netscape Navigator™. A computer becomes a required tool in our daily life. It is time to make use of the Internet for sharing or exchanging patient care records among hospitals.
The other drive is that the BNHI may introduce the concept of the global budget system into the payment policy very soon because of its unbalanced budget. Under the global budget system, the payment may be dependent on the served population of a hos-pital and not completely dependent on the amount of medical services. Thus, enabling a chart summary (or patient care records) to be shared among the hospitals is essential not only for delivering the quality of medical care but also for saving medical expenses.
2. Methods
In this paper, we investigated methods in structuring documents, proposed a scheme for representing the chart summary of patient care records using the eXtended Markup Language (XML) [15] and explored the web
technology to facilitate the exchanges of a chart summary over the Internet.
2.1. XML-based patient care records
The Standard Generalized Markup Lan-guage (SGML) has been the standard docu-ment commonly used by governdocu-ment and military organizations since 1986. However, it is too complex to be used for general pur-poses. In order to establish a document stan-dard for web applications, the World Wide Web Consortium (W3C) proposed an eX-tended Markup Language (XML), which is a subset of the SGML [16]. Similar to SGML, XML provides tagging mechanisms for con-structing structures of documents. XML al-lows tags to appear at significant places in a document. Tagging is a powerful tool that enables a computer to capture the meaning and structure of the document and facilitate the search on the web. Most web applications can support XML documents.
An XML document can contain the fol-lowing parts: the structural specification of a document (i.e. document type definition, DTD), the instance of the document specified by a DTD and the presentation specification of the document (i.e. XML Style-sheet Lan-guage, XSL).
2.1.1. Document type definition (DTD) A DTD is a set of rules that describe structural components or elements. Each rule specifies the name of an element type and the valid subelements for that element. The name of the element can be the markups (or tags) in an XML-based document. The structure hierarchy of the document is created through the use of markups that specify the beginning and the ending of each element. An element may require attributes to annotate itself with additional information. Attributes can be defined by using an ATTLIST declaration.
Let us use an example to illustrate the specifi-cation of a DTD.
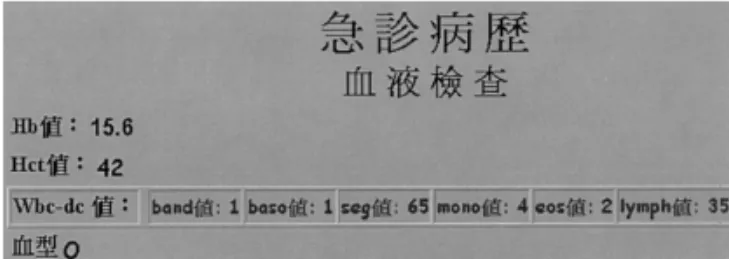
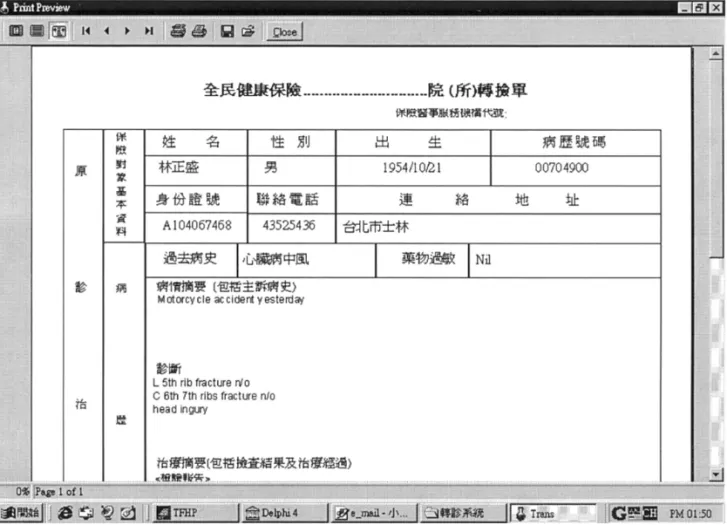
Refer to Fig. 1, there is a chart summary for an emergency transported patient. If it contains the patient’s hematology test, the hematology test must have items Hb, Wbc-dc and type. Again, the item Wbc-dc may fur-ther be annotated by detailed items such as band, baso, seg, mono, eos, and lymph. The type (blood) can only be one of the types A, O, B, AB and RH. The default is type ‘A’. The DTD specification of the chart summary is shown in Table 1.
