行政院國家科學委員會專題研究計畫 成果報告
探討半導體產業癌症及先天缺陷發生之風險
計畫類別: 個別型計畫 計畫編號: NSC92-2320-B-002-171- 執行期間: 92 年 08 月 01 日至 93 年 07 月 31 日 執行單位: 國立臺灣大學公共衛生學院職業醫學與工業衛生研究所 計畫主持人: 陳保中 計畫參與人員: 謝功毅 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 93 年 11 月 4 日
Exploring Risks for Reproductive Health and Cancer in Semiconductor Workers
Abstract
Problem: A retrospective cohort mortality and morbidity study was conducted to investigate the possible association between occupational exposure in semiconductor industry and cancer.
Methods: We obtained information of eight companies workers in the semiconductor cohort from the Bureauof Labor Insurance in Taiwan. Workers with cancer were identified after linking with databases of death and cancer registration from the Department of Health of Taiwan. The NIOSH life table analysis system was used to generate person-years-at-risk and the expected numbers of death for 94 categories of death, using Taiwan referent rates. Results: A total of 19,816male and 27,610 female workers had been employed during1980- 2000. From data linkage, we found 136 cancer cases and 60 cancer deaths. All malignant neoplasms were also less than expected, indicating apossible healthy worker effect. But there were slight increases of standardized mortality ratios and incidence ratios for cancers of nasopharynx, ovary, and leukemia with 95% confidence interval including 1.
Conclusions: Given that workers as generally still young, we recommend that the cohort need to be followed longer in the future.
Key words: standardized mortality ratios, standardized incidence ratios, cancer, semiconductor manufacture, Taiwan
Introduction
There are three categories in the semiconductor industry in Taiwan, and we’re going to aim at the design and manufacturing of semiconductor devices. Large quantities of potent gases, dopants, photoactive chemicals (photoresists, photoinitiators), solvents, and ionizing radiation are used in the semiconductor manufacturing process,1-4 but is uncertain about the
occurrence of cancer from exposures in this industry.
Previous research on cancer risks of working in the semiconductor industry is limited and has produced conflicting results.5-7 The aim of this study was to determine the cancer incidence and mortality of semiconductor workers in Taiwan, to evaluate suspected cancers and potential carcinogens in the semiconductor industry. It is worthy that to follow up the concerns that had been expressed, and to assess the need for further investigation.
Population and Methods
The original cohort consisted of 19,816 male and 27,610 female workers from eight
semiconductor companies in the Hsinchu Science-based Industrial Park (HSIP) which locates in the northwest of Taiwan. To be eligible for this cohort, workers in eight companies must be employed for a period of at least six months duringthe period 19 August 1980 to 21 June 2000. The identification (ID) numbers of cohort members were collected from the Bureauof Labor Insurance (BLI), and demographic data of date of birth, gender,and dates of new and change of employment, and retirement were retrieved. Then, each personal ID was linked with both the datasets of NationalMortality Registry (NMR) and cancer registry (NCR) from the Department of Health (DOH) of Taiwan.
The NMR has maintained a computerized file of all deathcertificates issued in Taiwan from 1980 to 2003. The underlying causeof death has been systematically coded according to the ninthrevision of the International Classification of Diseases (ICD9).The NCR was
established by record linkage of cancer registries 1980 through 2001, including identification number, dates of birth and death, places of living, codes of education and village, and ICD code. The cause of cancer was coded from the cancer registry by using the International Classification of Diseases for oncology (ICD-O). We included the following categories of neoplasm (ICD-9 code 140-239; ICD-O code 140-199; 981-984) as outcomes in our analyses. A total of 60 cancer deaths and 136 of cohort members occurredduring the follow up period, with a successful follow-up rateof 100%.
