The Prognostic Significance of Total Lymph Node Harvest
in Patients with T
2
–4
N
0
M
0
Colorectal Cancer
Hsiang-Lin Tsai&Chien-Yu Lu&Jan-Sing Hsieh&
Deng-Chyang Wu&Chang-Ming Jan&Chee-Yin Chai&
Koung Shing Chu&Hon-Man Chan&Jaw-Yuan Wang
Published online: 6 March 2007
# 2007 The Society for Surgery of the Alimentary Tract
Abstract In patients with radically resected colorectal carcinoma, lymph node involvement is particularly important for a good prognosis and adjuvant therapy. The number of such lymph node recoveries is still controversial, with recommendations ranging from 6 to 17 nodes. The aim of this study is to determine if a specified minimum number of lymph nodes examined per surgical specimen can have any effect on the prognosis of patients who have undergone curative resection for T2–4N0M0 colorectal carcinoma. Between September 1999 and January 2005, a total of 366 patients who
underwent radical resection for T2–4N0M0 colorectal carcinoma were retrospectively analyzed in a single institution. All
specimen segments were fixed, with node identification performed by sight and palpation. We excluded 186 patients who received postoperative adjuvant chemotherapy via oral or intravenous transmission to prevent possible chemotherapeutic effects on patients’ prognosis; therefore, a total of 180 patients with T2–4N0M0colorectal carcinoma were enrolled into this
study. After the pathological examination, a mean of 12 lymph nodes (range 0–66) was harvested per tumor specimen. No postoperative relapse was found in this group, where the number of examined lymph nodes was 18 or more. Univariate analysis identified the size of the tumor, depth of invasion, grade of tumor, and number of examined lymph nodes, which were significantly correlated with postoperative relapse (allP<0.05). Meanwhile, both the depth of tumor invasion and the number of harvested lymph nodes were independent predictors for postoperative relapse (P<0.05). The 5-year overall survival rate of T2–4N0M0colorectal carcinoma patients who had 18 or more lymph nodes examined was significantly
higher than those who had less than 18 nodes examined (P=0.015). Nodal harvest in patients undergoing radical resection for colorectal carcinoma was highly significant in the current investigation. Our results suggest that harvesting and examining a minimum of 18 lymph nodes per surgical specimen might be taken into consideration for more reliable staging of lymph node-negative colorectal carcinoma.
H.-L. Tsai
:
J.-S. Hsieh:
H.-M. Chan:
J.-Y. Wang (*)Department of Surgery,
Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung 807, Taiwan e-mail: [email protected]
H.-L. Tsai
Department of Emergency Medicine, Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung, Taiwan
C.-Y. Lu
:
D.-C. Wu:
C.-M. JanDepartment of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
C.-Y. Chai
Department of Pathology,
Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
K. S. Chu
Department of Anesthesia,
Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
J.-S. Hsieh
:
D.-C. Wu:
C.-M. Jan:
C.-Y. Chai:
K. S. Chu:
H.-M. Chan
:
J.-Y. WangFaculty of Medicine, College of Medicine, Kaohsiung Medical University,
Keywords Colorectal cancer . Lymph node number . Postoperative relapse . Survival
Introduction
The presence or absence of lymph node metastasis is pivotal in predicting the clinical outcome of patients who have undergone radical surgery for colorectal carcinoma (CRC). The presence of lymph node metastases often determines the use of adjuvant therapy; such adjuvant therapies have been shown unequivocally to provide a disease-free and overall survival benefit in patients with node-positive disease.1Furthermore, the presence of nodal metastases provides important prognostic information.2 There is a consistent risk of substaging tumors and understaging patients when no sufficient lymph nodes are retrieved. Therefore, an accurate assessment of the patho-logic status of the tumor lymph nodes in the resected specimen is essential for reducing the risk of understaging. The number of lymph nodes required for accurate staging of patients is controversial, with recommendations in the literature ranging from 6 to 17 nodes.3–7Current guidelines from the American Joint Committee on Cancer recommend the assessment of 12 nodes or more for accurate staging.8 Many factors that can lead to difficulty in establishing the minimum number have been identified. Among them is the lack of a constant number of lymph nodes in the various parts of the large bowel, the extent of surgical lymphade-nectomy, and the skill and energy of the pathologist.9
Many of the previous recommendations have been based on studies regarding the number of nodes examined in relation to node-positive rates rather than to postoperative relapse and survival data. Only recently have data from large clinical trials demonstrated a correlation between nodal harvest and long-term survival in patients with node-negative disease.9,10The aims of this study are to evaluate the clinical outcome of patients who have undergone radical surgery for T2–4N0M0 CRC and to determine if a
specified minimum number of examined lymph nodes per surgical specimen can have any effect on postoperative relapse and long-term survival.