As indicated in Table 1, the statement in the first line specifies that this is an XML document with version 1.0 encoded by the big5 Chinese character set. The second line and below describe the structure of elements including the name of each element and its subelement. In this example, Medical Records for Emergency use, EMR can have one or more than one set of elements ‘Hema-tology Test’. However, each ‘Hema‘Hema-tology Test’ must contain one and only one list of items ‘Hb,Wbc-dc, Type’. The attributes of item ‘wbc-dc’ can be declared using ‘AT-TLIST’. Note that, since the type can only be one of the types A, O, B, AB and RH, a vertical bar (‘ ’) is used in its declaration to indicate this option. The default value can also be declared in ATTLIST.
Through the DTD specification, an XML document can be validated. However, an XML document may not contain a DTD if it is well formed. This is described in the fol-lowing section.
Table 1 A DTD of a chart summary B?xml version=‘1.0’ encoding=‘big5’?\ EMR (HematologyTest)+\ B!ELEMENT HematologyTest (Hb,Wbc-dc,Type)\ B!ELEMENT Hb ( cPCDATA)\ B!ELEMENT Wbc-dc (EMPTY)\ B!ELEMENT
B!ATTLIST Wbc-dc band CDATA cREQUIRED
baso CDATA cREQUIRED seg CDATA cREQUIRED mono CDATA cREQUIRED eos CDATA cREQUIRED lymph CDATA cREQUIRED\ Type (EMPTY)\
B!ELEMENT
B!ATTLIST Type default (A O B AB RH) ‘A’\
The chart summary shown above is valid because it includes its DTD, named wfex.dtd. As mentioned, an XML document may not include the DTD part. If it is the case, the structures of elements in the document must be nested. That is, the starting tag and the end tag of a subelement must appear in be-tween the starting tag and the ending tag of the element that the subelement belongs. The XML document that meets the above re-quirement without a DTD is well formed. An XML document must be either valid or well formed.
2.1.3. XSL, the presentation of XML
documents
The second line in the XML-based chart summary shown in Table 2 specifies the pre-sentation style of the document. The presen-tation of XML documents can be specified using Style-sheet language (XSL). The XSL enables users to define their own presentation styles on their computer monitors. They can program their presentation templates using the XSL and then store them into different files with the extension ‘xsl’. In their XML documents, the corresponding xsl file must be included.
Again, refer to the example in Table 2, if the chart summary of the emergency trans-ported referral must be presented as shown in Fig. 1, the template can be programmed and saved as a ‘wfexxsl.xsl’ file. Note that the
second line in the XML-based chart
summary,
B?xml-stylesheet type=’text/xsl’ href = ’wfexxsl.xsl’?\
is used to include the xsl template file. The detailed content of the file is omitted because it is not our main focus here. Most commer-cial web browsers can now interpret the XSL specification. For example, Fig. 1 is the result 2.1.2. XML documents
An XML document consists of elements. There is one and only one root element. Each element must be labeled with a starting tag (Btag name\) and an ending tag (B/tag
name\). Refer to the example illustrated in
Fig. 2. The starting tag of the chart summary is specified as BEMR\ and the ending tag
as B/EMR\. More importantly, in an
XML document, the starting tag and the end tag of a subelement must appear in between the starting tag and the ending tag of the element that the subelement belongs. As the example described in the previous section, an instance of the XML-based chart summary corresponding to the DTD can be encoded as shown in Table 2.
of the interpretation of the chart summary by Internet Explore IE5.0 from Microsoft. 2.2. The representation of a chart summary
A referral initiation form (RIF) is a com-plete referral document shared between hos-pitals. It includes the referral’s chart summary, the reasons for referral, the infor-mation related to the physician who accepts the referral (accepting physician), the infor-mation related to the physician who refers the patient (referring physician), the treat-ment plan and the outcome of the treattreat-ment performed by the accepting physician. As shown in Fig. 5, the information shown at
the RIF is quite structured except for the chart summary.
The chart summary, abstracted from a set of patient care records is in fact somewhat arbitrary. It can be a full or minimum set of the patient care records. However, it must contain the essential information required for continual medical care for the emergency transported or referred patients. In our ap-proach, the chart summary is a basic unit that can be accessed or shared.
