行政院國家科學委員會專題研究計畫 成果報告
與胃癌、消化性潰瘍及宿主免疫力相關的特異性幽門螺旋桿
菌菌株蛋白之研究
計畫類別: 個別型計畫 計畫編號: NSC92-2314-B-002-142- 執行期間: 92 年 08 月 01 日至 93 年 07 月 31 日 執行單位: 國立臺灣大學醫學院內科 計畫主持人: 楊智欽 共同主持人: 蔡有光 計畫參與人員: 楊智欽、蔡有光 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 1 月 3 日
中文摘要
人類幽門螺旋桿菌 (Helicobacter pylori) 是一種常見的感染,且與胃炎,胃潰瘍 及胃部的癌症有密切的關係。幽門螺旋桿菌所引起的致病機轉目前仍不清楚。由 於此種感染普遍存在於正常及胃部有症狀的病人中,因此其導致不同程度疾病的 致病機轉可能與宿主因子以及Hp 菌株本身毒性因子兩者都有相關。我們之前也 發現一個 H. pylori 菌株蛋白和胃淋巴瘤以及另一個菌株蛋白和胃癌可能相關而 分別發表於文獻中。最近我們研究發現使用二維電冰法來分離菌株蛋白質可以較 之前使用的 1-D SDS-PAGE 有更好的解析能力,足以找出更多具有重要性的因 子。為了更進一步了解 H. pylori 感染宿主的致病機轉,我們將自門診內視鏡檢 中選取診斷為 Hp 陽性之胃部疾病(胃炎、消化性潰瘍、胃癌)為對象,同時對胃 部各夾取黏膜檢體送組織切片判定疾病類型且培養 H. pylori。將 H. pylori 在厭氧 的狀態下進行液體培養,然後萃取分泌性蛋白質。將萃取的蛋白質用二維電泳法 將蛋白質分離開來,再用銀染色法染色,最後分析不同疾病的 H. pylori 蛋白質, 再以液相層析—串聯式質譜儀做這些蛋白質樣本的身份鑑定分析,找出可能產生 不同臨床疾病有關的特異性菌株蛋白。結果我們發現:(1)菌體蛋白質:由十二 指腸潰瘍患者的幽門螺旋桿菌之二維電泳分析圖發現有 3 種蛋白質為十二指腸 潰瘍患者的特異性蛋白質而其它種類病(胃潰瘍、胃炎、胃癌)則沒有。2 種蛋白 質為胃炎患者的特異性蛋白質。2 種蛋白質為胃癌患者的特異性蛋白質。(2)分泌 性蛋白質:由胃炎患者的幽門螺旋桿菌之二維電泳分析圖發現2 種蛋白質為胃炎 患者的特異性蛋白質;1 種蛋白質為胃癌患者的特異性蛋白質。 關鍵詞:幽門螺旋桿菌、小鼠動物模式、主要抗原英文摘要
Recent studies strongly suggest that chronic infection with H. pylori is tightly associated with chronic gastritis, peptic ulcer, and gastric carcinoma. However, only a part of infected people develop signs and symptoms of gastric pathology. Thus, both host and microbial factors may lead to different outcomes of infection. Perhaps the greatest concern with regard to infection with H. pylori is the increased risk for the development of gastric cancers in adulthood. This is particularly relevant because infection dating from childhood appears to enhance the risk of carcinogenesis. Recently, in a continuous epidemiological study for the H. pylori infection in the adolescence and children, we have found a steady proportion of these young individuals year by year having the ability to produce spontaneous clearance of the H.