Material and Methods
Between September 1999 and January 2005, a total 925 patients underwent radical resection or palliative procedures for CRC at the Department of Surgery, Kaohsiung Medical University Hospital. Altogether, 366 patients (39.5%) had tumors classified as T2–4N0M0 CRC, that is, tumors that
have invaded between the muscularis propria and the pericolic–perirectal tissue of the large bowel wall without lymph node metastases, and all these patients received
radical resection. Radical resection is defined as any gross residual tumor that does not remain in the surgical bed, and the surgical resection margin is pathologically negative for tumor invasion. One hundred and eighty-six T2–4N0M0 CRC patients who had received postoperative
adjuvant chemotherapy were excluded to prevent the possible chemotherapeutic effects on patients’ prognosis, and the remaining 180 patients were enrolled into this study. For proximal colon tumors, lymphadenectomy was ex-tended to the origin of the ileocolic, right colic, and middle colic arteries. For distal colon lesions and rectal tumors, it was extended to the origin of the inferior mesenteric artery along the preaortocaval space. Total mesorectal excision was performed in all patients with tumors of the middle and lower rectum and a distal clearance of at least 2 cm from the edge of the tumor. Clinical stage and pathological features of the primary tumors were defined according to the sixth edition of the TNM staging system of the Inter-national Union Against Cancer.11
All the surgical specimens were fixed in 10% formalin solution and routinely processed for paraffin embedding. The number of examined lymph nodes was ascertained by reference to the histopathologic report of each patient. Lymph nodes were identified in the surgical specimens by sight and palpation. Routine histological examination was performed using hematoxylin and eosin staining. Histolog-ical processing of the specimens was the same for all patients. No special fat clearance or staining techniques were employed. The mesenteric and adventitial fat was carefully displaced by manual pressure, visually inspected for lymph nodes, and palpated for the presence of firm tissue that was indicative of a lymph node. Representative sections were examined in all grossly involved lymph nodes; grossly uninvolved lymph nodes smaller than 3 mm were submitted whole, and those 3 mm or larger were bivalved and submitted for routine hematoxylin and eosin examina-tion. The following histopathologic features were assessed for each tumor specimen including tumor type (classified as adenocarcinoma or mucinous carcinoma), invasive depth (classified as T2, T3, and T4), and tumor grade (classified as well, moderately, and poorly differentiated).
The median follow-up period was 36 months (range 18– 68 months). All 180 patients were routinely followed up on until their deaths. The serum carcinoembryonic antigen level was measured every 3 months for the first 2 years, and every 6 months for the following 3 years. Abdominal ultrasonography was performed every 6 months. Annual computed tomography for the chest and abdomen was also carried out. The development of new recurrent or metastatic lesions after operation was defined as a postoperative relapse. The median time to recurrence of these patients was 18.3 ± 4.5 months. The number of lymph nodes examined per specimen was recorded to determine if a
specific cutoff could affect clinical outcome. The cutoff we considered to be the best indicator for separating patients with regard to survival was that which showed the clearest rise in statistical significance. Patients were further divided into two groups based on the threshold of the adequate number of examined lymph nodes.