2.2.1. The structure of a chart summary The chart summary usually includes the information of the referral’s chief complaints, allergy, diagnosis, a care plan, the Glasgow
Table 2
An XML-based chart summary
B?xml version=‘1.0’ encoding=‘big5’?\ B?xml-stylesheet type=‘text/xsl’
href = ‘wfexxsl.xsl’?\
B!DOCTYPE EMR SYSTEM ‘wfex.dtd’\ BEMR\ BHematologyTest\ BHb\15.6B/Hb\ BHct\42B/Hct\ BWbc-dc\ Bband\1B/band\ Bbaso\1B/baso\ Bseg\65B/seg\ Bmono\4B/mono\ Beos\2B/eos\ Blymph\35B/lympho\ B/Wbc-dc\ BType\OB/Type\ B/HematologyTest \ B/EMR\
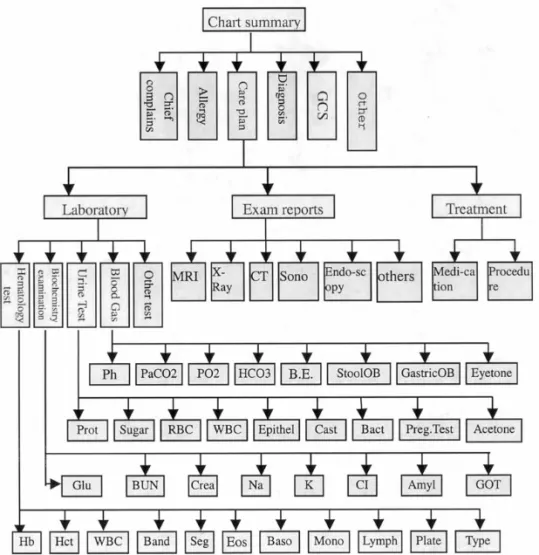
In the hierarchical tree, the chief com-plaints, allergy, diagnosis and the recommen-dations to accepting physicians are represented as leaf nodes. However, the GCS and the care plan are represented as branch nodes. This is because they contain structural elements. The GCS consists of the scale of eye-movement (E), the clearance of voice (V) and the response of motor mechanism (M). The care plan can usually be divided into laboratory test, radiology examination and treatment. Each part may contain several items. The hierarchical tree representing a chart summary is shown in Fig. 2. The tree is a graphical representation of a chart sum-mary and can easily be understood. It is a basic unit for sharing or exchanging patient care records among the hospitals in this pro-posed approach.
2.2.2. Representing a chart summary using
XML
A hierarchical tree of a chart summary can be transformed into an XML-based docu-ment corresponding to the tree. The transfor-mation can be performed by walking the tree in a depth-first order described below. Firstly, we can create an empty list, then, start walk-ing the tree from the root and add the root to an empty list. Then, we can proceed by the following steps:
1. remove the first node from the list, then adding all its children nodes to the end of the list if it has one or more.
2. Repeat step (1) until there is no more nodes in the list.
For each node, there is one and only one entry point and leaving point when walking the tree. The entry point corresponds to a starting tag and the leaving point corre-sponds to an ending tag. The transformation rules are described below.
1. The root is transformed to a starting tag corresponding to the entry of the document.
Coma Scale (GCS) and the recommendations for accepting physicians. The chief complaint represents how a patient describes his/her symptoms. The care plan describes what will be performed or what has been performed during the care of a patient and usually includes his/her laboratory tests, radiology (X-ray, endoscopy, sonograph, etc.) examina-tions and the treatment. The Glasgow Coma Scale (GCS) is used for evaluating the trauma of a patient’s nervous system. It is extremely important in dealing with emergency trans-ported patients.
A chart summary can be represented by a hierarchical tree in which each information element is represented by a node and the part-of relationship between nodes can be represented by a link. There are three kinds of nodes in the hierarchy. A root node has no parent node. It represents the starting entry point of the chart summary. There is one and only one root node in a hierarchy. A branch node must have children nodes that can be leaf nodes or branch nodes. A leaf node has no children. It is usually associated with a value or the raw data (such as strings, num-bers, etc.).
2. Create a starting tag for an element corre-sponding to a node to be removed from the list.
3. If the node is a leaf,
we include the value or raw data associ-ated with the node into the content of the element and create an ending tag for that element.
Otherwise (a branch node), if all its children nodes are removed from the list,
we create an ending tag for the element. 4. Repeat steps (2) and (3) until there are no
more nodes in the list.
The tree structure of a chart summary can directly be acquired when a user compiles the chart summary with the help of specially designed user interfaces. The tree representa-tion can then be transformed into the
corre-sponding XML-based one using the
transformation rules shown above. 2.2.3. Integrating XML-based chart
summaries into a database
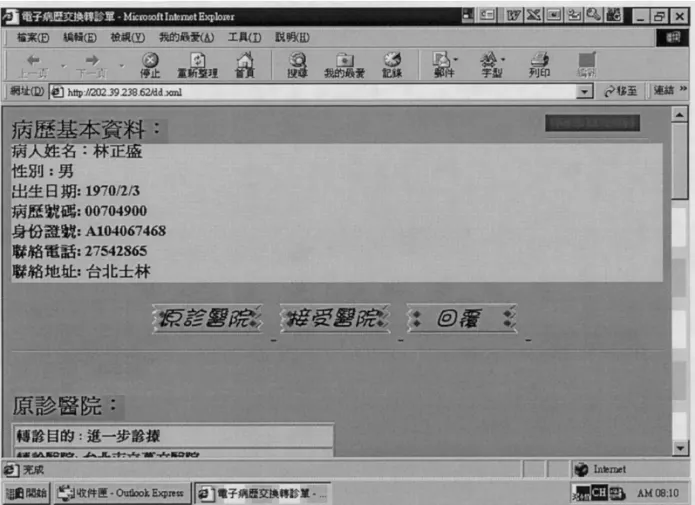
The XML-based chart summary is a media broadcasting on the Internet. When the me-dia is sent to a target hospital, it can be converted into the corresponding tree repre-sentation of the chart summary. The tree can be used to present the chart summary to physicians by a form-based user interface shown in Fig. 6 or if necessary, it can also be used to extract data items (elements or subelements) from the chart summary and save them into the database of the hospital information system.