pylori infection. Meanwhile, in another studies, we also have identified two candidate
proteins, one from the patients with gastric cancer, the other from the patients with gastric MALToma. In a pilot study, however, we have found many protein bands which demonstrated on a 1-D SDS-PAGE can be separated more clearly to several protein spots by 2-D gel electrophoresis plus immunoblotting detection. In this project, using technology of proteomics, we have found 1) whole-cell proteins: Three protein spots on the 2-DE gel were found in the H. pylori isolated from the patients with duodenal ulcer. These 3 protein spots were not found in the strains related to the patients with gastric ulcer and gastric cancer. Two protein spots on the 2-DE gel were specifically associated with chronic gastritis only. There were 2 protein spots on the 2-DE gel of H. pylori isolated from the patients with gastric cancer. These 2 protein spots were not noted in the strains related to the patients with other condition. 2) Secreted proteins: Two proteins spots were found from the H. pylori strains specifically related to the patients with chronic gastritis only. Meanwhile, there were one protein spot on the 2-DE gel of H. pylori isolated from the patients with gastric cancer. This protein spot was not noted in the strain associated with other disease patterns. This study will provide further insight not only in understanding of pathogenic mechanism in H. pylori infection, but also the direction of developing new therapies or vaccines.
Introduction
Helicobacter pylori, a Gram-negative spiral bacterium, has been first isolated
from a patient with chronic active gastritis since 1982 [1]. Recent studies strongly suggest that chronic infection with H. pylori is tightly associated with chronic gastritis, peptic ulcer, and gastric carcinoma [2-4]. However, only a part of infected people develop signs and symptoms of gastric pathology. Thus, both host and microbial factors may lead to different outcomes of infection. In spite of high prevalence in general population and increasing clinical attention has been paid on this infection, the knowledge of pathogenic mechanism of H. pylori infection is still limited.
The complexity of host-Helicobacter relationships with large variations in the severity of disease in infected population suggests that it is dependent on uncharacterized host factors, and the potentially specific disease related bacterial virulence factors. The role of cell-mediated immune responses in Helicobacter disease is still not clear. At present, it is known that H. pylori induces an infiltration with T lymphocytes, plasma cells, mononuclear phagocytes and neutrophils. Furthermore, expression of cytokines such as tumor necrosis factor (TNF), IL-1, IL-6 and IL-8 is also enhanced by the infection [5-9]. However, it is not known how the immune response and the mechanisms behind it related to disease outcome. Based on the presence of these two virulence determinants, strains can be divided into two major groups [10]; type I bacteria possess cagA and express both CagA and VacA, and type II bacteria do not have cagA and do not produce these proteins. Type I bacteria are found to link to duodenal ulceration and other severe gastric pathology. However, in the recent study [11], we found that Taiwanese patients are predominantly (98.2%) infected with cagA+ strains. Together with the extremely high prevalence of cagA+
isolates in Taiwan and their genetic divergence from other published strains, it is speculated that there may be specific populations of H. pylori strains within Taiwan. In another studies, we also have identified two candidate proteins, one from the patients with gastric cancer [12], the other from the patients with gastric MALToma [13]. In a pilot study, however, we have found many protein bands which demonstrated on a 1-D SDS-PAGE can be separated more clearly to several protein spots by 2-D gel electrophoresis plus immunoblotting detection. In this project, using technology of proteomics, we have tried to identify the possible candidates of H.
pylori antigens or proteins.
The aim of this study was to identify H. pylori proteins potentially and specifically associated with gastric cancer, peptic ulcer or gastritis.
Materials and Methods
In order to identify the possible disease specific proteins (or immunogens), different clinical isolated strains were analyzed by 2-D PAGE and detected by immunoblot analysis. The H. pylori bacterial strains were from ATCC standard strain and previously collected clinical isolates from 10 patients with chronic gastritis only, 10 patients with gastric ulcer, 10 patients from gastric cancer and 10 patients with duodenal ulcer.