Statistical Analysis
All data were analyzed by the Statistical Package for the Social Sciences, version 11.5 (SPSS Inc., Chicago, IL, USA). The univariate analysis of clinicopathologic features between the two groups was compared using the chi-square test. The multivariate analysis of independent prognostic factors for postoperative relapse was determined using logistic regression analysis. The cumulative survival rates were calculated by the Kaplan–Meier method, and the differences in survival rates were analyzed by the log-rank test. A P value of less than 0.05 was considered to be statistically significant.
Results
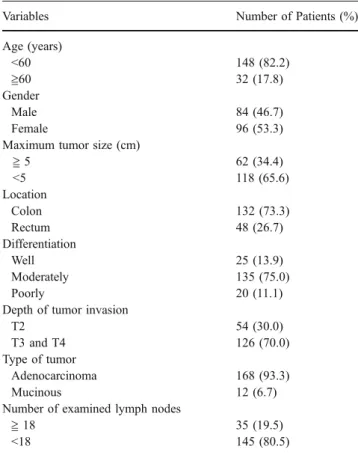
The clinical and pathologic data regarding the 180 T2–4N0M0
CRC patients are summarized in Table 1. There were 84 men (46.7%) and 96 women (53.3%). The average age was 69.0 years (range 32–93 years). The number of sites where the tumor was at the colon was 132 (73.3%) and 48 (26.7%) at rectum. One hundred and sixty-eight patients (93.3%) were classified as adenocarcinoma in histology, and 12 patients (6.7%) as mucinous carcinoma. With regard to the histological types of these tumors, 25 were well-differentiated carcinoma, 135 were moderately differentiat-ed carcinoma, and 20 were poorly differentiatdifferentiat-ed carcinoma. A mean number of 12 lymph nodes (range 0–66) were examined per tumor specimen. The average value of identified lymph nodes in tumors of the right colon, left colon, and rectum was 14.84, 11.28, and 10.12, respective-ly. From the relationship between postoperative relapse and the number of examined lymph nodes, we found that those with 18 or more lymph nodes had no postoperative relapse. Therefore, the adequate number of lymph nodes to separate the T2–4N0M0CRC patients into subgroups was set at 18 in
our study. The incidence of postoperative relapse among the subgroups with lymph nodes <18 was not prominently different, with a range of 25.0 to 30.8%. On the basis of this finding, 180 T2–4N0M0CRC patients were divided into two
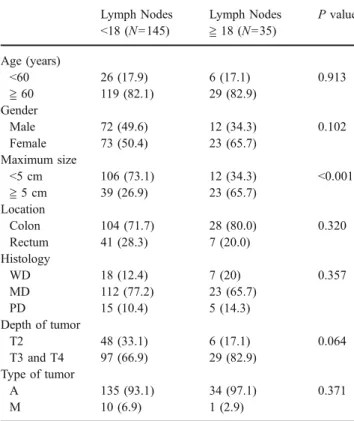
groups (group 1: examined lymph nodes fewer than 18; group 2: examined lymph nodes equal to or more than 18). By univariate analysis, there were no significant differences regarding the age, gender, tumor site, invasive depth, tumor
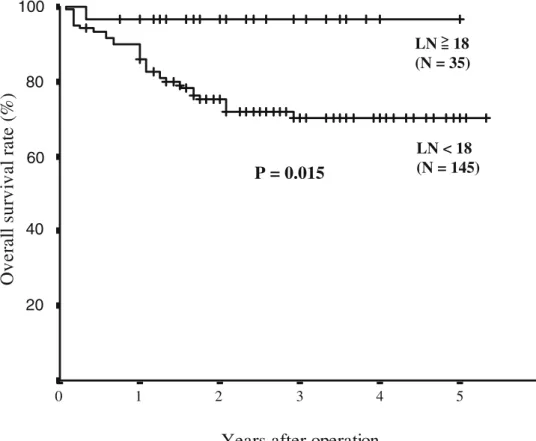
grade, and tumor type between the two groups, except for the tumor size between the two groups (Table2;P<0.001). Moreover, the presence of postoperative relapse signif-icantly correlated with the tumor size (P=0.040), invasive depth (P=0.031), histology (P=0.047), and the number of examined lymph nodes (Table3;P<0.001). Figure1details the overall survival rate of CRC patients according to the number of examined lymph nodes (≧ 18 or <18). The survival rate of the number of examined lymph nodes <18 group was significantly lower than that of the examined lymph nodes ≧ 18 group using a log-rank test (P=0.015). Using multivariate logistic regression analysis, both the number of examined lymph nodes (P=0.005) and depth of tumor invasion (P=0.028) were demonstrated to be independent predictors for postoperative relapse (Table4). Regarding the sites of postoperative relapse, 17, 9, 8, 7, 6, and 6 were attributed to the liver, local recurrence, peritoneal carcinomatosis, the bones, retroperitoneal causes, and the lungs, respectively.