Age, sex, and calendar-time- specific standardized mortality ratios (SMRs) and incidence ratios (SIRs) were derived from the modified life table analysis system (LTAS) developed by NIOSH8,9 to calculate person-years at risk (PYAR) and the expected number of deaths, using of general population in Taiwan. For each worker in our study, the period of observation started after 6 months of employment in eight semiconductor companies, whichever was later, and ended at date of death, or December 31, 2003, whichever was earlier. In addition,
person-years were stratified by gender, duration of employment, calendar year and company. All analyses were done using the PC version of the LTAS10 [http://www.cdc.gov/niosh/ ltindex.html]. We calculated the total number of deaths or cancers observed, and the SMR or SIR, and the 95% confidence interval (two sided) for both. To calculate the dose response relationship, we divided the workers into three groups based on the duration of employment, that is, employment of less than or equal to 4 years, longer than 4 year but less than or equal to 10 years, and longer than 10 years. Length of employment analysis was carried out for cancer sites with a minimum of three deaths (data not shown). The dose-response relationship of period effect was also estimated. We divided the workers into four groups based on four time intervals: 1980-1989, 1990-1994, 1995-1999, and 2000-2003 (data not shown).
Results
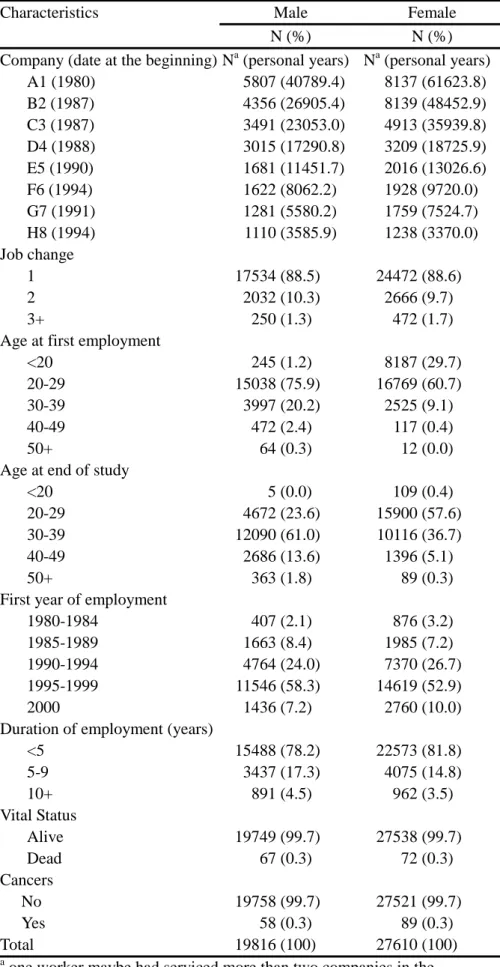
A total of 19,816 men and 27,610 female workers contributing men 136,718.6 and female 198,383.7 person-years were included in the study. Table 1 presents the distribution of the cohort by job change, age of first employment, age of study end, the first year of employment, duration of employment, vital status, cancers, and company. 25.3% male and 48.7% female workers came from Hsinchu county, and other workers came from different countries and cities. The duration of employment of the cohort is relatively short with a median of 3.1 (range 0.5–19.8) years. 89.6% of the cohort was first employed later than 1990. 67.1% of the cohort was 20-29 year old at first employment, and 90.2% of the cohort was 20-39 year old at study end. The median time since first employment, based on employment in the eight
semiconductor companies while they were operating, is 6 years. Almost all of the workers and person-years were from design and manufacturing of semiconductor devices or chips. Of the 13944 (26%) workers who had been employed at A1 company, 2348 (4.4%) had been employed at H8 company, and other workers had been employed at other six companies. But one worker maybe had serviced more than two companies in the eight semiconductor
companies.