1.) Extraction of bacterial proteins
The H. pylori bacterial strains were culture in Brucella broth containing 0.2% β-cyclodextrin without serum supplement for 3 days at 37℃ in a microaerophilic atmosphere (5% O2, 10% CO2, 85% N2). The cells were
pelleted by centrifugation at 3000rpm for 20 min, and then resuspended and sonicated in 1 ml of lysis buffer (20mM Tris, pH 7.5, 2% sodium lauroyl sarcosine). [14-15] Whole-cell protein extracts were obtained by centrifugation at 16000 x g 5 min. Secreted proteins were obtained from culture supernatant. [13]
2.) Two-dimensional polyacrylamide gel electrophoresis (2-D PAGE)
Protein-cyanine dye labeling - The protein samples were then
solubilzed in in lysis buffer (4M urea, 2M thiourea, 2% CHAPS, 2% SB3-10, 0.5% Triton X-100) by vortexing at room temperature for 1-2 h. The pH was adjusted to pH 8.5 for dye labeling. The 0.2 mM dye solution was added to final ratio of 50 mg protein: 200 nmol dye. The samples were vortexed briefly and left to stand for 15 min at room temperature and were then frozen at -70℃ for later use.
Isoelectric focusing (IEF) - The H. pylori proteins were resolved by IEF
on precast 17-cm Immobiline Dry strips with a linear pH gradient, (pH 4-7). The IPG strips were rehydrated, according to the manufacturer’s instructions, for 12 h at 25℃, together with the H. pylori proteins or cyanine dye-labeled proteins (approx 150 µg per strip) in a 200 µl solution containing 9 M urea, 4%(w/v) CHAPS, 2% (w/v) dithiotreitol, 2% (v/v) IPG buffer pH 4~7. IEF was performed in an IPGphor focusing apparatus (Amersham Pharmacia Biotech) for a total of 100 kV·h.
SDS polyacrylamide gel electrophoresis (SDS-PAGE)- Before a 2-DE
was started, IPG strips were equilibrated fro two intervals of 20 min each in a equilibration solution (50 mM Tris-HCl, pH 8.8 6M urea, 30% [v/v]glycerol, 1% w/v SDS, 1 % dithiotreitol). IPG strips were then
applied on the top (2/3) of 10% and bottom (1/3) of 12.5 % SDS-PAGE, then separation of proteins carried out under the same conditions as described for 1-D SDS-PAGE. After SDS-PAGE, cyanine dye-labelled protein gels were scanned directly using a F-5000 fluorescence scanner (Fuji) for image analysis. Gels were then processed for silver staining and followed by fluorescence image scanning.
3.) Grouping assay of 2-D immunoblot
Polypeptides resolved by 2-DE were electrophoretically transferred to PVDF membranes and residual binding capacity was blocked by BSA proteins. Membranes were placed in polyethylene bags and overlaid with; (i) pooled serum samples (n = 10) obtained from patients of gastritis only, and positive for H. pylori infection by culture of gastric biopsy; (ii) pooled serum samples (n = 10) obtained from patients of gastric ulcer, positive for
H. pylori infection; (iii) pooled serum samples (n = 10) obtained from
patients of gastric cancer, H. pylori positive; and (iv) pooled serum samples (n = 10) obtained from patients of duodenal ulcer, H. pylori positive. Sera were diluted 1:1000 in 10 ml incubation buffer and the incubation time would be 2 h at 25℃. Bound antibodies were detected by adding a 50 mM sodium acetate buffer (pH 5.0) containing 0.04% 3-amino-9-ethylearbazole and 0.015% H2O2.
4.) Difference assay of 2-D immunoblot
Polypeptides resolved by 2-DE were electrophoretically transferred to PVDF membranes and residual binding capacity was blocked by BSA proteins. Membranes were placed in polyethylene bags and overlaid with; (i) different serum samples (n = 10) obtained from patients of gastritis only, and positive for H. pylori infection by culture of gastric biopsy; (ii) different serum samples (n = 10) obtained from patients of gastric ulcer, positive for H. pylori infection; (iii) different serum samples (n = 10) obtained from patients of gastric cancer, H. pylori positive; and (iv) different serum samples (n = 10) obtained from patients of duodenal ulcer,
H. pylori positive. Sera were diluted 1:1000 in 10 ml incubation buffer and
the incubation time would be 2 h at 25℃. Bound antibodies were detected by adding a 50 mM sodium acetate buffer (pH 5.0) containing 0.04% 3-amino-9-ethylearbazole and 0.015% H2O2.