The data items of an XML-based chart summary are defined by its associated DTD. Similarly, the data items of a database are defined by the database schema. The relation-ships between the data items in the XML-based chart summary and those in the database can be analyzed. We can classify the relationships into three groups based on the definitions of the data items.
Common relationships: two data items are
common if the data item defined in a database is identical (in terms of their semantics) to that defined in the corre-sponding XML-based one.
Deri6ed relationships: if the value of the
data item defined in a database can be derived from the one or more data items defined in the corresponding XML-based chart summary, the former can be derived from the latter by using a function.
Independent relationships: if the data item
defined in the XML-based chart summary is independent from any one of data items defined in the corresponding data-base.
The integration of an XML-based chart summary into a corresponding database in a hospital information system can be done by firstly identifying their relationships of data items. If they are common, the data item in the XML-based chart summary can be di-rectly inserted into the corresponding data-base. If they are derived, the function must be specified for deriving the data item in the database in terms of the data item(s) in the corresponding XML-based chart summary. If they are independent, a new database can be created to accommodate the data items of the XML-based chart summary.
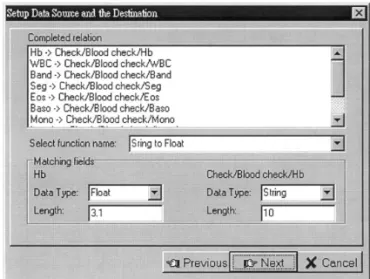
Let us illustrate the integration scheme by using the example shown in Table 2. In this example, suppose that the value of Hb is defined as string type in element Hematolo-gyTest in the DTD of the XML-based chart summary. However, it is defined as float type of attribute Hb in our database table. Therefore, their relationship is derived and a derived function Sting to Float, that con-verts a string to a float should be specified. The details of the operations for integration will be presented in Section 3.3.
3. Result
By using hierarchical trees to represent chart summaries and by using XML to con-vey the meaningful structures of chart sum-maries over the Internet, we developed a unified referral information system in which a referral’s chart summary or his/her RIF can be shared or exchanged over the Internet among hospitals. The details of the system are described in the following sections. 3.1. System description
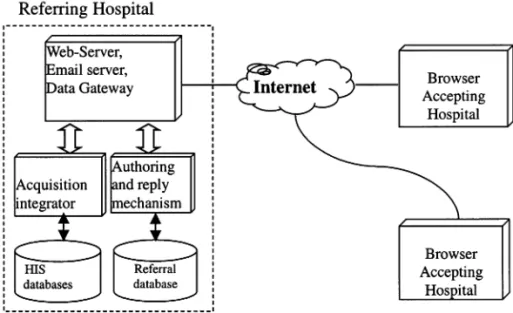
In the system, each hospital must have a web server and a gateway server as shown in Fig. 3. The server is used to provide inter-faces for manipulating the referral’s chart summary and to communicate with both the computer systems in the hospital and those outside the hospital. The gateway server is used to transform the requests or data from (to) the web server to (from) the clinical or administration information systems inside the hospital and to block unauthorized clients from accessing information stored in the hospital.