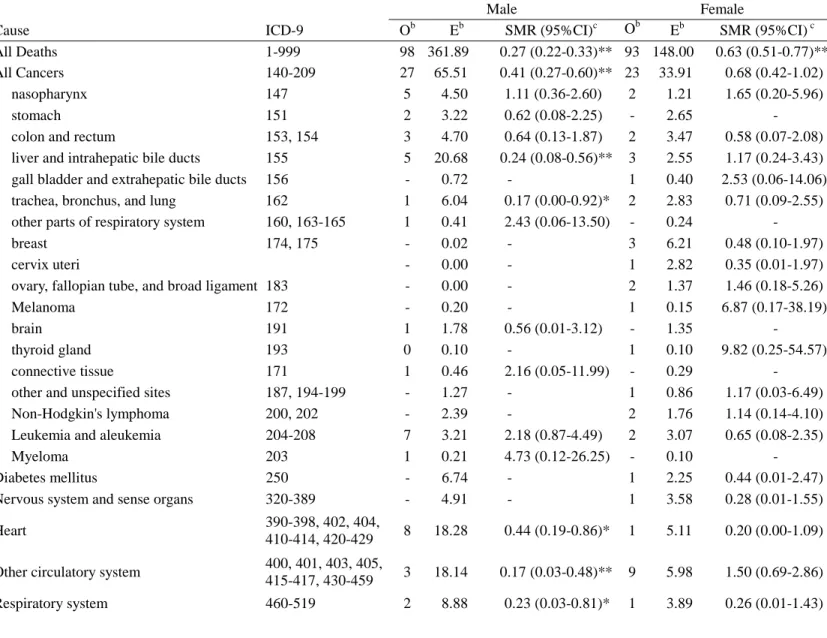
Table 2 shows the results of the analysis for all causes of death, and mortality from all causes was less than expected. Mortality from all malignant neoplasms was also less than expected. Among the outcomes of a priori interest, non-significant increases in mortality from
nasopharynx cancer, ovary cancer, and leukemia were observed. Within the major category of non-malignant neoplasm, mortality from other circulatory system, skin, and violence were non-significantly increased.
cancer was less than expected. Among the outcomes of a priori interest, non-significant increases in cancer morbidity from oral cavity, nasopharynx, other respiratory system, ovary, testes, other skin, connective tissue, and leukemia.
Discussion
We did not find any significant high risk for either the mortality or incidence of each cancer. There also was an obviously healthy worker effect in the semiconductor industry. (Table 2 and 3) However, we point out the possibility of cancers with potential carcinogens in this industry that justifies further investigation.
The observed numbers of all-cause death in males and in females were not significantly lower than the expected, and the observed numbers of cancers also were not significantly elevated. Firstly, these results could have been influenced with the small number of each cancer. It, however, is the best of our ability that the cohort was as complete as possible. A total of 47,426 workers in eight companies were completely collected from BLI,11 and members of the cohort were more than those in the past studies5-7 of the semiconductor industry. The cohort is shorter follow-up time, because the semiconductor industry was established for twenty years ago. Secondly, because we focused on the design and manufacturing of semiconductor devices only those processes were unique, Thirdly, cancer death and
registration from DOH were complete12 and accurate,13 due to the compulsory requirement by laws in Taiwan. The data of mortality or incidence rate in Taiwan was used in many mortality or morbidity studies,11-15 they had been verified in the past. However, we must take consideration into account of a healthy worker effect.
The healthy worker effect has been attributed to healthy individuals being selected for
employment.16,17 The discovery of a healthy worker effect was based on mortality studies, so that the proposition that occupational cohorts have lower disease incidence than the general population is speculative, and can only be clarified by concurrent analyses of disease
incidence and mortality.5-7 A reduced overall mortality for all cause deaths and morbidity for all cancer risks compared to the general population was also observed in our study, which was generally recognized as the so called healthy workers effect. The prevalence of tobacco smoking was 47.7% among male workers, and 5.9% among female workers in Taiwan.18 Approximately 9.3% of the female workers were smoking at the time of the survey.19 Smoking rate of female workers in the semiconductor industry was higher than female workers in Taiwan. Thus, a plausible explanation of the healthy worker effect, at least in the case of cancer, may be the selective employment of healthy workers from the source
population (healthy hire effect).