The spots, showing distinct antibody reactivity with patients were selected for the analysis of LC/MS/MS spectrometer. Briefly, gel pieces were washed with 100 mM ammonium hydrogen carbonate solution and acetonitrile followed by swelling in the digestion buffer containing 50 mM ammonium hydrogen carbonate, and trypsin at 37℃ overnight. The peptides were extracted with 5% formic acid and acetonitrile. Peptide sequences were obtained with a LCQ ion trap mass spectrometer (Finnigan). The acquired raw data were interpreted using SEQUEST browser software to search against published H. pylori protein or/and genome databases.
Results
Totally, the proteins extracted from 40 H. pylori isolates (10 for chronic gastritis only, 10 for DU, 10 for GU, and 10 for gastric cancer) were analyzed by 2-Dimension electrophoresis. The proteins were divided into two groups, whole-cell proteins and secreted proteins.
(1) whole-cell proteins
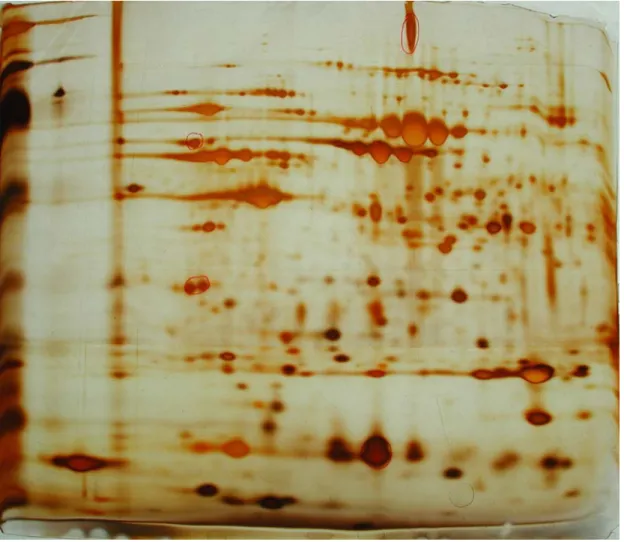
Three protein spots on the 2-DE gel were found in the H. pylori isolated from the patients with duodenal ulcer (Fig. 1). These 3 protein spots were not found in the strains related to the patients with gastric ulcer and gastric cancer. Two protein spots on the 2-DE gel were specifically associated with chronic gastritis only (Fig. 2). There were 2 protein spots on the 2-DE gel of H. pylori isolated from the patients with gastric cancer (Fig. 3). These 2 protein spots were not noted in the strains related to the patients with other condition.
(2) Secreted proteins
Two proteins spots were found from the H. pylori strains specifically related to the patients with chronic gastritis only (Fig. 4). Meanwhile, there were one protein spot on the 2-DE gel of H. pylori isolated from the patients with gastric cancer. This protein spot was not noted in the strain associated with other disease patterns (Fig. 5).
These specific protein spots on the 2-DE gel were cut down for in –gel digestion. The products were analyzed by LC/MS/MS spectrometer. These included heat shock proteins, chemotaxic proteins and proline peptidase.
Discussion
H. pylori has many putative virulence factors that may involved in the
pathogenicity. Two virulence factors associated with peptic ulceration were reported: the presence of a cytotoxin-associated gene (cagA) [16-17] and vacuolating cytotoxin activity (and vacA genotype) [18-21]. Although cagA does not directly mediate toxin activity [22], cagA+ strains are found significantly higher prevalence from patients
with duodenal ulcer disease than from patients with non-ulcer dyspepsia [16-17, 23-24]. The vacA protein (VacA), in contrast, has been shown to induce cytoplasmic vacuolation in vitro [25] and about 50% of H. pylori strains have vacuolating cytotoxic activity in cultured cells [25-26]. However, in the recent study [11], we found that Taiwanese patients are predominantly (98.2%) infected with cagA+ strains.