Discussion
Lymph node involvement is one of the most important prognostic factors after radical surgery for CRC.12–14 The
Table 1 Clinicopathologic Characteristics of 180 T2–4N0M0
Colorec-tal Cancer Patients
Variables Number of Patients (%)
Age (years) <60 148 (82.2) ≧60 32 (17.8) Gender Male 84 (46.7) Female 96 (53.3)
Maximum tumor size (cm)
≧ 5 62 (34.4) <5 118 (65.6) Location Colon 132 (73.3) Rectum 48 (26.7) Differentiation Well 25 (13.9) Moderately 135 (75.0) Poorly 20 (11.1)
Depth of tumor invasion
T2 54 (30.0)
T3 and T4 126 (70.0)
Type of tumor
Adenocarcinoma 168 (93.3)
Mucinous 12 (6.7)
Number of examined lymph nodes
≧ 18 35 (19.5)
prognostic value of lymph node involvement in patients who undergo resection for CRC has been well estab-lished.14–17 In addition to the prognostic significance of nodal metastases, the presence of tumor cells in the regional node basin is an important criterion for a recommendation of adjuvant systemic therapy.18An accurate examination of the surgical specimen is mandatory to assess the lymph node status of the tumor correctly.6 Theoretically, all the lymph nodes should be harvested from the surgical speci-mens and examined to confirm a tumor is negative of lymph node involvement.
The actual number of lymph nodes must be harvested and examined in the resected bowel because CRC has not yet been determined definitively. Despite recent interest in this subject, the number of nodes required to accurately stage patients is controversial, and considerable variation exists among studies. The variability in the number of lymph nodes in the various regions of the large bowel, the extent of surgical lymphadenectomy, the searching ability for lymph nodes by pathologists, and the different statistical methods employed in different studies are major impedi-ments. These variables most probably explain the lack of agreement in determining a universally valid minimum number of lymph nodes. Scott and Grace found that when at least 13 lymph nodes are examined histologically, more
than 90% of the specimens containing nodal metastases can be identified.18 In 1990, the Working Party Report to the World Congress of Gastroenterology in Sydney recommen-ded that a minimum of 12 lymph nodes be recovered.5 Goldstein et al.6reported the probability of correctly classi-fying a colorectal tumor as node-positive when 17 lymph nodes are examined. Similarly, the high-risk groups for recurrence/metastasis were identified in Dukes’ A and B CRC patients with harvested lymph nodes≦ 14.19Hernanz et al.20 and Caplin et al.21 demonstrated that a minimum of six lymph nodes examined per specimen is necessary for correct Dukes’ B staging, and six or fewer lymph nodes examined in Dukes’ stage B CRC patients correlated with poorer survival when compared with examining seven or more. Moreover, it has been suggested that the examination of at least 14 nodes after resection of T2 or T3 carcinoma of the colon and rectum will accurately stage the lymphatic basin.22