Large quantities of potent gases, dopants, photoactive chemicals (photoresists,
photoinitiators), solvents, and ionizing radiation are used in the semiconductor manufacturing process, but is uncertain about the occurrence of cancer from exposures in this industry. The toxic materials1 needed to make the wafer are staggering in amount and include highly
corrosive hydrochloric acid; metals such as arsenic, cadmium, and lead; volatile solvents such as methyl chloroform, toluene, benzene, acetone, and trichloroethylene; and toxic gases such as arsine. Many of these chemicals are known or probable human carcinogens in the
International Agency for Research on Cancer (IARC). The list of carcinogen group 1 included gallium, arsenic, beryllium, cadmium, benzene, ethylene oxide, benzedrine,and sulphuric acid mist1,22. Many by-products in the semiconductor manufacturing maybe were carcinogens, they were worthy to be explored.
two cohort studies5-7 had been followed up for more than 20 years, there is little consistency as to cancer mortality and morbidity in the semiconductor industry. Although we don’t know the cause of these discrepancies, it is worthy to mention any possible cancer related to the potential carcinogens. That is the occurrence of cancers equal to three or more cases and their SMR or SIR more than one in the two previous and our studies. Thus, digestive [150-158], respiratory [160-163], skin [172-173], and lymphatic and haematopoietic [200-208] were worthy to further discussion. Although a few cancer cases were observed, there was no cancer cluster in this study.
The limitations of cohort studies in the semiconductor industry in past were as follows. First, the follow-up time may be too short observe occupationally-related cancers. In addition, there was no information on exposure levels to carcinogens in the semiconductor companies. Moreover, those studies did not control for potential confounders, such as smoking, drinking, reproductive history, and dietary habits.
Nasopharyx, ovary, and testis cancers were found to have a potential risk in this study. The excess risk of the above-mentioned cancers was found in semiconductor studies. We had to identify those results, avoid overstatement, and findings must be interpreted more cautiously. There remains the possibility that some of this excess may be related to work at the
companies. It is inevitable that the workers are much younger whose average age is less than 50 years old and are not senior enough in the limitations of this study.
The confounders in exposure assessment and healthy worker effect caused lower evaluation of the effects in cancer risks in the semiconductor industry. So far, it is concluded that this study provided no evidence that occupational exposure in semiconductor industry was associated with human cancer risk. Therefore, it needs to follow up in the future.
References
1
Chepesiuk R. Where the chips fall: environmental health in the semiconductor industry. Environ Health Perspect 1999;107:A452-A457.
2
Wald PH, Jones JR. Semiconductor manufacturing: an introduction to processes and hazards. Am J Ind Med 1987;11:203-221.
3
LaDou J. Potential occupational health hazards in the microelectronics industry. Scand J Work Environ Health. 1983;9:42-46.
4
Chelton CF, Glowatz M, Mosovsky JA. Chemical hazards in the semiconductor Industry. IEEE Transactions on Education. 1991;34:269-288
5
Sorahan T, Waterhouse JAH, McKiernen MJ, Aston RHR. Cancer incidence and cancer mortality in a cohort of semiconductor workers. Br J Ind Med 1985;42:546-550.
6
Sorahan T, Pope DJ, McKiernen MJ. Cancer incidence and cancer mortality in a cohort of semiconductor workers: an update. Br J Ind Med 1992;49:215-216.
7
McElvenny DM, Darnton AJ, Hodgson JT, Clarke SD, Elliott RC, Osman J. Investigation of cancer incidence and mortality at a Scottish semiconductor manufacturing facility. Occup Med 2003;53:419-430.
8
Waxweiler RJ, Beaumont JJ, Henry JA, Brown DP, Robinson CF, Ness GO, et al. A modified life-table analysis system for cohort studies. J Occup Med 1983;25:115-124. 9
Steenland K, Beaumont J, Spaeth S, Brown D, Okun A, Jurcenko L, et al. New
developments in the Life Table Analysis System of the National Institute for Occupational Safety and Health. J Occup Med 1990;32:1091-1098.
10
Steenland K, Spaeth S, Cassinelli R 2nd, Laber P, Chang L, Koch K. NIOSH life table program for personal computers. Am J Ind Med 1998,34:517-518.