Although a strong association (100%) between cagA+ H. pylori and duodenal
ulceration is confirmed in this study, we also found that a very high proportion (94.4%) of non-ulcer dyspepsia patients were infected with cagA+ strains. These results thus
suggest that the prevalence of cagA+ strains may be different in particular geographic
or ethnic groups and that the presence of cagA cannot be used as a single reliable marker for predicting the high-risk patients in Taiwan.
Recently, in a continuous epidemiological study for the H. pylori infection in the adolescence and children, we have found a steady proportion of these young individuals year by year having the ability to produce spontaneous clearance of the H.
pylori infection. Meanwhile, in another studies, we also have identified two candidate
proteins, one from the patients with gastric cancer [12], the other from the patients with gastric MALToma [13]. Perhaps the greatest concern with regard to infection with H. pylori is the increased risk for the development of gastric cancers in adulthood. This is particularly relevant because infection dating from childhood appears to enhance the risk of carcinogenesis [27]. Because H. pylori infection is contracted primarily during the childhood years, additional epidemiological studies among pediatric populations are imperative [28].
The immunoregulatory and proinflammatory cytokines induced by H. pylori may influence the nature of the local T cell response. It is thought that helper T (Th) cells can be divided into two subsets, Th1, and Th2. The Th1 subset promotes cell-mediated immunity by producing mainly IL-2 and interferon-gamma (IFN-γ), and the Th2 subset, which is important for antibody response produces IL-4, IL-5 and IL-13. Evidences in recent research have strongly suggested that T cell mediated immune response may play an important role in induction of disease in H. pylori infection [29-34]. However, it is still not clear whether different outcome of the disease is modulated by the different type of T cell immune response although some
studies suggested that Th1 type cellular response may involved in the Helicobacter disease [34-37]. Little is known about whether Th2 response can be protective or whether modulation of these response can change the outcome of infection.
Meanwhile we have found many protein bands which demonstrated on a 1-D SDS-PAGE can be separated more clearly to several protein spots by 2-D gel electrophoresis plus immunoblotting detection. Using technology of proteomics, molecular biology, we have found two specific H. pylori proteins potentially specific associated with gastric cancer. The first protein (GC1) was a 36.6 kD chemotaxia protein that observed in 50% of gastric cancer patients. The second protein (GC2) spot was in isoelectric variant of a 40.8 kD proline peptidase that was seen in 60% of gastric cancer patient. However, their biological roles in pathogenesis of H. pylori infection need to be further investigated.
References:
1. Warren JR, Marshall BJ. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1993;I:1273-5.
2. Blaser MJ. Gastric Campylobacter-like organisms, gastritis and peptic
ulcer disease. Gastroenterology 1987;93: 371-83.
3. Blaser MJ. Helicobacter pylori: its role in disease. Clin Infect Dis
1992;15: 386-93.
4. Parsonnet J, Friedman GD, Vandersteen DG, Chang Y, Vogelman JH, Orentreich N, Sibley RK. Helicobacter pylori infection and risk of gastric carcinoma. N Engl J Med 1994;325:1127-31.
5. Bodger K, and Crabtree JE. Helicobacter pylori and gastric inflammation. Br Med Bull 1998;54:139-50.
6. Crabtree JE, Peichl P, Wyatt, JI, Stach U, LindleyIJD. Gastric
interleukin-8 and IgA interleukin-8 antibodies in Helicobacter pylori infection. Scand. J. Immunol. 1993;37:65-70.
7. Crowe SE, Alvarez L, Dytoc M, Hunt RH, Muller M, Sherman P, Patel J, Jin Y, Ernst PB. Expression of interleukin 8 and CD54 by human gastric epithelium after Helicobacter pylori infection in vitro. Gastroenterology 1995;108:65-74.