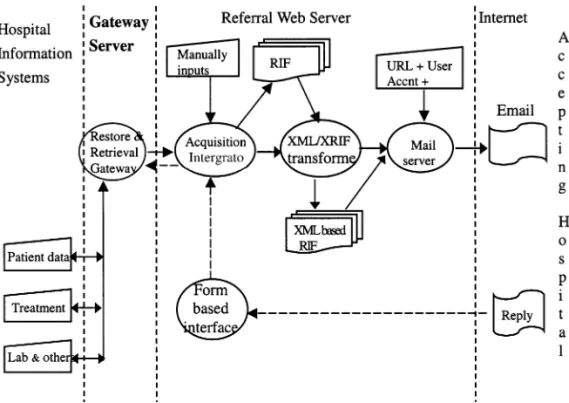
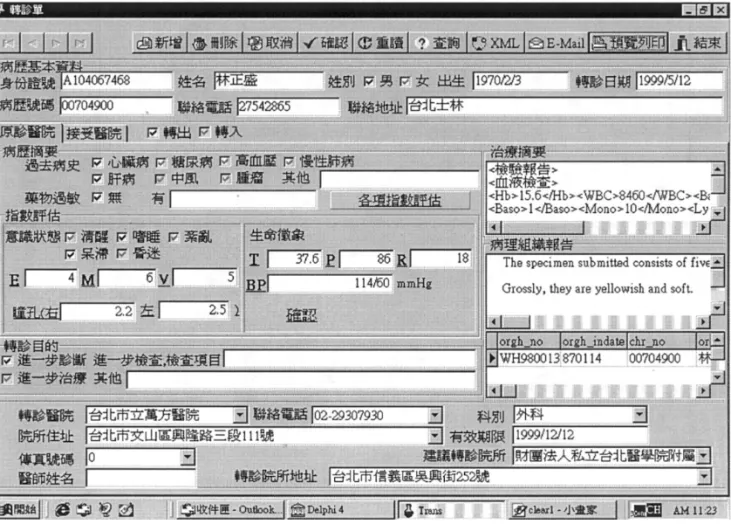
The major components of the referral in-formation system are shown in Fig. 4. The acquisition integrator helps a physician to collect the information required by a refer-ral’s RIF either from the existing hospital information systems or through manual in-put. It provides a form-based user interface as shown in Fig. 6. The form contains the information of a RIF. The physician can use the interface to compile the referral’s chart summary. In fact, the physician just needs to enter the referral’s unique identification to request the patient’s clinical information. The acquisition integrator sends the request to the gateway server. The gateway server dis-tributes the request and initiates the retrieval of the information from the corresponding hospital information systems. However, for information that isn’t stored in the hospital information systems, the interface also pro-vides authoring tools to assist the physician to manually input the information such as GCS, the outcome, etc. By means of the acquisition integrator, the acquired informa-tion of a RIF can be integrated and presented to users as forms. The users can then filter the information and compile the appropriate
Fig. 4. The major components of the web-based referral information system.
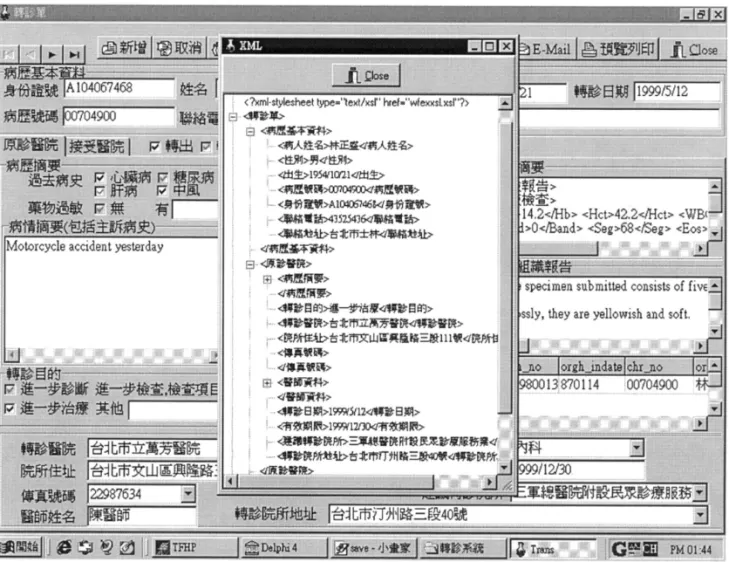
RIF which is sent to the RIF/XML trans-former for generation of an XML-based RIF. The RIF/XML transformer accepts a form-based RIF and then converts it into the corresponding hierarchical tree. A user can initiate the XML/RIF transformer by click-ing the XML button in Fig. 6. Based on the transformation rules described in the previ-ous section, the tree can be translated into the XML-based RIF as shown in Fig. 9. The XML-based RIF is the media for sharing and exchanging information between referring and accepting hospitals.
The e-mail server packs an XML-based RIF with a user account, the password asso-ciated with the account and the URL of the web server into an e-mail which is then sent to the accepting hospital over the Internet. Therefore, an authorized person of the ac-cepting hospital can log in to the web server with the URL, the user account and the password for reporting the referral’s medical
records back to the referring hospital. The user account and the password are assigned dynamically when the e-mail is generated to protect the patients’ care records from unau-thorized accesses.