As a rule, three variables must be considered when examining the issue of nodal harvest: patient factors, surgical factors, and pathologic factors. Patient factors
Table 3 Univariate Analysis of Clinicopathologic Features between
T2–4N0M0 Colorectal Cancer Patients with and Without
Post-operative Relapse Postoperative relapse (+) (N=42) (%) Postoperative relapse (-) (N=138) (%) P value Age (years) <60 7(16.7) 25(18.1) 0.830 ≧ 60 35(83.3) 113(81.9) Gender Male 20(47.6) 63(45.7) 0.823 Female 22(52.4) 75(54.3) Maximum size <5 cm 22(52.4) 96(69.5) 0.040 ≧ 5 cm 20(47.6) 42(30.5) Location Colon 31(73.8) 101(73.2) 0.936 Rectum 11(26.2) 37(26.8) Histology WD 2(4.8) 22(15.9) 0.047 MD 32(76.2) 104(75.4) PD 8(19) 12(8.7) Depth of tumor T2 7(16.7) 47(34.1) 0.031 T3 and T4 35(83.3) 91(65.9) Type of tumor A 37(88.1) 131(94.9) 0.120 M 5(11.9) 7(5.1)
Number of examined lymph nodes
<18 42(100) 103(74.6) <0.001
≧ 18 0(0) 35(25.4)
WD = well-differentiated, MD = moderately differentiated, PD = poorly differentiated, A = adenocarcinoma, M = mucinous carcinoma Table 2 Univariate Analysis of Clinicopathologic Features of
T2–4N0M0 Colorectal Cancer Patients Between the Number of
Examined Lymph Nodes <18 and≧ 18
Lymph Nodes <18 (N=145) Lymph Nodes ≧ 18 (N=35) P value Age (years) <60 26 (17.9) 6 (17.1) 0.913 ≧ 60 119 (82.1) 29 (82.9) Gender Male 72 (49.6) 12 (34.3) 0.102 Female 73 (50.4) 23 (65.7) Maximum size <5 cm 106 (73.1) 12 (34.3) <0.001 ≧ 5 cm 39 (26.9) 23 (65.7) Location Colon 104 (71.7) 28 (80.0) 0.320 Rectum 41 (28.3) 7 (20.0) Histology WD 18 (12.4) 7 (20) 0.357 MD 112 (77.2) 23 (65.7) PD 15 (10.4) 5 (14.3) Depth of tumor T2 48 (33.1) 6 (17.1) 0.064 T3 and T4 97 (66.9) 29 (82.9) Type of tumor A 135 (93.1) 34 (97.1) 0.371 M 10 (6.9) 1 (2.9)
WD = well-differentiated, MD = moderately differentiated, PD = poorly differentiated, A = adenocarcinoma, M = mucinous carcinoma
may reflect anatomic or individual variability in nodal harvest.23 For example, some studies have demonstrated that right-sided resections are associated with a greater nodal harvest than left-sided resections.20 Likewise, the mean number of examined lymph nodes for right-sided resections is more than left-sided resections in our investigations. Leopoldo et al.24 have also reported that lymph node retrieval in TNM stage II CRC patients is affected by the patient’s age, gender, tumor grade, and tumor site. Conversely, we have identified that a significant number of retrieved lymph nodes ≧ 18 is influenced by tumor size in our analysis. The incidence of ≧ 18 lymph node harvest increases with larger-sized≧ 5 cm tumors.