8. Fan XG, Yakoob J, Fan XJ, Keeling PW. Enhanced T-helper 2 lymphocyte responses: immune mechanism of Helicobacter pylori infection. Ir J Med Sci 1996;165:37-9.
9. Lindholm C, Quiding-Jarbrink M, Lonroth H, Hamlet A, Svennerholm A. Local cytokine response in Helicobacter pylori-infected subjects. Infect Immun 1998;66:5964-71.
10. Xiang Z, Censini S, Bayeli PF, et al. Analysis of expression of CagA and VacA virulence factors in 43 strains of Helicobacter pylori reveals that clinical isolates can be divided into two major types and that CagA is not necessary for expression of the vacuolating cytotoxin. Infect Immun 1995;63:94-8.
11. Yang JC, Wang TH, Wang HJ, et al. Genetic analysis of the cytotoxin-associated gene and the vacuolating toxin gene in
Helicobacyer pylori strains isolated from Taiwanese patients. Am J
Gastroenterol 1997;92:1316-21.
12. Wang JT, Chang CS, Lee CZ, Yang JC, Lin JT, Wang TH. Antibody to a Helicobacter pylori species specific antigen in patients with
1998;244:360-363.
13. Chang CS, Chen LT, Yang JC, Lin JT, Chang KC, Wang JT. Isolation of a Helicobacter pylori protein, FldA, associated with mucosa-associated lymphoid tissue lymphoma of the stomach. Gastroenterology
1999;117:82-88.
14. Masaru Y, Yoshino W, Yoshinao K, Toshiyuki I, Kazuhisa M, Akira M, Takashi U, Tsutomu C, Toru K. Cloning and characterization of a novel membrane-associated antigenic protein of Helicobacter pylori. Infect. Immun. 1999; 67:286-293.
15. Wang JT, Chang CS, Yang JC, Lin JT, Wang TH. Optimized conditions for growth and fermentation of Helicobacter pylori. J Microbiol Immunol Infect 1998;31:146-150.
16. Covacci A, Censini S, Bugnoli M, et al. Molecular characterization of the 128-kDa immunodominant antigen of Helicobacter pylori
associated with cytotoxicity and duodenal ulcer. Proc Natl Sci USA 1993;90:5791-5.
17. Crabtree JE, Taylor JD, Wyatt JI, et al. Mucosal IgA recongnition of
Helicobacter pylori 120 kDa protein. peptic ulceration and gastric
pathology. Lancet 1991;338:332-5.
18. Cover TL, Blaser MJ. Purification and characterization of the vacuolating toxin from Helicobacter pylori. J Biol Chem 1992;267:10570-5.
19. Telford JL, Ghiara P, Dell'Orco M, et al. Gene structure of the
Helicobacter pylori cytotoxin and evidence of its key role in gastric
disease. J Exp Med 1994;179 : 1653-58.
20. Cover TL, Tummuru MK, Cao P, et al. Divergence of genetic sequenced for the vacuolating cytotoxin among Helicobacter pylori strain. J Biol Chem 1994;269:10566-10573.
21. Phadnis SH, Ilver D, Janzon L, et al. The pathological significance and molecular characterization of the vacuolating toxin gene of
Helicobacter pylori. Infect Immun 1994;62:1557-1565.
22. Tummuru MKR, Cover TL, Blaser MJ. Mutation of the
cytotoxin-associated cagA gene does not affect the vacuolating cytotoxin activity of Helicobacter pylori. Infect Immun
1994;62:2609-13.
23. Cover TL, Dooley CP, Blaser MJ. Characterization and human serologic response to proteins in Helicobacter pylori broth culture supernatants with vacuolizing cytotoxin activity. Infect Immun
1990;58:603-10.
24. Cover TL, Glupczynski Y, Lage AP, et al. Serologic detection of infect with cagA+ Helicobacter pylori strains. J Clin Microbiol
1995;33:1496-500.