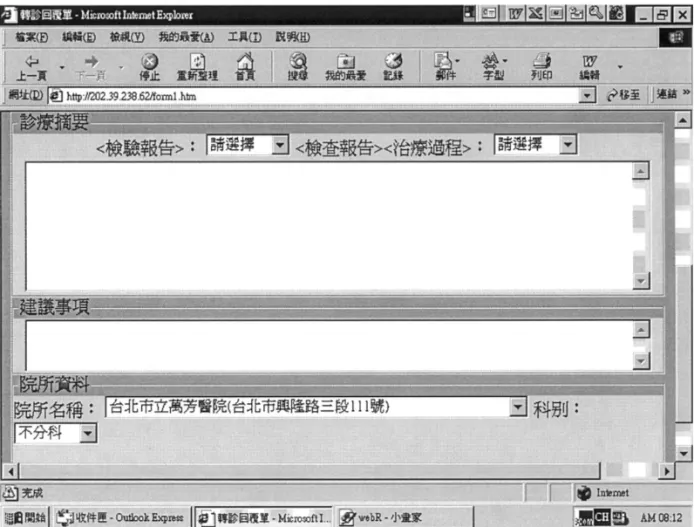
The authorized user of the accepting hospi-tal can report back to the referring hospihospi-tal the referral’s chart summary including his/her care plan, progress and the details of his/her treatment by directly filling forms as shown in Fig. 7 and Fig. 8 when logging in to the web server using the user account and pass-word. In contrast to the referring process, the acquisition integrator analyzes the items of the form-based RIF replied back from the accepting hospital and initiates requests to the gateway server for restoring the data items back to the hospital information sys-tems. Thus, the referring physician can re-view the referral’s RIF replied back from the accepting hospital at his/her computer for follow-up or other purposes.
3.2. The workflow of the referral information
system
The proposed system can easily be adapted into the existing system. It works as follows: 1. A physician prepares a patient’s chart summary using the form-based interface as shown in Fig. 6 when he/she decides to refer (or emergency transport) the pa-tient to the accepting hospital.
2. The summary of the patient’s medical care information can be collected auto-matically if the information is already stored in the hospital information sys-tems. The form-based interface also as-sists users to manually input the required information for compiling the chart summary.
3. After the physician has completed the chart summary, it is automatically sent to the referral service center.
4. When the patient comes to the desk of the referral service center, the center can access the patient’s chart summary and fill in the accepting hospital and other information that is required for referral management. The chart summary and other information are packed into the patient’s RIF. The RIF can be trans-formed into the corresponding hierarchi-cal tree (shown as Fig. 9) and the XML document, XRIF.
5. The RIF can be printed out and handed in to the patient. The patient’s XRIF plus the URL, user account and pass-word are also directly sent to the referral
Fig. 6. The form-based interface of acquisition integrator.
service center of the accepting hospital by e-mail over the Internet.
6. The patient must complete his registration at the desk of the referral service center of the accepting hospital. For operating con-venience, he/she can hand in his/her RIF to the coordinator of the center for regis-tration.
7. The coordinator confirms the patient by logging into his/her computer to check e-mails and saves the chart summary and the required information into the data-base corresponding to the hospital infor-mation system. He/she can also remote login to the web server of the referring hospital with the user account and pass-word. The coordinator can then help the patient to arrange a physician, and
for-ward the patient’s chart summary to the physician’s workstation.
8. The physician can review the patient’s chart summary which has been sent from the referring hospital at his/her worksta-tion. He/she can then perform diagnosis and make an appropriate care plan for further treatment.
9. When the patient has been discharged from the accepting hospital, the physician must prepare the chart summary plus the outcome of the treatment in reply to the referring hospital for that patient. The chart summary is sent to the referral service center. The coordinator of the center can upload the chart summary to the web server of the referring hospital using the provided function as shown in Fig. 8.
10. The chart summary replied from the ac-cepting hospital is tentatively stored in the web server of the referring hospital. After confirmation by the coordinator, the chart summary and RIF can be di-rected to the physician of the referring hospital for follow-up or other purposes. 3.3. The integrated referral information
system
The integration of an XML-based chart summary into a corresponding database in a hospital information system (HIS) can vary from one hospital to the other. Each hospital may have different platforms and vendors of database management systems. Also, the
defi-nition of an element in the XML-based chart summary may correspond to different data-base schemas of different HISs.
We designed a unified menu-based user interface to help users specify their data model and the relationships between the data items in the XML-based chart summary and those in their database. With reference to Fig. 10, the setup menu allows users to specify the database source patient personal data as the storage for the data items in the corresponding XML-based chart summary because the access mode is Write in.