Nevertheless, the impact of the pathology and surgery as it pertains to colorectal lymph node harvest is largely unreported. Given that this is a single institution, fairly
uniform pathological and surgical techniques would be expected. It is possible that some of the variability is patient related, i.e., that the number of lymph nodes in a given patient varies, and that this may have an independent effect on survival. In the present study, no postoperative relapse was observed in T2–4N0M0CRC patients with a harvest of
18 or more lymph nodes. On the other hand, our findings reveal that the number of lymph node retrievals of at least 18 was significantly related to the postoperative relapse for T2–4N0M0 CRC patients, in addition to the conventional
depth of tumor invasion in TNM staging. Indeed, the poorer overall survival rate is also observed in T2–4N0M0 CRC
patients with 17 or fewer lymph nodes examined. Because the number of examined lymph nodes has been proven to be crucial in the prediction of postoperative relapse for T2–4N0M0
CRC patients, the examination of 17 or fewer lymph nodes
Years after operation
6 5 4 3 2 1 0
O
v
e
ra
ll
s
u
rv
iv
a
l ra
te
(%
)
1.0 .8 .6 .4 .2 .0100
80
60
40
20
P = 0.015
LN
18
(N = 35)
LN < 18
(N = 145)
= > Figure 1 Cumulative overall5-year survival rates of T2–4N0M0
colorectal cancer patients were
analyzed by the Kaplan–Meier
method with the differences compared by a log-rank test. Patients who had 18 or more lymph nodes examined had a significantly higher survival rate than those who had less than 18 nodes examined (P=0.015).
Table 4 Correlation between Postoperative Relapse and Clinicopathologic Features of T2–4N0M0CRC Patients Using Multivariate Logistic
Regression Analysis
Variables b SE P value Hazard Ratio 95% Confidence Interval
Tumor size (≧ 5 cm/<5 cm) 0.713 0.500 0.154 2.040 0.766–5.437
Histology (PD/WD+MD) 0.125 0.759 0.869 1.133 0.256–5.018
Depth (T3+T4/T2) 1.039 0.473 0.028 2.826 1.117–7.147
Lymph node retrieval (<18/≧ 18) 3.019 1.081 0.005 20.481 2.462–170.399
in T2–4N0M0 CRC patients should be considered during
follow-up meticulously for postoperative surveillance. Perhaps patients with T2–4N0M0 CRC with 17 or fewer
nodes examined might be potential candidates for post-operative adjuvant chemotherapy. Despite the numbers of lymph node harvest or the extent of lymph node dissection not greatly improving the accurate tumor staging, the increase of examined numbers of tumor-free lymph nodes would probably decrease the incidence of understaging or alter further therapies for these patients. However, additional work in larger patient populations by means of long-term follow-up studies is mandatory for confirming this hypothesis.
Conclusion
In summary, the recovery and examination of at least 18 lymph nodes per surgical specimen may be essential in reaching a more strict level of accuracy when defining operations for T2–4N0M0 CRC as a curative resection. An
increase in the number of tumor-free lymph nodes has been suggested as clinically important, and this parameter should be taken into consideration in CRC patients without metastatic lymph nodes. Further investigation regarding surgical and pathologic standardization is needed with the goal of reducing variability, thus permitting more consistent staging of patients with CRC.
References
1. Wolmark N, Rockette H, Fisher B, et al. The benefit of leucovorin-modulated fluorouracil as postoperative therapy for primary colon cancers: results from the National Surgical Adjuvant Breast and Bowel
Project. J Clin Oncol 1993;11:1879–1887.
2. Greene FL, Stewart AK, Norton HJ. A new TNM staging strategy for node-positive (stage III) colon cancer: an analysis of 50,042
patients. Ann Surg 2002;236:416–421.
3. Greenson JK, Isenhart CE, Rice R, Mojzisik C, Houchens D, Martin EW Jr. Identification of occult micrometastases in pericolic
lymph nodes of Dukes’ B colorectal cancer patients using
monoclonal antibodies again cytokeratin and CC49. Cancer
1994;73:563–569.
4. Scott KWM, Grace RH. Detection of lymph node metastases in colorectal carcinoma before and after fat clearance. Br J Surg
1989;76:1165–1167.
5. Fielding LP, Arsenault PA, Chapuis PH, et al. Clinicopathologic staging for colorectal cancer: an international documentation system (IDS) and an international comprehensive anatomical terminology (ICAT). J Gastroenterol Hepatol 1991;6:325–344.