11
Wong RH, Chen PC, Du CL, Wang JD, Cheng TJ. An increased standardised mortality ratio for liver cancer among polyvinyl chloride workers in Taiwan. Occup Environ Med 2002;59:405-409.
12
Hsieh GY, Chen PC, Wang JD. Verification and correction of error for death registration data of the Department of Health R.O.C. between 1980 and 1997. Taiwan J Public Health. 2002;21:329-338.
13
Lu TH, Lee MC, Chou MC. Accuracy of cause of death coding in Taiwan: types of miscoding and effects on mortality statistics. Int J Epidemiol 2000;29:336-343. 14
Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, et al. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N Engl J Med 1997;336:1855-1859.
15
Chang YM, Tai CF, Yang SC, Chen CJ, Shih TS, Lin RS, et al. A cohort mortality study of workers exposed to chlorinated organic solvents in Taiwan. Ann Epidemiol
2003;13:652-660. 16
McMichael AJ. Standardized mortality ratios and the ‘‘healthy worker effect’’: scratching beneath the surface. J Occup Med 1976;18:165-168.
17
Wilcosky T, Wing S. The healthy worker effect. Selection of workers and work forces. Scand J Work Environ Health 1987;13:70-72.
18
Liang WM, Kuo HW, Wang CB. Prevalence of Tobacco Smoking, Drinking and Betel Nut Chewing among Taiwanese Workers in 1999. Mid-Taiwan J Med 2002;7:146-154. 19
Lin YP, Yen LL, Pan LY, Chang PC, Cheng TJ. Emerging epidemic in a rising industry: Cigarette smoking among Taiwanese female microelectronics workers. Public Health (Accepted).
20
Fowler BA, Yamauchi H, Conner EA, Akkerman M. Cancer risks for humans from exposure to the semiconductor metals. Scand J Work Environ Health 1993;19(Suppl 1):101-103.
21
Paustenbach DJ. Assessment of the developmental risks resulting from occupational exposure to select glycol ethers within the semiconductor industry. J Toxicol Environ Health 1988;23:29-75.
22
International Agency for Research on Cancer (IARC). IARC Monographs Programme on the Evaluation of Carcinogenic Risks to Humans. Available at
Table 1. The Characteristics for both male and female workers in the eight semiconductor companies
Characteristics Male Female N (%) N (%)
Company (date at the beginning) Na (personal years) Na (personal years) A1 (1980) 5807 (40789.4) 8137 (61623.8) B2 (1987) 4356 (26905.4) 8139 (48452.9) C3 (1987) 3491 (23053.0) 4913 (35939.8) D4 (1988) 3015 (17290.8) 3209 (18725.9) E5 (1990) 1681 (11451.7) 2016 (13026.6) F6 (1994) 1622 (8062.2) 1928 (9720.0) G7 (1991) 1281 (5580.2) 1759 (7524.7) H8 (1994) 1110 (3585.9) 1238 (3370.0) Job change 1 17534 (88.5) 24472 (88.6) 2 2032 (10.3) 2666 (9.7) 3+ 250 (1.3) 472 (1.7) Age at first employment
<20 245 (1.2) 8187 (29.7) 20-29 15038 (75.9) 16769 (60.7) 30-39 3997 (20.2) 2525 (9.1) 40-49 472 (2.4) 117 (0.4) 50+ 64 (0.3) 12 (0.0) Age at end of study
<20 5 (0.0) 109 (0.4) 20-29 4672 (23.6) 15900 (57.6) 30-39 12090 (61.0) 10116 (36.7) 40-49 2686 (13.6) 1396 (5.1) 50+ 363 (1.8) 89 (0.3) First year of employment
1980-1984 407 (2.1) 876 (3.2) 1985-1989 1663 (8.4) 1985 (7.2) 1990-1994 4764 (24.0) 7370 (26.7) 1995-1999 11546 (58.3) 14619 (52.9) 2000 1436 (7.2) 2760 (10.0) Duration of employment (years)
<5 15488 (78.2) 22573 (81.8) 5-9 3437 (17.3) 4075 (14.8) 10+ 891 (4.5) 962 (3.5) Vital Status Alive 19749 (99.7) 27538 (99.7) Dead 67 (0.3) 72 (0.3) Cancers No 19758 (99.7) 27521 (99.7) Yes 58 (0.3) 89 (0.3) Total 19816 (100) 27610 (100) a
one worker maybe had serviced more than two companies in the eight semiconductor companies.