Once the destination database source and the access mode have been setup, we can establish the connection to the database, ta-bles and attributes (or fields of the table) in
Fig. 8. A form-based interface for reply of referral information (II).
the HIS for saving the data items in the corresponding XML-based chart summary. Since the relationships of data items have been identified, if they are common, we sim-ply click on the data item and corresponding table and its field names. The selected items are shown on the window completed relation as shown in Fig. 11. However, if they are derived, the name of the function for deriving the data item in the database in terms of the data item(s) in the corresponding XML-based chart summary must be specified in the box selected function name as shown in Fig. 12.
By using the mechanisms shown above, we can integrate the XML-based chart sum-maries into the corresponding database in the existing hospital information systems.
4. Discussion and conclusion
The authors of this paper have developed a unified referral information system in which patient care records can be shared and inte-grated among hospitals over the Internet. It can not only facilitates the referral process but also maintains the integrity of a patient’s medical records from distributed hospitals. More importantly, in our approach, each sig-nificant piece of medical record is associated with a tag based on the syntax and semantics of the XML. The XML-based medical records enable a computer to capture the meaning and structure of the document on the web.
Currently the chart summary is paper-based and hence, it is time consuming and
incomplete [3 – 5]. However, as computer and communication technology advances and with applications on the Internet booming, the population of the Word Wide Web (or web, for short) is increasing [10,14]. Most hospital users are familiar with the opera-tions of web browsers such as Internet Ex-plorer or Navigator. It is time to implement a system in which patient care records can be shared among hospitals over the Internet.
The Taipei City Government established a computer-based emergency medical network system in 1998 [17,18]. The system can provide on-line queries to a number of avail-able intensive care unit (ICU) beds in the city hospitals. As the transported patients’
medi-cal records are usually acquired by telephone, referrals’ medical records cannot be trans-ported in time and are likely to be incom-plete. Our developed system compensates for this weakness. It supports exchange of medi-cal records among healthcare providers.
Sitting et al. developed a computer-based outpatient clinical referral system for the Brigham and Women’s Physician Hospital Organization (BWPHO) in Boston, USA. Based on their evaluation [19,20], the mean time required to complete a referral initiation form in the paper-based system and com-puter-based system are 125 s and 75 s, respec-tively. The mean number of items entered on the paper referral was 12.5 while the
Fig. 10. A set-up menu for database integration (I). Fig. 12. A set-up menu for database integration (II): for derived relationships.
puter system was 31. Although their system can speed up the referral process, the users tend to perform more entries. In our system we can reduce the number of manual inputs by automatically collecting the information that is already available in the hospital sys-tems at the time the physicians compile the referrals’ RIF.
More importantly, in our approach, each significant piece of medical record is associ-ated with a tag and is represented based on the syntax and semantics of the XML. Tag-ging is a powerful tool that enables a
com-puter to capture the meaning and structure of the document. XML-based medical records can pinpoint specific elements and filter the documents with particular characteristic ele-ments. Therefore, the XML-based medical records can be easily identified, verified and transformed from one system into the other in searches on the world wide web.
In addition to the description of patient care records, the standards for sharing and exchanging patient care records are also im-portant [21,22,8,23,24]. The Health Level Seven (HL7) is known for standards in ex-change of electronic medical care information in healthcare environments [2]. The HL7 is designed to standardize the format and pro-tocol for the exchange of certain key sets of data especially in financial information, diag-nosis and patient care flow among healthcare computer application systems. However, few hospital information systems in Taiwan were developed to conform to the standard and consequently, its implementation to exchange information is expansive.
Currently, most medical records are not explicitly segmented into meaningful pieces using the tagging markup techniques (e.g. BCT\CT reportB/CT\). The MEDLEE
Fig. 11. A set-up menu for database integration (II): table and fields selection.
system developed by the University of Co-lumbia [25 – 28] can extract the structures such as problem, body location, degree and some other item from chest radiology reports, mammography reports and some other medi-cal reports. The Unified Medimedi-cal Language System (UMLS) supported by the National Library of Medicine (NLM) contains a huge set of medical terms (Lexicons) and concepts (Meta-thesaurus) [29 – 33]. For future work, we will investigate the feasibility of making use of the MEDLEE and the UMLS as a standardized framework for restructuring pa-tient care records.
References
[1] The Bureau of National Health Insurance (BNHI), http://www.nhi.gov.tw/
[2] HL7: http://www.hl7.org
[3] IOM Institute of Medicine, The Computer-based Patient Records, An Essential Technology for Health Care, revised, National Academy Press, Washington DC, 1980.
[4] IOM, Reliability of National Hospital Discharge Survey Data. Report of a study, National Academy of Sciences, Washington, DC, 1980. [5] Richard S. Dick, B. Steen, Don E. Detmer, The
Computer-Based Patient Record: An Essential Technology for Health Care, revised, Committee on Improving the Patient Record, Institute of Medicine, 1997.