6. Goldstein NS, Sanford W, Coffey M, Layfield LJ. Lymph node recovery from colorectal resection specimens removed for adenocarcinoma: trends over time and a recommendation for a minimum number of lymph nodes to be recovered. Am J Clin Pathol 1996;106:209–216.
7. Fielding LP. Clinical-pathologic staging of large-bowel cancer: a report of the ASCRS Committee. Dis Colon Rectum 1988;31:204–209. 8. Nelson H, Petrelli N, Carlin A, et al. Guidelines 2000 for colon
and rectal cancer surgery. J Natl Cancer Inst 2001;93:583–596. 9. Fabio C, Annarita P, Vieri B, et al. Lymph node recovery from
colorectal tumor specimens: recommendation for a minimum number of lymph nodes to be examined. World J Surg
2002;26:384–389.
10. Fobnson PM, Malatjalian D, Porter GA. Adequacy of nodal harvest in colorectal cancer: a consecutive cohort study. J
Gastrointest Surg 2002;6:883–890.
11. International Union Against Cancer. TNM classification of malignant tumors, 6th ed. New York: Wiley-Liss, Inc., 2002. 12. Steup WH, Moriya Y, van de Velde CJ. Patterns of lymphatic
spread in rectal cancer. A topographical analysis on lymph node
metastases. Eur J Cancer 2002;38:911–918.
13. Park YJ, Park KJ, Park JG, Lee KU, Choe KJ, Kim JP. Prognostic factors in 2230 Korean colorectal cancer patients: analysis of consecutively operated cases. World J Surg 1999;23:721–726. 14. Wolmark N, Fisher B, Wieand HS. The prognostic value of the
modification of the Dukes C class of colorectal cancer: an analysis
of the NSABP trial. Ann Surg 1986;139:846–852.
15. Kubota K, Akasu T, Fujita S, Sugihara K, Moriya Y, Yamamoto S. Clinical and pathological prognostic indicators with colorectal
mucinous carcinomas. Hepatogastroenterology 2004;51:142–146.
16. Goldstein NS. Lymph node recoveries from 2427 pT3 colorectal resection specimens spanning 45 years: recommendations for a minimum number of recovered lymph nodes based on predictive
probabilities. Am J Surg Pathol 2002;26:79–89.
17. Petersen VC, Baxter KJ, Love SB, Shepherd NA. Identification of objective pathological prognostic determinants and models of
prognosis in Dukes’ B colon cancer. Gut 2002;51:65–69.
18. Scott KW, Grace RH, Gibbons P. Five-year follow-up study of the fat clearance technique in colorectal carcinoma. Dis Colon Rectum 1994;37:126–128.
19. Mukai M, Sato S, Nishida T, et al. Selection criteria for high risk and low risk groups of recurrence and metastasis in patients with primary colorectal cancer. Oncol Rep 2003;10:1753–1758. 20. Hernanz F, Revuelta S, Redondo C, Madrazo C, Castillo J,
Gomez-Fleitas M. Colorectal adenocarcinoma: quality of the assessment of lymph node metastases. Dis Colon Rectum
1994;37:373–377.
21. Caplin S, Cerottini JP, Bosman FT, Constanda MT, Givel JC. For
patients with Dukes’ B (TNM stage II) colorectal carcinoma,
examination of six or fewer lymph nodes is related to poor
prognosis. Cancer 1998;83:666–672.
22. Wong JH, Severino R, Homnebier MB, Tom P, Namiki TS. Number of nodes examined and staging accuracy in colorectal
carcinoma. J Clin Oncol 1999;17:2896–2900.
23. Canessa CE, Badia F, Socorro F, Fiol V, Hayek G. Anatomic study of the lymph nodes of the mesorectum. Dis Colon Rectum
2001;44:1333–1336.
24. Leopoldo S, Giovanni B, Domenico I, et al. Number of lymph nodes examined and prognosis of TNM stage II colorectal cancer. Eur J Cancer 2005;41:272–279.