Table 2. Observed and expected numbers of deaths for standardized mortality ratio (SMR) stratified by cause and gender in the eight semiconductor manufacturing companiesa
Male Female
Cause ICD-9 Ob Eb SMR (95%CI)c Ob Eb SMR (95%CI) c
All Deaths 1-999 98 361.89 0.27 (0.22-0.33)** 93 148.00 0.63 (0.51-0.77)**
All Cancers 140-209 27 65.51 0.41 (0.27-0.60)** 23 33.91 0.68 (0.42-1.02)
nasopharynx 147 5 4.50 1.11 (0.36-2.60) 2 1.21 1.65 (0.20-5.96)
stomach 151 2 3.22 0.62 (0.08-2.25) - 2.65 -
colon and rectum 153, 154 3 4.70 0.64 (0.13-1.87) 2 3.47 0.58 (0.07-2.08)
liver and intrahepatic bile ducts 155 5 20.68 0.24 (0.08-0.56)** 3 2.55 1.17 (0.24-3.43)
gall bladder and extrahepatic bile ducts 156 - 0.72 - 1 0.40 2.53 (0.06-14.06)
trachea, bronchus, and lung 162 1 6.04 0.17 (0.00-0.92)* 2 2.83 0.71 (0.09-2.55)
other parts of respiratory system 160, 163-165 1 0.41 2.43 (0.06-13.50) - 0.24 -
breast 174, 175 - 0.02 - 3 6.21 0.48 (0.10-1.97)
cervix uteri - 0.00 - 1 2.82 0.35 (0.01-1.97)
ovary, fallopian tube, and broad ligament 183 - 0.00 - 2 1.37 1.46 (0.18-5.26)
Melanoma 172 - 0.20 - 1 0.15 6.87 (0.17-38.19)
brain 191 1 1.78 0.56 (0.01-3.12) - 1.35 -
thyroid gland 193 0 0.10 - 1 0.10 9.82 (0.25-54.57)
connective tissue 171 1 0.46 2.16 (0.05-11.99) - 0.29 -
other and unspecified sites 187, 194-199 - 1.27 - 1 0.86 1.17 (0.03-6.49)
Non-Hodgkin's lymphoma 200, 202 - 2.39 - 2 1.76 1.14 (0.14-4.10)
Leukemia and aleukemia 204-208 7 3.21 2.18 (0.87-4.49) 2 3.07 0.65 (0.08-2.35)
Myeloma 203 1 0.21 4.73 (0.12-26.25) - 0.10 -
Diabetes mellitus 250 - 6.74 - 1 2.25 0.44 (0.01-2.47)
Nervous system and sense organs 320-389 - 4.91 - 1 3.58 0.28 (0.01-1.55)
Heart 390-398, 402, 404,
410-414, 420-429 8 18.28 0.44 (0.19-0.86)* 1 5.11 0.20 (0.00-1.09)
Other circulatory system 400, 401, 403, 405,
415-417, 430-459 3 18.14 0.17 (0.03-0.48)** 9 5.98 1.50 (0.69-2.86)
Digestive system 520-579 6 45.53 0.13 (0.05-0.29)** 2 5.56 0.36 (0.04-1.30)
Genitourinary system 580-629 - 4.12 - 2 2.55 0.79 (0.10-2.84)
Skin and subcutaneous tissue 680-709 - 0.80 - 4 2.43 1.65 (0.45-4.22)
Symptoms, signs and ill-defined conditions 780-796, 798, 799 2 21.73 0.09 (0.01-0.33)** 4 8.61 0.46 (0.13-1.19)
Accidents E800-E949 34 112.32 0.30 (0.21-0.43)** 23 41.47 0.55 (0.35-0.83)** Violence E950-E978 12 31.62 0.38 (0.20-0.66)** 18 17.64 1.02 (0.60-1.61) HIV-related 042-044 1 1.36 0.74 (0.02-4.10) - 0.13 - Other causes 001-009, 020-139, 240-246, 251-279, 630-678, 740-779, 794, 797, E980-E999, and blank 3 12.85 0.23 (0.05-0.68)** 4 9.20 0.43 (0.12-1.11)
a Person-years at risk and observed deaths began accruing in 1980 for the analysis based on rates for Taiwan. b O, observed; E, expected. ; c SMR, standardized mortality ratio, 95% CI, 95% confidence interval. * Two-sided Poisson, p , 0.05. ** Two-sided Poisson, p , 0.01.