[6] C.G. Annetine, H.V. Dawkins, Adopting New Medical Technology, Committee on Technological Innovation in Medicine, Institute of Medicine, 1994.
[7] A.R. Bakker, The development of an integrated and cooperative hospital information systems. Med. Inform. 9 (1984) 135 – 142.
[8] P.J. Branger, J.S. Duisterhout, Communication in healthcare, Methods Inf. Med. 34 (1995) 244 – 252. [9] CORBA: http://www.omg.org
[10] J.J. Cimino, S.A. Socratous, P.D. Clayton, Inter-net as clinical information system: application de-velopment using the World Wide Web, J. Am. Med. Inform. Assoc. 2 (1995) 273 – 284.
[11] CPRI Computer Based Patient Record Institute, Guidelines for Establishing Information Security
Policies at Organizations Using Computer-based Patient Record Systems, CPRI, Schaumburg, Ill, 1995.
[12] C.T. Liu, C.C. Lin, H.S. Chen, et al., Design and evaluation of an integrated telemedicine system, J. Biomed. Eng.-Appl. Basis Commun. 9 (2) (1997) 125 – 133.
[13] C.T. Liu, C.C. Lin, H.S. Chen, et al., Design and evaluation of an integrated telemedicine system, J. Biomed. Eng.-Appl. Basis Commun. 9 (2) (1997) 125 – 133.
[14] C.C. Lin, J.R. Duann, C.T. Liu, H.S. Chen, et al., A unified multimedia database system to support tele-medicine, IEEE Trans. Inf. Technol. Biomed. 2 (3) (1998) 183 – 192.
[15] XML: A kind of document standard. http:// www.xml.org
[16] C.E. Kahn, Standard Generalized Markup Lan-guage for self-defining structured reports, Int. J. Med. Inf. 53 (2-3) (1999) 203 – 211.
[17] Department of Health, The Executive Yuan, R.O.C.: http://www.doh.gov.tw/english/
[18] Department of Health, Taipei City Government. A computer-based resources management system for emergency medical care. http:// emr.health.gov.tw
[19] D.F. Sitting, W.W. Stead, Computer-based physi-cian order entry: the state of the art, J. Am. Med. Inform. Assoc. 1 (1994) 108 – 123.
[20] D.F. Sitting, T.K. Gandhi, M. Franklin, et al., A computer-based outpatient clinical referral system, Int. J. Med. Inform. 55 (1999) (1999) 149 – 158. [21] AMIA (American Medical Informatics
Associa-tion Board of Directors), Standards for medical identifiers, codes, and messages needed to create an efficient computer-stored medical record, J. Am. Med. Inform. Assoc. 1 (1994) 1 – 7.
[22] G.J.E. De Moor, Standardization in medical in-formatics, 61-66, in: J.H. van Bemmel, A.T. Mc-Cray (Eds.), 1993 Yearbook of Medical Informatics, Schattauer Verlag, Stuttgart, 1993. [23] G.J.E. De Moor, Standardization in medical
in-formatics, 61-66, in: A.T. van Bemmel, S. McCray (Eds.), Yearbook of Medical Informatics, Schat-tauer Verlag, Stuttgart, 1993.
[24] C. Friedman, Towards a comprehensive medical language processing system: methods and issues. Proc. AMIA Annu. Fall Symp. (1997) 595 – 599. [25] G. Hripcsak, G.J. Kuperman, C. Friedman,
Ex-tracting findings from narrative reports: software transferability and sources of physician disagree-ment, Methods Inf. Med. 1988 (37) (1998) 1 – 7.
[26] NL. Jain, C. Friedman, Identification of findings suspicious for breast cancer based on natural lan-guage processing of mammogram reports. Proc AMIA Annu Fall Symp. (1997) 829 – 833 [27] MEDLEE http://cat.cpmc.columbia.edu/medlee [28] MEDLEE (DEMO): http://cat.cpmc.columbia.
edu/medleexml/demo
[29] S. Dessena, A.R. Mori, E. Galeazzi, Development of a cross-thesaurus with Internet-based refine-ment supported by UMLS, Int. J. Med. Inf. 53 (1) (1999) 29 – 41.
[30] S.B. Johnson, A semantic lexicon for medical lan-guage processing, J Am Med Inform Assoc. 6 (3) (1999) 205 – 218.
[31] National Library of Medicine. 1999. UMLS Knowledge Sources 10th Ed. http://uml-sks.nlm.nih.gov
[32] EM. Van Mulligen, UMLS-based access to CPR data. Medinfo., 9 (Pt 1) (1998) 166-70
[33] E.M. Van Mulligen, UMLS-based access to CPR data. Unified Medical Language Systems, Int J Med Inf. 53 (2-3) (1999) 125 – 131.