25. Leunk RD, Johnson PT, David BC, et al. Cytotoxic activity in broth culture filtrates of Campylobacter pylori. J Med Microbiol
1988;26:93-9.
26. Cover Tl, Cao P, Lind CD, et al. Correlation between vacuolating cytotoxin production by Helicobacter pylori isolates in vitro and in vivo. Infecct Immun 1993;61:5008-12.
27. Mitchell HM, Li YY, Hu PJ, et al. Epidemiology of Helicobacter pylori in Southern China: identification of early childhood as the critical period for acquistion. J Infect Dis 1992;166:149-53.
28. Blaser MJ, Chyou PH, Nomura A. Age at establishment of
Helicobacter pylori infection and gastric carcinoma, gastric ulcer and
duodenal ulcer risk. Cancer Res 1995;55:562-5.
29. Crabtree JE. Immune and inflammatory responses to Helicobacter
pylori infection. Scand J Gastroenterol 1996;31(Suppl 215):3-10.
30. DiTommaso A, Xiang ZY, Bugnoli M, Pileri P, Figura, N, Bayeli PF, Rappouli R, Abrigani S, Demagistris MT. Helicobacter pylori-specific CD4(+) T cell clones from peripheral blood and gastric biopsies. Infect. Immun. 1995;63:1102-6.
31. Karttunen R, KarttunenT, Ekre HP, MacDonald TT. Interferon gamma and interleukin 4 secreting cells in the gastric antrum in Helicobacter
pylori positive and negative gastritis. Gut 1995;36:341-5.
32. Mohammadi M, Nedrud J, Redline R, Lycke N, Czinn SJ. Murine CD4 T cell reposne to Helicobacter infection: TH1 cells enhance gastritis and TH2 cells reduce bacterial load. Gastroenterology
1998;113:1848-57.
33. Pappo J, Torrey D, Castriotta L, Savinainen A, Kabok Z, Ibraghimov A.
Helicobacter pylori infection in immunized mice lacking Major
Histocompatibility Complex Class I and Class II functions. Infect Immun 1999;67:337-41.
34. Sommer F, Faller G, Konturek P, Kirchner T, Hahn EG, Zeus J,
Rollinghoff M, Lohoff M. Antrum- and corpus mucosa-infiltrating CD4 (+) lymphocytes in Helicobacter pylori gastritis display a Th1
phenotype. Infect Immun 1998;66:5543-6.
Brooks EG, Graham DY, Reyes VE, Ernst PB. Lymphocytes in the human gastric mucosa during Helicobacter pylori have a T helper 1 phenotype. Gastroenterology 1998;114:482-92.
36. D'Elios MM, Manghetti M, Almerigogna F, Amedei A, Costa F, Burroni D, Baldari CT, Romagnani S, Telford JL, Del Prete G. Different cytokine profile and antigen-specificity repertoire in
Helicobacter pylori-specific T cell clones from the antrum of chronic
gastritis patients with or without peptic ulcer. Eur J Immunol 1997;27:1751-5.
37. D'Elios MM, Manghetti M, De Carli M, Costa F, Baldari CT, Burroni D, Telford JL, Romagnani S, Del Prete G. T helper 1 effector cells specific for Helicobacter pylori in the gastric antrum of patients with peptic ulcer disease. J Immunol 1997;158: 962-7.
Fig. 1:whole-cell protein spots on the 2-DE gel of H. pylori strain associated with the DU patient
Fig. 2:whole-cell protein spots on the 2-DE gel of H. pylori strain associated with the chronic gastritis patient
Fig. 3:whole-cell protein spots on the 2-DE gel of H. pylori strain associated with the gastric cancer patient
Fig. 4:Secreted protein spots on the 2-DE gel of H. pylori strain associated with the chronic gastritis patient
Fig. 5:Secreted protein spots on the 2-DE gel of H. pylori strain associated with the gastric cancer patient