Table 3. Observed and expected numbers of malignant neoplasms (Mn) for standardized incidence ratio (SIR) stratified by cause and gender in the eight semiconductor manufacturing companiesa
Male Female
Cause ICD-O Ob Eb SIR (95%CI)c Ob Eb SIR (95%CI) c
All Cancers 140-199, 980, 981
-984 51 84.76 0.60 (0.45-0.79)** 85 114.56 0.74 (0.59-0.92)**
oral cavity 140, 141, 143-146,
148, 149 1 14.66 0.07 (0.00-0.38)** 2 1.09 1.83 (0.22-6.60)
major salivary glands 142 1 0.45 2.25 (0.06-12.49) - 0.49 -
Nasopharynx 147 9 8.20 1.10 (0.50-2.08) 4 3.05 1.31 (0.36-3.35)
Stomach 151 3 4.13 0.73 (0.15-2.12) 2 3.14 0.64 (0.08-2.30)
small intestine 152 1 0.41 2.41 (0.06-13.41) - 0.22 -
colon and rectum 153, 154 6 7.97 0.70 (0.27-1.64) 3 5.95 0.50 (0.10-1.47)
liver and intrahepatic bile ducts 155 8 18.15 0.44 (0.19 -0.87)* 3 2.68 1.12 (0.23-3.28)
Pancreas 157 - 0.87 1 0.29 3.43 (0.09-19.05)
other parts of respiratory system 160, 163-165 3 1.27 2.37 (0.49-6.92) - 0.84 -
Breast 174, 175 - 0.07 - 16 22.46 0.71 (0.41-1.16)
cervix uteri 179, 180 - 0.00 - 22 36.02 0.61 (0.38-0.92)*
ovary, fallopian tube, and broad ligament 183 - 0.00 - 8 5.64 1.42 (0.61-2.80)
Testes 186 3 1.19 2.53 (0.52-7.40) - 0 -
kidney and other urinary organs 189 1 1.37 0.73 (0.02-4.07) - 0.76 -
Bladder 188 1 1.67 0.60 (0.02-3.32) 1 0.38 2.62 (0.07-14.58)
Other skin 173 2 2.16 0.93 (0.11-3.35) 3 2.35 1.28 (0.26-3.73)
Brain 191 1 2.44 0.41 (0.01-2.27) - 2.25 -
thyroid gland 193 - 2.21 - 13 12.27 1.06 (0.56-1.81)
connective tissue 171 2 1.30 1.54 (0.19-5.57) - 1.38 -
other and unspecified sites 187, 194-199 1 3.85 0.26 (0.01-1.44) 4 2.96 1.35 (0.37 -3.46)
Leukemia and aleukemia 169, 980, 981-984 6 3.27 1.84 (0.67-4.00) 2 3.40 0.59 (0.07-2.13)
a Person-years at risk and observed cancers began accruing in 1980 for the analysis based on rates for Taiwan. b O, observed; E, expected.
c SIR, standardized incidence ratio, 95% CI, 95% confidence interval. * Two-sided Poisson, p , 0.05.